
Abstract

Raynaud’s phenomenon (RP) reflects episodic digital vasospasms primarily related to cold exposure. Primary Raynaud’s is a relatively common ailment without a clear cause, affecting close to 5% of the general population, but is generally self-limited and does not result in tissue loss. 1 However, secondary Raynaud’s is often associated with a more severe clinical sequelae driven by an underlying process, most commonly a connective tissue disorder, and can result in digital ulceration or gangrene in the most advanced forms. 2 Conservative measures and oral vasodilators are the mainstay of therapy for RP; however, there are little data, guidance, or understanding of practices for more severe cases of RP.3,4
To further evaluate practice patterns for patients with severe RP, we analyzed all hospitalized patients with a diagnosis of RP in the Nationwide Readmission Database (NRD) from 2016 to 2020 to evaluate associations and outcomes in a nationwide cohort (see online supplemental material). Additionally, with institutional review board approval, we reviewed an internal registry of hospitalized patients evaluated by our multidisciplinary team, which was formed in 2020. Consults are placed to the vascular medicine consult service and additional members of the team, including rheumatology, hand surgery, and pulmonary hypertension, are involved on the specific patient’s needs. Patients were included in this analysis if vasospasm was clinically believed to be a significant component of their digital ischemia.
In a review of the NRD, 4056 patients were admitted with a diagnosis of RP. Baseline characteristics and outcomes are noted in Table 1. The majority had an underlying connective tissue disease (69.8%) and a high prevalence of cardiovascular risk factors including tobacco use (41.3%), hypertension (36.1%), and diabetes mellitus (20.9%). Angiograms were rarely performed, particularly of the upper extremities. Sympathectomy was performed in only 1% of patients. Hand/finger amputation occurred in 8.7% and foot/toe amputation in 9.7%. After performing multivariable logistic regression, factors associated with amputation included diabetes, peripheral artery disease, tobacco use, anemia, hypertension, and CREST (calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia syndrome) (online supplemental Table 1).
Demographics and disease characteristics of patients admitted with Raynaud’s phenomenon in the Nationwide Readmissions Database from 2016 to 2020 (N = 4056).
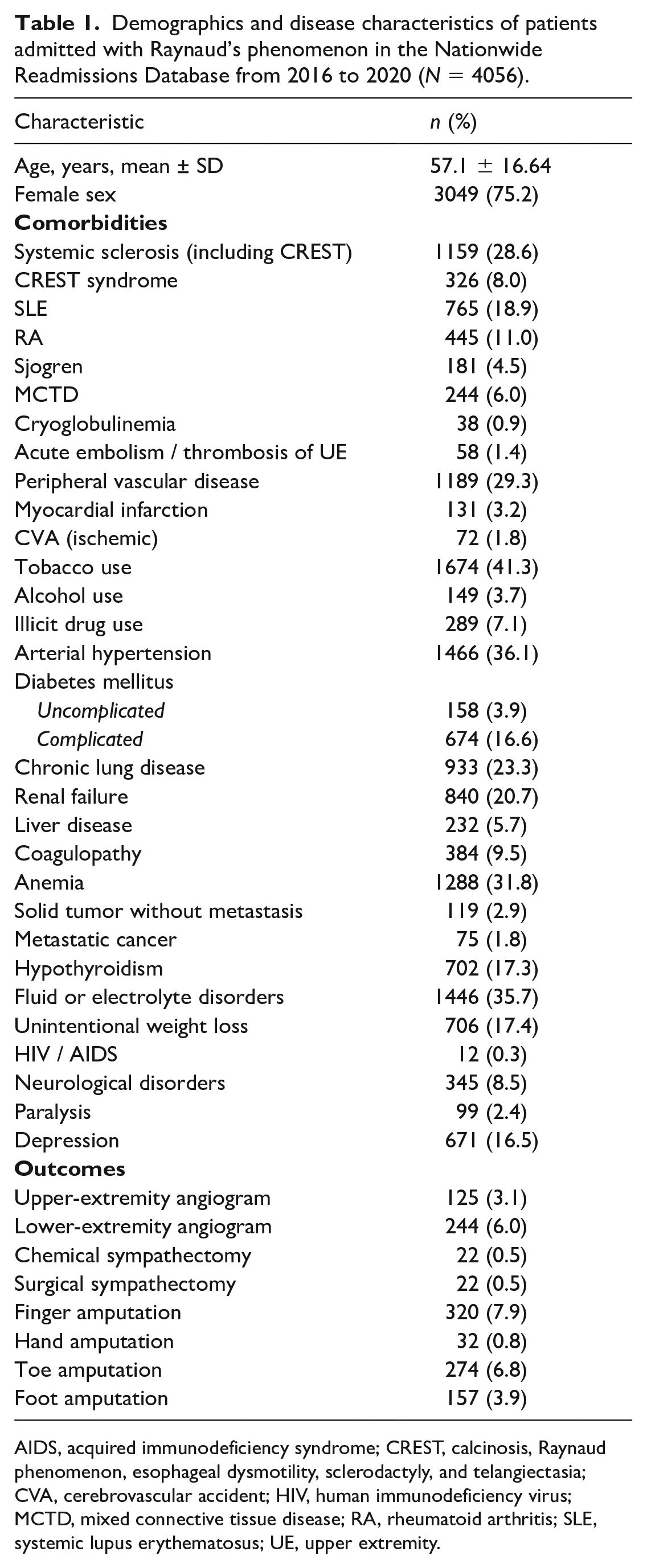
AIDS, acquired immunodeficiency syndrome; CREST, calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia; CVA, cerebrovascular accident; HIV, human immunodeficiency virus; MCTD, mixed connective tissue disease; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; UE, upper extremity.
In a review of our institutional registry, vascular medicine was consulted on 23 inpatients with RP or suspected RP from January 2020 through June 2023. Patients had an average age of 54 ± 13.8 years and 15 (65%) of the patients were women. Comorbidities included 16 (70%) with a prior diagnosis of a connective tissue disease, 10 (43%) with hypertension, five (22%) with type 2 diabetes mellitus, five (22%) with hyperlipidemia, and only one patient with peripheral artery disease. An invasive angiogram was performed in seven (30%). Advanced therapeutic interventions included eight (35%) patients who received intravenous vasodilators, four (17%) who underwent chemical sympathectomy, and three patients who underwent amputation.
In a nationwide cohort, hospitalization for RP is frequently associated with an underlying connective tissue disease and high rate of smoking. Nearly 20% of patients underwent amputation, but rarely had an angiogram performed during the same hospitalization. There is no billing code for intravenous vasodilator administration, so this could not be evaluated in the NRD, but was utilized in one-third of our patients. The role of sympathectomy is poorly defined in such patients, but is a consideration in those with advanced disease despite maximally tolerated medical therapy. Chemical sympathectomy confers overall low risk for complications. In small studies it has demonstrated improvement in perfusion, 5 but in randomized trials has not demonstrated benefit in patients with systemic sclerosis. 6 Sympathectomy was rarely performed nationally, though our group was more aggressive and performed this for patients with refractory ischemia. Additionally, angiograms were performed in a small minority of patients nationally. We more frequently perform angiography as a means to exonerate alternative contributors to digital ischemia, evaluate vasodilator response with administration of intra-arterial nitroglycerin, and better define digital artery anatomy.
The most notable limitation of our study is the inability to verify diagnoses and outcomes utilizing an administrative claims-based dataset like the NRD. It is possible that patients underwent amputation due to concomitant PAD, leading to an overestimate of the amputation rate. Most RP is managed as an outpatient, and as such, we also captured a unique population with severe manifestations. Additionally, our institutional experience was limited to patients in whom the vascular medicine service was consulted and to our unique team-based approach.
Given the relative infrequent nature of severe RP presentations and significant risk of amputation, with a dearth of evidence to guide optimal management, a multidisciplinary team with involvement of vascular medicine specialists at tertiary centers may be the most appropriate care model for such patients. As has been recommended for other vascular diseases like pulmonary embolism and acute aortic syndromes, 7 a multidisciplinary team approach allows exchange of ideas and increased experience with a unique set of specialists in an attempt to decrease the amputation rate and optimize short- and long-term outcomes. Further studies are warranted to evaluate optimal care for advanced RP and the role of a multidisciplinary team approach for improved clinical outcomes and the cost implications for such an approach Like many other vascular disease states, RP lacks a clear optimal approach to management. Vascular medicine specialists are well-positioned to lead multidisciplinary efforts to optimize care for complex RP.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X231220609 – Supplemental material for Advanced Raynaud’s disease: A vascular medicine-initiated team-based approach and nationwide cohort analysis
Supplemental material, sj-docx-1-vmj-10.1177_1358863X231220609 for Advanced Raynaud’s disease: A vascular medicine-initiated team-based approach and nationwide cohort analysis by Milan Kaushik, Sebastian E Beyer, Jennifer Nashel, Cyrus Kholdani, Arriyan S Dowlatshahi, Eric A Secemsky and Brett J Carroll in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Brett Carroll: Bristol Myers Squibb, institutional research support; Koya Medical, scientific advisory board. Eric Secemsky: research grants to BIDMC (Beth Israel Deaconess Medical Center): NIH/NHLBI K23HL150290, Food & Drug Administration, SCAI, BD, Boston Scientific, Cook, Abbott/CSI, Laminate Medical, Medtronic and Philips; consulting/speaking: Abbott/CSI, BD, Boston Scientific, Cook, Cordis, Heartflow, InfraRedx, Medtronic, Philips, RapidAI, Shockwave, and VentureMed. The remaining authors with no disclosures.
Funding
This study was supported by a Building the Evidence Base for Vascular Medicine Award from the Society for Vascular Medicine.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.