
Abstract

Keywords
What is spontaneous coronary artery dissection (SCAD)?
The heart is the pumping organ of the circulatory system. The coronary arteries are the blood vessels that supply oxygen and nutrient-rich blood to the heart. Blockage of a coronary (heart) artery can lead to a heart attack (myocardial infarction). These artery blockages are usually caused by atherosclerosis, or plaque build-up in the arteries. Spontaneous coronary artery dissection, commonly referred to as SCAD, is another cause of heart attack. SCAD is
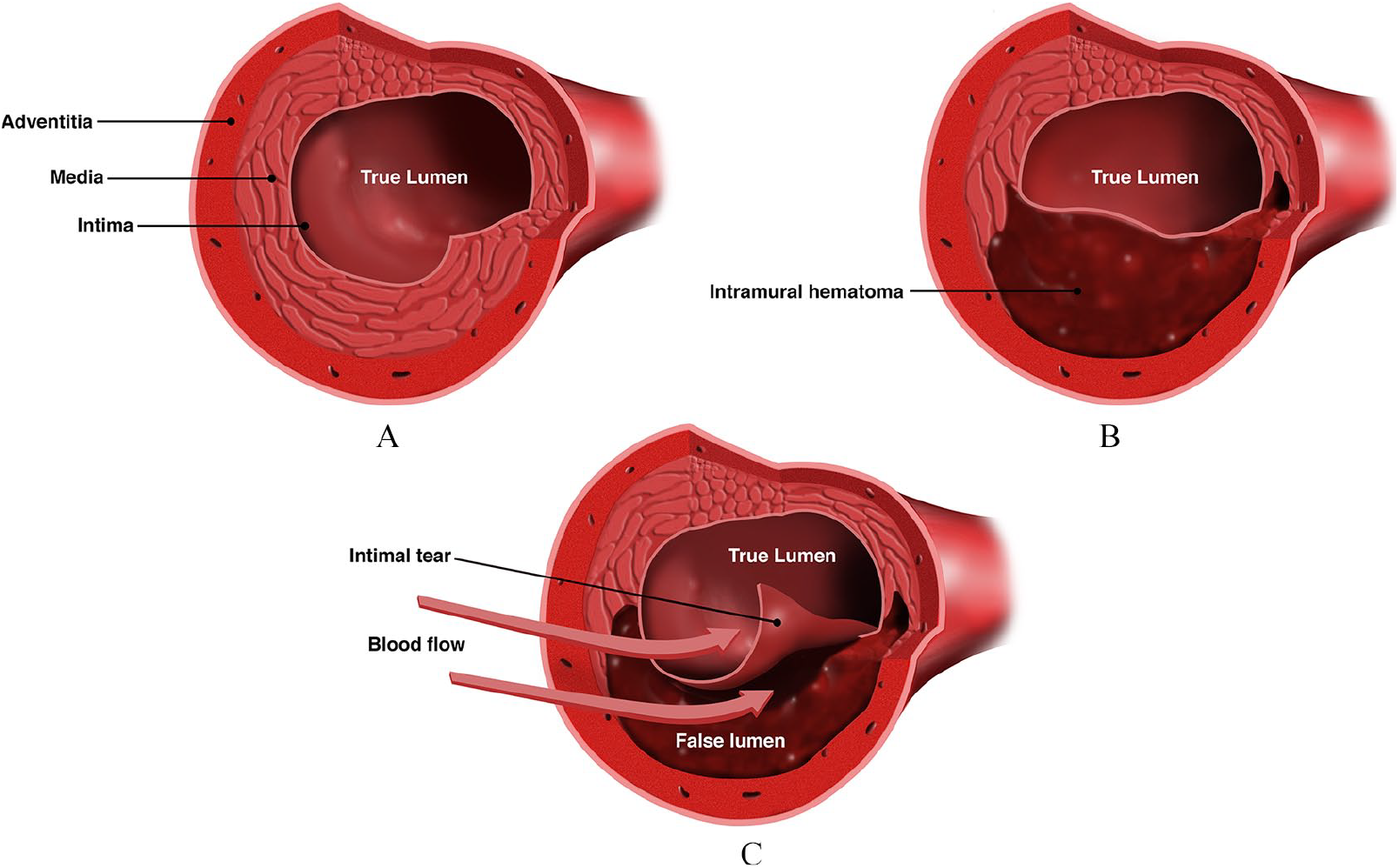
Diagram of SCAD causing sudden narrowing of a coronary artery. (A) Normal coronary artery in cross-section. The artery has three layers (intima, media, adventitia). (B) SCAD due to bleeding into the artery wall (intramural hematoma). (C) SCAD due to a tear of the inner lining of the artery wall (intimal tear). In both types of SCAD in (B) and (C), there is a narrowing of the true lumen of the artery, which is the portion of the artery that carries blood flow to the heart muscle.
What arteries are involved in SCAD?
In most people, there are three major coronary artery branches that supply blood flow to different parts of the heart muscle. These three arteries are the left anterior descending coronary artery (LAD), the left circumflex coronary artery (LCX), and the right coronary artery (RCA). The LAD and the LCX both arise from the left main coronary artery. Any coronary artery or its branches can be involved in SCAD; however, the most common artery affected is the LAD, which supplies blood to the front (anterior) part of the heart. 1 Other coronary artery branches may also be affected by SCAD, and more than one vessel may be affected by SCAD at the same time. The location of the arteries affected by SCAD and the severity of the blockage(s) determine the severity of symptoms and the extent of the heart attack.
What are the risk factors for SCAD?
As discussed below, several potential risk factors and predisposing conditions may lead to the development of SCAD. In contrast to heart attacks related to plaque or atherosclerosis, many of the usual cardiovascular risk factors, such as high cholesterol, diabetes, and tobacco smoking, are not significant risk factors for SCAD. In rare cases, SCAD may be precipitated by heavy physical exertion or extreme emotional upset. Research has shown that SCAD does not follow predicted inheritance patterns in families. Very few patients with SCAD have a family member who has also had SCAD. That being said, certain rare genetic (inherited) vascular diseases, such as the vascular type of Ehlers–Danlos syndrome, may be associated with SCAD. 1
Fibromuscular dysplasia (FMD) and other vascular abnormalities
SCAD may be a sign of an underlying vascular disease. In the past decade, researchers have identified a link between SCAD and the uncommon artery disease known as fibromuscular dysplasia (FMD). FMD is a nonatherosclerotic vascular disease that can cause narrowing, aneurysms, or dissections in arteries throughout the body. 2 With the common type of FMD, blood vessels look like ‘beads on a string’, which is known as multifocal FMD. Research has found that up to a half or more of patients with SCAD will have FMD when the other arteries outside of the heart are imaged.1,3–5 In addition to FMD, patients who have had SCAD are also more likely to have other vascular abnormalities outside of the heart, including important and potentially dangerous abnormalities such as brain aneurysms.1,5
Pregnancy-related SCAD
SCAD may occur during pregnancy or in the initial weeks after delivery. SCAD is the most common cause of heart attack during pregnancy; however, pregnancy-related SCAD is an uncommon form of SCAD overall. 1 The cause of pregnancy-related SCAD is not well understood but may be related to hormonal changes that can weaken the artery walls, changes in blood pressure, and/or changes in blood volume with pregnancy and delivery. Studies have shown that patients with pregnancy-related SCAD have worse outcomes, including a greater degree of heart muscle damage and a higher likelihood of having multiple coronary artery dissections than patients who have SCAD unrelated to pregnancy. 6
What are the symptoms of SCAD?
When SCAD occurs, it causes a heart attack. Thus, the symptoms of SCAD are those commonly associated with heart attack, including: pain, pressure or tightness in the chest, which may also travel to the neck/jaw or arms/shoulders (angina); trouble breathing; nausea and/or vomiting; or excessive sweating with no clear cause. In severe cases, patients may experience dizziness or pass out due to an abnormal heart rhythm and low blood pressure.
How is SCAD diagnosed?
Anyone experiencing symptoms of a heart attack should seek immediate medical attention by activating emergency medical services (i.e., dialing 911). The first step in the diagnosis of SCAD is to look for a heart attack or damage to the heart muscle. Tests in the emergency room usually include an electrocardiogram (ECG) and blood tests that detect damage to the heart muscle, such as the cardiac enzyme troponin. In some cases, the cardiac enzymes may be normal but changes on the ECG can still indicate reduced blood flow to the heart (ischemia). Following the ECG and blood tests, coronary angiography is necessary in most cases to confirm the diagnosis of SCAD (see below).
What is the initial treatment for a patient with SCAD?
Initial treatment of SCAD is primarily determined by making an accurate diagnosis; this is critical because treatment of SCAD differs from treatment for atherosclerotic heart attack (caused by plaque build-up). Since patients with SCAD are typically younger and may have few or no risk factors for having a heart attack, they do not fit the expected profile for a patient with a heart attack and may be misdiagnosed. When a heart attack is suspected, initial treatment may include aspirin and other blood thinners, medications such as beta-blockers to lower the blood pressure and heart rate, and nitroglycerin (i.e., an anti-anginal medication given either under the tongue, through paste or a patch on the skin, or through an IV line) to treat chest pain. The patient will also be put on a heart monitor to observe for any abnormal heart rhythms.
Coronary angiography
When a heart attack is suspected, either due to an abnormal ECG and/or abnormal cardiac enzymes, coronary angiography (also called cardiac catheterization) is the standard test used to assess for blockages in the coronary arteries. During this procedure, a special dye (i.e., contrast dye) is injected into the patient while X-ray images are taken so that any coronary artery blockages can be seen. The procedure is performed through a catheter, which is a tube that is placed through an artery of the leg (groin area) or the wrist. A coronary angiogram is an important test to determine the cause of heart attack, to identify the location and severity of blockages in the coronary arteries, and to determine whether the blockages look like they are due to atherosclerosis or SCAD. A coronary angiogram from a patient with SCAD is shown in Figure 2. Some research has looked at the use of a special computed tomography (CT) scan known as coronary CT angiography (CTA) to perform angiography of the coronary arteries noninvasively in the case of suspected SCAD, but this is not yet standard practice for initial diagnosis. In some cases, CTA may be used selectively in follow-up to demonstrate healing of the coronary arteries after SCAD. 1
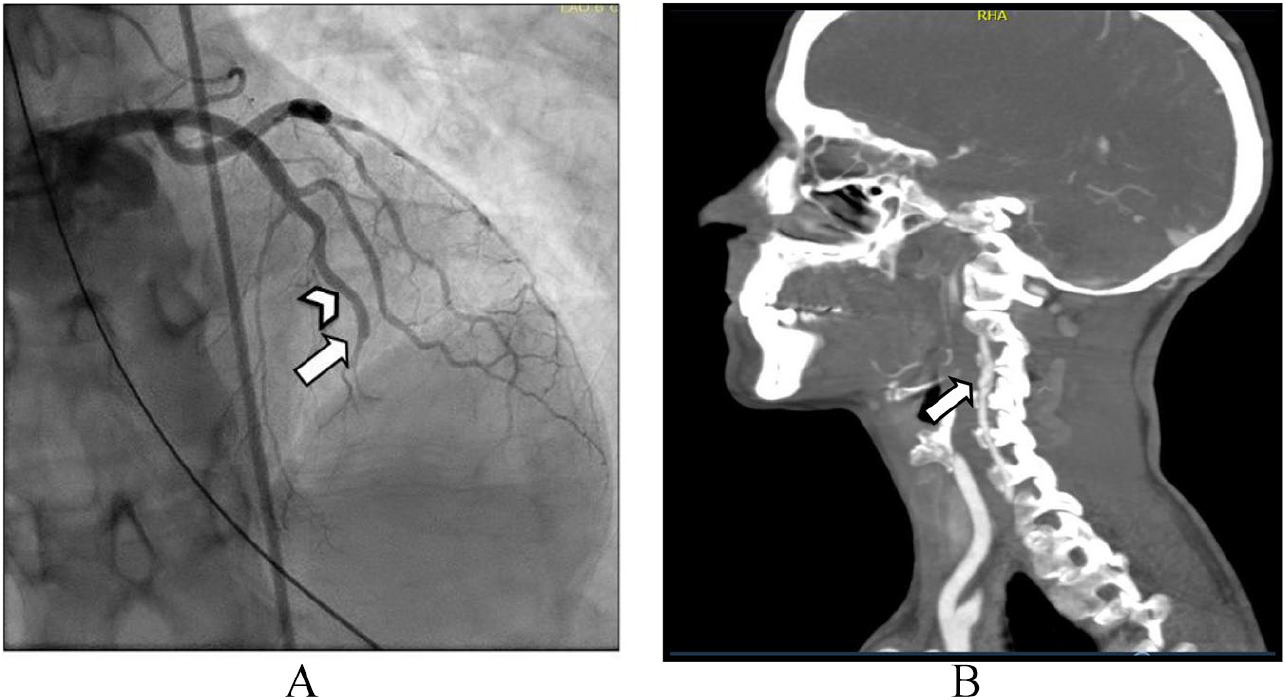
SCAD with other vascular abnormalities. This 57-year-old woman had chest pain and a heart attack. She was found to have SCAD of multiple coronary arteries. (A) The arrow points to the SCAD and total blockage (occlusion) of the LAD coronary artery. Note how the artery is normal above the arrow (arrowhead) and then suddenly tapers (arrow). (B) After initial recovery, she underwent imaging of the vessels outside of the heart and was found to have a dissection (tear) of the right vertebral artery with a bulge in the vessel called a pseudoaneurysm (arrow).
What is the long-term treatment for a patient after SCAD?
The best course of treatment for patients with SCAD may differ for each individual. It is important for patients to work closely with cardiologists and other health care providers who are familiar with SCAD to create a customized treatment plan. This plan may include medications, cardiac rehabilitation, and potential changes to lifestyle. Patients should also be evaluated for underlying conditions, such as FMD and other vascular abnormalities that may have contributed to developing SCAD.
Conservative versus interventional management after the coronary angiogram
Research has shown that the majority of patients who are having a heart attack due to SCAD can be treated with medications alone and do not require stents or other procedures to open the coronary arteries. 1 In fact, studies have found that most blockages in the coronary arteries heal completely within the weeks following SCAD. 1 For most patients in whom the diagnosis of SCAD is made on the coronary angiogram, medications (see below) and continuous monitoring in the hospital for several days after the heart attack will be sufficient initial treatment. For some patients with very severe coronary artery blockages due to SCAD (such as of the left main coronary artery) or who have ongoing chest pain or other complications (such as low blood pressure related to poor heart function or abnormal heart rhythms), coronary artery stenting or other procedure(s) to improve blood flow to the heart may be required. 1 In very rare and severe cases, open heart surgery and coronary artery bypass grafting may be necessary to treat SCAD.
What medications are needed after SCAD?
Most patients will be prescribed multiple medications after a SCAD. This change can be challenging for some patients who were previously healthy and did not need to take medications regularly. Medications are used to treat the initial heart attack that occurred as a result of the SCAD, to prevent complications, to treat any ongoing chest pain, and also to prevent another (recurrent) SCAD. Antiplatelet blood-thinning medications are important following SCAD and may be prescribed as a single agent (aspirin alone) or two agents in combination (aspirin plus either clopidogrel, ticagrelor, or prasugrel). Good control of blood pressure is important following SCAD. Beta-blockers are used to control both heart rate and blood pressure and to prevent and treat abnormal heart rhythms and heart failure. Recent research has suggested that beta-blockers may prevent another SCAD when used long-term, though this is an area that warrants additional study. 7 Patients who have impaired heart muscle function after SCAD, or who have high blood pressure following SCAD, may also be prescribed angiotensin-converting enzyme (ACE) inhibitors or angiotensin-receptor blockers. Patients should not stop any medications after a heart attack without first discussing it with their physician.
How is chest pain after SCAD treated?
Though the cause is not well understood, residual and recurrent chest pain in the initial weeks after SCAD is common. The chest pain experienced may closely resemble the pain felt during the initial heart attack or may be a different type of pain. Chest pain after SCAD can be a cause of stress and anxiety. A patient who experiences chest pain after SCAD should urgently follow up with her or his physician, particularly if the pain is similar to the original heart attack pain. In most cases, tests will be done to be sure there is no recurrent SCAD, including an ECG and blood tests for cardiac enzymes. Other tests may be ordered, such as a stress test with imaging, or, in some cases, repeat imaging of the coronary arteries either directly with a coronary angiogram or a noninvasive coronary CTA. Patients with persistent chest pain after SCAD may be prescribed additional anti-anginal medications, such as nitrates, calcium channel blockers, or the medication ranolazine, to improve symptoms and quality of life. For many patients with residual chest pain after SCAD, the pain dissipates over the weeks to months following the initial heart attack.
How can cardiac rehabilitation benefit patients who have had SCAD?
Patients who have had a heart attack due to SCAD may benefit from a cardiac rehabilitation program. Cardiac rehabilitation is a supervised exercise and education program that can help patients resume regular exercise and adjust to the life-changing event of a heart attack. During cardiac rehabilitation, an exercise (primarily walking) program is started with close cardiac monitoring by trained cardiovascular professionals. Although most cardiac rehabilitation programs are designed for older patients with heart attack due to atherosclerosis (plaque), some programs have adapted their activities for patients with SCAD. 8 All patients who have had SCAD need to resume a regular exercise program for long-term cardiovascular health and well-being, and cardiac rehabilitation can be a helpful step in this process.
Monitoring and testing for underlying vascular conditions/FMD
Patients with SCAD should follow up regularly with their SCAD care provider. Monitoring for chest pain, assessing risk for recurrent SCAD, checking for other abnormalities such as FMD, and providing psychological support are all important aspects of care after SCAD. Patients with SCAD should be checked for FMD and other vascular abnormalities outside of the coronary arteries with imaging tests.1,3 This screening is generally accomplished with CTA or magnetic resonance angiography (MRA) of the head and neck and the chest, abdomen, and pelvis. If FMD or other vascular abnormalities are found (such as aneurysms or dissections), consultation with vascular specialists, follow-up imaging, and possibly additional procedures may be required.
Should patients with SCAD undergo genetic testing?
For some patients, genetic testing may be recommended to screen for mutations in the genes for certain vascular connective tissue disorders (such as vascular Ehlers–Danlos syndrome, Loeys–Deitz syndrome, and others). 1 These genetic tests may help determine if there is an underlying genetic cause of SCAD. Genetic testing is not always needed but may be recommended for patients who have multiple aneurysms or dissections found on imaging studies, a strong family history of aneurysms or dissections, or certain features on physical examination that suggest a connective tissue disorder.
Mental health and support after SCAD
Monitoring and support for mental health and well-being is an important aspect of care for patients who have had a SCAD both in the short- and long-term. Many patients who have survived SCAD report traumatic or negative experiences during their diagnosis and care, which can lead to feelings of anxiety and depression. In addition, some patients face unique problems with health care providers’ lack of familiarity with the diagnosis of SCAD and FMD (if found), which can be an additional source of anxiety. Any symptoms of anxiety or depression related to the diagnosis of SCAD should be discussed openly with the health care team. Additionally, several organizations (listed below) can provide support for patients.
What are diet and exercise recommendations after SCAD?
The development of SCAD is not related to diet. However, eating a well-balanced diet, rich in fruits and vegetables, is important for overall cardiovascular health. In terms of exercise restrictions, recommendations vary from patient to patient, but in general it is recommended that patients who have suffered SCAD
Are there other issues patients who had have SCAD should be aware of?
Patients who have suffered a SCAD are at risk of suffering another SCAD (called recurrent SCAD) and need to be aware of the symptoms of another heart attack. They should seek emergency medical care if they develop these symptoms. Patients may also be advised to wear a medical alert bracelet or carry an emergency medical card identifying the patient as having ‘coronary artery dissection’, so that medical care providers have proper knowledge on how to proceed in the event of recurrent symptoms.
Most experts caution against pregnancy following SCAD due to the risk of recurrent SCAD. Patients who have had a prior pregnancy-associated SCAD are placed in a very high-risk category for future pregnancy. For young women with SCAD, the decision to become pregnant should be made after thorough discussion and careful evaluation by experts familiar with SCAD. Determining the best option for contraception (birth control) after SCAD also requires a thoughtful discussion with the medical team.
What other resources are there for patients who have had SCAD?
As the awareness, understanding, and diagnosis of SCAD have grown, so has support for research and programs for education and support for patients and family members. A number of advocacy organizations have focused their efforts on understanding SCAD and improving the lives of patients who have had SCAD. These organizations have excellent online resources for patients and health care providers, as well as information regarding ongoing research initiatives. These websites include those of the SCAD Alliance (www.scadalliance.org), Beat SCAD (www.beatscad.org.uk), and SCAD Research, Inc. (www.scadresearch.org). For patients with both SCAD and FMD, the FMD Society of America (www.fmdsa.org) may provide helpful information. Two other helpful sources of information regarding SCAD, particularly for health care providers, are scientific statements on SCAD published by the American Heart Association and the European Society of Cardiology in 2018.1,3
The `Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage.
The Vascular Disease Patient Information page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
Dr. Gornik is a member of the Medical Advisory Board of the FMD Society of America and has ownership/equity in FlexLife Health. Dr. Kim is a member of the Scientific Advisory Board of SCAD Alliance and participated in a Board Meeting for Acer Therapeutics. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.