
Abstract
Introduction:
Single bouts of prolonged bent-legged sitting attenuate popliteal endothelial-dependent vasodilation (as assessed via flow-mediated dilation [FMD]), which is partially attributed to arterial ‘kinking’. However, the impact of knee-flexion angle on sitting-induced popliteal FMD is unknown. The objective of this study was to perform separate laboratory and free-living studies to test the hypotheses that: (1) popliteal FMD impairments would be graded between knee flexions at 90° (bent-legged sitting) > 45° > 0° (straight-legged sitting) following a 3-hour bout of sitting; and (2) more habitual time spent bent-legged sitting (< 45°) would be associated with lower FMD.
Methods:
The laboratory study included eight young, healthy adults (24 ± 2 years; four women) who underwent two sitting bouts over 2 days with one leg positioned at a knee-flexion angle of 0° or 90° and the opposite leg at 45° knee flexion. Popliteal FMD was assessed at pre- and postsitting timepoints.
Results:
Sitting-induced reductions in FMD were similar between all knee-flexion angles (all, p > 0.674). The free-living study included 35 young, healthy adults (23 ± 3 years; 16 women) who wore three activPAL monitors (torso, thigh, shin) to determine detailed sedentary postures. Time spent sedentary (624 ± 127 min/day), straight-legged sitting (112 ± 98 min/day), and bent-legged sitting (442 ± 106 min/day) were not related to relative FMD (5.3 ± 1.8%; all, p > 0.240).
Conclusion:
These findings suggest that knee-flexion angle-mediated arterial ‘kinking’ during sitting is not a major contributor toward sitting-induced popliteal endothelial-dependent vasodilatory dysfunction.
Keywords
Introduction
Sedentary behavior is defined as any waking behavior characterized by a low-energy expenditure (i.e., ⩽ 1.5 metabolic equivalents) while in a sitting, reclining, or lying posture. 1 Current national 2 and international 3 activity guidelines recommend that adults limit their total sedentary time and duration of prolonged sedentary bouts for optimal health benefits. Specifically, excessive engagement in sedentary postures is a predominant, independent risk factor for cardiovascular diseases such as peripheral artery disease.4,5 Lower-limb arteries, particularly the popliteal artery, are common sites for the development of atherosclerosis and formation of aneurysms. 6 As such, excessive engagement in sedentary behaviors is likely to have detrimental consequences on popliteal endothelial health. Endothelial-dependent vasodilatory function may be noninvasively determined via the flow-mediated dilation (FMD) technique, 7 which uses high-resolution ultrasound to measure vasodilation in response to a hyperemic stimulus (i.e., shear stress) induced via a brief period of distal ischemia. 8 Lower FMD responses provide an indication for endothelial dysfunction and represent a greater risk of developing peripheral artery disease. 9 However, the current understanding regarding the impact of sedentary postures on lower-limb vascular function is limited, especially in the free-living environment.
Sedentary time is a ‘catch-all’ term used to encompass all sedentary postures. 1 Laboratory-based studies have consistently demonstrated that single bouts of prolonged sitting (i.e., ⩾ 3 hours) attenuate popliteal FMD responses.10 -16 The negative lower-limb endothelial consequences of prolonged sitting may be partially attributed to knee-flexion angle as a single, 3-hour bout of bent-legged (90°) side-lying provoked a decline in popliteal FMD that was not observed in the contralateral straight leg (0°). 17 Specifically, it is theorized that sitting-induced vascular dysfunction may be attributed to the mechanical deformation of the popliteal artery when the knee is bent.17,18 Though these laboratory-based studies have yielded important knowledge regarding the vascular consequences to sitting, the independent effect of knee-flexion angles during sitting have not been explored. Furthermore, objective characterization of how sedentary time is accumulated in a free-living setting, 19 including time spent in straight versus bent-legged sitting, has yet to be studied.
Our understanding of how habitual sedentary patterns impact popliteal function is limited, with null relationships observed between total sedentary time and FMD responses.20–22 Importantly, engagement in more frequent prolonged sedentary bouts is associated with worse popliteal FMD responses in healthy adults. 20 To date, free-living measures of sedentary time have been unable to differentiate between specific sedentary postures, 20 making it impossible to uncover how variations in hip- and knee-angle postures may impact lower-limb arterial health in real-world conditions. As such, our understanding of how habitual time spent in distinct sedentary postures (e.g., sitting versus lying, bent-legged sitting versus straight-legged sitting, etc.) relates to lower-limb endothelial-dependent function is unknown and warrants investigation.
We studied the acute and chronic impacts of knee flexion during prolonged sitting on popliteal vascular function using independent laboratory and free-living studies in healthy young adults. Specifically, the purpose of the laboratory-based study was to determine how the knee-flexion angle (0° [straight leg], 45°, 90° [bent leg]) altered the popliteal FMD response to a single bout of prolonged sitting (~3 hours). It was hypothesized that the degree of sitting-induced FMD impairment would be graded as the knee-flexion angle was increased (i.e., 90° > 45° > 0° [straight-legged sitting]). The free-living study determined whether habitual time spent sitting with straight versus bent legs was associated with popliteal relative FMD. It was hypothesized that greater habitual time spent sitting with bent legs (versus straight legs) would be associated with lower popliteal FMD responses in healthy young adults.
Methods
Participants
The laboratory-based study included eight young, healthy adults (24 ± 2 years, four women; Study 1). Based on an effect size reported for FMD in a previously conducted prolonged sitting study 23 (η2 = 0.481), a sample size calculation for a within-between-subject interaction using a repeated measure ANOVA model indicated that a minimum of six participants were required assuming an α = 0.05, 80% power, and correlation among repeated measures of 0.80. The free-living study included 35 young, healthy adults (23 ± 3 years, 16 women; Study 2). There were no overlapping participants in both study designs. Habitual, monitor-derived activity data from participants in the free-living study have been published previously in a study that examined the impact of sedentary postures on heart rate variability, 24 but the current study implemented novel analyses (i.e., straight- versus knee-bent sitting) to answer an independent research question. All participants were nonsmokers and had a resting seated blood pressure < 135 mmHg/< 85 mmHg. 25 Women were not pregnant or breastfeeding and self-reported having a regular menstrual cycle (~28 days). To minimize the potential confounding influence of endogenous or exogenous sex hormones on vascular function, 7 10 women (laboratory study: n = 2; free-living study: n = 8) were tested in the early follicular phase (i.e., days 1–5 following onset of menstruation) and two women from the free-living study were tested during the late luteal phase (i.e., days 10–15 following onset of menstruation) of their natural menstrual cycle. Furthermore, seven women (laboratory study: n = 1; free-living study: n = 6) were tested during the placebo/inactive phase of monophasic oral contraceptive pill use. Finally, one woman in the laboratory study used a copper intrauterine device. Prior to testing, verbal and written informed consent were acquired. All protocols and procedures conformed to the Declaration of Helsinki, with the exception of registration in a database, and were approved by the Dalhousie University Health Sciences Research Ethics Board.
Study 1: Laboratory-based experimental design
Participants visited the laboratory on 2 separate days and completed two, 3-hour prolonged sitting sessions. Day 1 consisted of the screening and informed consent, which included anthropometric measurements, prior to the popliteal ultrasound assessments. On Day 2, participants underwent additional popliteal ultrasound assessments and were equipped with a thigh-worn activPAL inclinometer (Pal Technologies Ltd, Glasgow, UK) for 7 subsequent days of wear. Days 1 and 2 were scheduled at the same time of day and no more than 48 hours apart.
Three knee-flexion angles (0° [straight leg], 45°, 90°] were randomly assigned between each leg over Days 1 and 2 (i.e., one knee-flexion angle per leg per day). On each day, one leg was always assigned the control knee-flexion angle of 45°, by which comparisons were assessed against the 0° and 90° knee-flexion angles assigned to the contralateral leg. The 45° knee-flexion angle was chosen as the repeated angle because it is in-between the two extreme knee-flexion angles investigated (i.e., 0° and 90°) and permits relatively undisturbed access for imaging without passively adjusting the leg. Following 10 minutes of prone rest, used to find the location of both popliteal arteries prior to baseline FMD, participants actively transitioned to a sitting position. Knee-flexion angles were positioned by the researcher via a goniometer, and maintained by supporting the feet, for the duration of the study.
The baseline FMD test commenced for the first leg at the assigned knee-flexion angle, while the contralateral leg was positioned at 0° knee flexion (i.e., straight) to minimize sitting-induced reductions in blood flow/shear stress. 26 After the first FMD assessment was completed, the contralateral leg was positioned to the assigned knee-flexion angle and the corresponding FMD was performed immediately thereafter. All FMD assessments were conducted in the sitting position to accurately capture the vascular environment associated with arterial ‘kinking’. Baseline FMD assessments were performed at the assigned knee-flexion angle unless the leg had to be passively moved to ~45° to accommodate a high-quality popliteal image (n = 2). During the prolonged seated period, participants were constantly monitored by research personnel to minimize excessive leg movements. The FMD assessments were then repeated for each leg after ~3 hours of sitting (same order as baseline testing).
Study 2: Free-living experimental design
Participants completed one laboratory visit. This involved completion of the screening and informed consent process, which included anthropometric measurements, prior to the popliteal ultrasound assessments. Popliteal FMD assessments were performed in the prone position, on the left leg, following an initial 10-minute rest period. All hemodynamic data were recorded directly following this resting period. All assessments were completed in a thermoneutral environment (21°C). Participants were equipped with three activPAL monitors at the end of this visit for 7 subsequent days of wear (see details below).
Anthropometrics and systemic hemodynamics
Height and weight were measured using a calibrated stadiometer/physician’s scale (Health-O-Meter, McCook, IL, USA) to the nearest 0.5 cm and 0.1 kg, respectively. These measures were used to calculate body mass index (BMI) as body mass ÷ height2 (kg/m2). Heart rate (HR), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were assessed via an automated vital signs monitor (Carescape v100; General Electric Healthcare, Mississauga, ON, Canada).
Habitual activity and posture monitoring
Participants in the laboratory-based study were equipped with one thigh-worn activPAL, whereas participants in the free-living study were equipped with three activPAL inclinometers positioned on their torso, thigh, and shin. All monitors were waterproofed via a nitrile finger cot and secured using Tegaderm medical dressing (3M; London, ON, Canada). 27 The thigh monitor was positioned on the right anterior thigh, one-third of the way to the knee from the hip. The shin monitor was positioned on the anteromedial side of the right tibia. The torso monitor was placed below the ribcage on the right side, parallel to the other two monitors (online supplemental Figure 1). Participants wore the activPAL monitors 24 hours/day for a minimum of 5 days (laboratory-based study: everyone wore for 7 days; free-living study: 6.8 ± 1.0 days; range: 5–7 days). 27 Participants self-reported their waking hours using a take-home sleep diary to ensure that only waking activity and not sleeping postures were used for sedentary outcomes.
For the laboratory-based study, the activPAL data were analyzed using a customized LabVIEW program (LabVIEW 2018; National Instruments, Austin, TX, USA) that estimated waking activities and summarized the daily averages of waking hours spent stepping, standing, and in sedentary postures. 28 For the free-living study, a custom-designed MATLAB program (R2022a; MathWorks, Inc., Natick, MA, USA) calculated knee and hip flexion angles, as described in detail and provided as open source elsewhere. 19 For the purposes of this study, hip angles < 30° (i.e., angle between torso and thigh monitor) were considered lying and angles > 30° were considered sitting. During sitting, knee angles > 45° and < 45° were classified as bent-legged and straight-legged sitting, respectively. Total time spent in each posture (sitting, lying, bent-legged sitting, and straight-legged sitting) was used to answer our primary research questions. However, prolonged time spent in each posture (defined as > 1 hour/bout) is also presented for completeness. In the free-living environment, prolonged sitting was defined at > 1 hour as previous lab-based studies have demonstrated significant attenuation of lower-limb FMD after only 1 hour of prolonged sitting 29 and evidence that adults rarely sit for 3 hours uninterrupted in free-living conditions. 30
Physical activity intensity was determined using a customized program (LabVIEW 2018) using the thigh monitor only in both the laboratory-based and the free-living studies. Step rate thresholds that corresponded to light, moderate, and vigorous intensity were determined for each individual based on height and time spent within these thresholds and were summed. 31
Popliteal flow-mediated dilation assessment
To minimize confounding influences on endothelial-dependent dilation, vascular assessments were performed 6 hours postprandially and after avoiding strenuous physical activity, as well as the consumption of products known to acutely influence FMD responses (e.g., caffeine, chocolate, kiwi, saturated fats, folic acid supplements, antioxidants, and multivitamin supplements) for 24 hours, consistent with FMD guidelines. 7
Popliteal assessments were conducted via duplex ultrasonography using a 12-MHz multifrequency linear array probe (Vivid i; General Electric Healthcare) and conducted following published guidelines. 7 The popliteal artery was imaged proximal to the bifurcation at, or slightly above, the popliteal fossa. Ultrasound videos were continuously recorded in real time during all FMD assessments. Red blood cell velocity (RBCv) was continuously recorded using a pulsed frequency of 5 MHz and an insonation angle of 60° that was maintained across all participants.
A pressure cuff was secured around the widest circumference of the calf and attached to a rapid inflation system (E20 and AG101; Hokanson, Bellevue, WA, USA). The cuff was inflated to the suprasystolic pressure of 250 mmHg for 5 minutes to ensure distal ischemia was maintained. Following cuff pressure release, lumen diameter and RBCv were continuously recorded for an additional 5 minutes. Superior and inferior edges of the pulsed-wave sample volume were adjusted to encompass the entire arterial lumen, as recommended in published guidelines. 7 Video signals obtained from the ultrasound were exported to an external laptop via a video graphics array converter (VGA 2 USB; Epiphan Systems Inc., Ottawa, ON, Canada) for offline analysis.
Artery lumen diameter, RBCv, and shear rate were analyzed using an automated, commercial edge-detection and wall-tracking software (FMD Studio, Cardiovascular Suite; Quipu, Pisa, Italy) demonstrated to have high reproducibility with the analyses of popliteal FMD.10,32,33 In the laboratory study, one sonographer was responsible for performing all FMD tests. Three sonographers were responsible for performing the FMD assessments in the free-living study. All sonographers were trained and the researcher who blindly analyzed the video files ensured they were of high quality to be included. Peak diameter was determined as the peak diameter following cuff-deflation using a 3-second moving average that was monitored up to 5 minutes postdeflation. Absolute FMD was quantified as FMD (mm) = peak diameter – baseline diameter. Relative FMD was quantified as FMD (%) = [(peak diameter – baseline diameter) ÷ baseline diameter × 100%]. Shear rate (/s) was calculated as [(8 × mean RBCv (cm/s)) ÷ baseline diameter (cm)]. Popliteal blood flow (mL/min) was determined as [mean RBCv (cm/s) × 60 (s/min) × π × lumen radius2 (cm2)]. The hyperemic shear rate area under the curve (SRAUC) was assessed between the start of cuff deflation to the time that the peak diameter occurred. The time-to-peak dilation (s) after cuff deflation was also recorded.
The statistical assumptions required to conduct allometric scaling or SRAUC-normalization of FMD were not met for either study.34,35 Specifically, the regression between the natural log of peak FMD diameter and resting diameter did not have an unstandardized β that deviated from 1 and an upper confidence interval < 1 (laboratory-based study: β = 0.990, 95% CI: 0.925–1.003; free-living study: β = 0.990, 95% CI: 0.955–1.025) and the regression between relative FMD and SRAUC did not have a y-intercept of zero (laboratory-based study: y-intercept = 2.259, 95% CI: 1.115–3.404; free-living study: y-intercept = 4.337, 95% CI: 2.881–5.792), which was unchanged when absolute FMD was used (laboratory-based study: y-intercept = 0.125, 95% CI: 0.066–0.185; free-living study: y-intercept = 0.260, 95% CI: 0.170–0.350).
Statistical analysis
Laboratory-based study
All dependent variables were normally distributed based on the results of a Shapiro–Wilk test (p > 0.082), except for resting shear rate, absolute FMD, relative FMD, and SRAUC (all, p < 0.033). To uncover the prolonged effects of sitting at different knee-flexion angles on popliteal function, linear mixed effect models were conducted to explore the differences in main outcomes (i.e., blood flow, shear rate, relative FMD, absolute FMD, SRAUC) using fixed effects for knee-flexion angle (0°, 45°, 90°) × time (baseline, 3 hours of sitting). Bonferroni post hoc testing was used for significant pairwise comparisons. All statistical analyses were completed in IBM SPSS, Version 28.0 (IBM Corp., Armonk, NY, USA). Statistical significance was accepted as p < 0.05. All data are presented as means ± SD.
Free-living study
All data were assessed for normality using a Shapiro–Wilk test. All variables were confirmed normal (all, p > 0.065) except prolonged lying, prolonged sitting, prolonged straight-legged sitting, prolonged bent-legged sitting, total lying, and total straight-legged sitting (all, p < 0.012). Independent samples t-tests or Mann–Whitney U-tests were conducted on age, height, weight, BMI, SBP, DBP, HR, and all habitual activity outcomes to assess whether participants in the laboratory-based study and the free-living study exhibited different characteristics. A Kruskal–Wallis test was used to characterize if there were differences in the amount of time spent in each sedentary posture. Bivariate Pearson Product Moment (normal) or Spearman Rank (nonnormal) correlations determined the relationship between detailed sedentary postures with popliteal FMD. Furthermore, women may 36 or may not 10 exhibit attenuated popliteal FMD responses to prolonged sitting compared to men. Accordingly, subsequent multiple regressions were conducted with FMD and postural outcomes to determine if sex influenced the relationship between FMD and posture.
Results
Acute impact of knee angle on prolonged sitting-induced endothelial function
Participants had an average age of 23 ± 3 (range: 19–31) years, and BMI of 22.3 ± 1.9 (20.8–26.1) kg/m2 (Table 1). Baseline systemic hemodynamics are presented in online supplemental Table 1. There was a main effect of time for popliteal RBCv, blood flow, and shear rate (all, p < 0.003), whereby each decreased from baseline to postsitting (Table 1). RBCv and blood flow (both, p < 0.042), but not shear rate (p = 0.069), had a main effect of angle. Though there were no significant post hoc effects for RBCv angle (0° vs 45°, p = 0.063), popliteal blood flow was lower at 45° (p = 0.006) and 90° (p = 0.009) compared to 0°. However, no time × angle interactions were observed in these popliteal hemodynamics (all, p ⩾ 0.239) (Table 1).
Resting popliteal and flow-mediated dilation outcomes from participants in the laboratory-based study (N = 8).
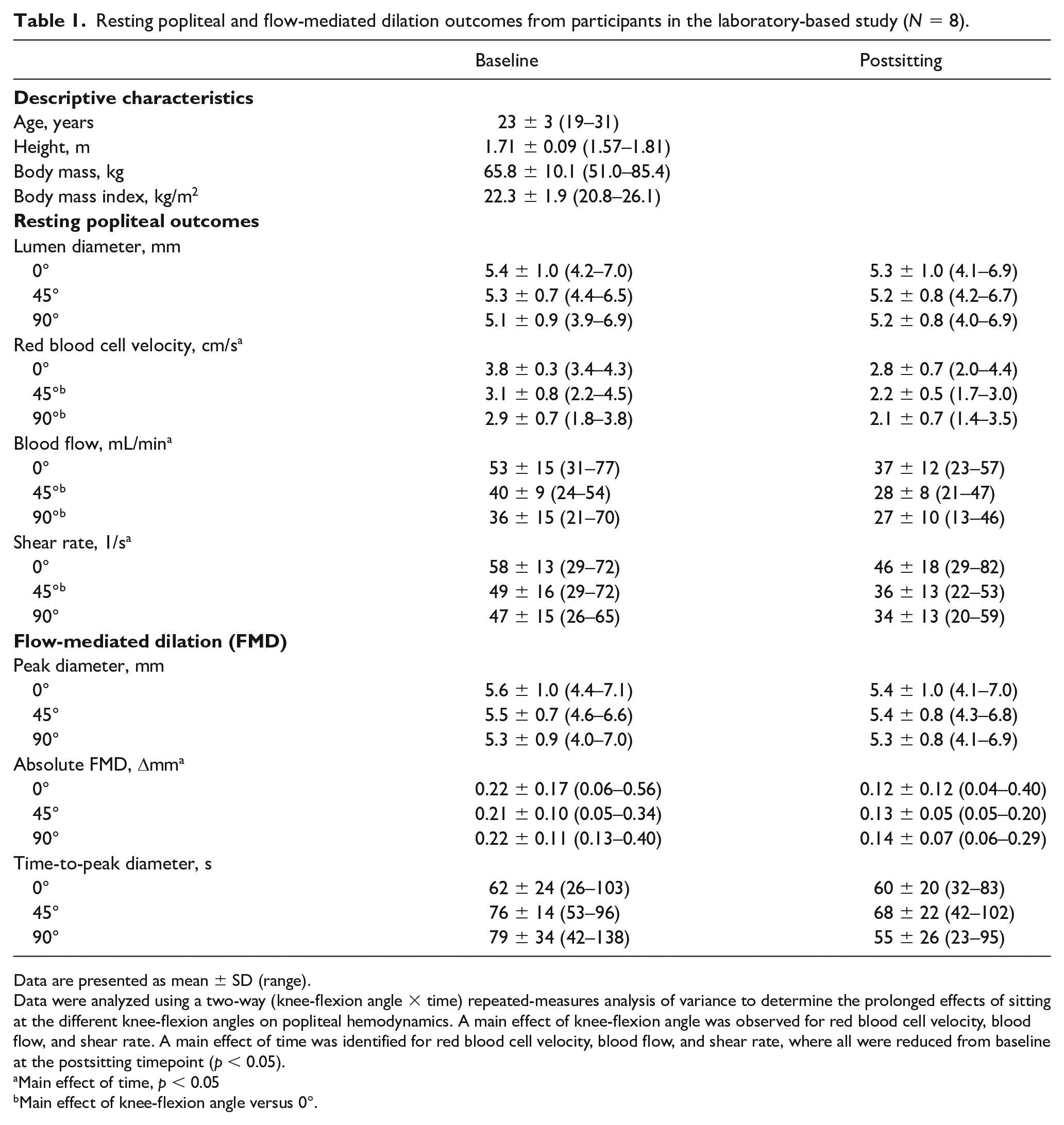
Data are presented as mean ± SD (range).
Data were analyzed using a two-way (knee-flexion angle × time) repeated-measures analysis of variance to determine the prolonged effects of sitting at the different knee-flexion angles on popliteal hemodynamics. A main effect of knee-flexion angle was observed for red blood cell velocity, blood flow, and shear rate. A main effect of time was identified for red blood cell velocity, blood flow, and shear rate, where all were reduced from baseline at the postsitting timepoint (p < 0.05).
Main effect of time, p < 0.05
Main effect of knee-flexion angle versus 0°.
Absolute and relative popliteal FMD responses were reduced (both, p < 0.010) postsitting (Figure 1). However, there was no effect of knee-flexion angle (both, p > 0.821), or differences in sitting-induced reductions in popliteal absolute or relative FMD between the three knee-flexion angles (i.e., interaction effect; both, p > 0.985). A main effect of angle was observed for SRAUC, where it was lower when the knee was flexed to 45° and 90° compared to the straight-leg condition (both, p < 0.021). However, there was no main effect of time (p = 0.384), nor an interaction effect (p = 0.474).
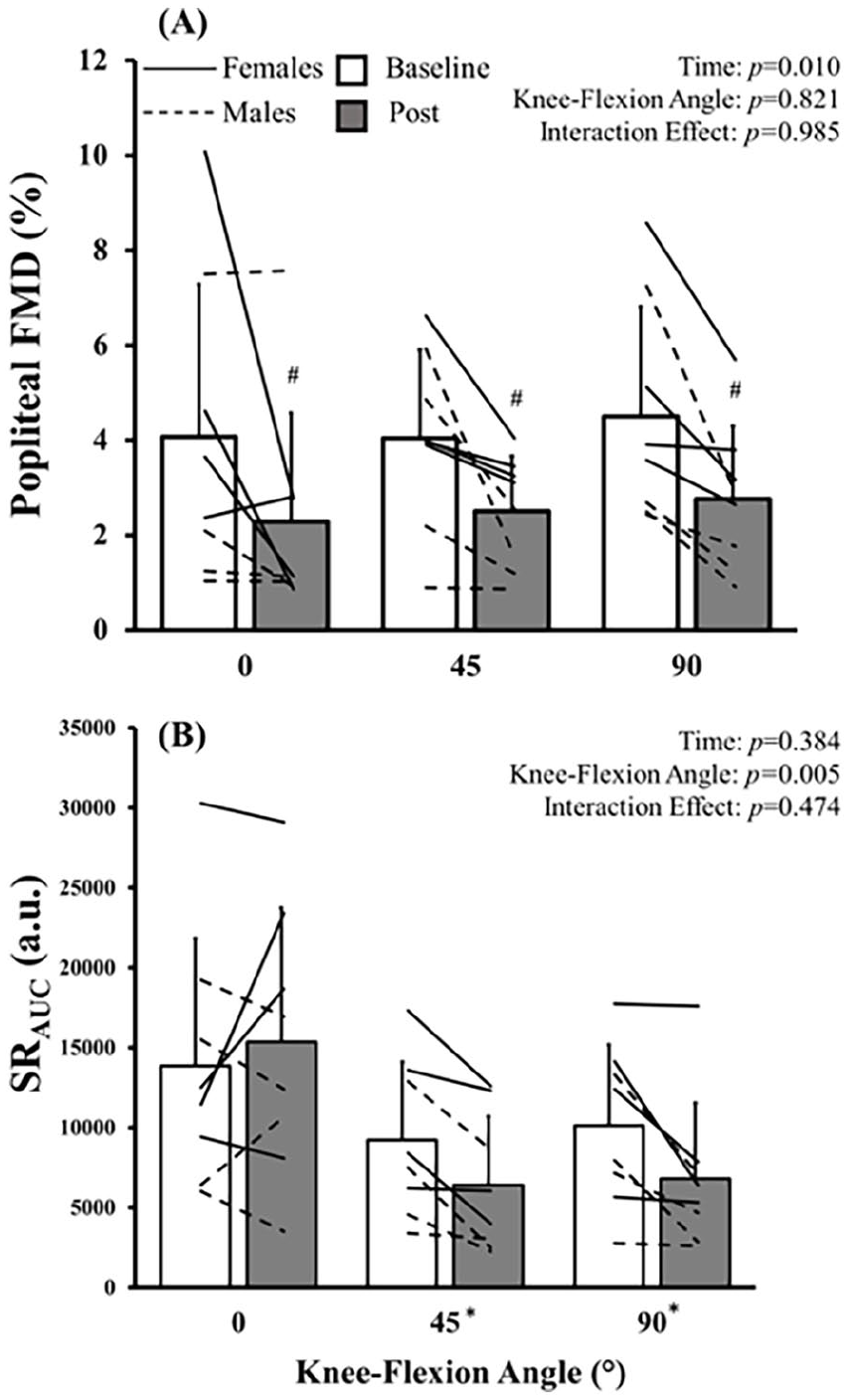
Group (mean ± SD) and individual (lines)
Relationship between free-living postures and endothelial function
Participants’ descriptive characteristics, systemic hemodynamics, and measures of popliteal function are presented in Table 2. Participants’ descriptive and habitual activity outcomes were not different compared to the laboratory-based study (all, p > 0.103), except those participants in the free-living study spent more time being sedentary and less time standing (both, p < 0.001).
Descriptive characteristics and resting hemodynamics for participants in the free-living study (N = 35).
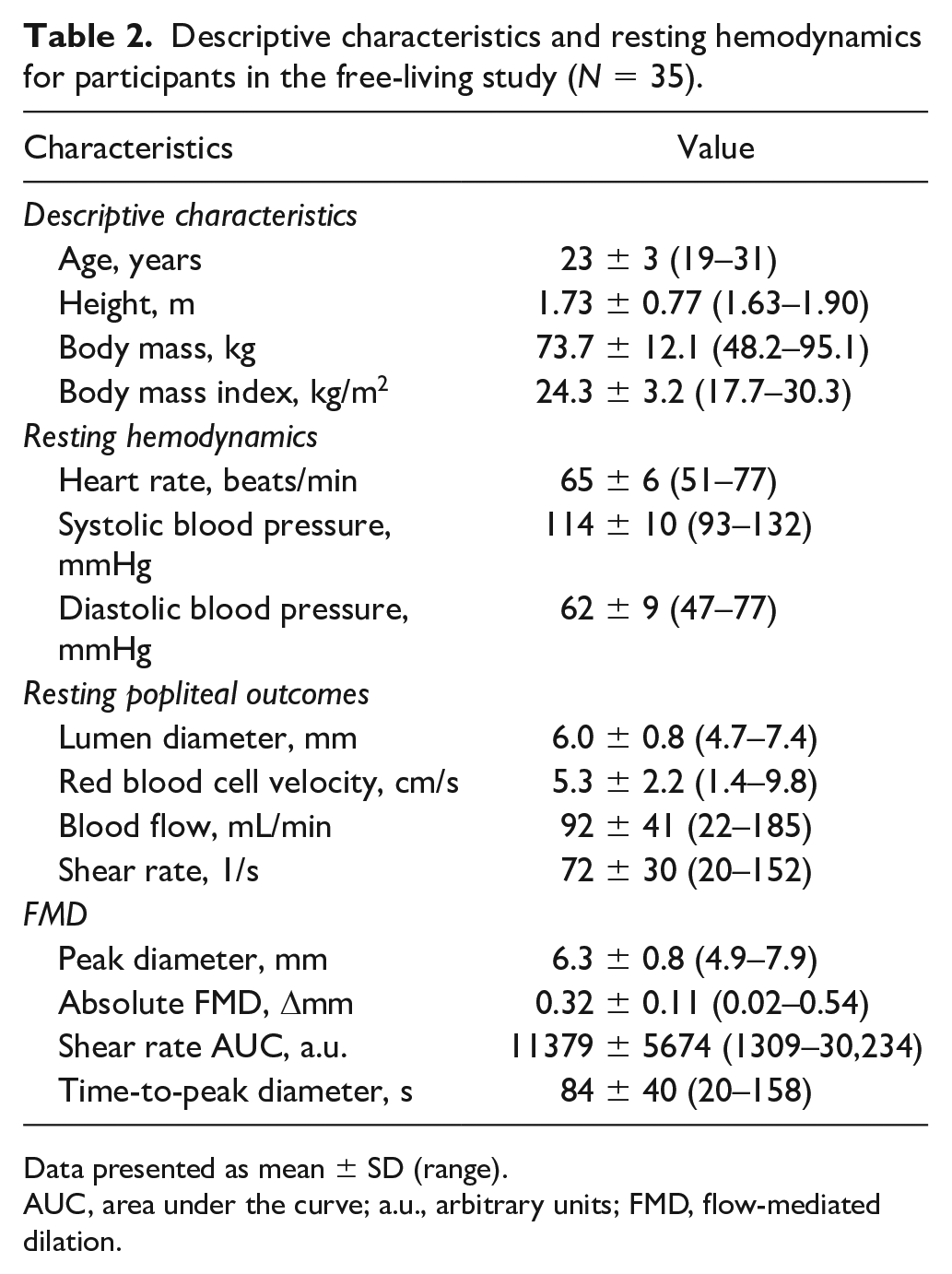
Data presented as mean ± SD (range).
AUC, area under the curve; a.u., arbitrary units; FMD, flow-mediated dilation.
There were no differences between the total sitting time (168 ± 95 min/day) and bent-legged sitting time (114 ± 67 min/day) (p = 0.216) or between lying time (38 ± 47 min/day) and straight-legged sitting time (54 ± 72 min/day) (p = 1.000). However, participants spent more time sitting than lying (p < 0.001) and in bent-legged sitting compared to straight-legged sitting (p < 0.001) (Table 3). Bivariate correlations demonstrated that relative popliteal FMD (5.3 ± 1.8%;all, p > 0.246; Figure 2), absolute FMD ( all, p > 0.293), and SRAUC (all, p > 0.205) were not associated with any sedentary posture outcomes. Importantly, this was unchanged when controlling for sex (all, p > 0.104). These observations were unchanged when time spent in prolonged postures was examined (online supplemental Figure 2).
Habitual activity outcomes from the free-living study (N = 35).
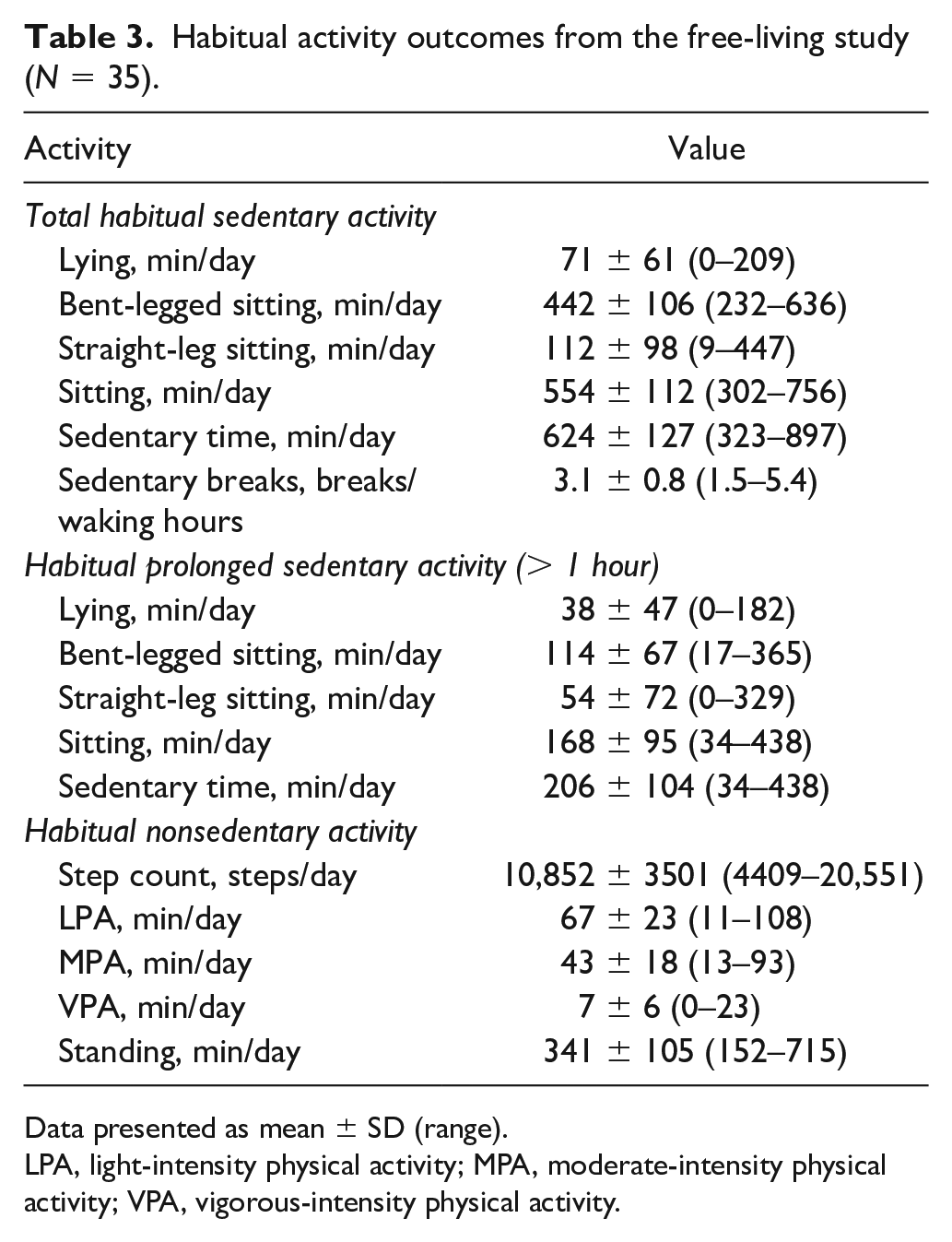
Data presented as mean ± SD (range).
LPA, light-intensity physical activity; MPA, moderate-intensity physical activity; VPA, vigorous-intensity physical activity.
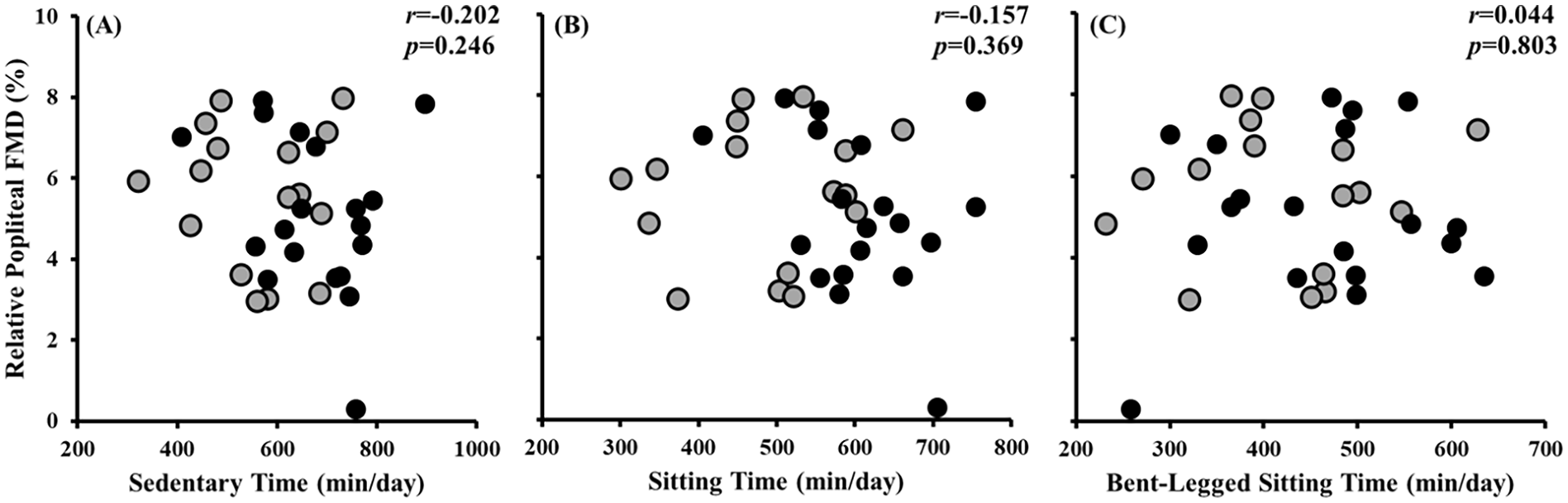
Pearson correlation between popliteal flow-mediated dilation (FMD) versus sedentary time
Discussion
We investigated the acute and chronic impact of knee-flexion angle during sitting on popliteal endothelial-dependent vasodilatory function in healthy young adults. Inconsistent with our hypotheses, knee-flexion angle did not influence the decline in popliteal FMD following a single bout of prolonged sitting. Similarly, neither time spent in bent-legged sitting, nor straight-legged sitting were associated with popliteal FMD responses in free-living conditions. Altogether, these observations demonstrate that leg position and the theorized magnitude of arterial ‘kinking’ do not influence the adverse vascular endothelial responses to sitting. Specifically, these findings suggest that sitting with straight legs does not provide protection to sitting-induced popliteal endothelial dysfunction.
Single bouts of prolonged sitting permit insight into the acute vascular responses to a sedentary posture. Our results are in contrast to another laboratory-based study that investigated the effect of a 3-hour bout of prolonged hip and knee flexion during a side-lying position with one leg bent (i.e., 90° angles at the hip and knee) and the contralateral leg straight (i.e., 0°, 90° angles at the hip and knee, respectively). 17 This previous study demonstrated that prolonged bending of the leg, but not prolonged straight-legged lying, caused reductions in popliteal FMD in young adults. 17 These divergent findings to the current investigation may be attributed to the differences in the sedentary posture used (i.e., side-lying versus sitting). Importantly, prolonged sitting is associated with a greater hydrostatic stress on systemic and popliteal hemodynamics during testing. Blood pooling in the lower legs is increased in the sitting versus lying posture due to hydrostatic forces 37 that contribute to reductions in blood flow and shear stress. 36 Specifically, hydrostatic pressure leads to lower-extremity venous pooling, and slower transit time through the venous circulation, which decreases venous return and stroke volume. 38 This decreased stroke volume and cardiac output leads to corresponding reductions in shear stress, the primary regulator of endothelial function.
Interestingly, sitting-mediated increases in venous pooling may provoke the venous distension reflex, whereby increased blood volume within the veins elicits a sympathoexcitatory pressor response. 39 Possibly, increased sympathetic vasoconstriction contributes to attenuated lower-limb FMD responses after sitting. Also, reductions in blood flow and shear stress contribute to established pathophysiological mechanisms (i.e., decreased nitric oxide bioavailability), which have been proposed to contribute to endothelial dysfunction using sitting models.40,41 Therefore, increased hydrostatic stress in the sitting posture may have contributed to attenuation across all knee angles. In support of this, the postsitting declines in blood flow and shear rate we observed were not different between knee angle conditions (all, p > 0.271; Table 1). Alternatively, low shear stress may increase production of endothelial-derived endothelin-1,42,43 a potent vasoconstrictor that may attenuate FMD responses. Nevertheless, our data refute that a possible mechanical deformation or ‘kinking’ of the popliteal artery with greater leg bending is a primary cause of popliteal endothelial dysfunction with sitting.
Laboratory models of prolonged sitting consistently demonstrate impaired endothelial-dependent vasodilatory function,10,14,21,26,29,41 but free-living models are less consistent. 20 Though the current laboratory-based study observed reductions in popliteal FMD following prolonged sitting, regardless of knee angle, the free-living study observed no associations between habitual time spent in sedentary postures and popliteal FMD. It has previously been documented that well-controlled, acute laboratory-based prolonged sitting studies have little ecological validity. 30 Specifically, younger adults rarely engage in uninterrupted bouts > 2 hours (i.e., only once every ~5 days). 30 While it is unlikely that participants engaged in prolonged sedentary bouts similar to those in the controlled laboratory environment, the stimulus (i.e., shear rate reductions) to elicit lower-limb endothelial dysfunction may not be sufficient. In addition, previous acute sitting studies have demonstrated that relatively short breaks in prolonged sedentary time (e.g., 5 minutes of walking) are effective in negating lower-limb FMD reductions. 29 In a free-living environment, sedentary breaks have also been positively correlated with popliteal endothelial function in young healthy adults. 20 Participants in the present study broke up their sitting ~3.1 times per waking hour (or every ~20 minutes) and averaged 10,000–12,000 daily steps (Table 3). Therefore, the breaks adults take in their habitual sedentary time, however brief, may have negated the endothelial dysfunction that is observed during controlled laboratory settings. Free-living settings may be limited to between-subject variability, but acute laboratory studies are useful for assessing the underlying mechanisms of sedentary postures. However, they may not translate to a free-living environment where posture and movement is not controlled or standardized. Our consistent observations, across both study designs, that knee-flexion angles did not impact popliteal FMD outcomes further strengthens the notion that the act of sitting, regardless of leg position, is detrimental to popliteal health.
Although lower-limb arteries are more susceptible to peripheral artery disease than upper-limb vessels, the popliteal artery may be the most susceptible. 44 This is the first study to investigate the prolonged impact of knee-flexion angle on popliteal FMD responses to an acute prolonged sitting bout, independent of hip flexion angle, with an attempt to translate these findings to the free-living environment. This study is further strengthened by the inclusion of objective, monitor-derived sedentary postures.
Inherently, the results of this study are limited to the popliteal artery, and it is unclear whether other cardiovascular outcomes may be altered by changing sedentary postures. However, popliteal artery function has clinically relevant outcomes 6 and has been well studied in the prolonged sitting literature. 15 In addition, this study also did not account for potential endothelial-independent mechanisms (i.e., vascular smooth muscle cell function) that may have contributed to the adverse vascular consequences associated with prolonged sitting. 16 Furthermore, despite including multiple study designs, whether long-term interventions that modify knee angle confer vascular benefits is unclear. This study is limited by a young and active (i.e., ~50 min/day moderate-to-vigorous physical activity) homogenous sample that may have preserved endothelial function despite accumulating > 10 hours/day of habitual sedentary activity. However, to our knowledge, this is the first study to investigate the acute and chronic impacts of knee-flexion angles during sitting on popliteal endothelial-dependent vasodilatory function. In adults with higher levels of peripheral artery disease, a higher level of calcification of the popliteal artery is associated with greater artery curvature and decreased axial length. 45 Therefore, future studies should investigate the effects of detailed sedentary postures in populations with vascular dysfunction (e.g., peripheral artery disease) or those confined to bed rest (e.g., hospital patients), whereby minor changes in leg position may be more efficacious in improving peripheral vascular function. 45
Conclusion
Overall, knee-flexion angle did not influence declines in popliteal artery FMD in response to a single bout of prolonged sitting, nor did time spent in knee-bent sitting in free-living conditions. In young healthy adults, leg bending is not a primary contributor to popliteal artery dysfunction following sitting and sitting with straight legs does not confer a healthier sitting posture. These results advance our understanding of habitual body positions on vascular function.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241238702 – Supplemental material for Sitting knee-flexion angle does not influence endothelial-dependent vasodilation in laboratory or free-living conditions
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241238702 for Sitting knee-flexion angle does not influence endothelial-dependent vasodilation in laboratory or free-living conditions by Madeline E Shivgulam, Myles W O’Brien, Yanlin Wu, Haoxuan Liu, Jennifer L Petterson, Beverly D Schwartz and Derek S Kimmerly in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Myles W O’Brien was supported by a CIHR Post-Doctoral Fellowship Award(#181747) and a Dalhousie University Department of Medicine University Internal Medicine Research Foundation Research Fellowship Award. Beverly D Schwartz and Jennifer L Petterson were supported by a Fredrick Banting and Charles Best CIHR Masters Award. Beverly D Schwartz and Madeline E Singlewire supported by Nova Scotia Graduate Scholarships. Madeline Shivlal was supported by a Heart & Stroke Bright Red Scholarship. Derek S Kimmerly received grants from the Canadian Foundation for Innovation: Leader’s Opportunity Fund, Faculty of Health Research Development, and Nova Scotia Health Research Foundation (NSHRF) Development/Innovation.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.