
Abstract

Keywords
What is Raynaud’s phenomenon?
Also called Raynaud’s disease or syndrome, Raynaud’s phenomenon is a blood vessel condition in which a person’s fingers or toes change colors. Raynaud’s phenomenon is named after the French physician (Dr Maurice Raynaud) who first described this condition. In Raynaud’s phenomenon, the fingers or toes may first turn white and/or bluish, particularly in cold temperatures. With rewarming, the fingers or toes may then turn red. The condition is often referred to as ‘primary’ or ‘secondary’ Raynaud’s. With primary Raynaud’s, there is no associated cause or explanation for the condition. Secondary Raynaud’s is due to other medical problems or other causes of spasm in the blood vessels.
When fingers and toes are exposed to cold temperatures, the blood vessels normally constrict, or become narrow, in order to conserve body heat. This process is called vasoconstriction. In the case of Raynaud’s, the vasoconstriction is excessive and is called vasospasm because there is such a dramatic reduction in blood flow. During the white phase, no blood flow is getting to the fingers or toes because of the spasm in the blood vessels. Subsequently, the tiny blood vessels dilate and are filled with blood that has no oxygen, which causes the fingers or toes to turn blue. Finally, the red phase occurs due to the dramatic increase in blood flow that happens after the spasm resolves when warmth returns. Not everyone with Raynaud’s will see all three of these color changes.
Who is at risk and what causes Raynaud’s?
Primary Raynaud’s is most common among young women. Overall, women are affected five times more often than men, and the onset is usually before age 30. The exact cause of primary Raynaud’s is not known (‘idiopathic’). Table 1 lists several of the causes of secondary Raynaud’s. For example, Raynaud’s is quite common in patients with scleroderma. It is also seen in patients with lupus (systemic lupus erythematosus or SLE), rheumatoid arthritis, and other autoimmune (rheumatologic) conditions. Some medications may cause secondary Raynaud’s. Secondary Raynaud’s may be suspected if the onset occurs later in life (particularly in a man) or if the symptoms are only in one hand or foot.
Some causes of secondary Raynaud’s phenomenon.
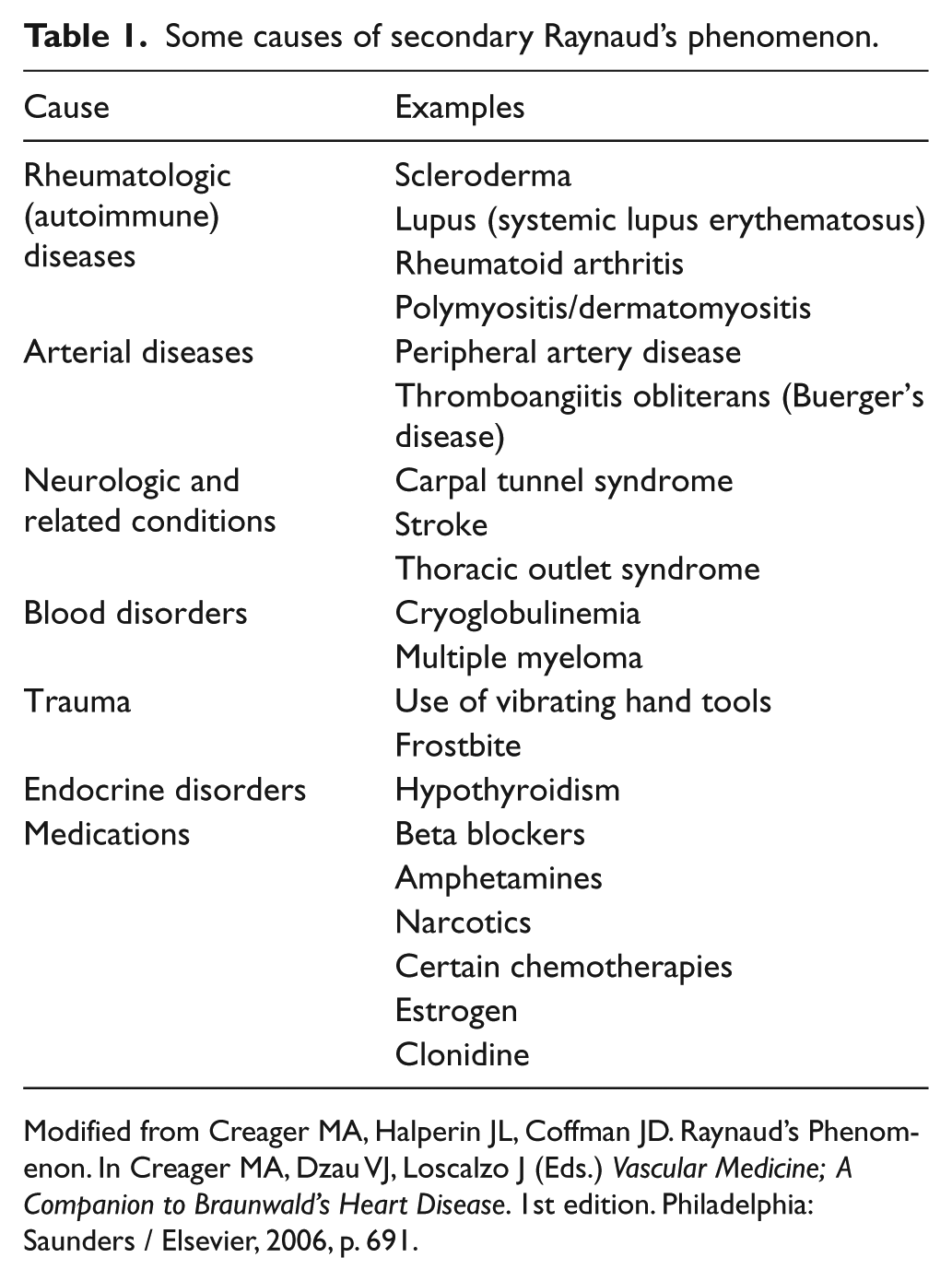
Modified from Creager MA, Halperin JL, Coffman JD. Raynaud’s Phenomenon. In Creager MA, Dzau VJ, Loscalzo J (Eds.) Vascular Medicine; ACompanion to Braunwald’s Heart Disease. 1st edition. Philadelphia: Saunders / Elsevier, 2006, p. 691.
What are the signs and symptoms of Raynaud’s?
A typical episode of Raynaud’s begins with the sudden onset of cold fingers with color changes. The symptoms are usually provoked by exposure to cold temperatures or emotional stress. Holding a cold drink or picking up frozen food or walking into the cold section of a grocery store may trigger an episode.
Figure 1 illustrates what fingers look like during the white phase. When the fingers or toes are white or blue, the symptoms may include a dull ache, discomfort, numbness, tingling, a pins and needles sensation, or a feeling of intense cold in the fingers. During the red phase, throbbing may occur. With primary Raynaud’s, symptoms usually develop in the fingers first and may only involve one or two fingers. Later, it may involve other fingers as well. The thumbs are generally spared in primary Raynaud’s. About 40% of people with Raynaud’s will also have symptoms in their toes.

Raynaud’s phenomenon in a young woman with primary Raynaud’s. The second, third, and fourth fingers appear white due to vasospasm (the ‘white phase’). The thumb and small finger are spared.
In the doctor’s office, the fingers may look completely normal in between episodes though the fingers or toes may be cool or clammy. The pulses should be normal. In a small number of people with primary Raynaud’s, the skin may thicken or tighten but ulcers or sores do not occur. With secondary Raynaud’s, the skin may be abnormal, with sores, pitting scars, or even gangrene of the fingers or toes in rare cases. The frequency and severity of the symptoms may be worse in patients with secondary Raynaud’s.
How is Raynaud’s diagnosed?
Primary Raynaud’s is usually diagnosed based on symptoms. Tests can be done in the vascular ultrasound laboratory to measure blood flow, but these tests are generally not necessary unless another artery problem (such as peripheral artery disease) is suspected. With a test called nailfold capillary microscopy, the tiny blood vessels under the fingernails are examined under a microscope.
Depending on the situation, blood tests may be ordered to help determine whether the Raynaud’s is primary or secondary. A commonly ordered blood test is the ANA, or antinuclear antibody test. In primary Raynaud’s, the ANA is negative or normal. However, having a positive or abnormal ANA does not necessarily mean that a rheumatologic or autoimmune condition is present. Other blood tests may include the erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP) if inflammation is suspected. Additional blood tests are tailored to the individual’s symptoms.
What are the risks of having Raynaud’s?
The prognosis for primary Raynaud’s is excellent. Other than the bothersome symptoms, there is no significant health risk of having primary Raynaud’s. Skin changes on the fingers are relatively rare. With secondary Raynaud’s, the risk of skin problems is higher. There are often risks associated with the underlying condition that caused the Raynaud’s (such as lupus). In some cases, a patient is initially thought to have primary Raynaud’s but then, years later, an autoimmune condition develops.
How is Raynaud’s treated?
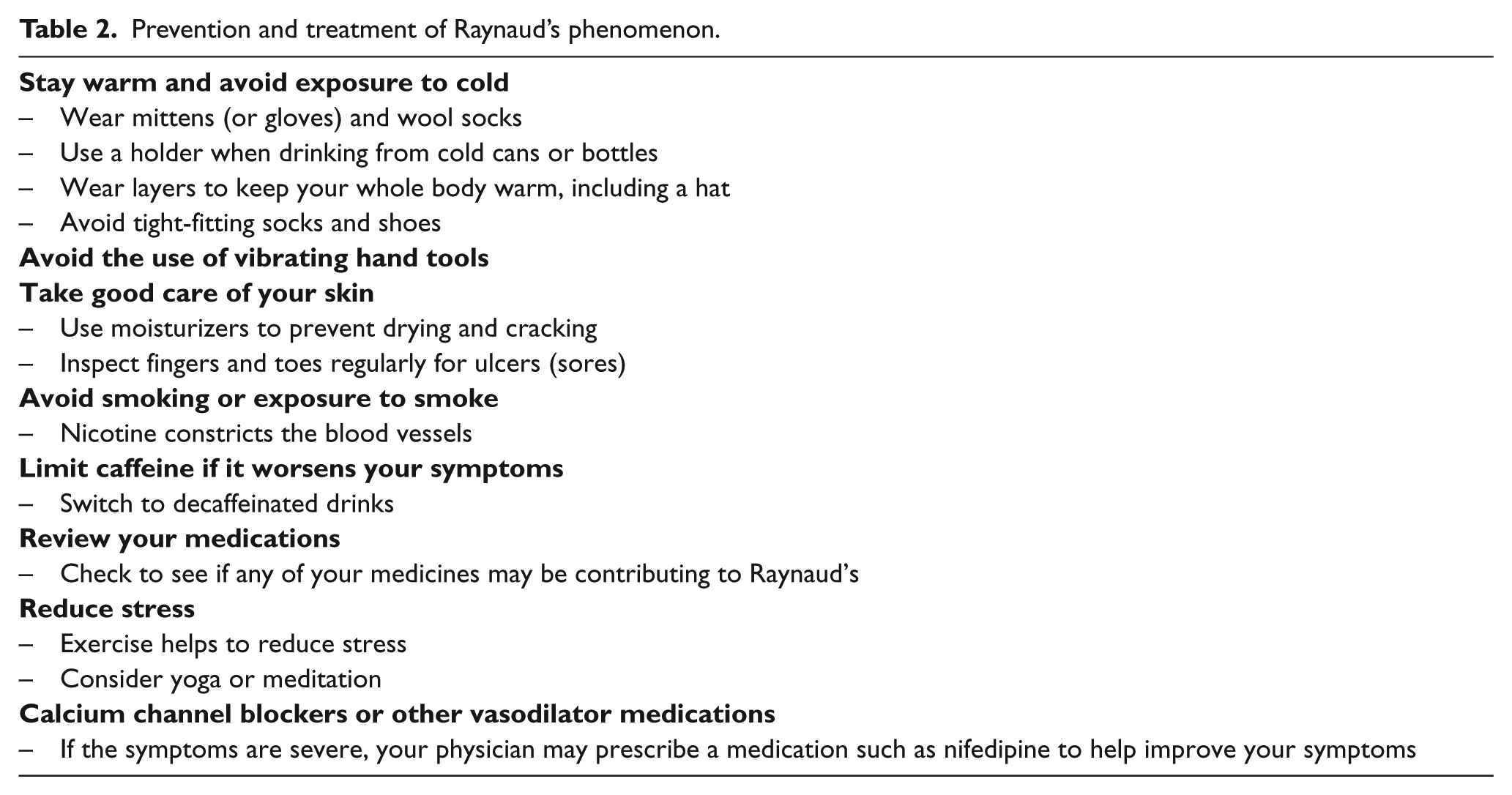
Avoiding exposure to cold temperatures is the most important aspect of the treatment of Raynaud’s. The entire body should be kept warm. If a secondary cause is found, then the treatment should be directed to that problem. For example, if the Raynaud’s is due to a medication, it should be stopped if possible to see if the symptoms go away. Or if thyroid function is underactive, treatment with thyroid hormone replacement may help. Table 2 lists several ways to help prevent Raynaud’s episodes. Most people with Raynaud’s do not require medication, and they are able to manage their symptoms through keeping warm, avoiding smoking, limiting caffeine, and reducing stress. In severe cases, the most commonly prescribed class of medications is calcium channel blockers such as nifedipine, although other vasodilator medications may be prescribed.
Prevention and treatment of Raynaud’s phenomenon.
Summary
Raynaud’s phenomenon is common, particularly among young women. Symptoms include color changes in the fingers or toes upon exposure to cold. In primary Raynaud’s, no cause is found, but patients with secondary Raynaud’s may have other medical conditions. The cornerstone of treatment for Raynaud’s is avoiding exposure to cold. Several lifestyle changes can reduce the frequency of episodes. Calcium channel blockers may be used if the symptoms are severe.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.