
Abstract
Aims:
To examine changes in child mental health symptoms following inpatient family unit treatment after long-term unsuccessful treatment in community and child psychiatry outpatient services. Follow-up from referral and admission to 3 and 12 months.
Methods:
Standardized questionnaires measuring the child mental health symptoms and parental anxiety and depression converted to standardized scores and compared to each child’s clinical diagnosis.
Results:
Significant group mean improvement on almost all problem scales at the 3-month follow-up (T2) remaining through 12-month follow-up (T3) relative to admission (T1). Aggression showed the highest levels and largest improvements. Statistically significant improvements were widespread, whereas clinically significant improvements were found for some diagnostic groups on diagnosis-related problems and secondary problems. Improvement in child symptoms were partly correlated with improvement in parental anxiety symptoms.
Implications:
Even previously nonresponding children may benefit from broad tailored interventions including parents and the wider system. Development of systematic component approaches is needed.
Background
We have chosen to study a relatively small clinical group of children: those referred to CAMHS family units (family inpatient units in child and adolescent mental health services at hospitals) offering inpatient evaluation and treatment for patients and parents together. These children are of interest because they are typically nonresponders to previous clinical services and have multiple problems combined with family problems. Furthermore, family units are scarcely studied with quantitative approaches. This study focuses on changes in child symptom and profiles 3 and 12 months after admission to the family units, related to child diagnoses and parental mental health symptoms.
These children are nonresponders in that they have not responded satisfactorily following evaluation and treatment in community services and in outpatient CAMHS services. They have a mean previous history of more than 4 years in community services and more than 2 years in CAMHS services (Rimehaug, Berg-Nielsen, & Wallander, 2012). Diagnostically, this is a heterogeneous group, with a high prevalence of comorbidity, including attentional, developmental, and learning problems; mental health problems (emotional, social, or behavioral); and family problems. They were admitted to the CAMHS family unit because of a combination of family problems and individual problems. The family problems may include parental problems regarding mental health, addiction, somatic health, criminal behavior, economic problems, traumatizing events and history, interaction problems, and conflicts between parents, with the child, with the extended family or with community or hospital services. Another consideration is that caring for children with prolonged problems can be emotionally taxing and burdensome for parents, who may experience self-blame (Moses, 2010) and emotional distress (Sawyer et al., 2002), especially when facing severe, long-standing problems including externalization problems (Early, Gregoire, & Mcdonald, 2002; Gowers & Bryan, 2005).
The primary aim of the family units is to improve parental coping and the interactional quality between parents and children. Changes in child symptoms are considered important but secondary aims. As part of the treatment process, family units often evaluate the system factors affecting the child and the family and often include a child diagnostic re-evaluation. Parents have often experienced prolonged strain and distress (Early et al., 2002; Gowers & Bryan, 2005), and their functioning likely differs from that of community parents (O’Connor, 2002). Bidirectional effects between child problems and system factors are expected (O’Connor, 2002), and the clinical process attempts to utilize parents as resources in treatment and to aid them in improving their parenting, implying extensive parental involvement (Sundet, 2009). The inpatient stay at family units typically lasts 2–4 weeks, with an outpatient follow-up period extending several months after discharge.
A Swedish study showed more positive family climate following family unit stays (Hansson et al., 1992). A Canadian study showed short-term improvements in child and parental symptoms and in family functioning (Volk, 2004). A Norwegian study showed that parental warmth increased following a family unit stay, especially toward children with attention, learning, and developmental problems, and that mothers’ anxiety symptoms improved significantly. These improvements correlated with improvements in child internalized and externalized symptoms on the Child Behavior Checklist (CBCL; Rimehaug et al., 2012). A similar study from Germany showed improvements in child symptoms, parenting, and parent mental health maintained across a 4-week follow-up after family unit treatment.
Aims
We therefore wanted to analyze the changes in child symptoms in family units more closely and with a longer follow-up period, along with associations with child diagnostic group and parental symptoms. This could be done by accessing supplementary data from the Norwegian study.
The child problems in this group are assumed to be chronic and heterogenic, although improvement in some of the symptoms and improved functioning are expected. We therefore aimed to evaluate changes in child symptom profiles and maximum scales rather than a single outcome.
Waiting for, entering, participating in treatment, being discharged, and returning to daily life may alter symptom profiles several times. We chose to concentrate primarily on the symptom changes between admission to the family unit and the 3-month outpatient follow-up but also extending this to a 12-month follow-up. For some of the children, symptoms were also evaluated before the waiting period preceding admission.
We will address four questions:
Did child symptoms change between admission and the 3-month follow-up, and were the changes sustained through the 12-month follow-up?
Did child symptom levels change during the waiting period?
Are changes in child symptoms and changes in parental mental health correlated?
Were there differences in child change profile between groups defined by child clinical diagnoses?
All questions were addressed according to each of the 10 symptom scales defined by the CBCL (Achenbach & Rescorla, 2001) and also for the first three questions for the scales showing the highest score for each child at admission or the greatest improvement at the 3-month follow-up. We also examined whether change from admission to the 3-month follow-up was related to a child’s age or gender.
Methods
Materials
The inpatient family unit samples
The families were recruited in a clinical multi-center study from those referred to three CAMHS family inpatient units. All referred families were consecutively invited to participate in the study during a 4-year period. The recruitment areas included two cities, several small towns, and large rural areas. Of 120 eligible families, at least one parent in 112 families gave their informed consent to participate and responded to other parts of a larger study. The CBCL was returned from 81 families on at least one occasion, T0–T1–T2–T3 (68% of those eligible). Of these participants, 74 completed the CBCL at admission (T1), 50 completed the 3-month follow-up after discharge (T2), and 33 completed the 12-month follow-up assessment (T3). T0 data collection occurred immediately after referral, prior to a waiting period that averaged 8 weeks.
CBCL data for T1 and T2 were thus available for 50 cases, including 40% of the originally eligible participants and 61% of those completing any CBCL. If both parents responded, the mother’s reports were selected to represent child symptoms. Parental anxiety and depression scores were available for 80% of those with T1–T2 CBCL data. Due to practical problems, as often occurs in naturalistic settings, the T0 measurement was collected only from a subsample of 11 out of the last 12 families invited into the study (representing 9% of those eligible, 22% of T1–T2 participants). Thus, the T0 measurement could only be used as a supplementary exploration of stability of T0–T1 symptom scores and is not included in the flowchart in Figure 1.
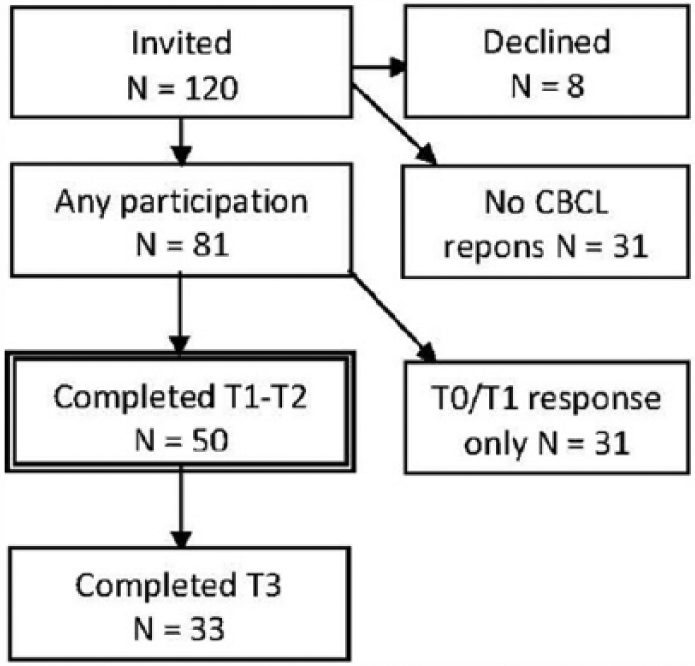
Participants flowchart; inclusion, and responses at each longitudinal stage T0-T1-T2-T3.
In the core sample of 50 families, 3 of the selected informants were fathers, and the average parental age was 40.2 years (SD, 7.2). In total, 30% of the referred children in these families were girls, and the mean age of the children was 11.2 years (SD, 2.3).
Questionnaires were distributed by clinicians and returned to research assistants at the family units in sealed envelopes.
The participating children had already received community services for an average of 5.1 years (SD, 2.7; range, 1.0–11 years) prior to receiving services in outpatient child psychiatric clinics for an average of 2.5 years (SD, 2.5; range, 0.5–10 years) before referral to the family unit.
Clinical services and diagnostic evaluation
The family units admit families for a 2- to 4-week stay. Each family member participates in a concentrated full-day schedule, with some days extending into the evenings, including assessment of the child and treatment for the child and family (Sundelin & Hansson, 1999; Sundet, 2009). Families admitted to family units represent approximately 1% of the cases referred to CAMHS services in the areas.
Parents not living together participate in the clinical process together, in parallel or during separate periods depending on the level of conflict between them. In some families, extended family is included in the clinical process, usually as outpatients. For children in foster care, foster parents are usually admitted, sometimes with biological parents included as outpatients.
The treatment programs are combinations of narrative and systemic family therapy (Lorås, Bertrando, & Ness, 2017) aimed at improving communication, mutual understanding, and daily interaction, combined with psychoeducational interventions aimed at improving understanding of child and parent functioning. In addition, manualized interventions for specific child diagnoses were used.
Clinical assessments are done using standardized instruments and based on International Classification of Diseases, 10th Revision (ICD-10) criteria discussed in a multidisciplinary team including a child psychiatrist or specialist in clinical psychology. We chose to categorize each child in one or two of the following four broad, overlapping categories: the “emotional” group (anxiety, affective, eating, and emotional disorders; F30–F42, F50, and F92–94; n = 16); the “developmental” group (developmental, learning, and tics disorders; F70–F89 and F95; n = 15); the “hyperkinetic” group (hyperkinetic disorders; F90.0–F90.9; n = 12); and the “conduct” group (conduct disorders; F91–F92; n = 6). In total, 40% of the children were assigned to two or more of these categories (comorbidity). One of the participating units did not report clinical diagnoses for the majority of cases, so this information was available for 34 cases; 68% of the sample.
Instruments
Child problems as described by parents were measured by the CBCL problem scales, Norwegian version (Nøvik, 1999), consisting of 120 items forming eight subscales and the subtotals of the Internalizing Problems Scale and Externalizing Problems Scale. The CBCL is part of a broader multi-informant assessment battery of competencies and mental health problems, the Achenbach System of Empirically Based Assessment (ASEBA; Achenbach & Rescorla, 2001).
Parental anxiety and depression symptoms were measured with the Hospital Anxiety and Depression Scales (HADS; Herrmann, 1997; Zigmond & Snaith, 1983). HADS produces separate scores for anxiety (seven items) and depression (seven items). Detailed accounts of the psychometric properties of the scales can be found elsewhere (Mykletun, Stordal, & Dahl, 2001). The concepts of parental anxiety and depression used in this article refer to symptom levels and not to diagnostic categories.
Statistics
All analyses were performed in SPSS 21.0 unless otherwise specified. All CBCL variables were represented by T-scores based on US norms, as Norwegian norms were not available to the clinics at the time of the study.
Change over time in the clinic sample for continuous variables was tested using general linear models (GLMs) repeated measurements. Due to a small T0 sample and T3 dropout, T0–T1 and T2–T3 longitudinal differences were analyzed separately from T1 to T2. Group differences for continuous variables are reported from one-way analysis of variance (ANOVA) GLM models.
Associations between continuous variables were analyzed with Pearson’s product–moment correlations in SPSS. The threshold for statistical significance was set at p < .05 unless otherwise specified. A threshold of p < .10 was allowed for the T1–T2 repeated measures, which tested a one-sided hypothesis of improvement rather than a general difference.
Due to high rates of comorbidity, low numbers and unbalanced group size, children in different diagnostic groups could not be directly compared in ANOVAs but are evaluated based on the standardized T-scores. The low number of subjects limited the statistical power for some comparisons related to the diagnostic groups and related to T0.
Multilevel analyses were not required in this study because there were no significant differences between the sampling clusters.
Results
Among those relatively few who were asked to complete the CBCL at admission, the total mean scores at referral (T0) for each problem subscale were in the high subclinical range (T = 65–70; Mean score at T0; M0 = 68.7, SD = 8.1) for all eight subscales and remained at that level in this subsample at admission (Mean score at T1; M1 = 65.7, SD = 6.5).
In the main study period T1–T2, no symptom scale showed average change for all participants at a clinically significant level (ΔT1–2 > 10), reflecting problem heterogeneity and outcome heterogeneity for the total sample. However, the average change for the total sample was statistically significant for all symptom scales when testing for improvement only (one-sided test; p < .10 as minimum), with the largest average change for aggression (see Table 1). However, the individual top scale at T1 and largest change at T1–T2 could be seen on any of the eight symptom scales, confirming the diagnostic heterogeneity of the sample. Clinically significant changes (ΔT1–2 > 10) were observed on at least one scale for 68% of the children, with 22% improving more than 20 T-points on at least one scale (see Figure 2). At T3, the 12-month follow-up, 30% did not respond or had missing data on the CBCL, but a simulation showed that even if all missing observations at T3 were replaced with T1 values (= no change), there were still statistically significant group average improvements from T1 to T3 for all eight symptom scales, with an average tendency toward larger improvements at long-term follow-up.
Change in child CBCL symptom level from admission to 3-month follow-up (T1 to T2) after family inpatient stay.
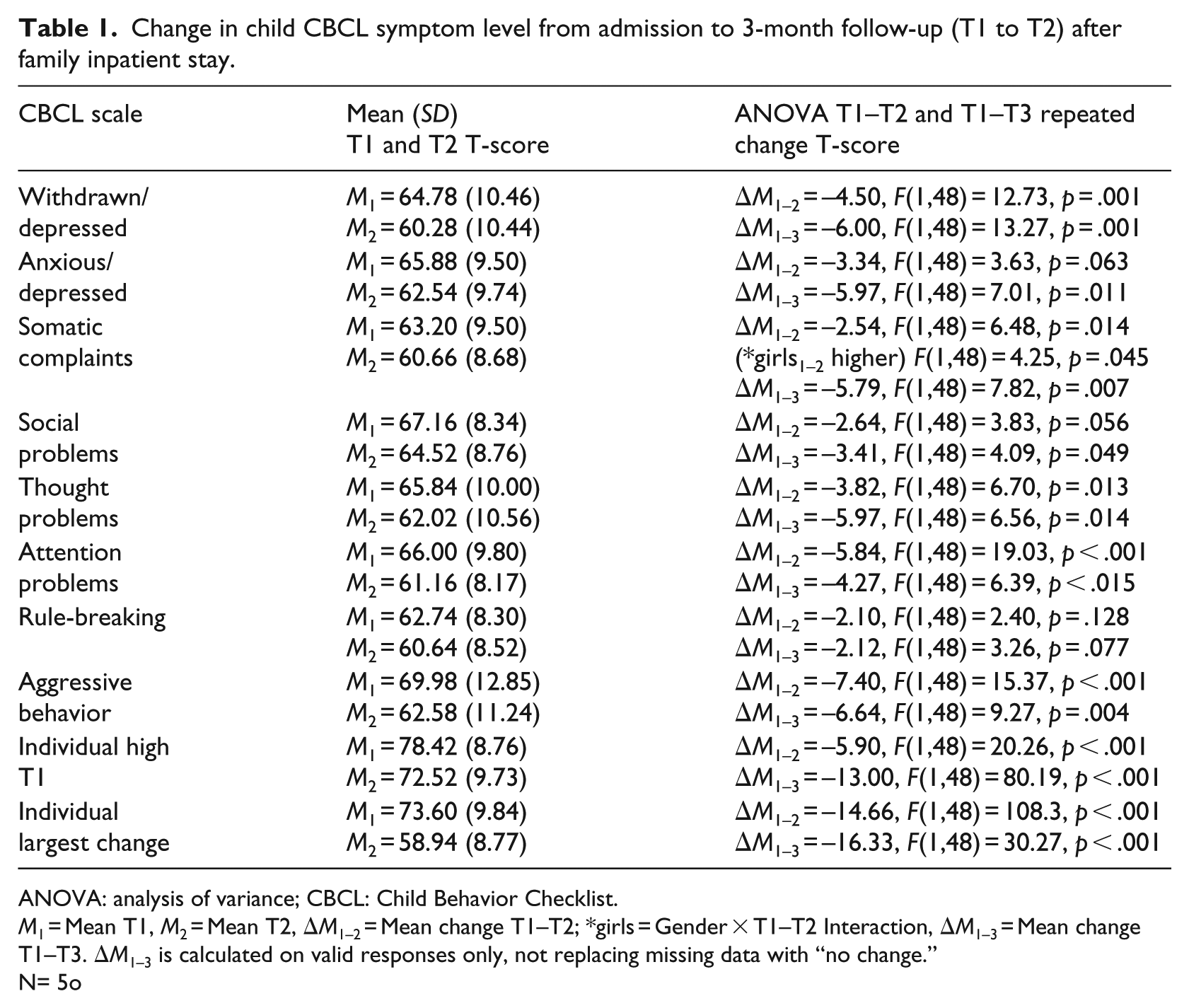
ANOVA: analysis of variance; CBCL: Child Behavior Checklist.
M1 = Mean T1, M2 = Mean T2, ΔM1–2 = Mean change T1–T2; *girls = Gender × T1–T2 Interaction, ΔM1–3 = Mean change T1–T3. ΔM1–3 is calculated on valid responses only, not replacing missing data with “no change.”
N= 5o
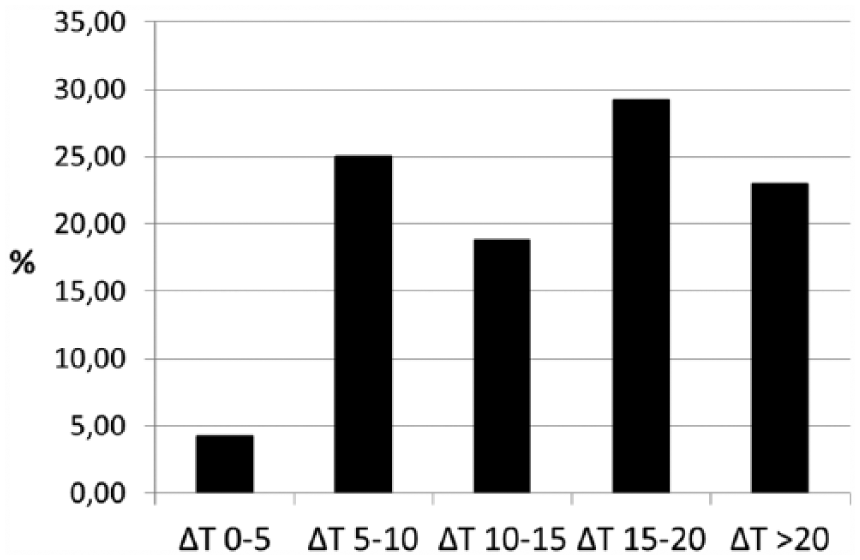
Rate of largest individual change among child CBCL problem scales distributed across categories of improvement in symptom T-score; Δ T from admission to 3-month follow-up.
When separating the four major nonexclusive diagnosis groups, there were marked group differences in the profiles of symptom change. Four scales showed significant average change in three of the groups, namely, withdrawn/depressed problems, attention problems, thought problems, and aggressive behaviors (see Table 2 and Figure 2). The exceptions were withdrawn/depressed problem did not improve significantly in the “hyperkinetic” group, but were close to normal or low subclinical levels. Thought problems did not change in the “developmental” group but improved within subclinical or normal levels for the other groups. Attention problems improved significantly subclinical to nonclinical level in the “emotional” group, but did not change significantly in the “conduct” group. Aggressive behaviors that showed the highest levels at T1 and the greatest decrease from T1 to T2 did not show that in the “developmental” group.
Four major ICD-10 diagnostic groups change on Child Behaviour Checklist (CBCL) problem scale T-scores; means T1 and T2 and ANOVA for the longitudinal changes. Only scales with T1-T2 change > 5 (T-scores) included in the table.
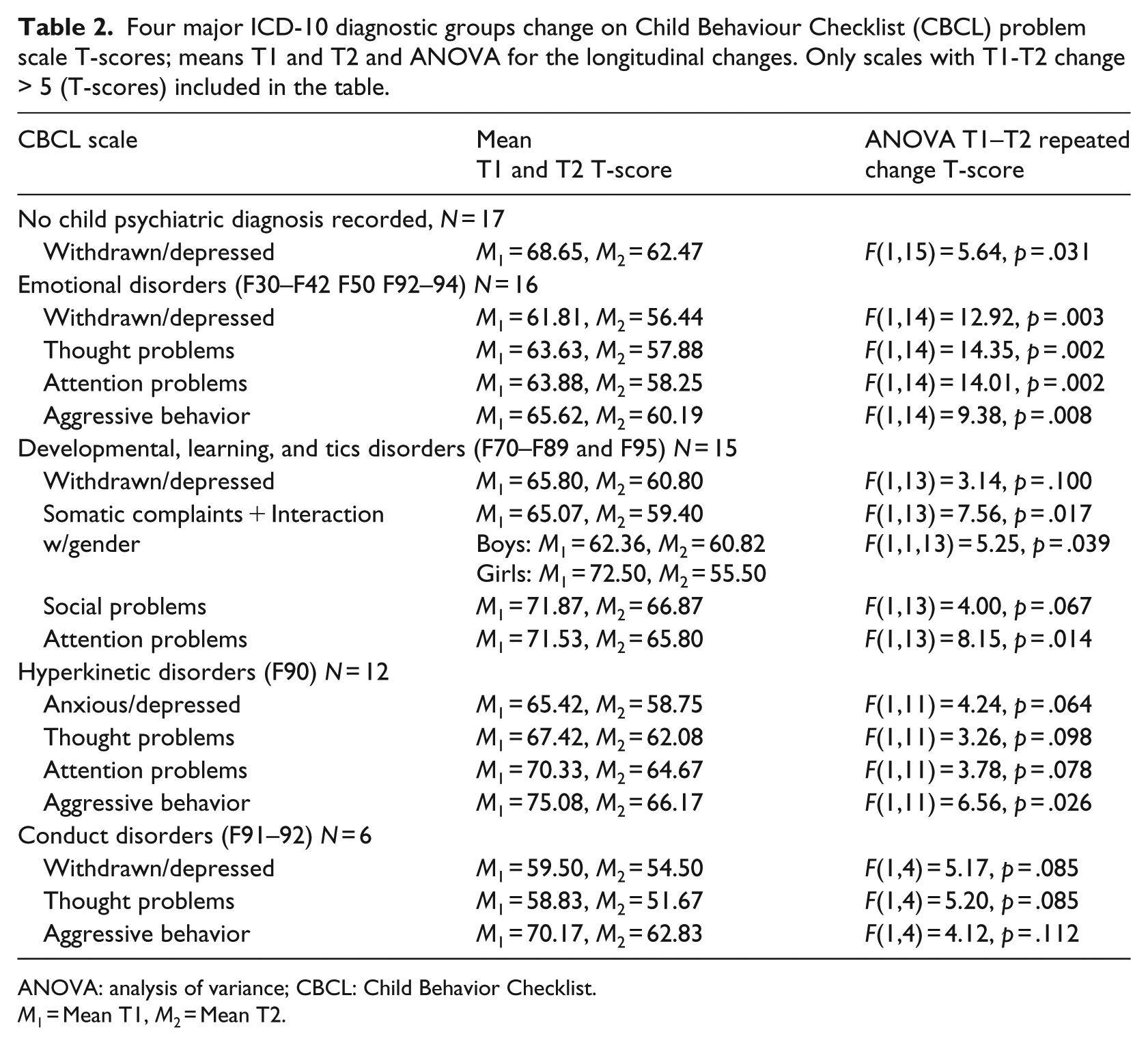
ANOVA: analysis of variance; CBCL: Child Behavior Checklist.
M1 = Mean T1, M2 = Mean T2.
Anxious/depressed problems, social problems, and somatic problems (only among girls) showed statistically significant changes in one group each (see Table 2 for details).
All scales with significant average changes showed an effect size greater than d = 0.30 (Figure 3), with the majority between d = 0.40 and d = 0.70—when analyzing the whole sample together.
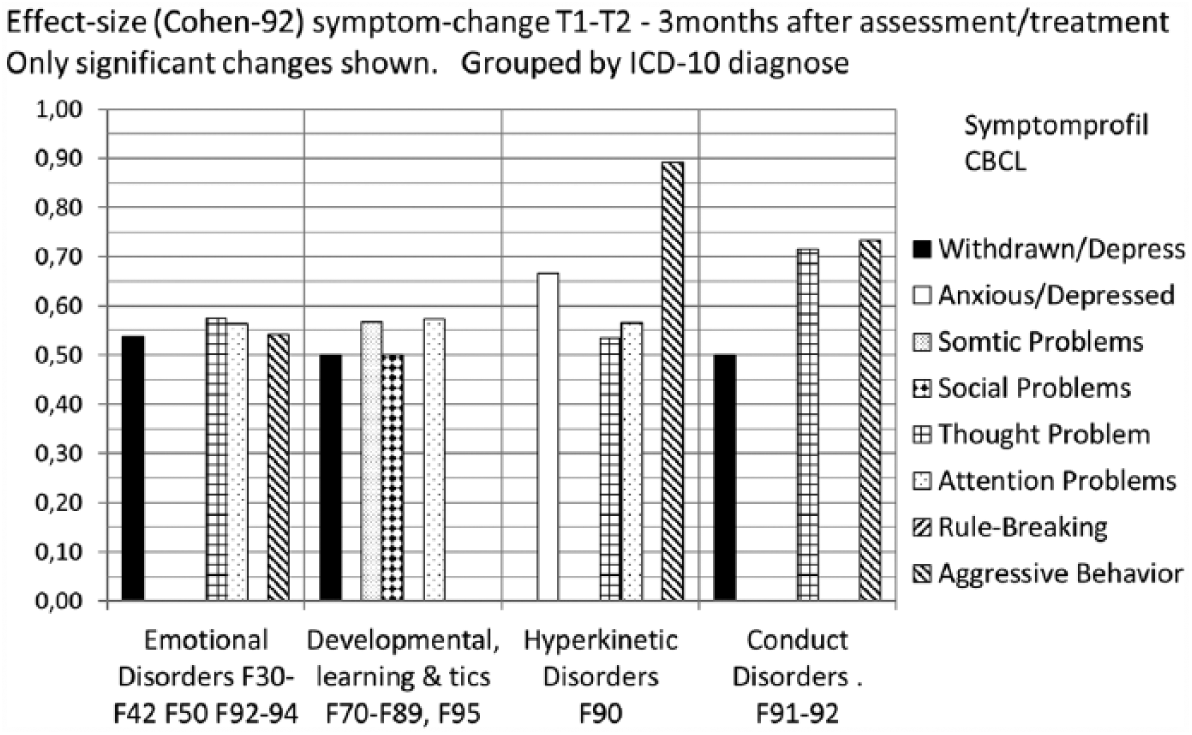
Effect size (Cohen’s d) of child symptom change on CBCL problem scales T1-T2 (from admission into family units to 3-month follow-up). Cases grouped by nonexclusive ICD-10 diagnoses (comorbidity allowed). Only scales with T1-T2 change > 5 (T-scores) included.
Because of the heterogeneity of symptoms between children, the maximal T1 scale and the scale with individually maximal T1–T2 change were selected for analysis (including all participants in the analysis). The individual maximum scale at T1 showed an average improvement of ΔT1–2 = 5.9 T-points (F(1,48) = 20.26, p < .001), which is an effect size of d = 0.64, and the individual maximal-change scale showed an average decrease of ΔT1–2 = 14.66 T-points (F(1,48) = 108.43, p < .001), which is an effect size of d = 0.62. Only four children (8%) did not show any improvement (meaning an improvement of less than 5 T-points or an increased symptom level on all scales).
With respect to the demographic variable groups and those who dropped out from T2 toT3, there were no significant differences in T1 levels or T1–T2 changes, except for the gender difference for somatic problems (see Table 2).
The parental reduction in anxiety symptoms but not depressive symptoms was correlated with child CBCL symptom improvements for five of the eight scales, namely, child anxiety, depressiveness, social problems, and rule-breaking (r = .33–.36, p < .05 for each), and stronger for aggression (r = .47, p < .01). This was also the case for the maximal T1 scale improvement (r = .46, p < .01) and maximal-change scale improvement for each child (r = .39, p < .05). For more extensive descriptions and analyses of parental changes, see Rimehaug et al. (2012).
Discussion
The aim of this study was to examine changes in the symptom scales and profiles of children admitted with their families to 2–4 weeks of evaluation and treatment at CAMHS family units. The main challenge was handling the heterogeneity in individual problem symptoms and the heterogeneity in profile of change. This attempt is solved with three strategies: (1) selecting groups with the same diagnosis, (2) selecting an individual outcome variable based on the highest level before treatment, and (3) selecting individual outcome based on the variable with largest individual change.
During the waiting list period, descriptive data indicate stability rather than change. During the active period from admission to the 3-month follow-up, almost all CBCL problem scales showed statistically significant reductions except for rule-breaking behavior, and the improvements remained throughout the 12-month follow-up period. At least one symptom scale showed a clinically significant change (ΔT1–2 > 10) among the majority, showing that significant improvement was possible for these previously nonresponding children.
The average child symptom levels at T1 and T2 were in the high and low subclinical range between T = 60 and 70 with wide variability reflecting heterogeneity and high levels for many individuals. This was confirmed by individual top scale average at T1 with a distribution mainly in the clinical range above T = 70, indicating a clinically significant symptom level for most children.
Change depending on clinical diagnosis
The hypothesis that we would find different symptom change profiles related to clinical diagnosis was supported by finding statistically and clinically significant changes in partly different selections of symptom scales depending on clinical diagnosis. Some of these improvements showed average improvement from the subclinical range (T = 60–70) toward normal values (T = 50–60), whereas others moved from clinical (T > 70) to the subclinical range (see Table 2 and Figure 3).
Among children with emotional disorders, the average significant symptom changes on the withdrawn, thought, attention, and aggressive problems typically moved from subclinical toward normal levels, suggesting improvements in cognitive-behavioral stress symptoms rather than improvement in diagnosis-related emotional problems.
Among children with developmental disorders, social problems and attention problems improved from clinical toward subclinical levels (for girls, this included also somatic problems), whereas withdrawal symptoms improved within subclinical levels. This pattern indicated improved functioning and improved interactions with their surroundings, while the diagnosed developmental condition can be assumed to be permanent.
Children with hyperkinetic disorders showed an average improvement in aggressiveness and attention problems from clinical to subclinical levels, showing diagnosis-relevant reductions in conflicts with other people and improved in attention problems with a hyperkinetic disorder. This group also showed an improvement within subclinical levels of anxiousness and thought problems, suggesting less rumination and fewer negative daily life events.
Children with conduct disorders showed average improvement in aggressive behavior from clinical to subclinical levels, suggesting improved core symptoms of their diagnosis. They also showed an average improvement in withdrawal and thought problems close to normal levels, suggesting improved cognitive-emotional and social functioning.
In general, these previously nonresponding or unsatisfactorily treated children showed improvement in diagnosis-related symptoms and symptoms that may reflect secondary or comorbid problems or environmental stressors, such as family problems, bullying, relationship problems, and other combined risks.
Strengths and weaknesses
The main strength of this study is its success in recruiting families with nonresponding children and following most of them for 12 months. Another strength, the use of standardized instruments to measure child and parent symptoms, allowed the use of standardized scores implicitly comparing to community reference values. However, using US norms in the scoring of CBCL may lead to the underestimation of the severity of the child problems since Norwegian parents are known to report lower child symptom levels on the CBCL than parents in most other countries (Achenbach & Rescorla, 2007).
This clinical sample was highly selected through years of service decisions prior to admission to the family units. Thus, these parents are not representative of parents with children treated at psychiatric clinics in general, but they may represent important aspects of unsuccessfully treated cases. Such cases are routinely encountered in clinics but are very rarely the focus of research, except as nonresponders to specific treatments.
The group mean results may conceal subgroup variation and individual patterns that the present design and analytic strategy could not detect.
The use of clinical diagnoses limits the reliability of classification. The small size of some diagnostic groups is a consequence of the naturalistic design and impedes some statistical comparisons. The low numbers of conduct disorders, the high comorbidity, and the unbalanced size of the diagnostic groups complicated the comparison between them. We attempted to compensate for this by describing changes in standardized T-scores as an expression of the effect size of the improvements. Using this double comparison, we also allowed the use of one-sided significance tests in the repeated-measures ANOVAs, testing only the hypothesis of improvement or not, which is clinically meaningful.
The heterogeneity of the clinical program, with few common or standardized elements and considerable flexibility related to the problems of each family and child, also limits the possibility of drawing firm conclusions regarding what caused the improvements.
Implications
Interpretations and implications must be discussed with caution from this naturalistic study. However, lasting clinical improvements among children with chronic problems and unsatisfactory responses to previous interventions seem possible. These children and their families are less eligible for standard treatment programs intended for relatively well-delimited conditions because of comorbidity between child disorders as well as family problems and problems with private and professional surroundings. They probably require a wider range of treatment components, including diagnostic re-evaluation and family interventions, ideally including the social network, school, and local community in the interventions. Specific treatment components should be manualized and tested for effectiveness. There is also a reason to believe that it can be helpful to bring together clinicians, parents, teachers, and children to develop a better understanding of each child’s experiences and functioning.
Footnotes
Acknowledgements
The authors wish to thank the participating clinics in the Nord-Trøndelag Health Trust and the Bergen Health Trust for valuable assistance in inviting participants and completing data collection. The author alone is responsible for the content and writing of the article. Trial registration: ![]() NCT00184327.
NCT00184327.
Availability of data and materials
The datasets collected and analyzed during this study are available on request from the corresponding author.
Ethical consideration
Ethical approval of the study was obtained from the Regional Committee for Medical Research Ethics in Central Norway. Written parental consent to participate was obtained by clinicians after distribution of written information and invitation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.