
Abstract
There is a growing body of evidence that peripheral artery disease (PAD) may be impacted by depression. The objective of this study is to determine whether outcomes, primarily major amputation, differ between patients with depression and those without who presented to hospitals with critical limb ischemia (CLI), the end-stage of PAD. A retrospective cohort of patients hospitalized for CLI during 2012 and 2013 was identified from the National Inpatient Sample (NIS) using ICD-9 codes. The primary outcome was major amputation and secondary outcomes were length of stay and other complications. The sample included 116,008 patients hospitalized for CLI, of whom 10,512 (9.1%) had comorbid depression. Patients with depression were younger (64 ± 14 vs 67 ± 14 years, p < 0.001) and more likely to be female (55% vs 41%, p < 0.001), white (73% vs 66%, p < 0.001), and tobacco users (46% vs 41%, p < 0.001). They were also more likely to have prior amputations (9.8% vs 7.9%, p < 0.001). During the hospitalization, the rate of major amputation was higher in patients with comorbid depression (11.5% vs 9.1%, p < 0.001). In multivariable analysis, excluding patients who died prior to/without receiving an amputation (n = 2621), comorbid depression was associated with a 39% increased odds of major amputation (adjusted OR 1.39, 95% CI 1.30, 1.49; p < 0.001). Across the entire sample, comorbid depression was also independently associated with a slightly longer length of stay (β = 0.199, 95% CI 0.155, 0.244; p < 0.001). These results provide further evidence that depression is a variable of interest in PAD and surgical quality databases should include mental health variables to enable further study.
Introduction
Peripheral artery disease (PAD) is a global health problem with increasing incidence, 1 high economic burden, 2 and poor patient outcomes including associated cardiovascular disease, 3 disability, 4 and low quality of life. 5 PAD shares many traditional risk factors with cardiovascular disease (e.g. hypertension, smoking, and diabetes), 6 and ongoing research continues to highlight additional risk factors such as mental illness. The link between depression and vascular disease initially emerged in studies of patients with coronary artery disease (CAD).7,8 Although traditional risk factors including smoking and physical inactivity explain part of the association, 9 depression remains a strong independent risk factor for CAD. 10
Some preliminary evidence suggests that depression also affects outcomes among patients with PAD. For example, depression was associated with reduced walking distance 11 and greater pain at rest, even when adjusting for disease severity. 12 After peripheral vascular interventions (PVI), patients with depression achieve less functional benefit, 13 are more likely to experience restenosis, and continue to have worse symptoms. 14 They are also at higher risk for cardiovascular events and development of PAD in the other limb. 15 A recent retrospective cohort study from a VA database found that among veterans with incident PAD, those with comorbid depression had higher rates of mortality and major amputation. 16 However, no study has yet examined population-level civilian data to determine whether depression affects inpatient outcomes for those with critical limb ischemia (CLI), the most advanced stage of PAD.
Among patients hospitalized for vascular disease, depression has also been associated with worse inpatient outcomes. A study of patients undergoing elective coronary artery bypass grafting (CABG) found that those with higher depressive symptoms on the Beck Depression Inventory prior to CABG had increased odds of an inpatient stay greater than 1 week, believed to be mediated by persistently elevated high-sensitivity C-reactive protein (hs-CRP). 17 Supporting studies have found comorbid depression associated with higher mortality, length of stay, and resource utilization in surgical inpatients 18 as well as in patients hospitalized for cardiovascular disease 19 and heart failure. 20
This study examines whether comorbid depression is associated with worse outcomes for inpatients hospitalized for treatment of CLI, the most advanced stage of PAD, using the National Inpatient Sample (NIS), which is a nationwide database of patient hospitalizations. We hypothesize that our primary outcome of major amputation, as well as secondary outcomes of inpatient mortality and length of stay, would be higher in those with depression compared to those without depression.
Methods
Data source
Data were obtained from the NIS from 2012 and 2013 to enable a retrospective cohort study of patients with CLI, with and without depression. These were the most recent years of data available to our institution at the time data collection was conducted in 2017. Published annually by the Agency for Healthcare Research and Quality, the NIS is a patient-level administrative claims database that represents approximately 20% of discharges from US community hospitals, stratified by various hospital characteristics. The stratified systematic random sample contains de-identified discharge data from approximately 8 million hospitalizations annually. The NIS includes data on patient demographics, primary and secondary diagnoses, medical comorbidities, surgical procedures, length of stay, discharge disposition, and hospital charges that can be converted to estimate total costs. Information on hospital characteristics for each discharge is also available and includes size, geographic location, and teaching status.
Study population
Diagnoses and procedures performed during a single inpatient stay are identified in the NIS using the standard International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes. For the years 2012 and 2013, the NIS provides up to 25 diagnoses and 25 procedures for each hospitalization record. All adult patients (⩾ 18 years of age) primarily hospitalized for medical and/or surgical treatment for CLI were included in this study. The list of ICD-9-CM diagnosis and revascularization procedure codes, as well as the inclusion criteria used to select the study population, are available in online Supplemental Table 1 and were adapted from published studies by Agarwal et al.21,22 The codes for major amputation correspond to amputations of the lower limb, including the foot and ankle. The resulting cohort of hospitalized patients with CLI was stratified based on the presence or absence of comorbid depression, which was defined using ICD-9 diagnostic codes for major depression in a manner consistent with Arya et al. 16 (see online Supplemental Table 1 for complete ICD-9-CM definitions).
The following baseline patient characteristics were also collected: age, sex, race, smoking status, socioeconomic status (SES; defined as median income by quartile by residential code), and medical comorbidities (online Supplemental Table 1). The NIS provides information on 29 predefined comorbidities, as part of the Elixhauser Comorbidity Index, for each hospital discharge record based on previously defined ICD-9-CM codes. In addition to comorbid depression, the following Elixhauser comorbidities were collected to determine the prevalence of each disease in our patient population: congestive heart failure, chronic pulmonary disease, uncomplicated diabetes, diabetes with chronic complications, hypertension, liver disease, obesity, and renal failure. Furthermore, CAD, 16 prior amputation, 22 and tobacco use (current and former) 23 were added as additional comorbidities, using previously published methods, from codes available in the database.
Prior to initiating statistical analysis, the study was submitted to the University of California San Francisco (UCSF) Institutional Review Board (IRB) and determined to be exempt because the de-identified NIS does not involve human subjects research as defined by federal regulations.
Study outcomes
This study aimed to evaluate the relationship between comorbid depression and inpatient outcomes in patients hospitalized for CLI. The primary outcome of interest was major amputation, and secondary outcomes were hospital length of stay and inpatient mortality. While length of stay and inpatient mortality are directly coded in the NIS, major amputation was identified using ICD-9-CM codes consistent with prior studies.21,22 Additional outcomes such as rates of surgical and endovascular revascularization were also identified. Finally, rates for several potential complications including myocardial infarction (MI), pulmonary failure, deep vein thrombosis (DVT)/pulmonary embolism (PE), blood transfusion, pneumonia, acute renal failure, surgical site infection, and gastrointestinal bleed (GI) bleed were derived from prior publications and internally validated.24–27 Owing to limitations of the data source, including the difficulty of extracting complete data on the accurate timing of inpatient procedures, a longitudinal analysis could not be performed. Therefore, all outcomes were extracted from administrative billing records submitted after discharge.
Statistical analysis
Descriptive statistics were used to define our population of hospitalized patients with CLI based on age, sex, race, tobacco use, SES, comorbidities, revascularization procedures, perioperative complications, inpatient mortality, major amputation, and average length of stay. Baseline characteristics and outcomes among CLI inpatients with and without comorbid depression were compared by Student’s t-test for continuous variables and Fisher’s exact test for categorical variables. Because the length of stay had a rightward skew, it was reported as a median with its corresponding interquartile range and a non-parametric Wilcoxon rank sum test was used to compare those with and without comorbid depression.
Multivariable analyses were performed to determine the association between comorbid depression and the primary outcome of major amputation as well as secondary outcomes of length of stay and in-hospital mortality. Patients who died prior to discharge without receiving an amputation were excluded from multivariable analysis for major amputation (n = 2621) because it could not be determined whether they would, or would not, have undergone an amputation had they survived. Additionally, because length of stay was not normally distributed, it was log-transformed for multivariable analysis to improve model fit. The final models controlled for age, sex, race, SES, tobacco use, prior amputation, and comorbidities. A possible interaction between depression and sex was also investigated by the inclusion of an interaction term in the model. Furthermore, to exclude patients incorrectly identified as having CLI, a sensitivity analysis using a more restrictive definition of CLI was performed (see online Supplemental Table 1 for complete ICD-9-CM definitions). All statistical analyses were conducted using Stata 14 software (StataCorp, College Station, TX, USA).
Results
The primary definition of CLI yielded a sample of 116,008 patients hospitalized in 2012 and 2013, including 10,512 (9.1%) with comorbid depression. Those with depression were slightly younger (64.4 ± 13.7 vs 66.8 ± 13.7, p < 0.001) and more likely to be female (54.9% vs 40.9%, p < 0.001) and Caucasian (73.1% vs 65.8%, p < 0.001). They were more likely to report tobacco use (45.8% vs 40.7%, p < 0.001) and have several comorbidities, including obesity (15.5% vs 10.8%, p < 0.001), diabetes with chronic complications (25.0% vs 20.3%, p < 0.001), and prior amputation (9.8% vs 7.9%, p < 0.001). The full demographic and comorbidity results for the entire cohort, as well as depressed and non-depressed subgroups, are reported in Table 1. Overall, those who received an amputation had an inpatient mortality rate of 3.7% (n = 398) and those who did not receive an amputation had a mortality rate of 2.5% (n = 2621).
Characteristics of the full cohort and stratification by depression status (n = 116,008).
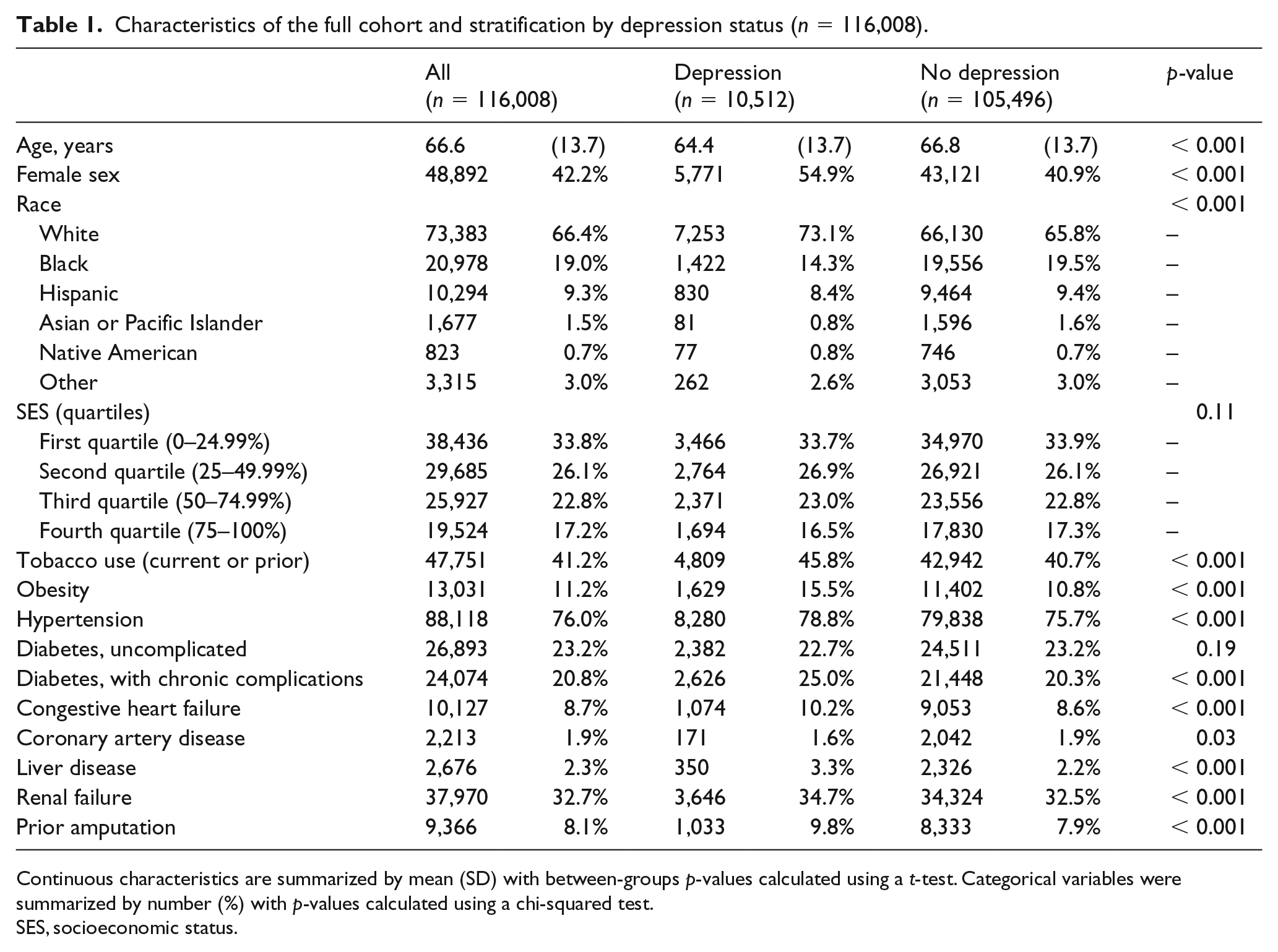
Continuous characteristics are summarized by mean (SD) with between-groups p-values calculated using a t-test. Categorical variables were summarized by number (%) with p-values calculated using a chi-squared test.
SES, socioeconomic status.
Comorbid depression was significantly associated with the primary outcome of major amputation (11.5% vs 9.1%, p < 0.001). Meanwhile, for the secondary outcomes, those with depression had a longer length of stay (6 days, IQR 3–10 vs 5 days, IQR 2–9; p < 0.001), but contrary to the hypothesis, were less likely to die during their hospitalization (1.8% vs 2.7%, p < 0.001). For other outcomes, the rates of surgical revascularization were slightly lower among those with depression (31.5% vs 35.0%, p < 0.001) and they were less likely to have an MI (2.5% vs 3.3%, p < 0.001). Otherwise, revascularization and complication rates were similar between groups (Table 2).
Outcomes across the full cohort and stratification by depression status (n = 116,008).
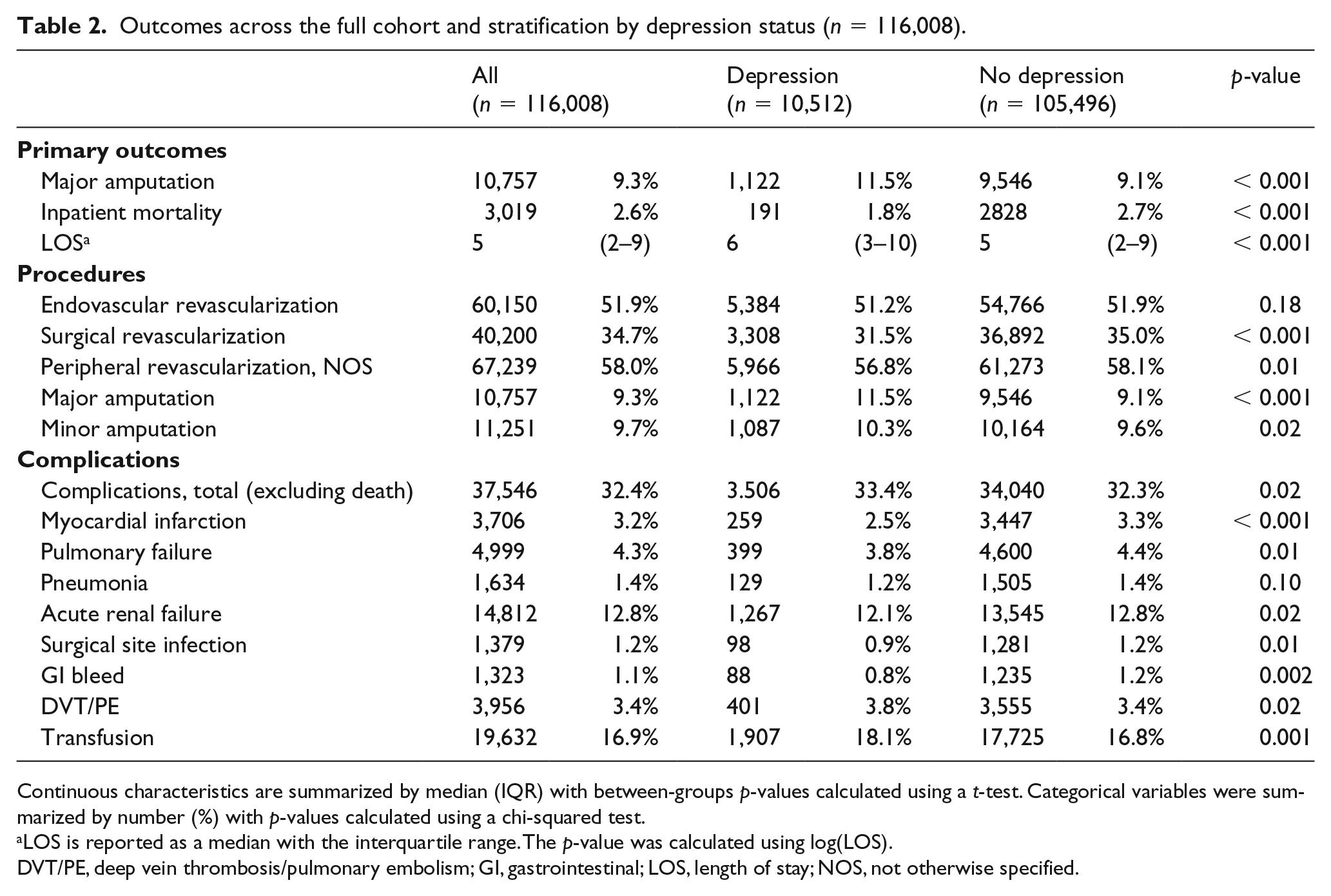
Continuous characteristics are summarized by median (IQR) with between-groups p-values calculated using a t-test. Categorical variables were summarized by number (%) with p-values calculated using a chi-squared test.
LOS is reported as a median with the interquartile range. The p-value was calculated using log(LOS).
DVT/PE, deep vein thrombosis/pulmonary embolism; GI, gastrointestinal; LOS, length of stay; NOS, not otherwise specified.
In a model controlling for age, sex, race, SES, and multiple medical comorbidities, including prior amputation (Table 3), inpatients with depression had 39% higher odds of receiving a major amputation during their hospitalization (adjusted OR 1.39, 95% CI 1.30, 1.49; p < 0.001). There was a significant interaction between sex and depression (p = 0.03), with men who have depression being 50% more likely to undergo an amputation compared to those without depression (adjusted OR 1.49, 95% CI 1.36, 1.64; p < 0.001), and women with depression being 32% more likely (adjusted OR 1.32, 95% CI 1.18, 1.44; p < 0.001). While the quantitative risk for men was higher, both men and women with depression experienced increased odds of major amputation. Furthermore, only a minority of patients undergoing major amputation had a procedure code for endovascular (18.3%) or surgical revascularization (13.6%). Finally, to address whether some of the patients with CLI receiving major amputations underwent amputations due to complications from diabetes rather than PAD, a sensitivity analysis was performed excluding patients who had diabetes with complications and found similar results (adjusted OR 1.44, 95% CI 1.32, 1.57; p < 0.001).
Multivariable analysis for major amputation, inpatient mortality, and LOS between those with and without depression.
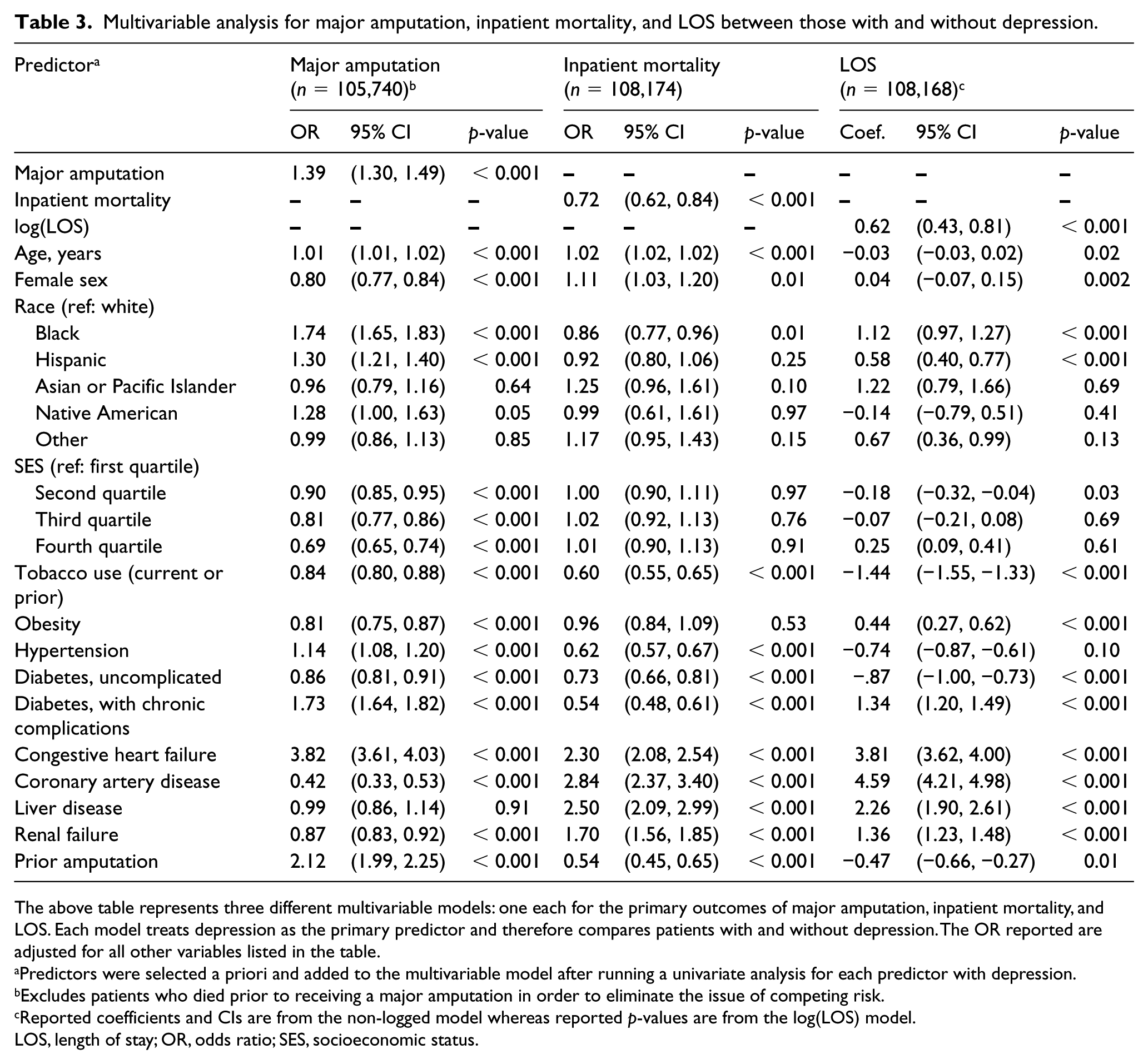
The above table represents three different multivariable models: one each for the primary outcomes of major amputation, inpatient mortality, and LOS. Each model treats depression as the primary predictor and therefore compares patients with and without depression. The OR reported are adjusted for all other variables listed in the table.
Predictors were selected a priori and added to the multivariable model after running a univariate analysis for each predictor with depression.
Excludes patients who died prior to receiving a major amputation in order to eliminate the issue of competing risk.
Reported coefficients and CIs are from the non-logged model whereas reported p-values are from the log(LOS) model.
LOS, length of stay; OR, odds ratio; SES, socioeconomic status.
Patients with comorbid depression also had a longer median length of stay (6 days, IQR 3–10, vs 5 days, IQR 2–9), even when limiting the analysis to patients who survived. Paradoxically, depression was independently associated with a lower risk of inpatient death (adjusted OR 0.72, 95% CI 0.62, 0.84; p < 0.001) despite higher odds of major amputation. Additional analyses were performed to determine whether receiving an amputation reduced the odds of subsequent death during the hospitalization. Across the entire sample, patients who had a major amputation had a higher rate of inpatient mortality (3.7% vs 2.5%, p < 0.001). Repeating the inpatient mortality model (reported in Table 3), but restricting it to only those who did not have a major amputation at any point during the hospitalization, yielded similar results, with depression associated with decreased odds of death (adjusted OR 0.71, 95% CI 0.60, 0.85; p < 0.001). As a result, while patients with depression were more likely to undergo amputation, there was no evidence that this reduced their likelihood of inpatient death.
Finally, a sensitivity analysis was performed using a more restrictive definition of CLI as described in online Supplemental Table 1 to determine whether the definition of ICD-9 codes used for CLI affected the key findings. The restricted sample included 91,133 patients and the results of the multivariable analysis were similar to the initial findings (online Supplemental Table 2). Comorbid depression was associated with greater odds of major amputation (adjusted OR 1.42, 95% CI 1.32, 1.52; p < 0.001) and a longer LOS (adjusted coef. 0.74, 95% CI 0.56, 0.94; p < 0.001). Meanwhile, comorbid depression was again associated with lower odds of inpatient mortality (adjusted OR 0.78, 95% CI 0.65, 0.94; p = 0.008).
Discussion
In this nationally representative inpatient cohort, we found that comorbid depression was independently associated with increased risk of major amputation in patients admitted for CLI. It was also associated with a prolonged LOS and paradoxically decreased odds of inpatient death. The increased rate of amputation may be explained in part by confounding risk factors such as age and comorbid disease burden; however, patients with depression were younger and multiple comorbidities were included in the adjusted analysis. Given the large sample size and multiple potential confounders included in the multivariable model, an adjusted OR of 1.39 for major amputation may be clinically significant. While the NIS is limited in terms of the clinically relevant information it provides, and the possibility of residual confounding remains, these findings provide evidence supporting existing literature of a relationship between depression and worse vascular outcomes.
Depression is a well-recognized risk factor for CAD, 28 and given similar etiology and pathogenesis between CAD and PAD, depression has recently been explored as a risk factor for PAD. Among patients with PAD, depression has been associated with disease progression, 15 impaired walking capacity, 29 worse surgical outcomes, 14 and increased overall mortality. 30 As demonstrated in this sample, patients with depression are more likely to be female, obese, and tobacco smokers, and more likely to have comorbidities that increase cardiovascular risk, including complicated diabetes, heart failure, liver disease, and renal failure. These social and behavioral characteristics and medical comorbidities only partially account for the poor outcomes discussed above. 31 Therefore, the mechanisms linking depression and vascular disease warrant further investigation 32 and a recent review proposes several behavioral as well as biological mechanisms. 33
The potential mechanisms include dysfunction of the autonomic nervous system, 34 hypothalamic-pituitary-adrenal axis, 35 platelet activity,36,37 and endothelial function.38,39 Depression has also been associated with elevated levels of inflammatory markers,40–42 and Hernandez et al. found increasing levels of inflammation associated with a higher burden of depressive symptoms as measured by the Patient Health Questionnaire - 9 (PHQ-9) in veterans with PAD. 43 Thus, these mechanisms suggest pathways in which CLI could be more severe in patients with depression, increasing the risk of major amputation. Additionally, patients with worse revascularization outcomes 14 are at a higher risk of amputation. However, the NIS lacks variables to define the severity of CLI (e.g. Rutherford, Fontaine classifications), so the present study cannot definitively determine if patients with depression had more severe disease upon their hospital admission. While in some cases a major amputation might have followed a failed revascularization procedure during the hospitalization, most patients who had an amputation did not undergo a revascularization procedure during the same hospitalization.
Additionally, comorbid depression has been associated with prolonged hospital stays in patients admitted with cardiovascular disease or heart failure. These studies attributed increased LOS to a greater burden of medical comorbidities, worse self-care, poor compliance with medications, and differences in discharge planning, although these explanations have not been rigorously proven. 44 We found that depression was associated with prolonged hospital stay among patients admitted for CLI, and these findings are consistent with existing literature.
The unexpected finding that depression was associated with reduced in-hospital mortality is intriguing. In a study of surgical patients admitted to the ICU, those with comorbid depression had adjusted ORs of 1.19 (95% CI 1.02, 1.38) for in-hospital mortality and 1.23 (95% CI 1.05, 1.43) for 30-day mortality when compared to patients without depression. Specifically, among patients with PAD, a recent study not restricted to the inpatient setting found that for veterans with incident PAD, those with comorbid depression had a 17% higher risk of mortality in an adjusted analysis (hazard ratio 1.17, 95% CI 1.14, 1.20). 16 Another study of patients undergoing lower extremity revascularization also found higher rates of mortality among those with comorbid depression. 15 Instead, the findings of the present study suggest that depression is protective against in-hospital mortality; however, our data do not allow us to assess the impact of depression on mortality following the immediate admission period.
While patients with depression were more likely to undergo amputation, there was no evidence that amputation reduced the risk of death. In fact, patients undergoing major amputation were more likely to die and restricting the analysis to only patients who did not undergo amputation at any point during their hospitalization did not affect the results. Abrams et al. suggested that inpatient mental health codes could be a proxy for a lower severity hospital course and that these patients were less likely to have complicated hospital courses with long lists of high priority billing codes, making depression more likely to be coded. 45 Therefore, prospective studies are needed to examine the association between depression and mortality in patients with CLI.
Further elucidation of the pathways linking depression and PAD is crucial to improving care in populations with these diseases. Better understanding of this relationship between mental and physical well-being could lead to discoveries of new treatment methods (such as anti-inflammatories or fish oil supplementation) as well as alter the standard of how clinicians manage surgical patients with these comorbidities by better managing mental health. The American Heart Association has recently begun to recognize depression as a risk factor for coronary artery atherosclerosis and currently recommends depression screening in these individuals. 46 We suggest further exploration of depression as a modifiable risk factor for PAD and encourage increased awareness in the surgical community of the effects that mental health can have on vascular disease. A concrete step forward would be to collect mental health variables in surgical and vascular health databases such as the National Surgical Quality Improvement Project (NSQIP) or Vascular Quality Initiative (VQI).
Limitations
While the study was well powered with a large, nationally representative sample, the major limitation was its restriction to a single inpatient stay, which prevented determination of causality. Additionally, as with any observational study utilizing billing records, the analyses could be affected by unmeasured confounders. Since the NIS is an inpatient administrative database, the analysis was limited to the information and variables obtainable from billing codes. This could introduce bias and variability of diagnoses and procedures depending on how likely physicians were to code for depression and how accurate their depression diagnoses were. For defining CLI, the present study utilized code combinations that have been previously reported 21 and tried to address variability by doing sensitivity analyses. Additional limitations include lack of clinical measurements that would indicate PAD or depression severity at the time of hospital admission, as well as lack of data on medication use, medication compliance, or lab data that could suggest an underlying physiologic mechanism (e.g. high-sensitivity C-reactive protein). Additionally, there were no data on history of prior lower extremity revascularization, and, since a prior intervention would increase the risk of an amputation, this is an important unmeasured confounder. While the effect size of the association for the primary outcome of major amputation may be clinically significant, the clinical quality and utility of administrative databases such as the NIS is inferior to that of clinical quality databases such as VQI or NSQIP, and the potential for residual confounding remains.
Conclusion
Using a large representative nationwide sample, this study demonstrates that depression is independently associated with a 39% increased odds of major amputation in patients admitted for CLI. This is consistent with previous literature documenting worse outcomes in patients with PAD and depression, and provides further evidence that depression should be more widely recognized as a risk factor for worse outcomes in PAD. Additionally, this further supports collection of depression measurements in databases that measure the quality and outcomes of surgical procedures. In conclusion, this study informs physicians of the health impacts of depression and could establish a more accurate risk assessment of patients with comorbid depression. Future studies can help ascertain whether depressed patients delay seeking care and present later in the disease course, as well as whether these patients would benefit from earlier interventions including antidepressant use.
Supplemental Material
10.1177_1358863X19880277_Supplemental_tables – Supplemental material for Association of comorbid depression with inpatient outcomes in critical limb ischemia
Supplemental material, 10.1177_1358863X19880277_Supplemental_tables for Association of comorbid depression with inpatient outcomes in critical limb ischemia by Greg J Zahner, Abigail Cortez, Erin Duralde, Joel L Ramirez, Sue Wang, Jade Hiramoto, Beth E Cohen, Owen M Wolkowitz, Shipra Arya, Nancy K Hills and S Marlene Grenon in Vascular Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge the work and guidance of Janet Coffman and Jennifer Creasman in helping us select an appropriate database and extract relevant data from the NIS.
Authors’ note
The abstract was presented at the Arteriosclerosis, Thrombosis, and Vascular Biology Annual Conference 2018, San Francisco, CA, USA, May 9-12, 2018.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through UCSF-CTSI Grant Number TL1 TR001871, with additional student research support from the Society for Vascular Surgery Student Research Fellowship Award and the American Heart Association Student Scholarship (Dr Zahner). Furthermore, this work was supported by start-up funds from the University of California San Francisco and the Northern California Institute for Research and Education, by Award Number KL2RR024130 from the National Center for Research Resources, Award Number 1K23HL122446-01 from the National Institutes of Health/NHLBI, and a Society for Vascular Surgery Seed Grant and Career Development Award (Dr Grenon). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health. The funding organizations were not involved in the design and conduct of the study, collection, management, analysis, and interpretation of the data, or preparation, review or approval of the manuscript.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.