
Abstract

Acute pulmonary embolism (PE) is among the leading causes of cardiovascular-related death.1,2 PEs often occur in patients with complex medical histories, significant comorbidities, or concomitant acute illness. 3 Identifying the primary cause of death in this population can be difficult. Furthermore, PE-related mortality is not well defined in the literature,4,5 which limits the ability to assess PE-associated outcomes in both observational and clinical trials. Death indices, which rely on death certificates to ascertain cause of death, serve as a primary source of mortality outcomes in many epidemiological studies and are subject to error. 6 Previous studies have shown that cause of death recorded on death certificates often differs from documentation in the medical record, but this has not been assessed in the PE population.7,8 It is critical that appropriate causes of death be reported on death certificates to ensure accuracy of epidemiologic studies. Inaccuracies in death certificates also make disease-related outcomes prone to bias, and potentially misleading. We hypothesized that inaccuracies may be amplified among those diagnosed with PE, a population with numerous risk factors for mortality. We compared the cause of death as documented on the death certificate with cause of death ascertained by expert adjudication of medical records for patients hospitalized with acute PE who died during the hospitalization.
We included patients admitted to a tertiary care hospital with an acute PE diagnosis between August 1, 2012 and July 1, 2018. A retrospective chart review was performed to identify patient demographics, comorbidities, treatment, and outcomes. Cause of death was adjudicated by three independent physicians (WE, SM). A fourth expert, (BC), reviewed cases to identify cause of death if a majority was not met by the original three independent physicians. Two physicians (WE, MK) independently compared the adjudicated cause of death with that documented on death certificates. If there was discordance between the independent reviewers, the two physicians (WE, MK) reached a consensus. PE-related death was defined as death due to cardiogenic or obstructive shock, respiratory failure without infection, or an alternative underlying pulmonary process. This study was approved by the Beth Israel Deaconess Medical Center Institutional Review Board.
Of 2052 patients admitted with acute PE during the study period, 53.1% were women, 65.5% were White, and the average age was 63.1 ± 16.3 years. A total of 130 patients (6.3%) died before discharge. Of all deaths, the rate of PE-related mortality by death certificate (25/130, 19.2%) was similar to that determined by medical chart adjudication (29/130, 22.3%). However, there was significant disagreement among primary cause of death between the two sources. Only 28.0% (7/25) of PE-related deaths cited on death certificates were consistent in identifying cause of death when compared with chart adjudication (Figure 1A). Overall, 64.6% (84/130) of PE and non-PE chart-adjudicated causes of death disagreed with that listed on the corresponding death certificate. In 20.0% (26/130) of cases, the adjudicated cause of death by chart review was not mentioned as the primary cause of death on the corresponding death certificate. Death certificates cited pulmonary causes (42/130, 32.3%), PE (25/130, 19.2%), and cancer (15/130, 11.5%) as the three most common causes of death among the study cohort, whereas chart-associated adjudication determined that cancer (41/130, 31.5%), PE (29/130, 22.3%), and infection (23/130, 17.6%) were the three most common causes of death (Figure 1B). Only 6.9% (9/130) of patients had a pulmonary cause of death and less than 1% (1/130) of patients died owing to a myocardial infarction.
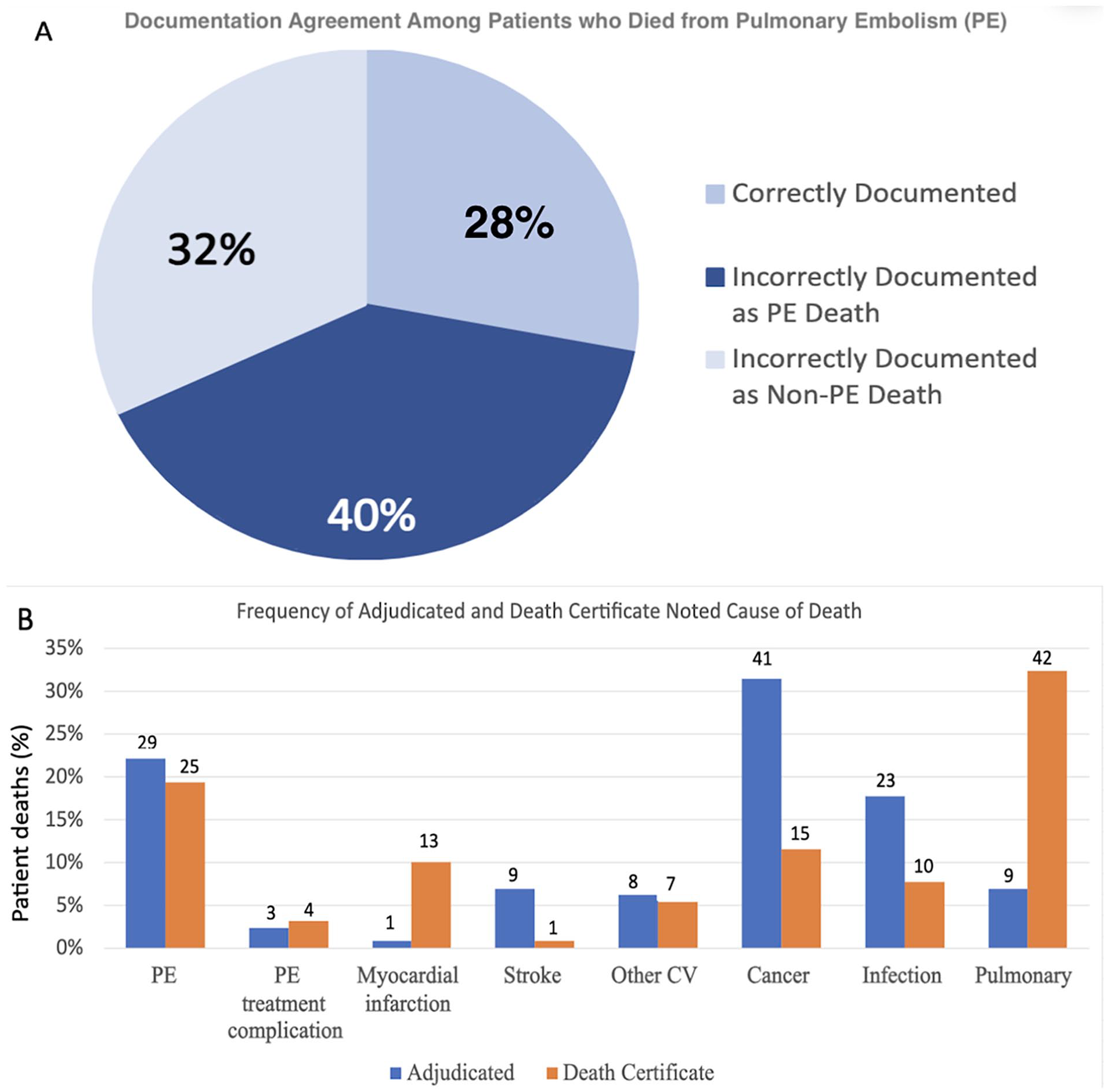
Accuracy of death certificate documentation based on adjudicated cause of death.
Among patients with acute PE, there was substantial disagreement between death certificate and adjudicated cause of death. This disagreement was evident both in patients diagnosed with acute PEs and in those who were determined to have expired directly from acute PE by chart adjudication. These low agreement rates underscore the inaccuracies of death certificate-ascertained cause of death. Furthermore, pulmonary causes and myocardial infarction were significantly over-reported on death certificates, whereas stroke, infection, and cancer were underreported. Although the cause of this discrepancy is unclear, this may be secondary to bias from subacute or chronic medical illnesses being overlooked as the primary source of death.
This study adds to a growing body of literature documenting the inaccuracies of death certificates for determining cause of death.9,10 There are likely several reasons for the errors in cause of death reporting. The lack of a definition for PE-related death in the literature prevents clinicians from taking a systematic approach to postmortem documentation. Furthermore, cause of death evaluation is often not emphasized in medical training, resulting in trainees or other medical team members completing documentation that is inconsistent with the patient’s clinical course. An over-reliance on death certificates to identify PE-related mortality could introduce bias into epidemiologic and comparative outcomes research. Completing accurate death certificate documentation is crucial to understanding mortality trends in the PE population. This lack of consistency in death reporting underscores the importance of establishing clear criteria for PE-related death. Provider education on appropriate death certificate completion may improve death certificate accuracy. Further quality improvement studies are needed to assess strategies to improve cause of death reporting and documentation.
Footnotes
Acknowledgements
This study was presented at the Society for Vascular Medicine’s Vascular Scientific Sessions in Washington, DC (September 2023).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Eric Secemsky reports grants (to institituion) from Abbott/CSI, BD, Boston Scientific, Cook, Medtronic, and Philips; and speaking/consulting fees from Abbott/CSI, BD, BMS, Boston Scientific, Cagent, Conavi, Cook, Cordis, Endovascular Engineering, Gore, InfraRedx, Medtronic, Philips, RapidAI, Shockwave, Terumo, Thrombolex, VentureMed, and ZOLL. The remaining authors have no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.