
Abstract
Background
Peripheral artery disease (PAD) affects 12–20% of Americans over 60 years of age. 1 The most severe form of PAD, chronic limb-threatening ischemia, has a 20–30% risk of lower-extremity amputation.2,3 Moreover, individuals who suffer limb loss have up to 50% 1-year mortality, 4 and the care of patients with major amputations is estimated to cost more than $9 billion (USD) annually. 5 Patients with PAD face significant socioeconomic barriers to health care, often lack healthcare insurance, and have difficulty accessing the healthcare system – all of which can lead to a higher risk of amputation.6,7 In particular, Medicare beneficiaries with PAD also face significant socioeconomic barriers due to incomplete or partial coverage. 8
To improve healthcare coverage for at-risk adults, in 2014 the Affordable Care Act (ACA) was enacted, which expanded Medicaid eligibility and led to an expansion in the number of dual Medicare/Medicaid eligible individuals. As a result, adults with an income level up to 138% of the federal poverty level became eligible for the Medicaid Expansion (ME) coverage, leading to an overall decline in the uninsured population by 46.5% in 2016. 9 This improved coverage led to an increase in the prescription of evidence-based cardiovascular medications, including statins, antihypertensives, and antihyperglycemic agents.10,11 Not all states adopted ME, but those states that did saw a significant decline in cardiovascular mortality compared to nonexpansion states, especially those deaths attributable to hypertensive heart disease and congestive heart failure.12,13
However, it is unclear whether ME has led to concomitant improvements in outcomes for patients with PAD. Published reports on this topic demonstrate conflicting results. ME appears to have improved access to peripheral vascular interventions, 14 but its impact on mortality and lower-extremity amputation is not well described. Elucidating whether ME has led to improved outcomes among patients with PAD would serve to inform resource allocation for targeted health policy interventions for this at-risk group. Therefore, the aim of this study was to measure the impact of ME on mortality and leg amputations among Medicare beneficiaries with PAD.
Methods
Data source and study population
We studied Medicare beneficiaries from 2011 through 2018. We used the 100% sample MedPAR (inpatient) and Part-B (outpatient) Carrier files from 2011 to 2018 and queried them to identify all fee-for-service Medicare beneficiaries during that interval. Next, we applied a list of International Classification of Diseases, Ninth Revision and Tenth Revision codes derived in prior work to identify beneficiaries with a diagnosis of PAD (online supplemental material).15 –17 We then limited the cohort to fee-for-service beneficiaries who met the following criteria: (a) coverage for at least 1 year during the interval; (b) US residents; (c) age 65 years or older; and (d) no missing data on mortality (online Supplemental Figure 1). The Dartmouth-Hitchcock Institutional Review Board approved the study and waived the need for consent.
Exposure
Our primary exposure was whether or not a state had adopted ME on January 1, 2014 (online Supplemental Table 1). States, including the District of Columbia, that adopted ME after this time were included in the sensitivity analysis listed below.
Primary outcomes
Our primary outcomes were change in 1-year all-cause mortality, and any leg amputation (major and minor) over the course of the study (2011–2018). We determined vital status using the Medicare Master Beneficiary Summary File. We defined leg amputation using a list of Healthcare Common Procedure Coding System codes that have been derived by our group and others (online Supplemental Figure 1).15 –17
Statistical analysis
We described continuous variables using means and SDs and compared them with t-tests. We described categorical variables as percentages and compared them with the chi-squared test. We calculated the percent of the cohort suffering mortality for each month of the study interval. We then compared these percentages across the exposure groups. We performed a state-level difference-in-differences (DID) analysis to compare the risk of mortality among beneficiaries from states who adopted ME versus those from states that did not adopt it. The estimates were adjusted for age, sex, race, geography (rural vs urban based on rural–urban commuting area codes), and comorbidities (atrial fibrillation, congestive heart failure, ischemic heart disease, hypertension, hyperlipidemia, history of transient ischemic attack or stroke, diabetes, anemia, hip fracture, dementia, chronic obstructive pulmonary disease, chronic kidney disease, malignancy, and obesity). We then repeated these analyses for the outcome of leg amputation. We conducted prespecified subanalyses of patients stratified by sex, race, geographical area (Northeast, Midwest, South, and West), Medicare/Medicaid dual eligibility, and after excluding states who adopted ME after April 1, 2014. We provided two-sided p-values and those below 0.05 were considered statistically significant.
Results
Characteristics of the cohort
We included 37,743,929 patients over the 8-year period, 18,587,572 in ME states and 19,156,357 in non-ME states (Table 1). Patients in ME states were older (mean ± SD age in ME states: 78.7 ± 8.4 vs non-ME states: 78.1 ± 8.2 years, p < 0.0001), more likely to be women (ME states: 55.1% vs non-ME states: 53.8%, p < 0.0001), Hispanic (ME states: 5.4% vs non-ME states: 4.4%, p < 0.0001), residing in an urban area (ME states: 89.1% vs non-ME states: 84.1%, p < 0.0001), and dual eligibile for both Medicare and Medicaid coverage (ME states: 23.3% vs non-ME states: 20.7%, p < 0.0001). Compared to patients in ME states, those in non-ME states were more likely to have a history of congestive heart failure, ischemic heart disease, hypertension, hyperlipidemia, chronic obstructive pulmonary disease, ischemic stroke or transient ischemic attack, and obesity (all p < 0.0001).
Baseline characteristics of patients in states with versus without Medicaid Expansion.
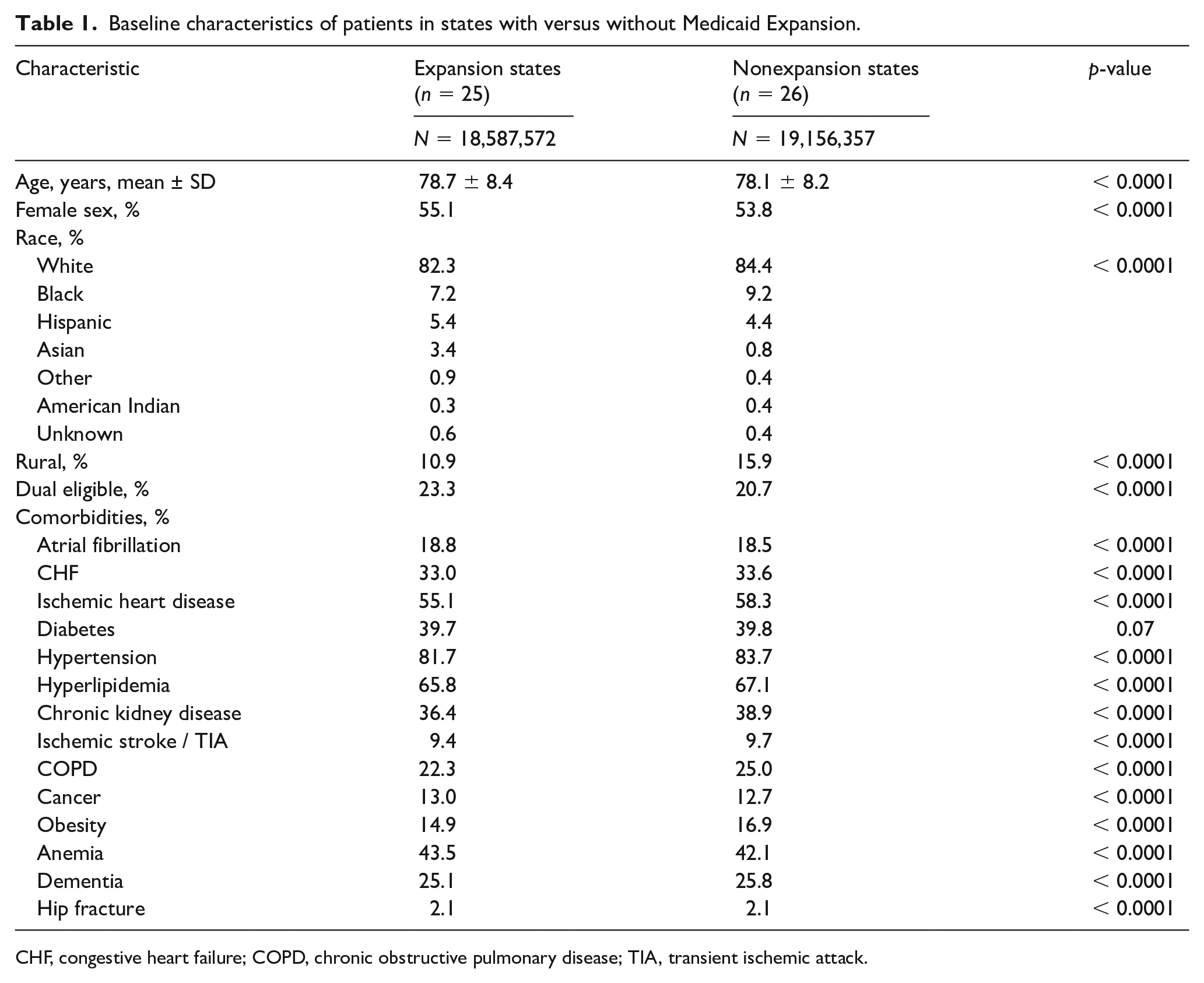
CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; TIA, transient ischemic attack.
Mortality in states with Medicaid Expansion (ME) versus non-ME states
The average unadjusted 1-year mortality decreased both in ME states from 9.10% in 2011 to 8.3% in 2018 (p < 0.001), and in non-ME states from 9.5% in 2011 to 8.7% in 2018 (p < 0.001) (Figure 1). Across the entire cohort, the adjusted DID model revealed that ME was not associated with a change in 1-year mortality (p = 0.15). Similar trends were observed when stratified by sex (Figure 2), race (Figure 3), and region (Figure 4). Trends were similar when stratified by dual-eligibility status or excluding states who adopted ME after April 1, 2014.
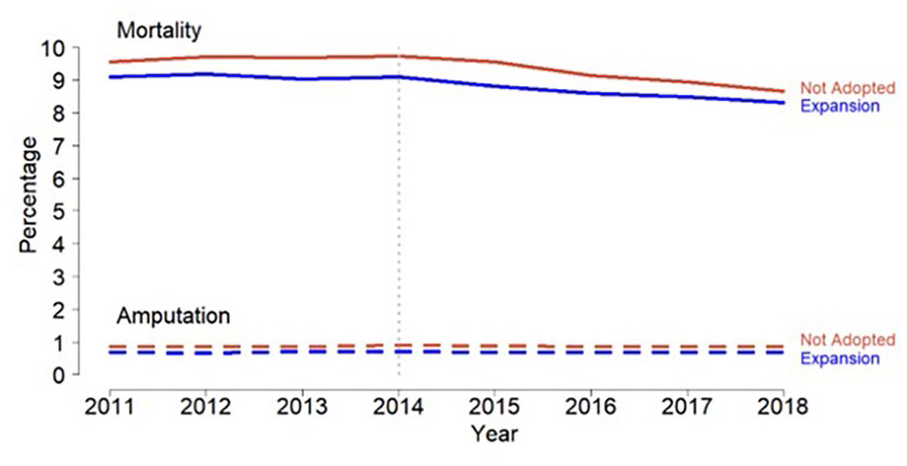
One-year mortality and amputation rates in Medicaid-Expansion versus non-Medicaid Expansion states.
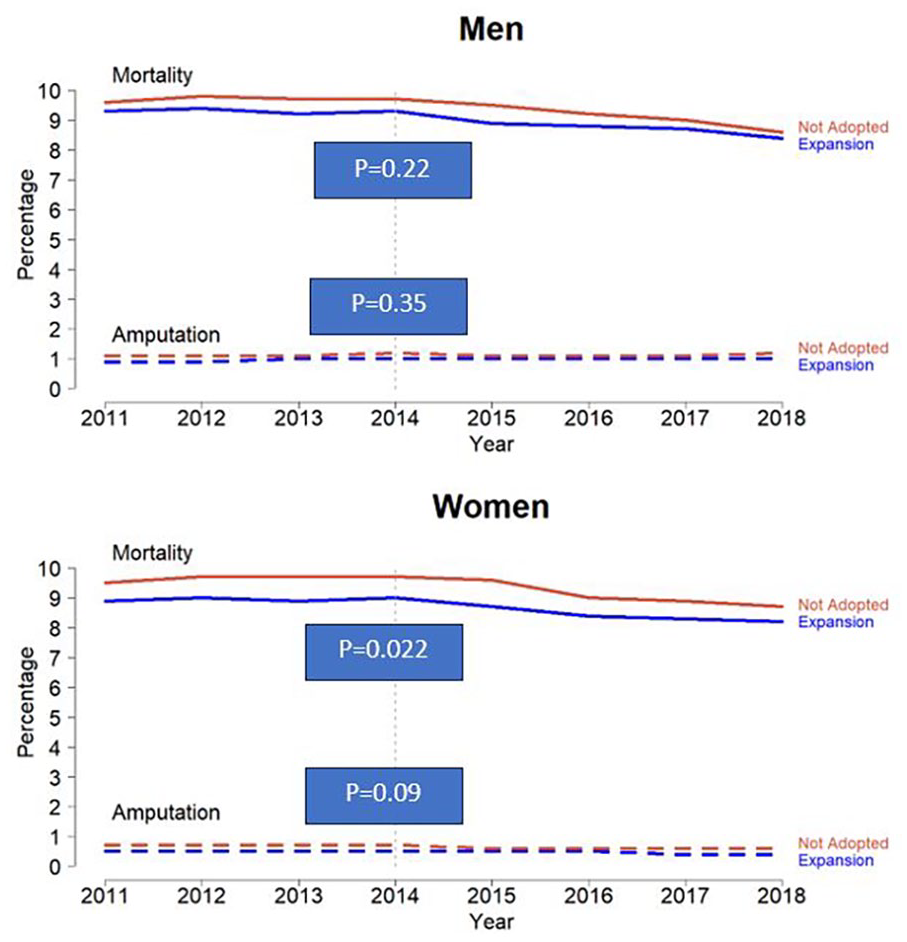
One-year mortality and amputation rates in Medicaid-Expansion versus non-Medicaid Expansion states stratified by sex.
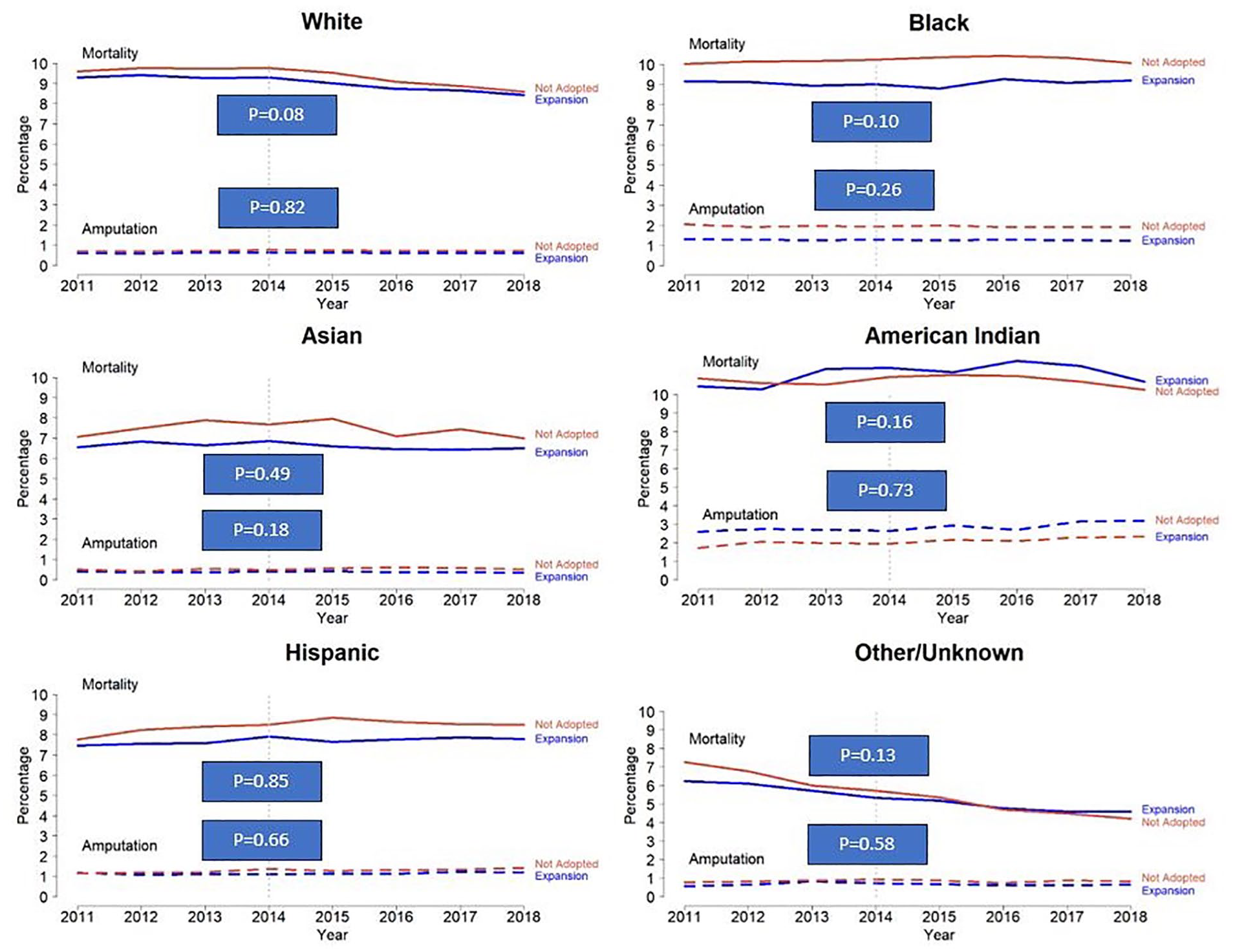
One-year mortality and amputation rates in Medicaid-Expansion versus non-Medicaid Expansion states stratified by race.
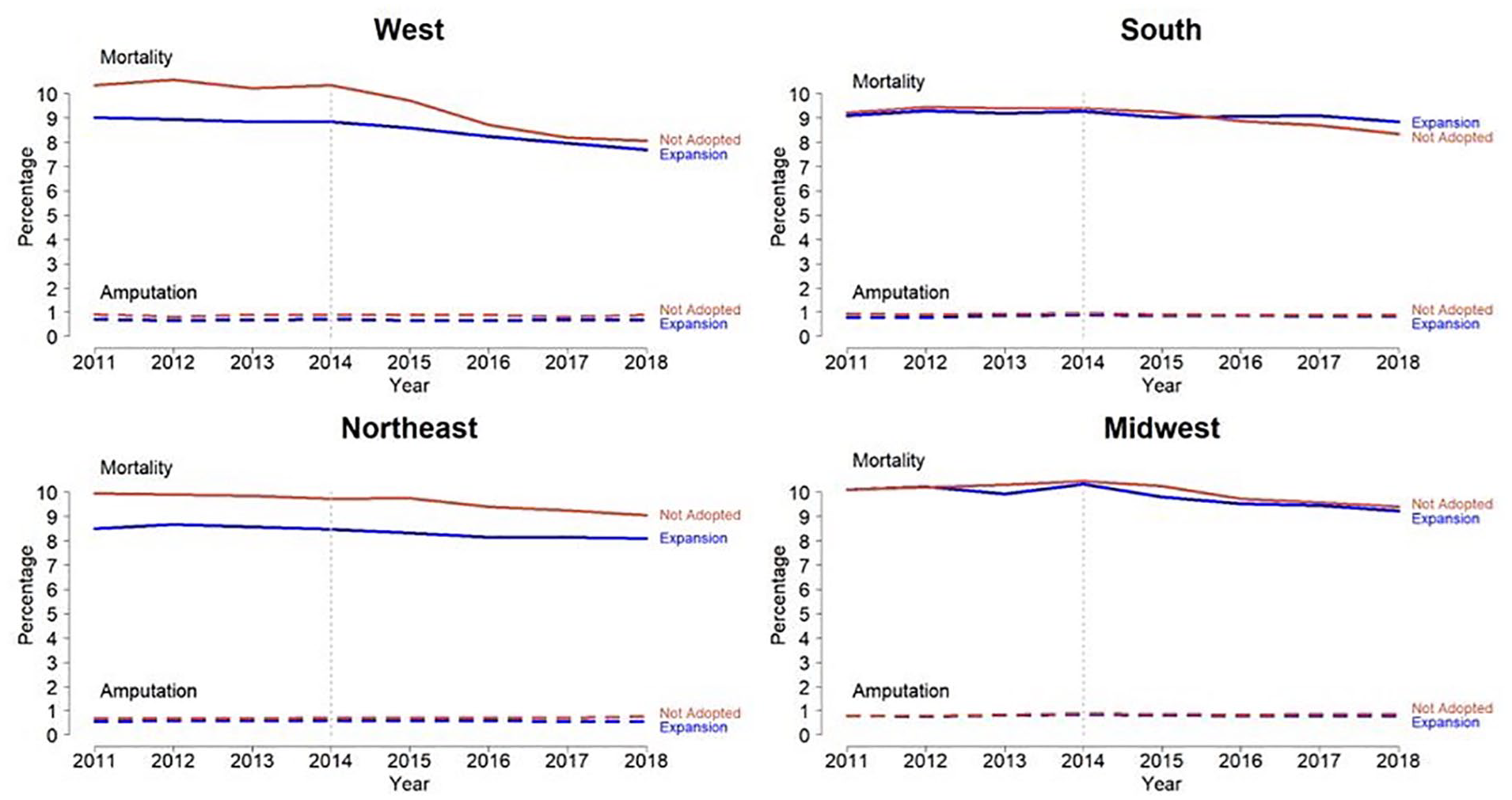
One-year mortality and amputation rates in Medicaid-Expansion versus non-Medicaid Expansion states stratified by region.
Amputation rates in ME versus non-ME states
The average unadjusted 1-year amputation rates remained unchanged over the study period in both ME states, from 0.69% in 2011 to 0.69% in 2018 (p = 0.65), and in non-ME states from 0.86% in 2011 to 0.87% in 2018 (p = 0.17) (Figure 1). Across the entire cohort, the adjusted DID model revealed that ME was not associated with a change in 1-year amputation (p = 0.34). Similar trends were observed when stratified by sex (Figure 2), race (Figure 3), region (Figure 4), or type of amputation (major vs minor; online Supplemental Figure 2) or excluding states who adopted ME after April 1, 2014. In patients with dual eligibility, the adjusted DID model revealed that 1-year amputation rates decreased significantly in men whereas the ME was associated with a 0.12% (95% CI: 0.02–0.30) decrease in amputation rates (p = 0.03), but no statistically significant difference was noted among women (p = 0.87).
Discussion
In this study of nearly 38 million Medicare beneficiaries with PAD, we found that the implementation of ME at the state level was not associated with a decrease in 1-year mortality or lower-extremity amputation. We found similar trends in subanalyses after stratifying by sex, race, and region. In patients with dual eligibility, ME was associated with a decrease in amputation rates only in men. Our findings build upon the existing evidence by employing a DID modeling technique, which may reduce unmeasured confounding. These findings indicate that though other studies have documented that the ME is associated with improvements in healthcare delivery,9 –13 these benefits do not appear to lead to measurable improvements in mortality and amputation rates among beneficiaries with PAD.
Signed into law on March 3, 2010, the ACA, a US federal statute, was designed to improve access to health care in people with low socioeconomic status, establish new health insurance marketplaces, and expand Medicaid eligibility for low-income adults. 9 States implementing ME saw a significantly greater increase in prescriptions of antihyperglycemic medications, including glucagon-like peptide 1 receptor agonists and sodium-glucose cotransporter 2 inhibitors, 10 with a significant reduction in hospitalizations for diabetic ketoacidosis, 18 and improvement in glucose control. 19 Similar trends were seen with cardiovascular prescriptions, including statins, antihypertensives, and P2Y12 inhibitors, 11 and with improved access to smoking-cessation treatments. 20 Importantly, although a significant increase in antihyperglycemic and cardio-vascular prescriptions was seen in both ME and non-ME states, the number of prescriptions was significantly higher in ME versus non-ME states, as evaluated with DID analysis.10,11 Moreover, ME has been associated with improvement in hypertension control, 19 and 4 per 100,000 fewer deaths due to cardiovascular mortality, 13 especially due to hypertensive heart disease and congestive heart failure. 12 Despite improved access to health care, including a significant decrease in the proportion of uninsured hospitalizations for myocardial infarction, stroke, and heart failure in ME states, ME has not been associated with improved in-hospital all-cause mortality.21 –23
Conversely, published reports of whether ME has led to improvements among patients with PAD have shown conflicting results. ME has been associated with improved access to vascular procedures, including elective lower-extremity revascularization, 24 as well as lower in-hospital mortality and 1-year incidence of repeat procedures or major amputation among patients who underwent surgery. 14 The association with amputation is less clear. Although ME was associated with a decreased rate of amputations in Arkansas, 25 ME was not associated with a decrease in amputation rates or increased utilization of vascular procedures in New York or Arizona. 26 This is consistent with our nationally representative study of patients with PAD in which ME was not associated with a decrease in all-cause mortality or amputation, even when stratified by sex, race, or region.
We performed a subanalysis of patients who had dual eligibility for Medicare and Medicaid, a high-risk subgroup of Medicare patients. One prior study comparing dual-eligible beneficiaries to the general Medicare population undergoing peripheral vascular intervention for critical limb-threatening ischemia found higher rates of major amputation and death among dual-eligible patients. 27 This suggests that these patients continue to suffer from delayed diagnosis and treatment, despite improved access to health insurance. We found that in the subset of dual-eligible patients with PAD, ME was not associated with lower mortality, even when stratifying by sex or race. Although ME was not associated with overall lower rates of amputation, men in states with ME saw a decline in rates of amputation compared to men in non-ME states, although this finding was not seen in women. A reason for this finding may be due to the discrepancy in PAD care for men and women, as women are significantly less likely to receive guideline-directed medical therapy 28 or undergo revascularization for PAD. 29
We found that ME was not associated with improved survival or decreased amputation when stratified by region or by urban/rural area. In prior studies, individuals in rural areas and with lower socioeconomic status had a significantly higher risk of amputation due to PAD compared to those in urban areas and with higher socioeconomic status,27,30 despite receiving similar care (imaging and medications) after diagnosis of PAD. 27 This effect has been shown to be amplified in non-White patients. 31 This is thought to be due to delayed access to health care due to lack of insurance coverage. In 2008, Oregon introduced a limited expansion of the Medicaid program by randomly choosing 30,000 eligible individuals, providing an opportunity to evaluate health outcomes of individuals with and without ME. 32 This experiment resulted in improved access to healthcare services and reduced financial strain equally among the urban and rural populations. 33 After ME was enacted, insurance coverage improved significantly in the rural population, especially among low-income childless adults. 34
Our results showing that ME was not associated with reduced mortality or amputation for Medicare beneficiaries indicate that there is further work to be done to improve outcomes among Medicare beneficiaries with PAD. Despite improvement in their access to health care, patients with PAD, compared to other disease processes (i.e., hypertension, diabetes, coronary artery disease), do not appear to have enjoyed the same benefits of improved outcomes. The etiology of these findings is yet to be elucidated but certainly is influenced by the fact that individuals with PAD are less likely to receive secondary prevention therapies compared to those with cardiac disease. 35 Importantly, among Medicare beneficiaries undergoing major amputation for chronic limb-threatening ischemia, more than 60% did not undergo an angiogram or revascularization in a year preceding the amputation. 36 This suggests that a multifaceted approach is necessary to improve outcomes in patients in PAD – not only at the policy level but also at the individual health system level. Focus on timely diagnosis of PAD and institution of secondary prevention measures that are known to improve outcomes is paramount.
Limitations
Our study has several limitations. As Medicare data are designed for billing, it can be difficult to identify true clinical events from claims codes. However, we have previously validated claims data directly against patient chart review and telephone interviews in several studies.15 –17 Therefore, we believe the results obtained in this analysis should be accurate. Next, the DID analysis is limited by the assumptions imposed on the model. For this case, the assumption is that states who adopt ME offer it to all patients with PAD who are eligible. Given that Medicare billing claims data were used in the analysis, it is reasonable to assume that patients who qualify will have been offered ME to improve billing and reimbursement. Furthermore, this type of analysis is specifically designed to evaluate policy changes over time. 37 Additionally, we studied 1-year change in outcomes, which may be too short to see a change in rates of mortality and amputation. Finally, our study did not include patients who were not Medicare eligible (i.e., uninsured patients who received Medicaid as part of ME). However, ME provides dual eligibility for individuals with incomes up to 138% of the federal poverty level, who would receive benefits that may not be otherwise covered by Medicare; or that an individual may not afford.
Conclusions
Medicaid Expansion is not associated with reduced mortality or leg amputation in Medicare beneficiari-es with PAD. Although this policy intervention has improved outcomes for other disease processes, patients with PAD do not appear to have derived the same beneficial impact.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X241237776 – Supplemental material for The impact of the Affordable Care Act Medicaid Expansion in Medicare beneficiaries with peripheral artery disease
Supplemental material, sj-docx-1-vmj-10.1177_1358863X241237776 for The impact of the Affordable Care Act Medicaid Expansion in Medicare beneficiaries with peripheral artery disease by Stanislav Henkin, Stephen A Kearing, Pablo Martinez-Camblor, Nikolaos Zacharias, Mark A Creager, Michael N Young, Philip P Goodney and Jesse A Columbo in Vascular Medicine
Supplemental Material
sj-jpg-1-vmj-10.1177_1358863X241237776 – Supplemental material for The impact of the Affordable Care Act Medicaid Expansion in Medicare beneficiaries with peripheral artery disease
Supplemental material, sj-jpg-1-vmj-10.1177_1358863X241237776 for The impact of the Affordable Care Act Medicaid Expansion in Medicare beneficiaries with peripheral artery disease by Stanislav Henkin, Stephen A Kearing, Pablo Martinez-Camblor, Nikolaos Zacharias, Mark A Creager, Michael N Young, Philip P Goodney and Jesse A Columbo in Vascular Medicine
Supplemental Material
sj-jpg-2-vmj-10.1177_1358863X241237776 – Supplemental material for The impact of the Affordable Care Act Medicaid Expansion in Medicare beneficiaries with peripheral artery disease
Supplemental material, sj-jpg-2-vmj-10.1177_1358863X241237776 for The impact of the Affordable Care Act Medicaid Expansion in Medicare beneficiaries with peripheral artery disease by Stanislav Henkin, Stephen A Kearing, Pablo Martinez-Camblor, Nikolaos Zacharias, Mark A Creager, Michael N Young, Philip P Goodney and Jesse A Columbo in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the Department of Medicine Scholarship Enhancement in Academic Medicine Award Pro-gram, Dartmouth-Hitchcock Medical Center. Dr Columbo was supported by the NIH/NHLBI (award number: K08HL165087) and the Society for Vascular Surgery.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.