
Abstract
Background:
We aimed to describe patient and limb outcomes in the decade after endovascular revascularization for chronic lower-extremity peripheral artery disease (PAD).
Methods:
We assessed outcomes in patients having endovascular revascularization of the superficial femoral artery in two centers between 2003 and 2011 and followed for a median 9.3 (25–75%: 6.8, 11.1) years. Outcomes included death, myocardial infarction, stroke, repeat limb revascularizations, and amputations. We used competing risks analysis with clustering by patient to determine the hazard ratios (HR) and 95% CI for patients, and procedural characteristics for cause of death, cardiovascular events, and major adverse limb events (MALE).
Results:
There were 253 index limb revascularizations in 202 patients followed for a median 9.3 years. Patients had intensive medical treatment with 90% on statins and 80% on beta-blockers. During follow up there were 57 (28%) cardiovascular deaths and 62 (31%) noncardiovascular deaths. Of the 253 limbs, 227 (90%) were free of MALE over follow up and 93 (37%) had MALE or minor repeat revascularization. In multivariable models, cardiovascular death significantly associated with critical limb ischemia (HR = 3.21, 95% CI = 1.84, 5.61) and noncardiovascular death with chronic kidney disease (HR = 2.69, 95% CI = 1.68, 4.30), and smoking (HR = 2.75, 95% CI = 1.01, 7.52). MALE or minor repeat revascularization associated with critical limb ischemia (HR = 1.43, 95% CI = 0.84, 2.43), smoking (HR = 2.49, 95% CI = 1.26, 4.90), and lesion length > 200 mm (HR = 1.51, 95% CI = 0.98, 2.33).
Conclusions:
Among patients with intensive medical therapy, the risk of noncardiovascular death was high and similar to cardiovascular death. Endovascular intervention can have acceptable long-term results. Future studies should evaluate strategies to reduce both cardiovascular and noncardiovascular deaths.
Background
Chronic lower-extremity peripheral artery disease (PAD) may be asymptomatic, cause claudication with leg discomfort during activity, or present as critical limb ischemia (CLI) with limb pain at rest, gangrene, or other tissue loss.1,2 Patients with PAD have a high risk of adverse cardiac and cerebrovascular events (MACCE) such as myocardial infarction or stroke.1,2 In addition, CLI increases the risk of major adverse limb events (MALE) such as amputation.1,2 Current guidelines recommend exercise and medical therapy to reduce the risk of MACCE and claudication, and support revascularization for lifestyle-limiting claudication and CLI.1,2 Endovascular therapy is increasingly the first mode of revascularization, and in the United States there are over 130,000 endovascular treatments per year for femoral-popliteal PAD among Medicare beneficiaries alone. 3
The outcomes of patients having revascularization for PAD are often limited to short-term follow up (1–3 years) and tend to focus on the patency of the artery or bypass graft. In these reports, the short-term risk of MACCE is higher in patients needing PAD revascularization compared to patients who do not require revascularization.4,5 MALE in the first year after femoral-popliteal endovascular interventions are worse with longer lesions, diabetes mellitus, chronic kidney disease (CKD), and smoking. 6
However, the causes of mortality and MACCE over the longer time frame and number of procedures required to prevent recurrent claudication or MALE are unknown and have a direct impact on therapies to prevent death and MACE, patient quality of life, and healthcare costs. Although clinical trials of revascularization are rare, the durability of endovascular revascularization is often considered inferior to lower-extremity bypass grafting.1,2 The aim of this study was to assess the clinical outcomes including causes of mortality, MACCE, amputations, and the number of procedures required to treat recurrent symptoms in the 10 years after an endovascular procedure for superficial femoral artery disease.
Methods
All patients having their first endovascular revascularization of the superficial femoral artery for lifestyle-limiting claudication or CLI between 2003 and 2011 by the cardiovascular divisions in two centers (VA Boston and the Brigham and Women’s Hospital) were included in this retrospective cohort study. Subsequent interventions in the opposite leg were included in the limb outcomes analysis. The study was approved by the VA Boston and Brigham and Women’s Hospital institutional review boards.
In patients with claudication, endovascular intervention was offered if patients continued to have severe claudication after several months, unsupervised exercise therapy, and, where indicated, a trial of cilostazol. In patients with CLI, endovascular intervention was offered after noninvasive or invasive arteriograms defined the extent of disease. The use of stents and adjunctive therapies were at the discretion of the operator, but stents were usually used for longer lesions. Patients were followed in the outpatient clinic at 3 months and then at intervals of 6–12 months after the index procedure.
Demographic and comorbidity data
Data on demographics, cardiovascular risk factors, comorbidities, and medications at the time of the index procedure were extracted from the electronic medical record. Smoking status was defined as current, former, or never smoked. Diabetes was defined as a diagnosis of diabetes mellitus and or treatment for diabetes. CKD was defined as a creatinine level > 1.5. Procedural details were extracted from the endovascular procedure report form. These included the presence of chronic total occlusions and the pre- and posttreatment stenosis of the lesion. The angiograms of the procedure were reviewed to check the length of the lesion against the balloons and stents used, and the number of tibial patent arteries (runoff). The maximum and minimum balloon and stent diameters were recorded, as was the success of the procedure. Lesion length was stratified as < 100 mm, 100–199 mm, or ⩾ 200 mm. The Trans-Atlantic Societies Consensus (TASC) classification of the lesion (A or B vs C or D) was used, and adjunctive therapies such as atherectomy.
Outcomes
Clinical outcomes of death, nonfatal myocardial infarction, and stroke were assessed from the Brigham and Women’s electronic medical record, which also included outcomes recorded in over 11 affiliated hospitals and clinics (now part of Mass General Brigham healthcare), and from the VA electronic medical record including all presentations in the national VA healthcare system. Cause of death for VA Boston patients was obtained from the Center of Excellence for Mortality Data Repository, Joint Department of Veterans Affairs and Department of Defense Suicide Data Repository – National Death Index. Cause of death for patients treated at Brigham and Women’s Hospital was obtained from the Center for Disease Control National Death Index. Cause of death was grouped into cardiovascular deaths and noncardiovascular deaths (cancer deaths, pulmonary deaths, other deaths) using International Classification of Diseases 10th Revision (ICD-10) codes (online Supplementary Table 1).
Limb outcomes including repeat endovascular procedures due to recurrent severe claudication or CLI, vascular surgery (common femoral artery endarterectomy or open bypass grafting), minor amputation (below the ankle), and major amputation (above the ankle) were extracted from the electronic health records. MACCE was defined as a cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke. MALE was defined as major amputation, new bypass graft, or thrombolysis, and MALE or minor revascularization was defined as MALE or any repeat revascularization during follow up. 7 All outcomes were assessed up to December 2020.
Statistics
All data were analyzed using Stata 16 (StataCorp LLC, College Station, TX, USA). Baseline demographics, comorbidities, and stent dimensions were described as means and SD, or frequencies and percent as appropriate. Patients were defined as having CLI if at least one limb had an index procedure for CLI. Cause of death was grouped as cardiovascular (heart or stroke) death, cancer death, chronic obstructive airways/pneumonia/or other infection death, and all other causes of death. Multivariable hazard ratios (HR) and 95% CIs for clinical outcomes were assessed from cause-specific hazard models for all-cause mortality, and competing risks analyses using Fine–Gray subdistribution models for all other outcomes. 8 The competing risks were noncardiovascular death for the outcomes of cardiovascular death and MACCE, cardiovascular death for the outcome noncardiovascular death, and all-cause death for the outcome of MALE. Cumulative incidence functions derived from these models were used to graph the incidence of each outcome over 10 years. Limb outcomes of MALE or minor repeat revascularization included the index event in either limb, and analyses were assessed by models clustered by patient. Supplementary analyses using cause-specific hazard models addressed hazards of the rate of each outcome and are considered more pertinent to addressing the etiology of the outcomes (online Supplementary Appendix). 8 All multivariable models entered variables with a p < 0.1 on univariable analysis and backward regression was used to select the final models with a p-value to remove < 0.2.
Results
There were 202 patients having 253 index endovascular procedures for superficial femoral PAD. Patients were followed until death or for a median 9.3 years (25–75%: 6.8, 11.1 years; maximum 15.4 years). Table 1 describes the demographics, cardiovascular risk factors, comorbidities, and medications at the index procedure by subsequent death or survival during follow up and univariable HR, 95% CI for death. Half of the patients had diabetes mellitus, one-quarter were current smokers, and most patients had hypertension or high cholesterol. This cohort had a high penetrance of guideline-directed medical therapy with 90% of patients on statins, over 80% on beta-blockers, and over 60% on angiotensin-converting enzyme (ACE) inhibitors. The overall mean (SD) low-density lipoprotein (LDL) cholesterol was 77 (30) mg/dL and systolic blood pressure was 131 (21) mmHg, which was comparable to many clinical trials of cholesterol and blood pressure lowering at the time of their index procedure. Increasing age, male sex, CKD, and an index procedure for CLI were associated with all-cause death on univariable analysis.
Description of 202 patients by all-cause death over follow up.
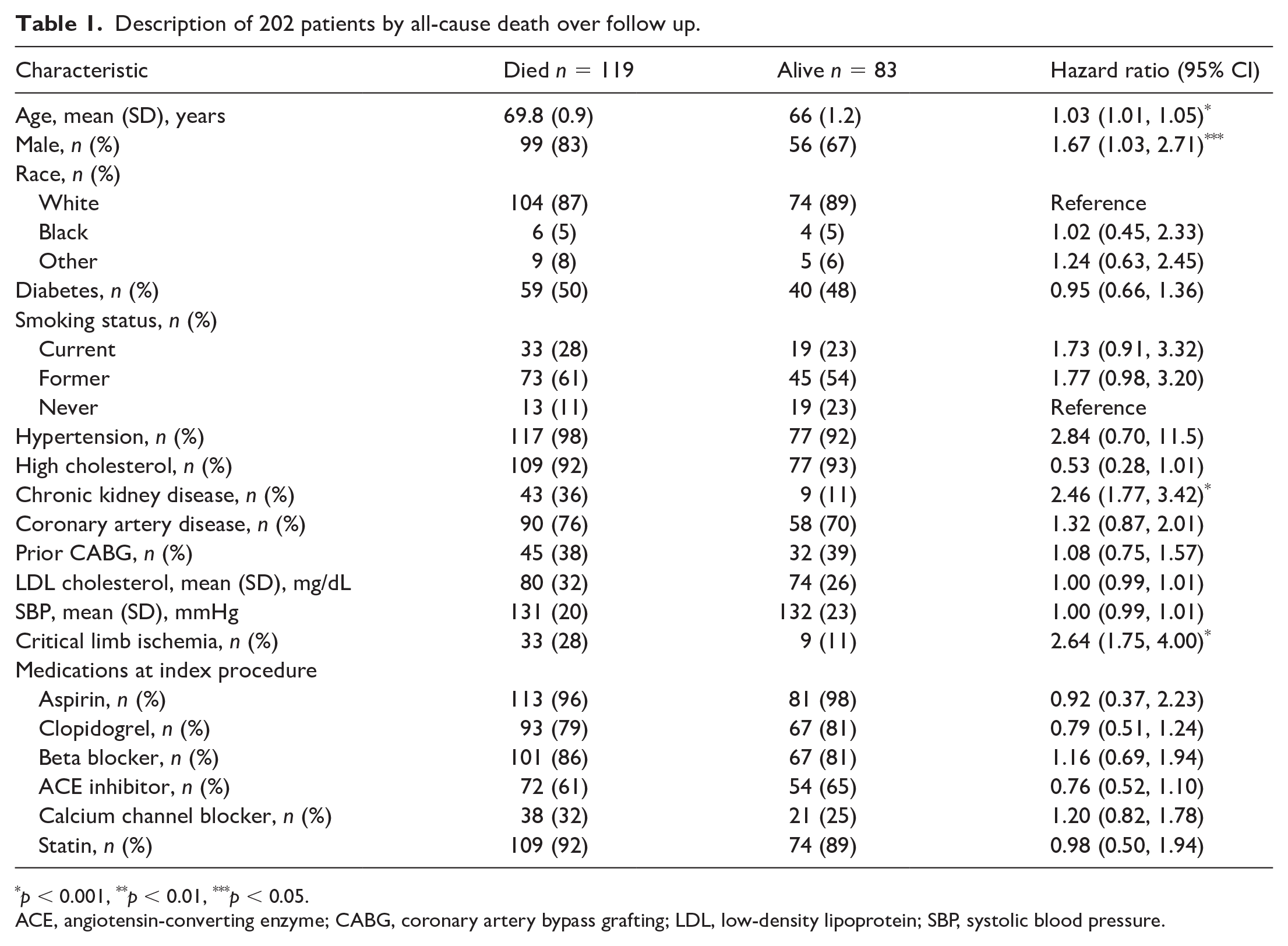
p < 0.001, **p < 0.01, ***p < 0.05.
ACE, angiotensin-converting enzyme; CABG, coronary artery bypass grafting; LDL, low-density lipoprotein; SBP, systolic blood pressure.
During follow up there were 119 (59%) deaths, including 57 (28%) cardiovascular deaths and 62 (31%) noncardiovascular deaths (including 22 cancer and 22 pulmonary/infection deaths). Figure 1 shows cumulative incidence plots for all-cause death and cause-specific death over 10 years of follow up. Cardiovascular deaths were the most common cause of death (48%), with cancer causing 18% of deaths, chronic obstructive pulmonary disease (COPD)/infection causing 18% of deaths, and other causes were 7% of deaths. Figure 2 shows the survival without events, nonfatal MI and strokes, fatal cardiovascular events, and fatal noncardiovascular events. Although cardiovascular death is the most common cause of death, noncardiovascular deaths are equally as prevalent over the decade after a femoral artery intervention.
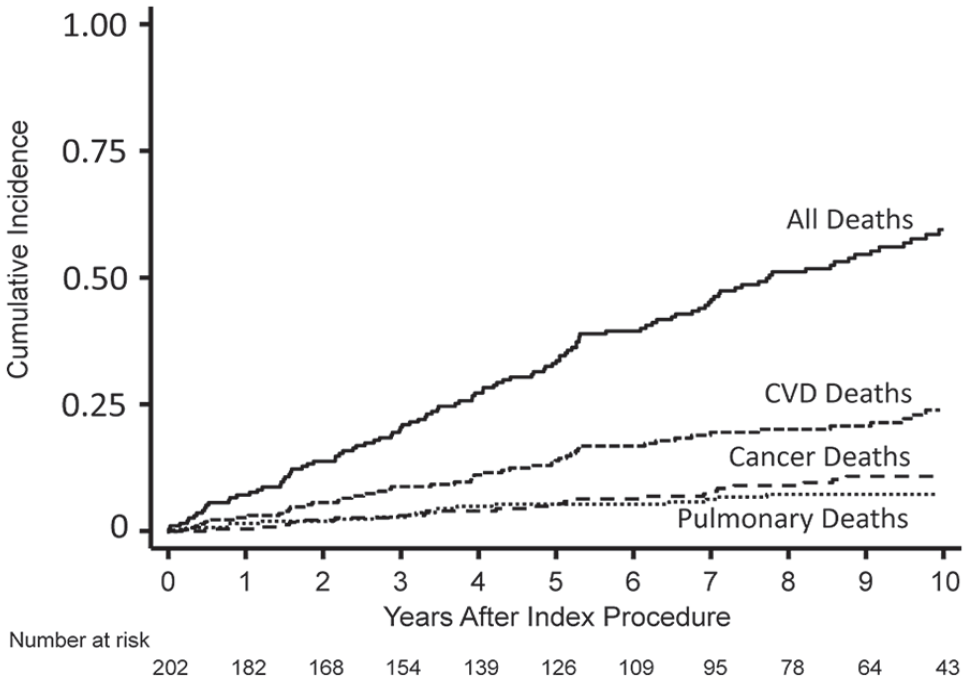
Cumulative incidence derived from competing risks analysis for all-cause death, cardiovascular death, cancer deaths, and pulmonary or infection deaths in 202 patients up to 10 years after endovascular femoral artery revascularization.
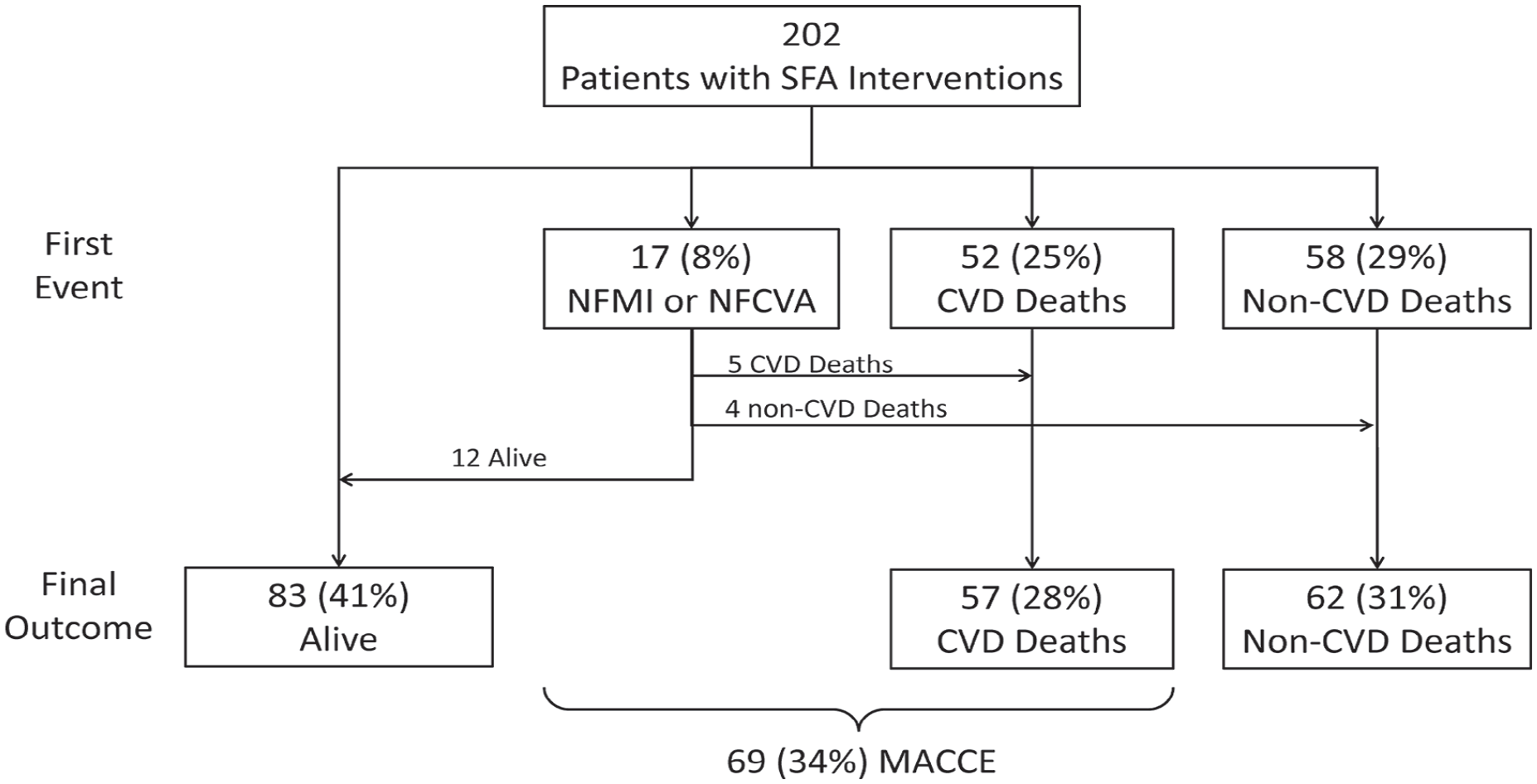
Patient-level outcomes of death, cause of death, and MACCE in 202 patients treated with endovascular revascularization for femoral peripheral artery disease.
Table 2 describes the presentation and procedure details at the index procedure for each limb. Overall, the indication for the index procedure was CLI in 46 (18%) limb procedures, 144 (57%) limbs had a chronic total occlusion, TASC C or D lesions were present in 117 (49%) limbs, and 87 (37%) lesions were 200 mm or longer. There were 93 (36.8%) MALE or minor repeat revascularizations. Baseline factors related to MALE or minor repeat revascularization in follow up included CLI, tissue loss, TASC C or D lesion, lesion length ⩾ 200 mm, a higher preprocedure stenosis, and the use of thrombolysis at the index procedure.
Description of 253 limbs at the index procedure by subsequent MALE or minor revascularization.
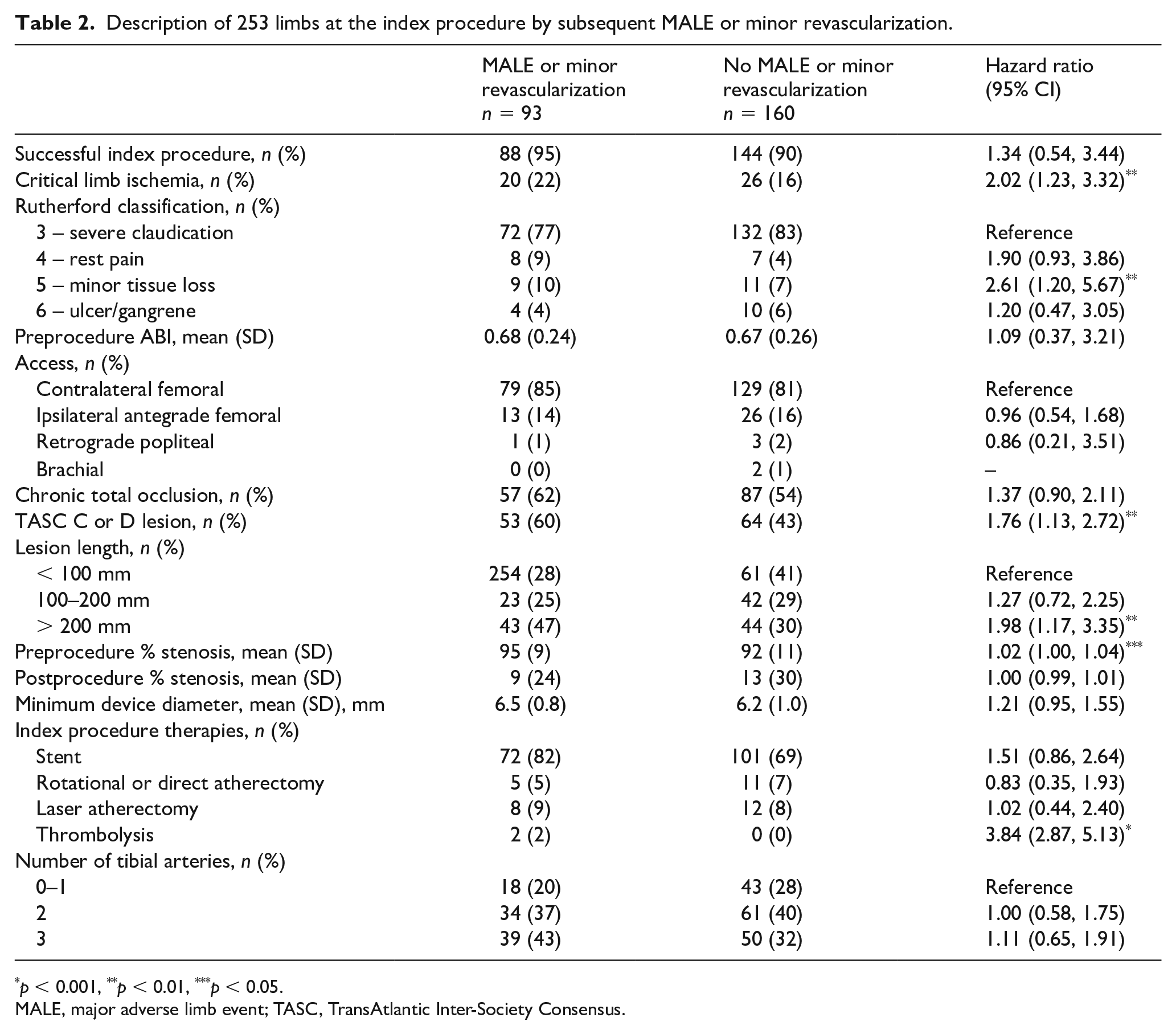
p < 0.001, **p < 0.01, ***p < 0.05.
MALE, major adverse limb event; TASC, TransAtlantic Inter-Society Consensus.
Figure 3 shows the initial success of the index procedure and subsequent repeat revascularization and amputations. Among all 253 limbs, 232 (92%) were successful and 21 were unsuccessful, with five unsuccessful procedures requiring surgical bypass. Of all limbs, 227 (90%) were free of MALE (surgical revascularization or above-knee amputation) over follow up. Of the 232 limbs with an initial successful procedure, 140 (60%) required no further revascularization or amputation. Of the successful procedures, 75 limbs (32%) required between one and three repeat endovascular procedures, 13 (6%) limbs required surgical revascularization, eight (3%) had a minor amputation, and 11 (5%) had a major amputation. Of the 126 repeat revascularization procedures, 113 (90%) were endovascular and 13 (10%) were surgical (Figure 3). Of the 13 subjects requiring surgical revascularization, nine (69%) had subsequent procedures in follow up, including three revisions by balloon angioplasty or stenting, one repeat common femoral endarterectomy, four graft thromboses followed by above or below-knee amputation, and one local thigh abscess excised and drained.
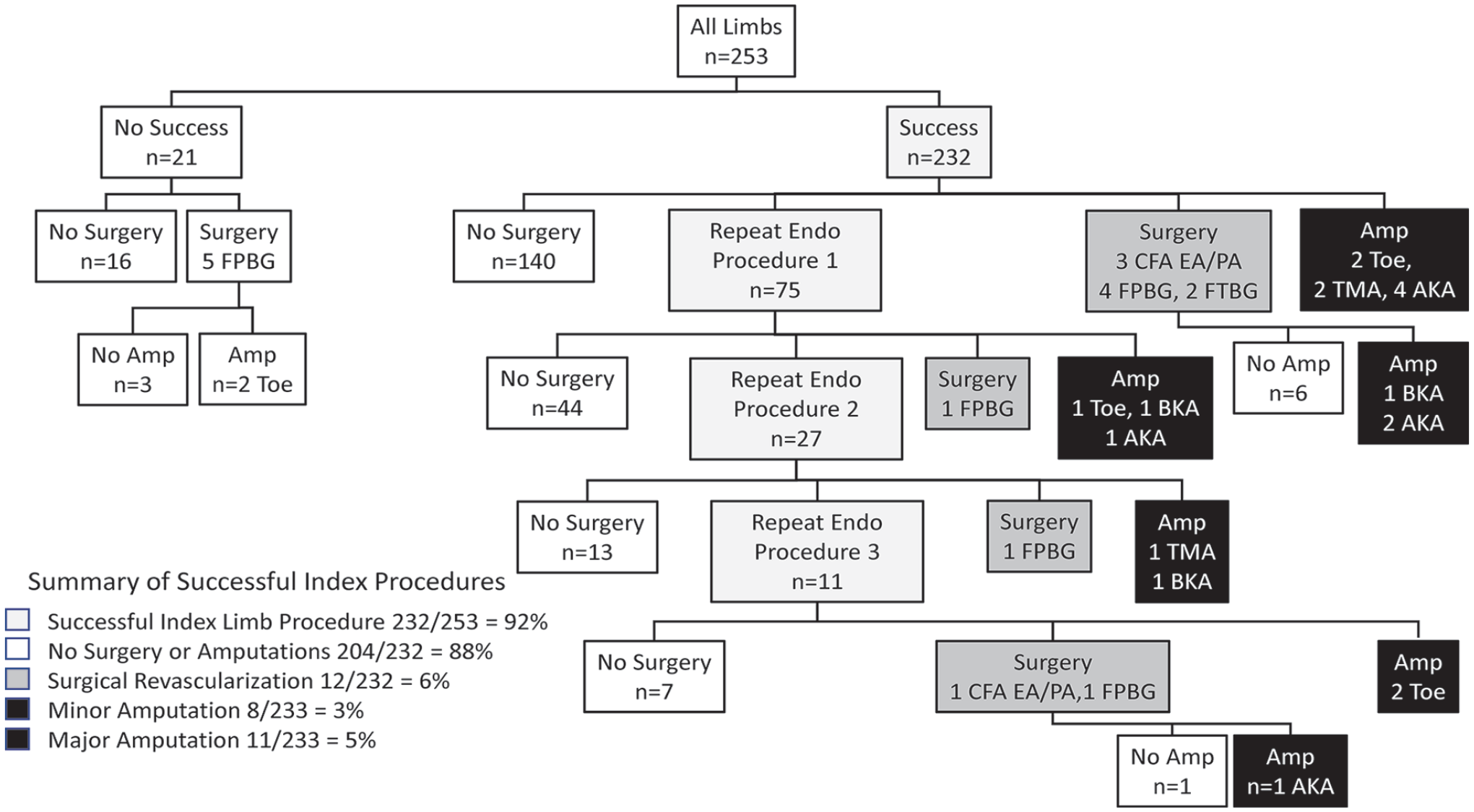
Limb outcomes in 253 limbs treated with endovascular revascularization for femoral peripheral artery disease.
Online Supplemental Figures 1 and 2 show the limb outcomes stratified by limbs treated for claudication and CLI. MALE occurred in 25 limbs with 13 (6%) limbs treated for claudication and 12 (26%) limbs treated for CLI. MALE or minor revascularization occurred in 71 (37%) limbs treated initially for claudication and 17 (44%) limbs treated initially for CLI. The symptoms preceding MALE or minor revascularization in limbs treated initially for claudication were recurrent claudication in 49 (69%) limbs and CLI in six (8%) limbs, and for limbs initially treated for CLI, nine (53%) had recurrent claudication and five (29%) had recurrent CLI. Figure 4 shows the limb outcomes for patients with a successful index procedure. Amputations were more common in patients having an index procedure of CLI with four (10%) minor amputations and seven (18%) major amputations.
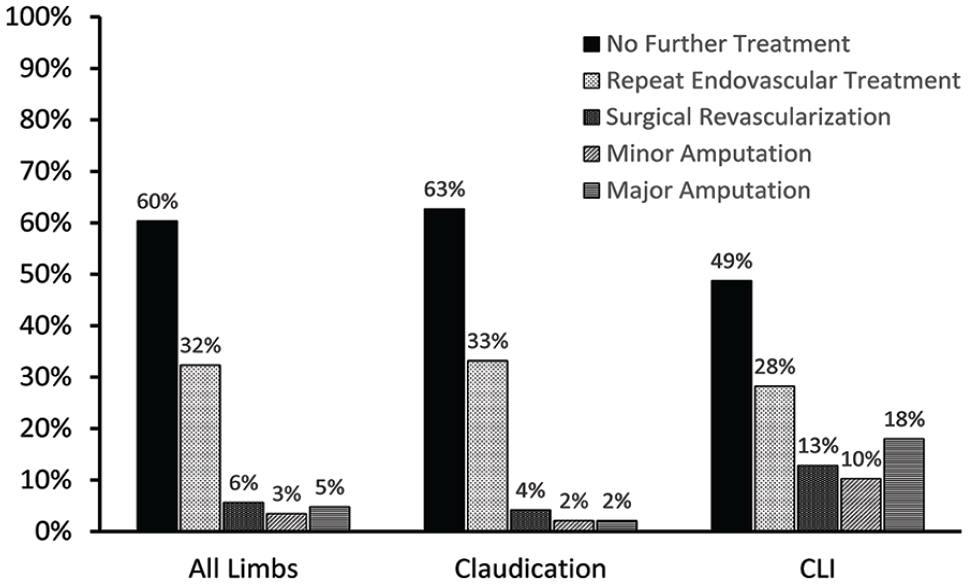
Limb outcomes in 232 limbs successfully treated by endovascular revascularization for femoral peripheral artery disease for all limbs and stratified by limbs treated for claudication and critical limb ischemia.
Table 3 shows the final multivariable models for all-cause death, cardiovascular death, MACCE, noncardiovascular death, and MALE or minor revascularization. Male sex was associated with a higher incidence of all-cause death, cardiovascular death, and MACCE. CLI was associated with a higher incidence of all-cause death, cardiovascular death, MACCE, and MALE or minor repeat revascularization. CKD was associated with a higher risk of all causes of death and noncardiovascular death. Statin therapy was associated with a lower risk of cardiovascular death and MACCE. Current smoking was associated with a higher risk of noncardiovascular death and MALE or minor repeat revascularization. Long lesion length (> 200 mm) was associated with a higher risk of MALE or repeat revascularization.
Hazard ratios (95% CIs) from competing risk Fine–Gray subdistribution multivariable models for all-cause and cause-specific death, MACCE, and MALE or minor repeat revascularization.
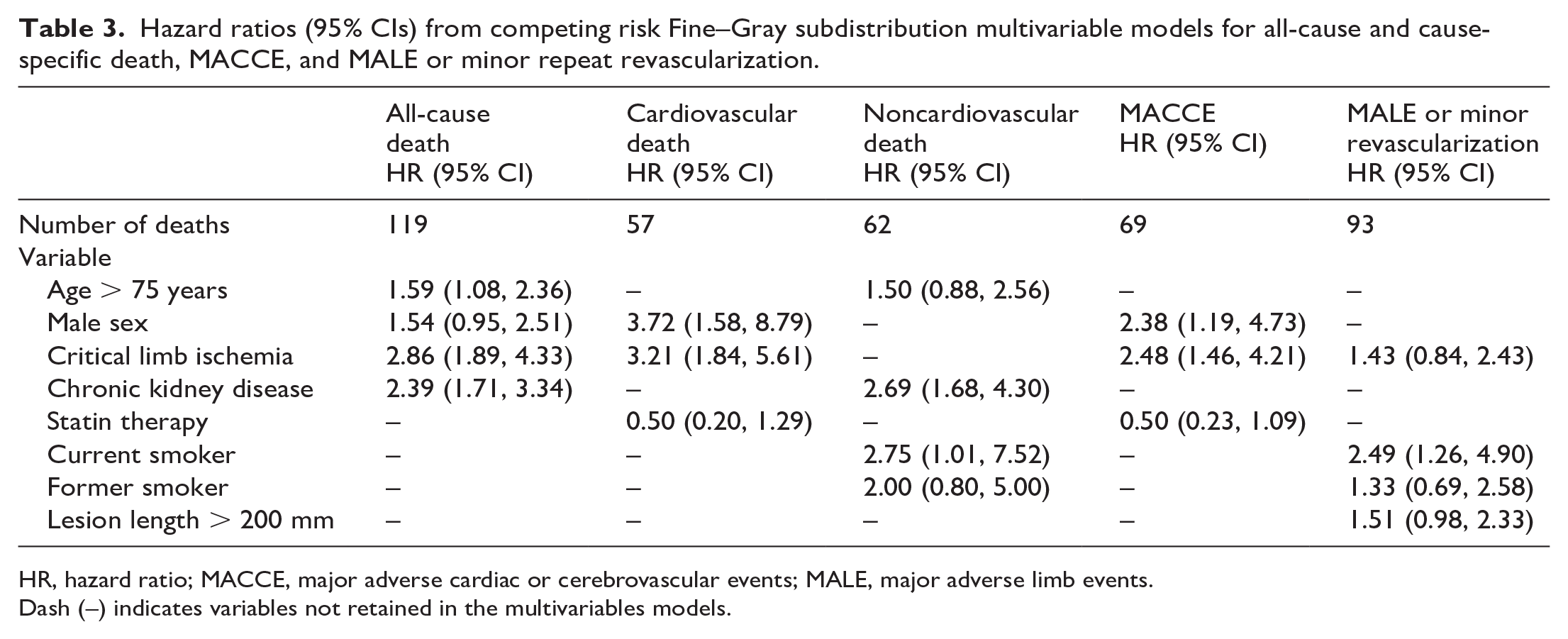
HR, hazard ratio; MACCE, major adverse cardiac or cerebrovascular events; MALE, major adverse limb events.
Dash (–) indicates variables not retained in the multivariables models.
Online Supplementary Table 2 shows the HRs from cause-specific hazard models for the rates of outcomes in patients who were free of competing events. CKD was associated with higher rates of cardiovascular death and MACCE but was not selected in the competing risks models (Table 3), reflecting its greater effect on noncardiovascular death.
Discussion
Endovascular revascularization of the superficial femoral artery for claudication or CLI is increasingly common, but the long-term clinical and limb outcomes in patients on guideline-directed medical therapy are uncertain. In this study, of patients with high rates of statin use, good blood pressure and LDL cholesterol control, and who are followed systematically and regularly by cardiologists with expertise in vascular medicine, endovascular revascularization with or without repeat endovascular procedures offered a durable therapy over 10 years in over 90% of limbs with claudication and over 75% of limbs with CLI. However, the rates of death, cardiovascular death, and MACCE in the decade after an endovascular procedure remain high in this population.
Cardiovascular events and cause of death
Although statin therapy and the intensive cardiovascular risk factor control likely lowered the risk of cardiovascular events in this population, half of the deaths were due to noncardiovascular causes with cancer and pulmonary disease or infection significant contributors to death. PCSK9 inhibitors and low-dose direct oral anticoagulants, which were unavailable for most of the study period, would likely lower the risk of cardiovascular events based on recent trials.9,10 Antiinflammatory interleukin (IL)-1β antagonists such as canakinumab and colchicine could be considered as they lower the risk of cardiovascular disease in patients with coronary disease.11 –13 However, these immune modulating therapies may increase the risk of infection,12,13 and would need to be tested in this population to ensure they were safe and did not increase noncardiovascular deaths.
Although more contemporary guideline-directed medical therapy for atherosclerosis (e.g., PCSK9 inhibitors) would have lowered cardiovascular events further, these interventions would not impact noncardiovascular deaths related to cancer, pulmonary disease, and infections. 14 In our study, CKD and smoking were associated with noncardiovascular deaths and justify strategies to reduce these risk factors. For example, patients with PAD may benefit from specific programs of intensive smoking cessation, a low-dose lung computed tomography (CT) scan in smokers to identify early lung cancer, or more intensive treatment of diabetes mellitus with glucagon-like peptide 1 (GLP-1) agonists and sodium-glucose cotransporter-2 (SGLT2) inhibitors to prevent progression of kidney disease. Given the high rates of noncardiovascular outcomes, multidisciplinary collaborations with pulmonologists, endocrinologists, and others may help lower noncardiovascular outcomes in patients with advanced PAD.
Limb outcomes
Endovascular therapy successfully managed 88% of limbs over follow up without MALE defined as need for surgical revascularization or above-knee amputation. Endovascular treatment for femoral artery disease in this study resulted in a durable outcome without a need for any further intervention in 60% of limbs overall, although the rate was lower in limbs initially treated for CLI (50%). Of limbs requiring repeat revascularization during follow up, 90% were managed by repeat endovascular procedures. The need for further endovascular revascularization, surgical revascularization, or amputation in the other 40% of limbs highlights the importance of continued regular follow up and surveillance for recurrent adverse limb outcomes. In this study, we generally evaluated patients 3 months after their initial procedure and then at 6-month intervals after this time using ankle–brachial indices and duplex ultrasound, particularly if symptoms recurred. Thus, endovascular revascularization (like surgical revascularization) is not a curative procedure, but rather all revascularization requires a long-term contract between patient and physicians to monitor the disease and to identify severe claudication or CLI that may require repeat revascularization.
Overall, MALE rates were low and particularly after revascularization for claudication (2% minor amputation and 2% major amputation). Most MALE or minor revascularization events were associated with recurrent severe claudication. Recurrent CLI with a nonhealing ulcer or rest pain or need for amputation occurred more often in limbs that were initially revascularized for CLI. These adverse events issue a note of caution when considering endovascular revascularization for femoral artery PAD, particularly in patients with mild claudication and reasonable functional capacity. Many patients with claudication can be managed with medical therapy such as cilostazol and supervised exercise therapy (which was only covered by third-party payers at the end of this study). 15 However, in patients with lifestyle-limiting claudication where cilostazol is contraindicated, ineffective, or causes side effects, this study suggests that femoral artery endovascular revascularization can offer durable results over 10 years at acceptable risk in the setting of routine surveillance. The addition of supervised exercise therapy, now funded by third-party payers, would likely improve outcomes after endovascular revascularization. 15
Our cohort immediately preceded the approval of drug-coated balloons and stents and the use of more potent antithrombotics. In the 1–5 years after endovascular revascularization, these therapies have lower rates of repeat revascularizations,16–18 but the mortality rates in patients treated with or without these devices in large administrative databases is no different, with 5-year mortality in the 30–50% range,19,20 which is similar to our study (5-year Kaplan–Meier rate = 34%). Nevertheless, drug-coated balloons and stents with newer atherectomy devices in more contemporary practice may further reduce MALE.
Patients with CLI were at higher risk of death and adverse limb events over the 10 years of follow up as reported in other shorter follow-up studies.21,22 Recurrent limb events were higher in limbs treated for CLI compared to claudication, and higher in smokers compared to nonsmokers over the decade of follow up as they are in shorter-term studies of 1–3 years of follow up.4,6,23,24 The only procedural factor related to MALE or repeat intervention was long lesion length (⩾ 200 mm). Chronic total occlusions, which were half of the lesions in this study, number of patent tibial arteries (runoff), and adjunctive devices were not related to the risk of MALE or repeat intervention, although these may be more important factors for tibial artery revascularization.
Study limitations
The limitations of this study include the observational design, which limits the interpretation of risk factors for outcomes, but does not detract from the description of the high rates of these outcomes over the decade of follow up. The proportions of men and White race were high, reflecting the VA group of patients. The Brigham and Women’s group sex and race breakdown was 40% women, 82% White, 9% Black, 5% Hispanic, and 5% unknown. The VA group were 96% White and 99% men. This compares to VA enrollees of all ages in New England in 2018 of 8% women, 93% White, 3% Black, and 3% Hispanic. 25 The reasons for low representation of women and minorities in the VA group may reflect an older age group where the proportion of women and minorities is lower than the data for all age groups, or misclassification of race and ethnicity, particularly of Hispanic ethnicity.26,27 However, the regional data suggest that minorities are less likely to enroll in the VA or have less access to revascularization, as indicated by other studies.6,21 These concerns justify the mission for equitable access to high-quality care in the VA and other healthcare systems.28,29 We were not able to assess the effect of more recent medications (e.g., PCSK9 inhibitors and direct oral anticoagulants), which based on recent trials would reduce the risk of MACCE. 9 Similarly, drug-coated balloons and stents were not available during the time of this study, but, based on recent trials with 5 years of follow up,16 –18,30 would decrease the need for reintervention and should be considered in these lesions as currently recommended by the Food and Drug Administration. 31 Medication use was based on prescribing from the medical chart and may not reflect fill-rates or actual use. We were not able to assess the impact of supervised exercise therapy, which was not approved during most of the follow-up time. The generalizability of the low MALE rates may reflect experienced endovascular operators and intensive surveillance over follow up that may not be available in all communities.
Conclusion
In this study of patients with femoral artery PAD treated by endovascular revascularization, who had high penetrance of guideline-directed medical therapy, durable outcomes over 10 years were achievable with close surveillance and mostly repeat endovascular revascularization as needed. Despite intensive atherosclerosis risk factor control, death rates over 10 years were high, and noncardiovascular deaths accounted for half of the overall deaths. Other contemporary therapies will likely decrease cardiovascular events, but decreasing smoking rates, preventing CKD, and other strategies to prevent cancer, may also be important targets for noncardiovascular death. These provide opportunities for specialists in vascular medicine to coordinate multidisciplinary efforts to reduce cardiovascular, noncardiovascular, and adverse limb events.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231174052 – Supplemental material for Patient and limb outcomes 10 years after endovascular revascularization of the superficial femoral artery for peripheral artery disease: The Boston Femoral Artery Endovascular Revascularization Outcomes (Boston FAROUT) study
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231174052 for Patient and limb outcomes 10 years after endovascular revascularization of the superficial femoral artery for peripheral artery disease: The Boston Femoral Artery Endovascular Revascularization Outcomes (Boston FAROUT) study by Scott Kinlay, Piotr Sobieszczyk, Andrew C Eisenhauer, Simon Ostrowski and Thomas M Todoran in Vascular Medicine
Footnotes
Data availability
Requests for data can be made to the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by a VA Clinical Science Research and Development Award 1/01CX001549 awarded to Scott Kinlay. Mortality data were provided by the Center of Excellence for Mortality Data Repository, Joint Department of Veterans Affairs and Department of Defense Suicide Data Repository – National Death Index, and by the Center for Disease Control National Death Index. The contents of this article do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.