
Abstract
Objectives
To elucidate the clinical significance of differences between home- and clinic-measured systolic blood pressure (SBP) in patients with treated hypertension, and to assess the correlations between SBPs and arterial stiffness.
Methods
Patients with treated hypertension measured their blood pressure (BP) themselves once, at home, in the morning (<1 h after awakening) using an automated oscillometric sphygmomanometer. Clinic BP was measured once, at an outpatient clinic on the same day, using a similar instrument. Arterial stiffness was measured by cardio–ankle vascular index (CAVI). Differences between home and clinic SBPs, and the correlations between CAVI and home SBP, clinic SBP, and the difference between home and clinic SBPs, were analysed.
Results
Seventy-six patients with treated hypertension (mean age, 71 years) were evaluated. There was no statistically significant difference between home and clinic SBP (mean ± SD 132 ± 14 and 133 ± 16 mmHg, respectively). Home SBP showed no correlation with CAVI, whereas clinic SBP showed a weak correlation. The difference between the home and clinic SBP showed a stronger correlation with CAVI, and was statistically significant.
Conclusions
The difference between home- and clinic-measured SBP showed a better correlation with arterial stiffness than did either home or clinic SBP alone.
Keywords
Introduction
It is well known that hypertension is a risk factor for cardiovascular events including stroke, ischaemic heart disease and heart failure.1–3 The clinical studies producing these results have, however, been performed using clinic blood pressure (BP) as the only measure of BP. 4 There is increasing evidence regarding the usefulness of BP measurements conducted at home, by patients themselves.5,6 Average values of home BP measurement are generally stable; therefore, reproducibility of home BP measurements is considered to be good. 7 Home BP measurement is useful for assessing the effectiveness of antihypertensive drugs. 8 Patients with hypertension who exhibit a discrepancy between home and clinic BP measurement are described as having either “masked” hypertension, if home BP is higher, 9 or “white coat” hypertension, if home BP is lower. 10 It is supposed that patients with “masked” or “white coat” hypertension are at heightened risk of cardiovascular events.11–13 Thus, both clinic and home BP measurements are important markers for BP control, in clinical settings.
Arterial stiffness is an index for assessing atherosclerosis, and is also an independent predictor of cardiovascular events (including fatal and nonfatal coronary events) and fatal strokes in hypertensive patients.14,15 The cardio–ankle vascular index (CAVI) is an index of arterial stiffness 16 that has been used for assessing such stiffness in the clinical setting. 17
The present study evaluated the differences between single, same-day, home and clinic systolic BP (SBP) measurements in patients with treated hypertension. The study also assessed the correlation between arterial stiffness measured by CAVI and home SBP and clinic SBP, and also assessed the difference between the two SBPs.
Patients and methods
Study population
Consecutive patients who had been diagnosed with hypertension (defined as SBP ≥140 mmHg and/or diastolic BP (DBP) ≥90 mmHg) who attended a regular hypertension clinic at Kagawa University Hospital, Kagawa, Japan, were enrolled into the study. The diagnosis of hypertension was based on one BP reading within 1 year of study entry. This study was conducted between January 2012 and December 2012. All patients were treated with at least one antihypertensive drug. The dose of antihypertensive therapy was stable and changes to therapy were not allowed within 3 months prior to study entry. Patients with a history of heart failure, stroke or obvious heart disease were excluded.The protocol was approved by the Ethics Committee of Kagawa University. Written informed consent was obtained from all participants.
BP measurement
Participants were asked to measure their home BP once, in the morning (<1 h after awakening and before taking any antihypertensive drug) on the same day they were due to visit the outpatient clinic. They measured their BP in the upper right arm, in the sitting position, using their own automated oscillometric sphygmomanometers and without a human observer. Patients were not specifically trained by study staff to use the sphygmomanometers, but they were asked to follow the instruction manuals. Because patients were using their own sphygmomanometers there was no standardization in the equipment used and it was unknown whether their equipment was properly calibrated. The results were recorded manually by the patients. The patients were asked to record systolic and diastolic BP readings in the morning (<1 h after awakening and before taking any antihypertensive drug) every day, in booklets provided by the investigators.
Patients attended the outpatient clinic visit on the morning of the same day as they recorded their home SBP, for measurement of their SBP in a clinical setting. There was no set limit to the time between the home and clinic SBP measurements, and patients were not instructed as to whether or not they could take their hypertension medication before or after the clinic visit.
When participants arrived at the outpatient clinic, they rested for ≥1 min before their SBP was measured. Clinic SBP was measured once, while the patient was in the sitting position, by a physician trained in using the automated oscillometric sphygmomanometer (HEM-1040, Omron, Kyoto, Japan).
Both home and clinic SBP measurements for each patient were based on a single reading. There was no protocol in the case of aberrant readings. Differences between the single home and clinic SBP readings for each patient were calculated. These SBP measurements were performed within 3 months before or after the day when the CAVI measurements or blood examinations (see below) were performed.
Assessment of arterial stiffness by CAVI
The CAVI was measured using an automatic vascular screening system (VaSera™ VS-1000; Fukuda Densi, Tokyo, Japan), with the patient resting in a supine position. Pulse wave velocity (PWV) was obtained by dividing the vascular length by the time it took for the pulse wave to propagate from the aortic valve to the ankle. SBP and DBP were measured at the brachial artery. The formula used to calculate CAVI was as follows: CAVI = a[(2ρ/ΔP) × ln (SBP/DBP) PWV 2 ] + b, where ΔP is SBP – DBP, ρ is blood density, and a and b are scale conversion constants to match aortic PWV. The principle underlying the CAVI has been described previously. 16 The CAVI reflects the stiffness of the aorta, femoral artery and tibial artery as a whole; theoretically, it is not affected by BP. All these measurements and calculations were performed on the VaSera™ VS-1000. For each patient, electrocardiogram electrodes were placed on both wrists, a microphone for detecting heart sounds was placed on the sternum, and cuffs were wrapped around both arms and both ankles. After automatic measurements, the values of right and left CAVI were calculated. The mean values of the right and left CAVI scores were used for analysis.
Blood sample collection
Blood samples were taken in the morning after an 8-h overnight fast. Blood was collected into tubes containing 1.8 mg/ml ethylenediamine tetra-acetic acid and was analysed immediately. Serum total cholesterol, triglyceride, high-density lipoprotein cholesterol (HDL-C), glycosylated haemoglobin (HbA1c), and uric acid concentrations were measured by standard laboratory techniques. Relationships between laboratory data, BP parameters and other clinical characteristics, including CAVI, were analysed.
Statistical analyses
Statistical analyses were performed using the SPSS® statistical software package, version 18.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Data were expressed as the mean ± SD. A paired t-test was used to compare the single home and clinic SBP measurements. Correlations between SBP parameters and other variables were assessed by univariate linear regression analyses. Values of P < 0.05 were considered to be statistically significant.
Results
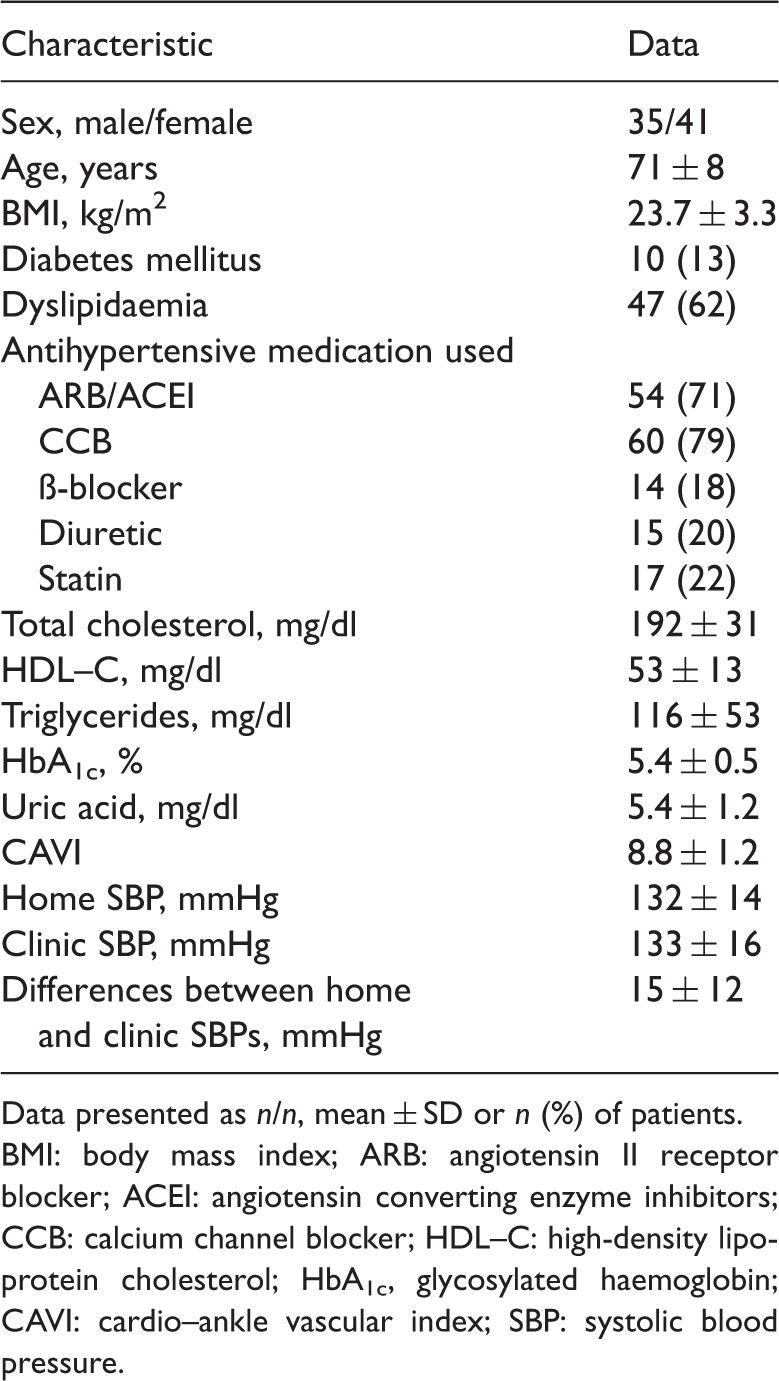
A total of 76 patients (35 males, 41 females; mean ± SD age 71 ± 8 years [range 53–88 years]) were included in the study. Clinical and demographic characteristics of the patients are presented in Table 1. The high mean value of CAVI indicated the presence of arterial stiffness in the patient group as a whole. The mean values of home and clinic SBP were not particularly high: in all patients, hypertension was being appropriately controlled by medication. Figure 1 shows the differences between same-day home and clinic SBP measurements. Compared with home SBP, the clinic SBP increased in 40 (53%) patients but decreased in 36 (47%) patients, and there was no significant overall difference between the mean home and clinic SBPs. The mean of the individual differences between the two measurements was 15 ± 12 mmHg.
Difference between same-day home- and clinic-measured systolic blood pressure (SBP) readings in patients with treated hypertension (n = 76). There was no significant overall difference between the mean ± SD SBP measured at home (132 ± 14 mmHg) and in the clinic (133 ± 16 mmHg); one measurement per location. Central black horizontal lines show the mean values for each timepoint; extremities of vertical lines show the SD. Clinical and demographic characteristics of patients with treated hypertension (n = 76), included in a study examining the clinical significance of differences between single, same-day, home- and clinic-measured systolic blood pressure readings. Data presented as n/n, mean ± SD or n (%) of patients. BMI: body mass index; ARB: angiotensin II receptor blocker; ACEI: angiotensin converting enzyme inhibitors; CCB: calcium channel blocker; HDL–C: high-density lipoprotein cholesterol; HbA1c, glycosylated haemoglobin; CAVI: cardio–ankle vascular index; SBP: systolic blood pressure.
Home-measured SBP did not show a significant correlation with age, whereas clinic-measured SBP showed a weak correlation with age (r = 0.297, P = 0.009), and the difference between the home and clinic SBP showed the strongest correlation with age (r = 0.486, P < 0.001) (Table 2). Similarly, home-measured SBP showed no correlation with CAVI, but clinic-measured SBP showed a weak correlation with CAVI (r = 0.316, P = 0.005), and the difference between home and clinic SBP showed the strongest correlation with CAVI (r = 0.600, P < 0.001) (Figure 2; Table 2). There was also a significant correlation between BMI and home-measured SBP (P = 0.010), and between uric acid and the difference between the home and clinic SBPs (P = 0.037) (Table 2).
Relationships between cardio–ankle vascular index (CAVI) and (a) home systolic blood pressure (SBP), (b) clinic SBP, and (c) the difference between home and clinic SBPs, measured during a single day in patients with treated hypertension (n = 76). The home SBP measurements showed no correlation with CAVI (r = 0.105, P ≥ 0.05), but clinic SBP showed a weak correlation with CAVI (r = 0.316, P = 0.005). The difference between home and clinic SBPs showed the best correlation with CAVI (r = 0.600, P < 0.001). Linear regression analyses of the relationships between home systolic blood pressure (SBP), clinic SBP and the difference between home and clinic SBP (measured once on a single day), with other clinical characteristics, in patients with treated hypertension (n = 76). Univariate linear regression analyses. BMI: body mass index; ARB: angiotensin II receptor blocker; ACEI: angiotensin converting enzyme inhibitors; CCB: calcium channel blocker; HDL–C: high-density lipoprotein cholesterol; HbA1c, glycosylated haemoglobin; CAVI: cardio–ankle vascular index; SBP: systolic blood pressure; NS: not statistically significant (P ≥ 0.05).

Discussion
The present study evaluated the clinical significance, in patients being treated for hypertension, of the difference between single home and clinic SBP measurements. These measurements were taken on the same day (by the patient and physician, respectively), and the clinical significance was evaluated by analysing the correlation between differences in BP and arterial stiffness, as assessed by CAVI. The study demonstrated the following: (i) that there was a high degree of variability in home and clinic SBP measurement, with values measured at the outpatient clinic showing an increase in 53% of patients and a decrease in 47% of patients, compared with values taken at home on the same morning; (ii) there was no significant mean difference between individual home and clinic SBP measurements; (iii) same-day home and clinic SBPs showed no or weak correlations with arterial stiffness, assessed by CAVI, while the difference between home and clinic SBPs showed a stronger correlation with arterial stiffness. The finding that, in approximately one half of the patients, the clinic SBP measurements were higher than the home SBP measurements, while in the other half the reverse was true, may indicate that the study included some patients who were prone to the ‘white-coat effect' and some who had ‘masked hypertension'. As the study only took a single home and clinic measurement from each patient, however, the likelihood of natural variability in BP readings cannot be ruled out.
The main purpose of the present study was to evaluate whether there was any clinical significance in the calculated difference between home and clinic SBPs. Compared with either measurement alone, the difference between home and clinic SBPs showed a stronger correlation with arterial stiffness, as estimated by CAVI. In addition, correlations between atherosclerosis-related factors (namely, BMI and uric acid levels) and the home SBP measurement, and the difference between home and clinic SBPs, respectively, were observed. Studies have demonstrated associations between systemic atherosclerotic change and 24-h18,19 or visit-to-visit 20 BP variability. There are, however, few data about the relationship between atherosclerosis and same-day SBP differences between home and clinic SBPs. It is possible that patients with a large variation between home and clinic SBP measurement are at heightened risk of developing atherosclerosis. Recently, visit-to-visit variability in SBP has been shown to be a predictor of stroke.21,22 Thus, we consider that clinical examination and care for atherosclerosis-related diseases may be needed in patients who show a large variation between home and clinic SBPs. In addition, and perhaps a greater level of attention should be paid to the magnitude of differences between home and clinic SBPs, rather than the absolute values of each measurement.
Age is an important risk factor in atherosclerosis,23,24 and CAVI is a parameter of arterial stiffness that reflects one important factor of atherosclerosis. It is well known that the CAVI increases with advancing age,16,17 and that increased BP variability is a characteristic of elderly patients with hypertension.25,26 This may explain the correlation we observed between the difference between the home and clinic SBP, and both age and CAVI.
There were several limitations to the present study. First, participants measured their home BP using their own equipment, which was different compared with the equipment used in to measure the clinic BP. In addition, there was very likely to be a high degree of inter-individual variability in the make and model of equipment used for home BP measurements. Also, there was no way of knowing if the patient’s own equipment had been properly calibrated. Therefore, potential variations between home and clinic SBP measurements due to lack of standardization cannot be ruled out. Secondly, only one BP measurement was taken in each setting (home and clinic) for each patient. Consequently, the calculated difference between the home and clinic values could be due to natural daily variations in BP rather than any clinically significant effect. Thirdly, neither atherosclerosis nor its progression was actively assessed in the present study. Finally, there was no specification to the patient as to whether they could take their prescribed hypertension medicine before or after the clinic visit. Thus, the timing of antihypertensive drug administration in the morning may have influenced the clinic BP reading. These limitations regarding the methodology may have affected the results of this study. Larger studies that take an average of multiple measurements of patients’ SBP both at home and in the clinic, on a single day and over time, should be carried out to verify the clinical significance of the findings of this study.
In conclusion, the difference between single home and clinic SBP measurements, in patients with treated hypertension, showed better correlation with arterial stiffness than did either the specific home or clinic SBP measurement itself.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported in part by a Grant-in-Aid (Scientific Research [B]) No. 23300190 to S.S.) for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology, Japan and Japan Society for the Promotion of Science (JSPS).