
Abstract
Erectile dysfunction (ED) is associated with cardiovascular disease (CVD) and CVD mortality. However, the relationship between ED and subclinical CVD is less clear. We synthesized the available data on the association of ED and measures of subclinical CVD. We searched multiple databases for published literature on studies examining the association of ED and measures of subclinical CVD across four domains: endothelial dysfunction measured by flow-mediated dilation (FMD), carotid intima–media thickness (cIMT), coronary artery calcification (CAC), and other measures of vascular function such as the ankle–brachial index, toe–brachial index, and pulse wave velocity. We conducted random effects meta-analysis and meta-regression on studies that examined an ED relationship with FMD (15 studies; 2025 participants) and cIMT (12 studies; 1264 participants). ED was associated with a 2.64 percentage-point reduction in FMD compared to those without ED (95% CI: –3.12, −2.15). Persons with ED also had a 0.09-mm (95% CI: 0.06, 0.12) higher cIMT than those without ED. In subgroup meta-analyses, the mean age of the study population, study quality, ED assessment questionnaire (IIEF-5 or IIEF-15), or the publication date did not significantly affect the relationship between ED and cIMT or between ED and FMD. The results for the association of ED and CAC were inconclusive. In conclusion, this study confirms an association between ED and subclinical CVD and may shed additional light on the shared mechanisms between ED and CVD, underscoring the importance of aggressive CVD risk assessment and management in persons with ED.
Keywords
Introduction
Despite concerted preventive efforts, cardiovascular disease (CVD) continues to be the leading cause of mortality globally. 1 Sixty-six percent of these deaths can be attributed to atherosclerotic CVD (ischemic heart disease, ischemic stroke, and peripheral vascular disease).1,2 As a response to the significant burden of CVD, there has been increased focus on traditional CVD risk factor identification and risk stratification, with the hope of identifying persons that are most likely to benefit from prevention therapy.
Subclinical CVD independently predicts CVD events, and its absence is associated with minimal CVD risk, even in the presence of other traditional risk factors.3–8 Thus, subclinical CVD assessment is often used as an adjunct to traditional CVD risk stratification. Several non-invasive methods of assessing subclinical CVD have been developed, with the most popular being the coronary artery calcium (CAC) score, 9 a marker of coronary atherosclerosis, and carotid intima–media thickness (cIMT), a marker of the arteriosclerosis and atherosclerosis of the carotid arteries. 10 Markers of endothelial function, such as brachial artery flow-mediated dilation (FMD) and the reactive hyperemia index (RHI),11,12 as well as other markers of vascular function, are also used to assess subclinical CVD in research settings. 13 Erectile dysfunction (ED) is a common disorder with an overall prevalence of around 18% in men aged 20 or more years. 14 The proportion of ED by cause has not been well described in the literature. However, a small series with 69 participants indicated that a vascular disorder (evaluated by penile color Doppler ultrasound) was associated with ED in about 34% of non-hypogonadal, non-neuropsychiatric patients. 15 In multiple studies including systematic reviews, ED has been shown to be associated with an increased risk of CVD.16–18
ED and subclinical CVD have similar risk factors (age, obesity, smoking), 19 and it is thought that both conditions have shared mechanisms. However, the relationship between ED and subclinical CVD is not as clear as that for established CVD as the studies examining this association are limited by less than ideal sample sizes, and have had conflicting results. Particularly, it is unknown which markers of subclinical CVD have the greatest or most consistent association with ED.
Delineating a consistent, strong association of ED with subclinical CVD will help in establishing ED as a simple and effective marker of underlying subclinical CVD. In such an instance, measures of ED could be a simple effective CVD risk stratification tool, particularly in young men who are less likely to undergo aggressive CVD risk assessment and management. This systematic review and meta-analysis is aimed at examining and synthesizing the current evidence describing the relationship between ED and measures of subclinical CVD with a view to highlighting the strength of the associations where possible and to identify gaps in knowledge for future research.
Methods
We systematically searched PubMed, Excerpta Medica Database (EMBASE), Web of Science, Cumulative Index to Nursing, Allied Health Literature (CINAHL), the Cochrane Library of Trials, and Scopus for published studies assessing the association of ED and markers of subclinical CVD between 1964 and 2016. As part of our search strategy, we divided vascular markers into four domains: endothelial function, carotid atherosclerosis, coronary atherosclerosis, and other markers of vascular function (ankle–brachial index (ABI), pulse wave velocity (PWV), and toe–brachial index (TBI)). In addition to ED, search terms were generated to represent each domain and include variations of the following: coronary artery calcification, carotid intima–media thickness, flow-mediated dilatation, brachial reactivity, reactive hyperemia index, ankle–brachial index, toe–brachial index, and pulse wave velocity. We excluded studies with non-standardized assessments of ED, those whose participants had known CVD, and studies without comparison groups for ED. We also excluded case reports and case-series, studies without full text and those whose full text were not in English. One reviewer conducted the search (BV) and two reviewers assessed studies for eligibility (BV and EA). Only studies that were agreed upon by both reviewers as meeting the specified eligibility criteria were included in the review.
Erectile dysfunction assessment
To be included in the review, the study had to have a standardized measurement of ED (a validated questionnaire or other clinically acceptable measure) and a subclinical marker of CVD in at least one of the earlier mentioned domains. ED and its severity are most frequently assessed using the International Index of Erectile Function questionnaires. The IIEF-15 is a 15-item questionnaire that assesses four domains of male sexual function. The IIEF-5 is an abridged version of the original 15-item questionnaire. Both of these questionnaires are validated, have a high degree of sensitivity and specificity for detecting ED, and are widely used in research studies.20,21
Description of outcome measures
Endothelial dysfunction is most commonly assessed by flow-mediated dilation (FMD) of the brachial artery. FMD, most often assessed in the brachial artery, is captured by ultrasonographic measure of changes in vessel diameter over a period of time (often 60 seconds) after deflation of a cuff placed around the vessel. These changes are measured as percentage difference from baseline. 11 The cIMT is measured by ultrasound assessment of either the common carotid artery or the internal carotid arteries, or both, 22 and is expressed in millimeters (mm). CAC is measured by a computed tomography (CT) scan assessment of the coronaries and algorithms are used to determine its standardized Agatston score. 9 PWV is a measure of arterial stiffness; the aortic PWV is more of a measure of central arterial stiffness while the brachial–ankle measures peripheral arterial stiffness. ABI and TBI, both measured by Doppler assessment of systolic pressures in the lower and upper extremities, are often used to determine peripheral artery disease and can be used as markers of subclinical CVD in persons who have no clinical symptoms of CVD. 23
Assessment of study quality
We formally assessed all studies for quality using the ‘Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies’ developed by the National Institutes of Health and freely available on the Internet. 24 This 14-item scoring tool was developed for longitudinal, cross-sectional and case–control studies (Supplementary Table 1). Each item was scored ‘1’ for ‘Yes’ or met criteria or ‘0’ for ‘No’ or did not meet criteria. For questions whose answers could not be deciphered from the published study, ‘UA’ (unable to assess) was given, while ‘N/A’ was given for questions that were not applicable (such as questions asking about loss to follow-up in studies that are cross-sectional or case–control). Two reviewers (CUO and EA) independently assessed quality for each study and disagreements on scoring were settled by discussion. A numeric score was assigned to each study based on the total number of items scored ‘1’. We decided that studies with scores of 10 or more were of high quality, those with 7–10 were intermediate quality, while those with less than 7 were deemed to be of lower quality. A summary of the assessment of included studies can be found in the Supplementary Table 2.
Meta-analysis
We decided a priori to conduct a meta-analysis if there were three or more studies with comparable outcomes. We considered outcomes comparable if the measures of subclinical CVD were the same, had similar categorizations if and where applicable, and had similar units of measurements. Only FMD and cIMT met these criteria. The data from each study included in the meta-analysis were manually extracted and copied into an Excel sheet. All statistical analyses were performed using the software package R (Version 3.1.1; R Foundation for Statistical Computing, Vienna, Austria). The R function metacont and metareg in package meta 25 was used for the meta-analysis of the continuous outcomes (i.e. FMD (measured as percentage change in brachial arterial dilation) and cIMT (measured in mm)). Inverse variance weighting was used for pooling, absolute mean differences (referred to as mean difference from on) were generated and the results from random effects models 26 are presented with their corresponding forest plots. Measures of heterogeneity (I2) and between study variance (τ2; tau-squared) are also reported. Owing to the presence of significant heterogeneity encountered with the meta-analysis, we sought to determine the source(s) of this heterogeneity. Therefore, subgroup meta-analyses were conducted to assess the influences of age, ED assessment type (short vs standard form of the IIEF), study publication date and study quality on the results of the meta-analysis. We also conducted a sensitivity analysis sequentially excluding the three studies that deviated the most from the absolute mean difference (and seen as outliers in the forest plot) in each meta-analysis. To assess for the risk of publication bias, a funnel plot of the studies was generated and a formal test of asymmetry, the weighted linear regression of the treatment effect on its standard error, 27 was conducted.
Results
Figure 1 describes the results of the search. A total of 28 studies met the criteria for inclusion in the review. Many of the included studies measured multiple subclinical CVD outcomes. In all, 15 studies examined endothelial dysfunction as an outcome, with all these measuring FMD and none measuring RHI.28–42 Twelve studies examined cIMT outcomes,28,34,35,38,40,42–48 five studies measured CAC28,29,37,49,50 and six studies had various measures of vascular stiffness and peripheral vascular disease such as PWV, Augmentation Index (AIx), ABI, and TBI.28,51–55 All the studies with FMD (n=15) and cIMT (n=12) outcomes were included in the meta-analysis regardless of their quality. None of the other outcome measures met our a priori meta-analysis criteria. Among the CAC studies, two compared continuous measures of CAC (mean and median) between ED groups, while the others were binary but had inconsistent cut-offs for abnormal CAC values. Among the other measures of vascular function, three studies measured ABI: two were continuous outcomes and one was binary. No other measure of vascular function was assessed in three or more studies. All studies included in this review were either case–control or cross-sectional studies; no longitudinal studies met the inclusion criteria. The description of the studies, grouped by their subclinical CVD outcomes, can be found in Table 1.
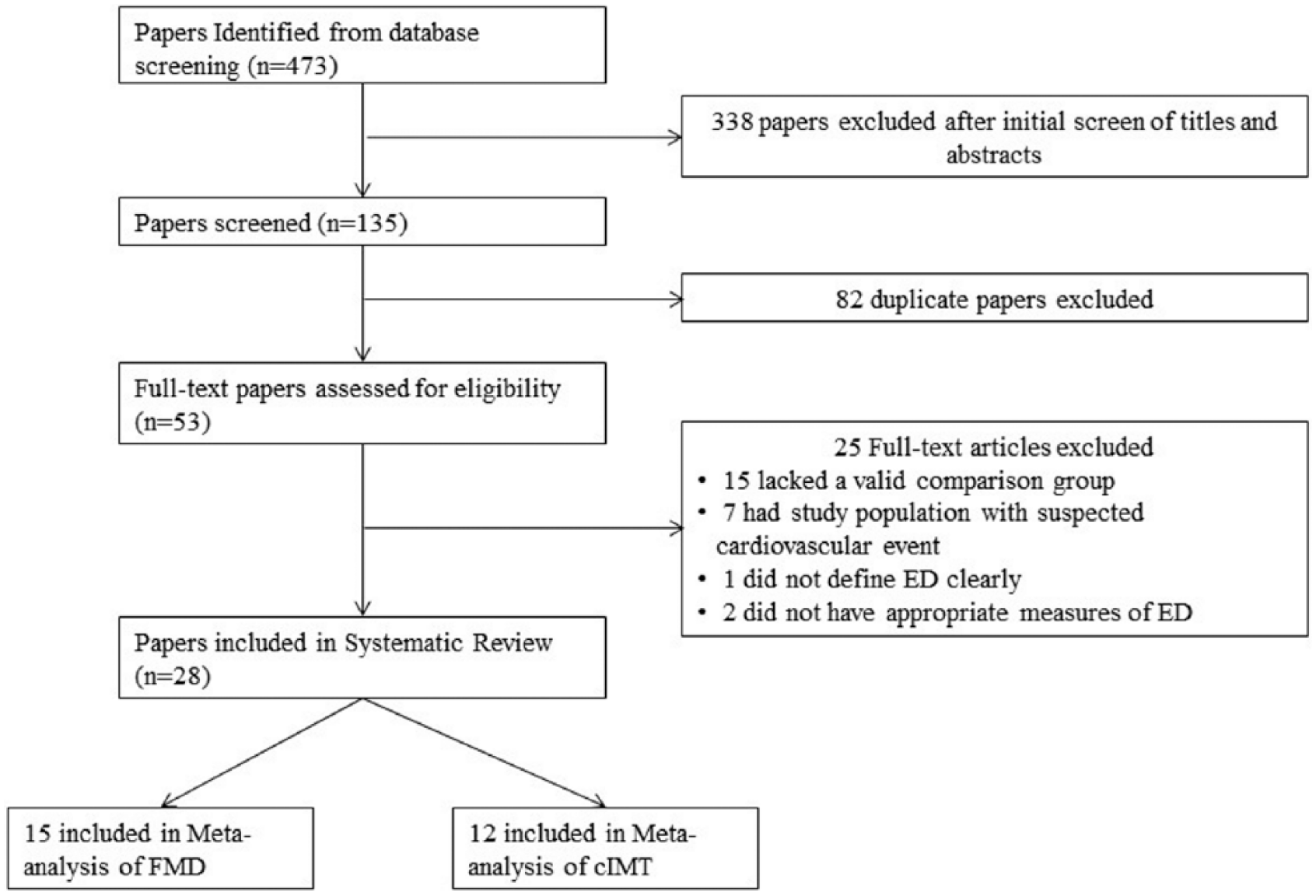
Systematic review search results.
Description of studies included in the review.
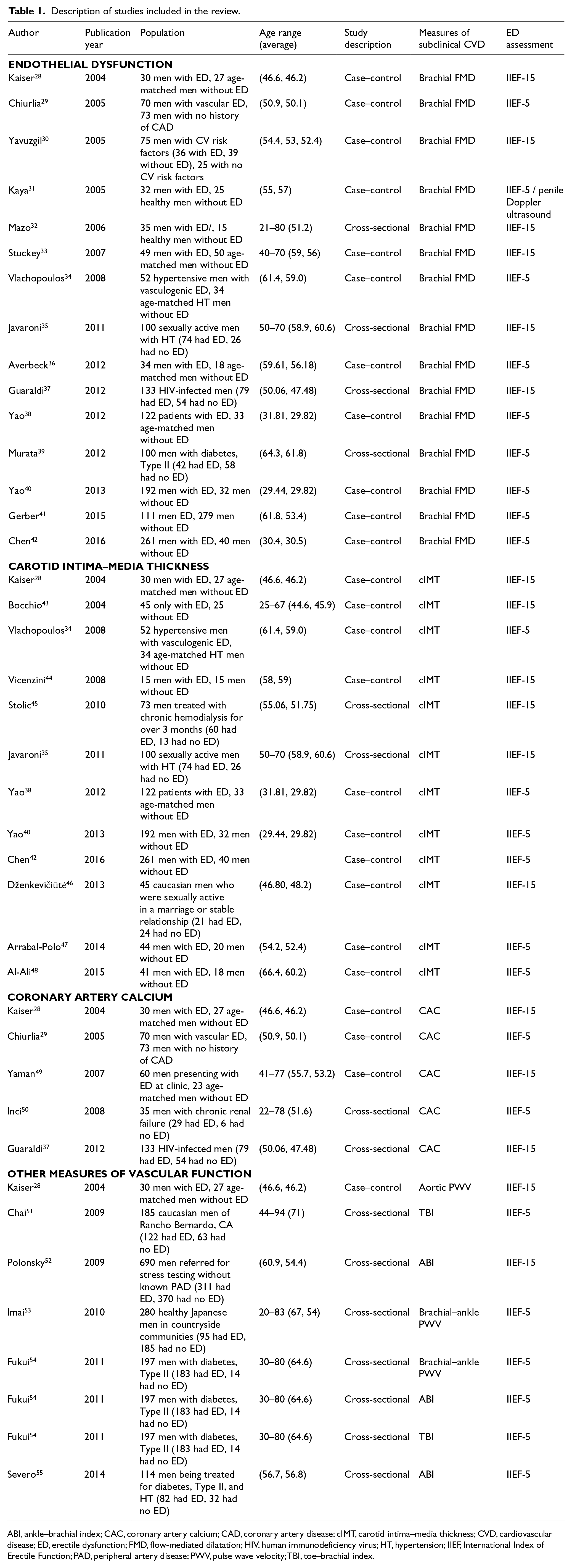
ABI, ankle–brachial index; CAC, coronary artery calcium; CAD, coronary artery disease; cIMT, carotid intima–media thickness; CVD, cardiovascular disease; ED, erectile dysfunction; FMD, flow-mediated dilatation; HIV, human immunodeficiency virus; HT, hypertension; IIEF, International Index of Erectile Function; PAD, peripheral artery disease; PWV, pulse wave velocity; TBI, toe–brachial index.
Erectile dysfunction and flow-mediated dilation
As shown in Figure 2, the meta-analysis of the association between ED and FMD demonstrates a significant relationship between ED and FMD. A total of 15 studies with 2025 participants examined the relationship between ED and FMD.28–42 They all measured brachial FMD; however, the methods of FMD assessment were not universal among the studies. Seven of the 15 studies had the cuff placed on the forearm (including one which described the wrist),28–32,37,39 while the others either had the cuff inflated over the arm36,38,40,42 or did not specify.33–35,41 In addition, the inflating pressures were inconsistent as studies reported pressures between 250 mmHg and 300 mmHg,28,30–32,38,40,42 while others had cuff pressures 50 mmHg above the systolic BP.29,33–36,39 One study had cuff pressures at least 100 mmHg above the systolic BP. 37 Cuff occlusion lasted for 4–5 minutes in most of the studies and the brachial artery diameter was measured at baseline and at 30–90 seconds post cuff occlusion in most studies. ED was assessed using the International Index of Erectile Function questionnaire (IIEF-15, five studies) or its short form (IIEF-5, ten studies). Using a random-effects model (REM), the meta-analysis of the pooled studies showed that persons with ED had FMD 2.6 percentage points less than those without ED (mean difference –2.64; 95% confidence interval (CI): –3.12, −2.15). There was significant between-study variability, with an I2 of 97% (Figure 2). In sensitivity analysis, sequential exclusion of the three most deviated studies resulted in a minimal change in the overall heterogeneity (I2 = 97.0%; p-value ≤ 0.001) (Supplementary Table 3). In subgroup meta-analyses, the mean difference was significantly different in age and study quality groups. However, none of the subgroups within any of the groups had a different direction of association, making them unlikely to have accounted in entirety for the significant heterogeneity between studies (see Table 2). More details on the results of the subgroup meta-analyses are shown in Supplementary Figures 1–4.
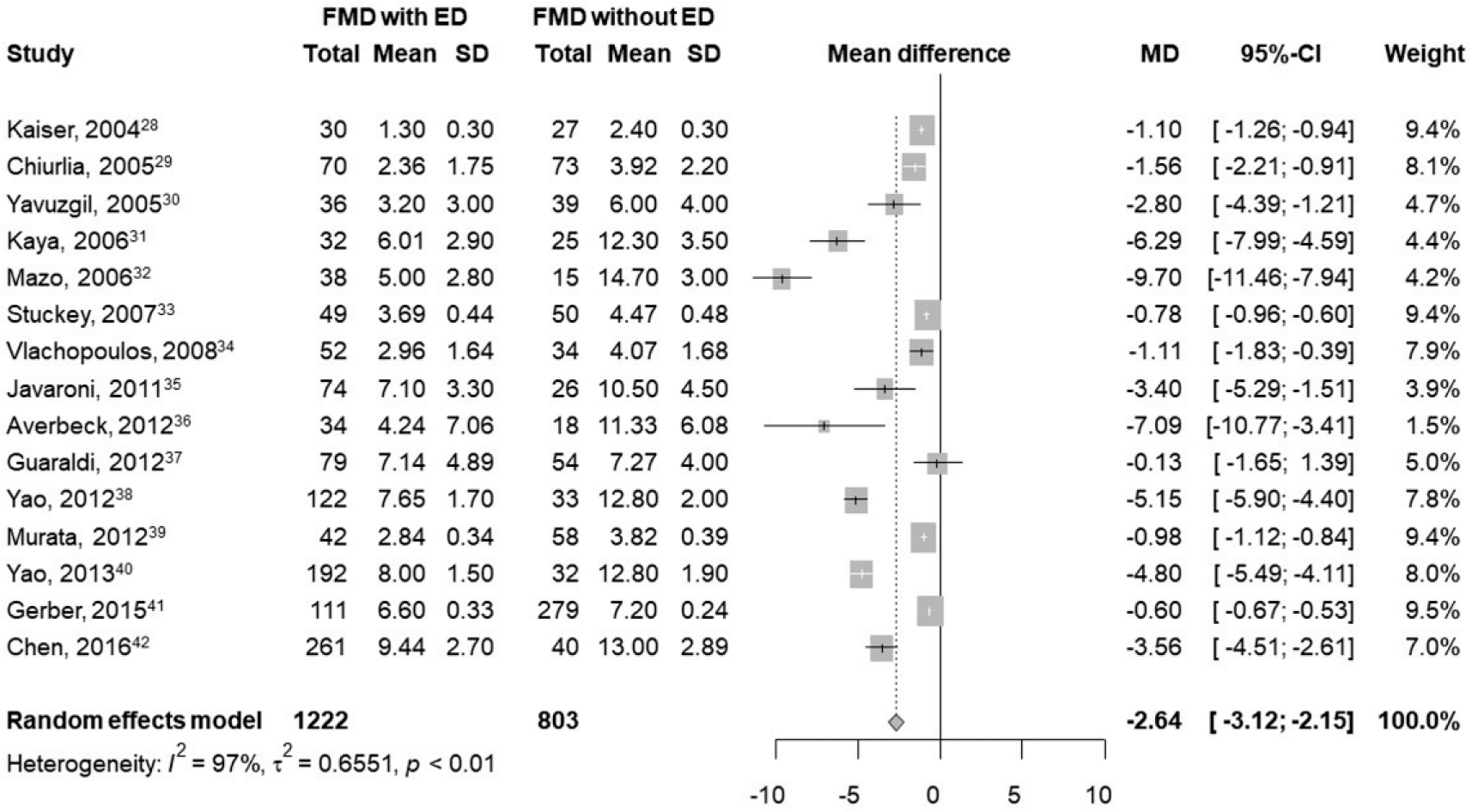
Meta-analysis of studies on the relationship between erectile dysfunction (ED) and flow-mediated dilatation (FMD). Results are shown as differences in percentage change between ED and non-ED groups and their pooled mean difference (MD).
Summary of stratified meta-analyses assessing the association of ED with FMD and cIMT.
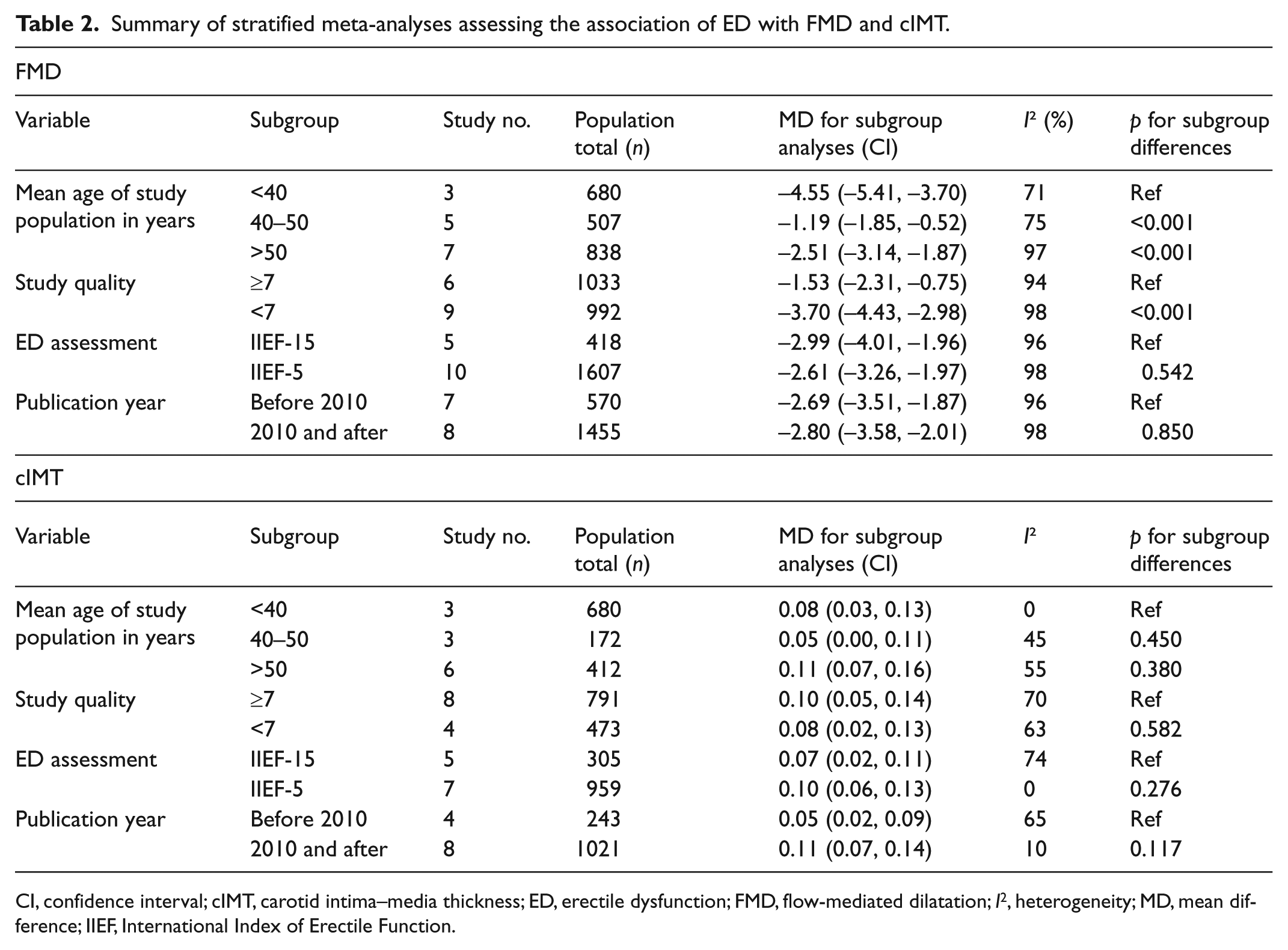
CI, confidence interval; cIMT, carotid intima–media thickness; ED, erectile dysfunction; FMD, flow-mediated dilatation; I2, heterogeneity; MD, mean difference; IIEF, International Index of Erectile Function.
Erectile dysfuntion and carotid intima-media thickness
Figure 3 shows a forest plot for the meta-analysis of the association between ED and cIMT. Overall, a significant association is demonstrated. Twelve studies with 1264 participants assessed the relationship between ED and cIMT.28,34,35,38,40,42–48 Eight of these studies assessed IMT in the common carotid arteries,28,34,35,42–44,46,48 one study measured IMT at the common carotid, carotid bifurcation and the proximal internal carotid artery on each side, 43 while no location was specified in three studies.38,40,45,47 The methods of assessing ED were also the IIEF-15 (seven studies) and the IIEF-5 (five studies). Persons with ED had significantly greater cIMT (0.09 mm) than those without ED (mean difference: 0.09 mm; 95% CI: 0.06 mm, 0.12 mm). There was also substantial heterogeneity between cIMT studies (I2 = 73%). In a subgroup meta-analysis, neither age, ED questionnaire type, study quality, nor publication year was a source of heterogeneity, as there was statistical similarity in the mean difference within these groups. Details of the subgroup meta-analysis results can be seen in Table 2. More details on the subgroup meta-analysis are shown in Supplementary Figures 5–8. In sensitivity analysis, exclusion of the three most influential studies revealed an attenuation of heterogeneity among studies that was statistically non-significant (I2 = 0%; p-value = 0.75) (Supplementary Table 3). The study by Kaiser et al. 28 appears to be most responsible for the heterogeneity observed in this meta-analysis, as exclusion of this study alone resulted in more than a 25% drop in I2 (71% to 21%, see Supplementary Table 3).
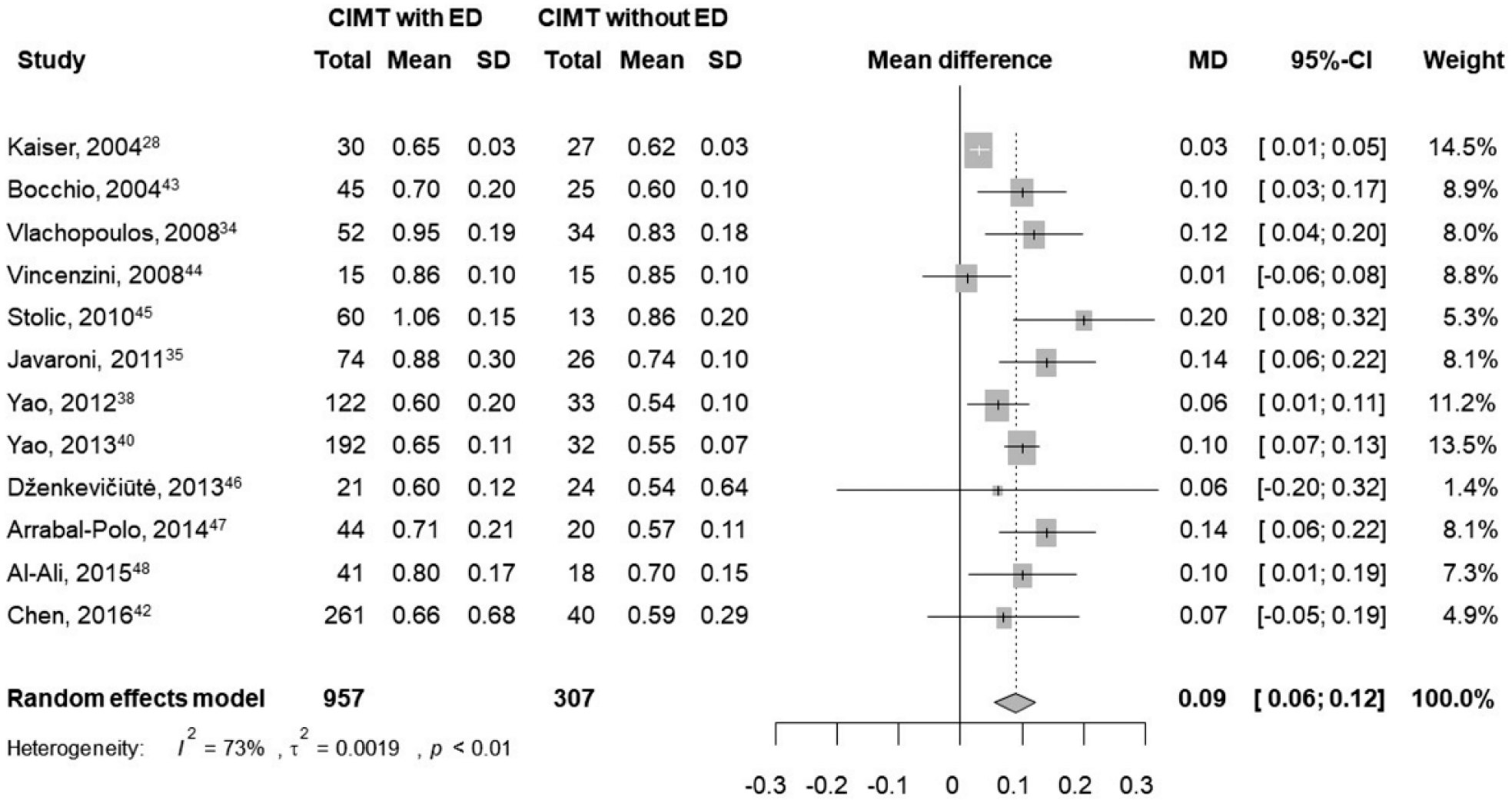
Meta-analysis of studies on the relationship between erectile dysfunction (ED) and carotid intima–media thickness (cIMT). Results are shown as differences in mean cIMT (in mm) between ED and non-ED groups and their pooled mean difference (MD).
Erectile dysfunction and coronary artery calicification
Five studies examined the association between ED and CAC28,29,37,49,50 (Table 3). Two of the five studies showed a significant association between ED and CAC.29,49 Both of these studies demonstrated greater CAC burden among those with ED compared to those without ED. In general, all the CAC studies had sample sizes less than 200.
Summary of subclinical atherosclerosis measures and their association with ED. a
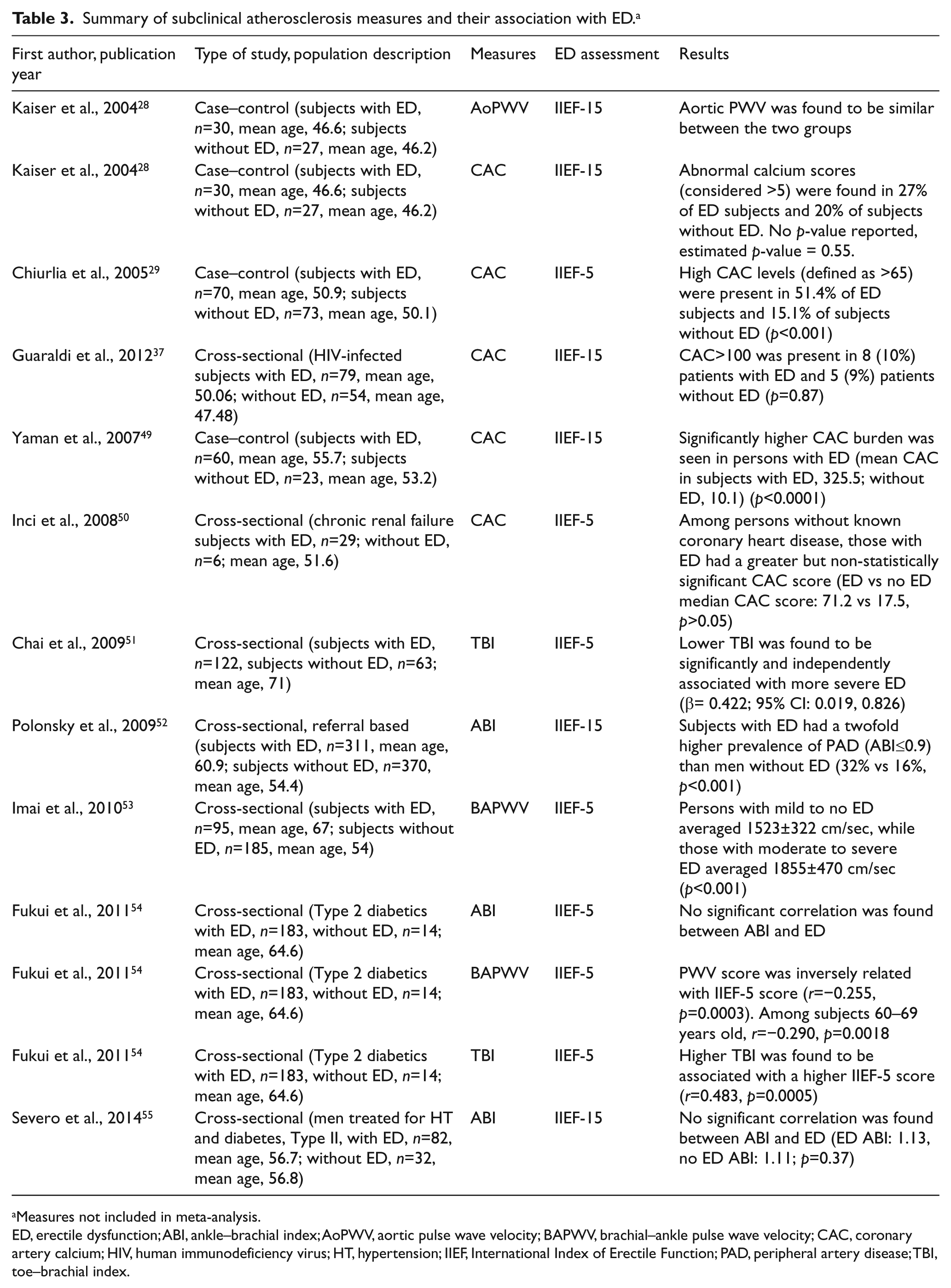
Measures not included in meta-analysis.
ED, erectile dysfunction; ABI, ankle–brachial index; AoPWV, aortic pulse wave velocity; BAPWV, brachial–ankle pulse wave velocity; CAC, coronary artery calcium; HIV, human immunodeficiency virus; HT, hypertension; IIEF, International Index of Erectile Function; PAD, peripheral artery disease; TBI, toe–brachial index.
Erectile dysfunction and other measures of vascular function
Six studies assessed the relationship between ED and other various measures of vascular function (some studies assessed vascular function using more than one measure).28,51–55
Among the three studies that examined the relationship between ED and ABI, two of them demonstrated no association with ABI, while one study showed that the prevalence of ED was two times higher among persons with an ABI ≤0.9 than those with an ABI >0.9. Both studies showing no association between ED and ABI were conducted in primarily diabetic populations.
Only two studies examined the association between ED and TBI, with both studies showing similar results. One of these studies determined that ED was significantly associated with a lower TBI, while the other showed that lower scores on the IIEF-5 (increased likelihood of ED) were associated with a lower TBI.
Similar to TBI, two studies assessed the association of ED and BAPWV, with both studies showing that ED was significantly associated with this marker of vascular function. However, the only study that assessed the relationship with AoPWV did not show any significant association.
Assessment of publication bias
For the studies included in the meta-analysis (i.e. those assessing the association of ED with FMD and ED with cIMT) we assessed the likelihood of publication bias by creating a funnel plot and conducting formal tests of asymmetry (Supplementary Figures 9 and 10). In both FMD and cIMT studies, linear regression tests of funnel plot asymmetry were not statistically significant, indicating a lower likelihood of publication or other bias.
Discussion
In this systematic review and meta-analysis, we demonstrate that ED is associated with subclinical CVD in most, but not all studies. The evidence is strongest for the association of ED with poor endothelial function (measured by FMD) and carotid disease, both of which demonstrated significant association in meta-analyses. These relationships remained consistent within age, study quality, methods of assessing ED, and publication year subgroups. Importantly, ED, when identified by a simple five-item questionnaire (IIEF-5), shows similar relationships with endothelial dysfunction and carotid atherosclerosis as the longer form of the questionnaire (IIEF-15). This underscores the IIEF-5 utility for identifying persons at risk of subclinical CVD. Although age accounted for some heterogeneity between FMD studies, participants in all age groups demonstrated a significant association of ED with subclinical CVD. This is particularly important in younger men who are less likely to be screened for subclinical CVD and who may be presenting to a provider for the first time with symptoms related to ED. Our study findings indicate that such men are at greater risk of having identifiable subclinical CVD and will benefit from an active CVD work-up.
Coronary artery calcium, an assessment that is most predictive of coronary artery disease, had varying results as only two of the five studies showed an association with ED. Most of the CAC studies had small sample sizes (most studies had less than 200 participants), which may limit a study’s ability to detect small differences between groups and may account for the lack of association seen. Thus, there is inconclusive evidence to either prove or refute an association between ED and CAC, and larger studies are needed.
Among the measures of vascular stiffness, ABI had conflicting associations with ED, while ED was consistently associated with lower TBI and increased BAPWV. We note that both studies with no significant associations of ED with ABI were conducted among primarily diabetic participants. Previous studies among diabetic individuals have shown that ABI is a poor marker of cardiovascular disease mortality and that TBI has a better predictive value.56,57 Thus, among the non-ABI studies, ED appears to identify peripheral vascular stiffness (irrespective of diabetic status) as all the studies showed a significant relationship with markers of peripheral vascular function. In addition, all three studies in non-diabetic populations showed a significant association between ED and peripheral vascular function.51–53 Summed together, our findings suggest that ED is associated with peripheral vascular disease and that non-ABI measures may be important tools in the assessment of persons with diabetes and ED. We would also emphasize that ABI has been demonstrated to be a poor measure of vascular stiffness in diabetic participants.56–58 More studies are required on the measures of central arterial function, as we found only one study that measured the AoPWV. 28
It is thought that endothelial dysfunction, an early marker of atherosclerosis, is also one of the earliest abnormalities seen in persons with ED. 40 Therefore, persons with ED and endothelial dysfunction may benefit from aggressive CVD preventive management, even if there are no other obvious CVD risk factors (as may be seen in young persons with ED). On the other hand, ED also identifies markers of advanced subclinical vascular disease such as ABI and TBI, especially among men without diabetes. This is particularly significant as men without diabetes are probably less likely to be assessed for peripheral artery disease, especially if they are asymptomatic like those in the studies. Considering the significant morbidity and mortality burden associated with peripheral vascular disease, 59 our results suggest that ED may be a marker of subclinical CVD and atherosclerosis, even in patients without an overt diagnosis of peripheral vascular disease. ED may be used to identify patients who may benefit from early screening for vascular dysfunction.
Both ED and increased cIMT are predictive of stroke.60,61 Thus, our findings in which there is increased cIMT in persons with ED support earlier findings from prospective studies on ED and stroke, and suggest that cIMT assessment in persons with ED may improve stroke risk stratification.
ED and CVD are thought to share common mechanisms. Both disorders are associated with increasing age, alcohol use, smoking, obesity, diabetes, and sedentary lifestyle. 19 These risk factors are strongly associated with conditions contributing to poor vascular flow, such as endothelial dysfunction and atherosclerosis. Our finding, in which there is a consistent association of ED with three of the four domains of subclinical CVD we assessed (endothelial dysfunction, carotid atherosclerosis, and other markers of vascular function), further supports the theory of shared mechanisms between ED and CVD. However, longitudinal relationships would need to be assessed to further define the pathogenetic role atherosclerosis plays in ED.
Previous studies have demonstrated the utility of CVD risk reduction (through lifestyle changes and/or statins) in improving ED; however, the benefits of CVD risk reduction on ED improvement are still not widely publicized, especially to men who are less likely to participate in lifestyle improvement programs.62–64 Our study supports a more aggressive CVD risk assessment and management of persons with ED, including among young men who may otherwise have been categorized as low risk due to their young ages. The measures of subclinical disease included in this review (with the exception of CAC) can be assessed by non-invasive office-based procedures with no radiation risk and whose results can be available during a clinic visit. Such easy-to-conduct tests coupled with the ability to identify ED through the use of a short questionnaire (IIEF-5) make ED identification and subsequent assessment of subclinical CVD feasible in a primary care office setting.
Limitations
One of the weaknesses of our review is that all the studies in this review are either cross-sectional or case–control in design. This is reflected in the relatively low scores in quality that the studies in this review received. As such, we are unable to assess the temporal relationship between ED and subclinical CVD. Additionally, we are unable to control for many covariates such as hormone levels, diet (which may affect hormone levels), disorders resulting in cavernosal fibrosis, kidney function, depression status or medication use, which were not adjusted for or reported in most of the studies. These conditions also cause ED and are not necessarily vascular and may serve as potential confounders. The absence of patient-level data on participants who are on optimal guideline-directed CVD therapy makes it impossible to account for the effect of prevention interventions on the relationship between ED and CVD. Other weaknesses include a significant heterogeneity of values within the studies in the meta-analysis. Sensitivity analysis excluding the most outlier studies did not significantly change statistical heterogeneity among the FMD studies. However, among the cIMT studies, this analysis showed a decline of the I2 to 0 without a significant change in the absolute mean difference. We could not determine the source of this heterogeneity, even after conducting subgroup analysis. Reasons for this may be the very diverse populations included across the studies, some assessments being operator dependent (such as FMD), or differences in how cardiovascular disease risk assessments are organized and reported. Age and study quality only contributed partly to the heterogeneity between studies, as demonstrated in our subgroup meta-analyses. We were unable to account for intra-study differences in age as the subgroup analyses only accounted for age differences across (but not within) studies. Other unaddressed sources of heterogeneity include the inter-operator (and possibly intra-operator) differences that were likely to have occurred in these studies. This may be more prominent for the brachial artery FMD measurement, which is heavily user dependent and which did not have a uniform standard of measurement (as noted in the Methods section). Unfortunately, we are unable to assess or account for these differences in our meta-analyses. Our assessment of funnel plot asymmetry suggests an increased likelihood of publication bias among the FMD and cIMT studies.
Conclusion
This study demonstrates an association between ED and measures of subclinical CVD, shedding more light on the relationship between ED and CVD, and suggests that ED may be useful in CVD risk stratification. Future research should focus on determining the longitudinal relationship between ED and subclinical CVD and should involve larger sample sizes. As coronary artery calcification testing becomes more common, larger studies on its relationship with ED should also be conducted.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.