
Abstract
Hypertension is a leading risk factor for morbidity and mortality worldwide. Accurate measurement of office blood pressure (BP) is critical to diagnosis and determining the efficacy of therapy. Current guidelines recommend more than one in-office BP measurement to improve accuracy. 1 Multiple office BP readings result in lower averaged BP, better correlation with ambulatory BP, and improved cardiovascular risk prediction.2,3 This is thought to be due to higher initial BP from the alerting reaction and a partial contribution of regression to the mean with subsequent measurements.3, 4 However, features that contribute to changes in BP with additional in-office measurements remain unclear. We studied primary care clinic patients with an initial elevated BP to determine predictors of BP changes with a second measurement.
Institutional Review Board approval was obtained through Vanderbilt University Medical Center (VUMC) including a waived requirement for written informed consent. Over 11 weeks at 16 VUMC primary care clinics, quality initiative clinic personnel were asked to take a second consecutive BP measurement in patients with an initial systolic BP > 140 mmHg or diastolic BP > 90 mmHg. BP measurement was performed with Welch Allyn (Skaneateles Falls, NY) wall-mounted auscultatory or Phillips SureSign (Cambridge, MA) oscillometric devices. Medical histories and demographic data were obtained from the medical record, and laboratory values within 90 days of the BP measurement were included.
Of 2272 patient encounters for which the initial BP was > 140 mmHg systolic or > 90 mmHg diastolic, and a second BP measurement was obtained, 714 encounters were excluded for no laboratory data being available within 90 days, three encounters were excluded due to no body mass index data, and two for heart rate < 10 beats per minute, which was deemed artifactual. This left 1553 patient encounters for analysis. Two group comparisons were performed with the Mann–Whitney test. Multivariable linear regression was used to determine predictors of systolic BP changes while controlling for covariates. Statistical testing was performed using GraphPad Prism version 9.3.1 (GraphPad Software, Boston, MA).
Demographic data for participants are shown in online Supplemental Table 1. In these individuals with elevated BP, a second BP measurement resulted in a 6.2 mmHg lower systolic (p < 0.0001; Mann–Whitney) and 3.0 mmHg lower diastolic BP (p < 0.0001; Mann–Whitney) (online Supplemental Table 1). There were no significant differences in the change between the first and second measurement based on whether BP was measured via auscultatory or oscillometric methods (systolic mean ± SEM: −6.7 ± 11.7 vs −5.9 ± 10.5, respectively, p = 0.19; diastolic: −3.3 ± 9.0 vs −2.8 ± 8.9, p = 0.62). Multivariable linear regression revealed features associated with decreased systolic BP with a second measurement including a higher first BP reading, younger age, male sex, and Asian race (Table 1). Of note, there were no significant associations with method of BP measurement, use of particular antihypertensive therapies, or heart rate (Table 1).
Multivariable linear regression of predictors of the change in systolic blood pressure from the first to second readings.
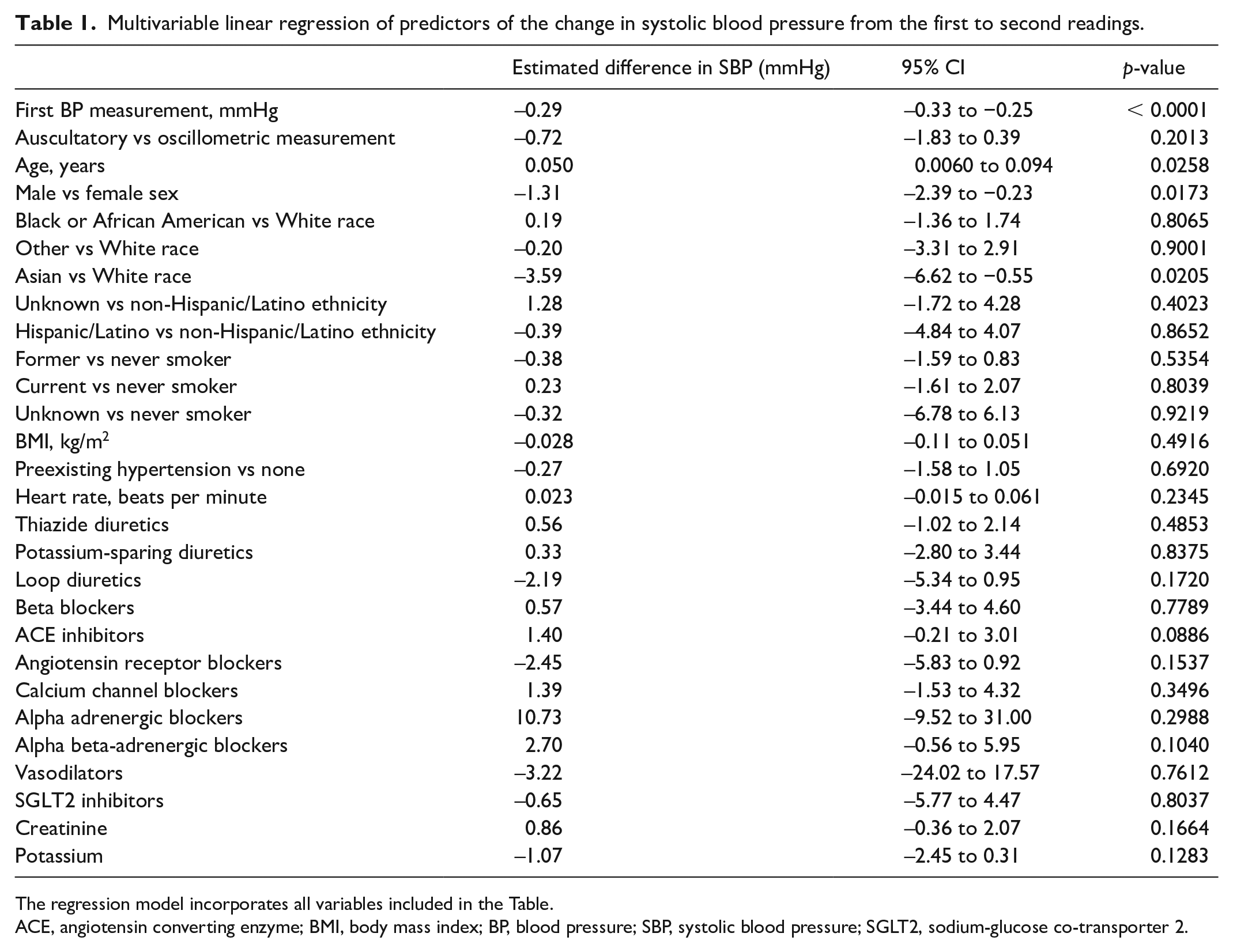
The regression model incorporates all variables included in the Table.
ACE, angiotensin converting enzyme; BMI, body mass index; BP, blood pressure; SBP, systolic blood pressure; SGLT2, sodium-glucose co-transporter 2.
Although guidelines recommend more than one in-office BP measurement for hypertension diagnosis or treatment decisions, real-world logistical challenges have kept this from being performed uniformly.1,3,5 We found a lower systolic and diastolic BP with a second reading, consistent with prior studies.3,4 We also present novel evidence that higher initial BP, male sex, younger age, and Asian race are predictors of BP decreases with a second measurement in individuals with elevated first readings. Higher initial BP resulting in a greater decrease with a second reading is consistent with a prior retrospective study 3 and likely reflects increased sympathetic outflow as part of the alerting reaction that raises the initial BP which declines with subsequent measurements. 4 The alerting reaction is a psychological stress reaction to the initial BP measurement with associated increased sympathetic outflow. 6 Our finding that male sex is associated with a greater BP decrease with repeat measurements is also consistent with this, given that men exhibit increased sympathetic nervous system activity compared to women.7,8 The association of younger age with larger systolic BP decreases on second measurement also likely reflects a greater contribution of sympathetic outflow in young individuals that is overcome by increased arterial stiffness with older age. 9 Although baseline heart rate did not predict changes in systolic or diastolic BP, additional studies of heart rate variability or muscle sympathetic nerve activity will be required to determine the direct association of sympathetic outflow with initial and subsequent BPs. Importantly, the association of these demographic features would not be expected if BP reductions were simply a function of regression to the mean, suggesting that physiological factors contribute to this observation. Finally, there was no difference in the change in BP from the first to the second readings with auscultatory or oscillometric devices, indicating that clinics implementing ascertainment of two BP measurements would expect to observe the same decreases in BP using either type of device.
A prior study identified a lower proportion of African Americans with decreased BP on additional measurements compared to sustained hypertensives. 4 We did not observe this relationship, though our study population consisted of a limited number of African American participants. We did observe a novel association of Asian race with BP decreases on subsequent readings. This warrants further investigation including in cohorts with greater representation of Asian race, particularly given the increased hypertension and cardiovascular disease risk among those of South Asian ancestry. 10
Limitations of our study include that only patients with an initial BP > 140/90 mmHg were included, so further studies will be needed to determine if findings are similar in those with initial normotensive BPs. In addition, our analysis does not include comparison to out of office BP readings, which are also recommended for hypertension diagnosis and to guide treatment decisions. 1 Finally, there was not a defined period of rest before obtaining the first BP measurement, so there could be a contribution to the reduction in BP with the second measurement from additional time for rest.
Overall, our analysis confirms prior findings that obtaining a second BP measurement results in a lower average BP reading.3,4 In addition, certain features such as younger age, male sex, Asian race, and higher elevated first BP reading predict decreases with a second reading, which are consistent with an excessive alerting response. Our findings also suggest that certain populations may derive particular benefit from a second measurement, including younger men, Asian individuals, and those with a more elevated first BP reading which can help avoid inappropriate hypertension diagnoses and/or over-treatment.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X241257140 – Supplemental material for Predictors of blood pressure reductions with a second measurement in individuals with uncontrolled blood pressure in primary care clinics
Supplemental material, sj-docx-1-vmj-10.1177_1358863X241257140 for Predictors of blood pressure reductions with a second measurement in individuals with uncontrolled blood pressure in primary care clinics by Matthew R Alexander, Neeraja B Peterson, Suman Kundu, Eric Farber-Eger, Wanpen Vongpatanasin, Matthew S Freiberg, Quinn S Wells, Phillip A Cook and Joshua A Beckman in Vascular Medicine
Footnotes
Declaration of Conflicting of Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joshua Beckman reports consulting for JanONE, Janssen, and Novartis; and ownership in Janacare. The other authors have no conflicts of interest.
Funding
This work was supported by the National Institutes of Health (K08HL153786-01 to Matthew Alexander and HL131977 to Joshua Beckman and R33AG068486 to Wanpen Vongpatanasin).
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.