
Abstract
Background:
Hispanic and Latino patients are under-represented in existing healthcare disparities research in pulmonary embolism (PE). The goal of this study was to determine if differences in PE severity, treatment modality, or in-hospital outcomes exist for Hispanic or Latino patients with PE.
Methods:
All PE cases from 2013 to 2019 at a single institution were reviewed. Clinical characteristics, imaging findings, intervention types, and in-hospital and 30-day outcomes were collected. Two cohorts were created based on patients’ self-reported ethnicity. Outcomes were compared using univariate and multivariate analysis.
Results:
A total of 1265 patients were identified with confirmed PE; 474 (37%) identified as Hispanic or Latino. Hispanic or Latino patients presented with high-risk PE significantly less often (19% vs 25%, p = 0.03). On univariate analysis, Hispanic or Latino patients had lower rates of PE-specific intervention (15% vs 19%, p = 0.03) and similar rates of inpatient mortality (6.8% vs 7.5%, p = 0.64). On ordinal regression analysis, Hispanic or Latino ethnicity was associated with lower PE severity (OR 0.69, 95% CI 0.54–0.89, p = 0.003). In subgroup analyses of intermediate and high-risk PEs, ethnicity was not a significant predictor of receipt of PE-specific intervention or in-hospital mortality.
Conclusions:
At this institution, Hispanic or Latino patients were less likely to present with high-risk PE but had similar rates of inpatient mortality. Future research is needed to identify if disparities in in-hospital care are driving perceived differences in PE severity and what addressable systematic factors are driving higher-than-expected in-hospital mortality for Hispanic or Latino patients.
Background
Pulmonary embolism (PE) is a leading cause of mortality worldwide and is the primary cause of more than 36,000 deaths and 180,000 hospitalizations each year in the United States (US) alone. 1 Unfortunately, there is an ever-growing body of evidence demonstrating that disparities exist in both access to care and quality of care received for PE in the US.2,3 When compared to White Americans, Black Americans have been shown to have an elevated incidence of venous thromboembolism (VTE) and are almost twice as likely to be hospitalized on presentation. 4 When hospitalized, the likelihood of procedural intervention is significantly lower, 5 and these patients suffer an almost 50% higher age-adjusted PE-related mortality.6,7
Despite existing literature clearly demonstrating racial disparities in VTE care between White and Black patients, research has been limited in examining disparities with regards to ethnicity. This is likely due to both a focus on race and how race and ethnicity data are structured. Although the relationship between race and ethnicity is complex and multifaceted, existing categorization systems used by hospitals and national databases typically follow the US Census Bureau definitions and consider race (e.g., White, Black, Asian, Native Hawaiian/Pacific Islander, Native American or Alaskan Native, two or more races, or other) and ethnicity (e.g., Hispanic or Latino or Non-Hispanic nor Latino) separate categories.8–10 In the 2020 census, only 22% of Hispanic or Latino patients identified as White or Black, with almost 75% identifying as two or more or other races. 11 Analyses focusing on Black versus White race or excluding the groups ‘other’ or ‘two or more’ races end up excluding the majority of Hispanic or Latino patients. This helps to explain why Hispanic or Latino patients comprise < 1% of existing PE study cohorts despite making up almost 19% of the US population.5,12–15
The goal of this study was to address this gap by focusing specifically on ethnicity and utilizing data from a single institution located in a predominantly Hispanic and Latino neighborhood of New York City. Existing disparities research in PE has demonstrated a complex interplay between race, disease severity, and PE outcomes. 16 Given Hispanic or Latino patients bear a greater burden of severe disease with respect to many health conditions in the US,17–19 this study investigates the relationship between ethnicity and disease severity for Hispanic or Latino patients with PE. This study also evaluates the impact ethnicity and disease severity have on both in-hospital PE management and outcomes to identify potential inequities in healthcare delivery. The authors hypothesized that Hispanic or Latino patients would have a higher incidence of high-risk PE, a lower incidence of surgical or catheter-based intervention, and a higher likelihood of in-hospital and 30-day mortality after adjusting for clinical characteristics when compared to non-Hispanic or Latino patients.
Methods
Data collection and cohort definition
A retrospective analysis of all adult patients (> 18 years old) diagnosed with PE at a large, academic medical center in New York City from January 2013 through June 2019 was conducted; 1898 possible cases were identified. All charts were manually reviewed and cases without radiographic or echocardiographic evidence of PE were excluded (n = 478, 25%). Cases missing demographic data or clinical characteristics (n = 155, 11%) were then excluded from the analysis, yielding a final study population of 1265 patients (Figure 1). The institutional review board at the principal investigator’s institution approved this study and waived the requirement for informed consent (protocol AAAQ2600).
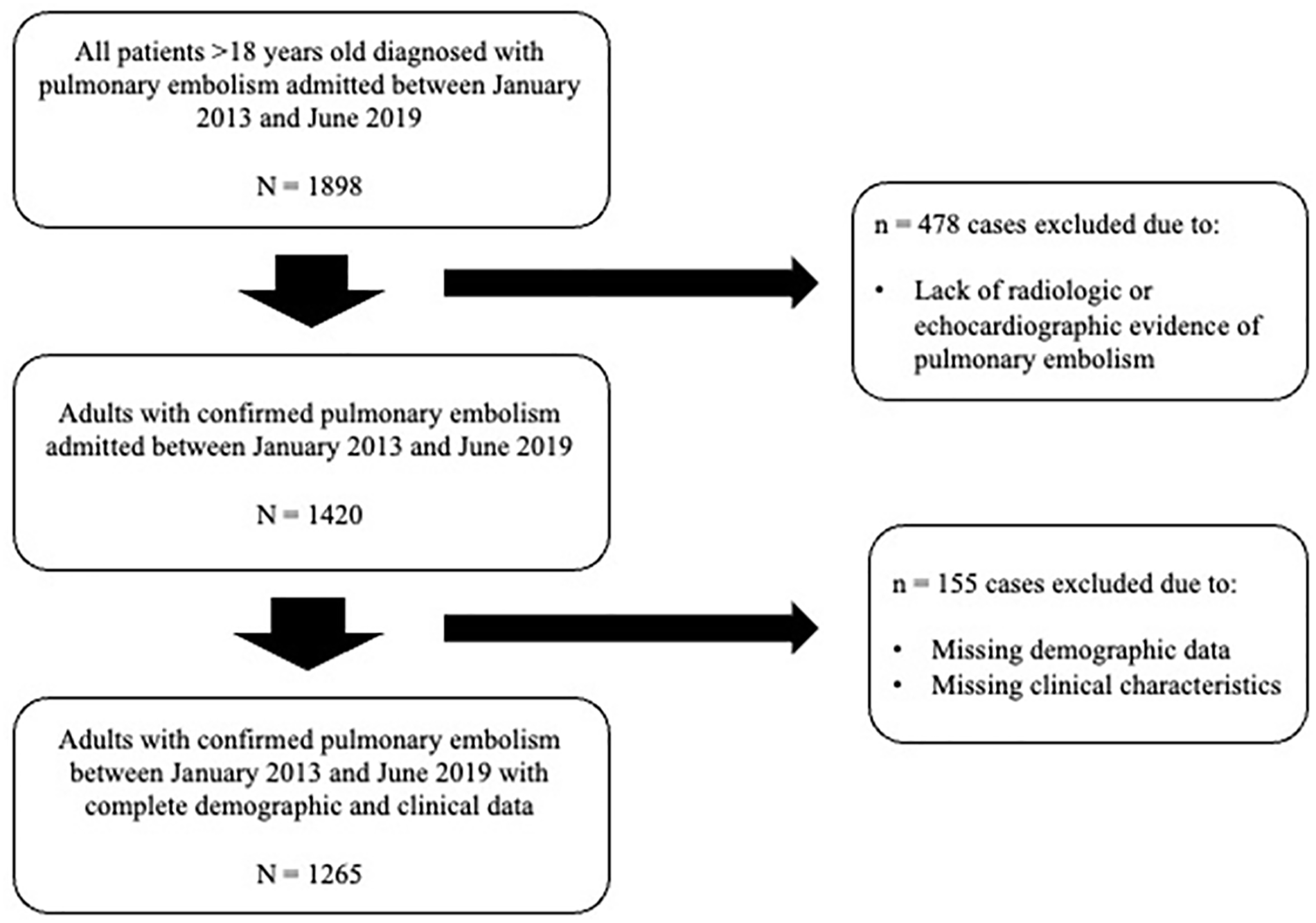
Study flow diagram.
Variables collected
Demographic data were extracted from the electronic medical record (EMR), including age, sex, race, and ethnicity, all of which were self-reported by the patient. Ethnicity was reported according to the standards described in the Journal of the American Medical Association by Flanagin et al., with the term Hispanic encompassing people originating from Spain or other Western Spanish-speaking countries and the term Latino encompassing those originating from Cuba, Mexico, Puerto Rico, and some countries in Central or South America and the Caribbean. 20 Race and ethnicity were considered independent variables as defined by the US Census Bureau, with Hispanic or Latino and non-Hispanic or Latino patients being able to identify as any race (excluding White, Black, Asian, Native Hawaiian/Pacific Islander, Native American or Alaskan Native), two or more races, other race, or not report their race at all. 11
Baseline clinical characteristics were also extracted from the EMR, including body mass index (BMI) and smoking, as well as a history of hypertension, diabetes, heart failure, chronic lung disease, end-stage renal disease (ESRD), or cerebrovascular accident (CVA). Specific risk factors for venous thromboembolism (VTE) were also collected, including prior VTE, malignancy, current hormone use, recent immobilization, and recent surgery or trauma. 21
Vital signs (systolic blood pressure, mean arterial pressure, heart rate, respiratory rate, oxygen saturation) and supplemental oxygen requirement during the first 24 hours after presentation were then extracted. Patients were categorized as having hemodynamic instability if they had a sustained systolic blood pressure less than 90 mmHg or a vasopressor requirement. 22 Presenting vital signs along with demographic and clinical characteristics were utilized to assign each patient a PE Severity Index (PESI) score and Simplified PESI (sPESI) score.23,24 If available, the first transthoracic echocardiogram (TTE) after admission was reviewed by a cardiologist board certified in echocardiography to identify patients with signs of right ventricular (RV) dysfunction (e.g., increased RV size, decreased RV function, RV pressure overload, RV volume overload, McConnell’s sign, or presence of an intracardiac thrombus). 22
RV size and function were assessed qualitatively and TTE readers were blinded to patient ethnicity. The presence and timing of interventricular septum flattening were utilized to identify patients with RV volume overload and/or RV pressure overload. Septal shift away from the center of the RV solely at end-diastole signified isolated RV volume overload, and a shift at both end-systole and end-diastole signified RV pressure overload.25,26 Cardiac biomarkers were also collected including Troponin I, Troponin T, B-type natriuretic peptide (BNP), and N-terminal prohormone BNP (NT-proBNP). Biomarker values were compared to reference values for each test to identify patients with elevated biomarker levels. If available, computed tomography angiography (CTA) images and interpretations were reviewed to identify PE location. Cases admitted to the intensive care unit (ICU), intubated, or cannulated to extracorporeal membrane oxygenation (ECMO) were also identified.
Outcome measures
The primary outcome of interest was PE severity. Cases were classified as high risk, intermediate–high risk, intermediate–low risk, or low risk according to the 2019 European Society of Cardiology (ESC) Guidelines. 22 Secondary outcomes of interest included treatment modality along with in-hospital all-cause mortality, in-hospital PE-related mortality, GUSTO (Global Use of Strategies to Open Occluded Arteries bleeding criteria) moderate or severe bleeding, 30-day all-cause mortality, 30-day PE-related mortality, and readmission rate. Mortality was considered PE-related if PE was either the immediate cause of death, a contributor to the cause of death, or if the cause of death occurred as a complication of PE treatment. Treatment modality was categorized as either systemic lytic therapy, targeted intervention (surgical embolectomy, pulmonary thromboendarterectomy, catheter thrombectomy, or catheter-directed thrombolysis), or preventative therapy (inferior vena cava filter placement). 5 Patients were classified as receiving PE-specific intervention if they received systemic lytic therapy, a targeted intervention, or preventative therapy as opposed to anticoagulation (AC) alone.
Statistical analysis
All statistical analyses were performed in SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA). A two-tailed p-value of 0.05 was considered significant. Two cohorts were created based on patients’ self-reported ethnicity: Hispanic or Latino and non-Hispanic or Latino. Demographic and clinical characteristics along with presenting characteristics were compared between cohorts using univariate analysis. Continuous variables were presented as mean (SD) or median (IQR) and compared using Student’s t-tests or Mann–Whitney U-tests depending on the normality of the data distribution. Categorical variables were presented as frequency (percentage) and compared using chi-squared tests and Fisher’s exact tests when necessary. Next, PE severity, receipt of PE-specific intervention, and in-hospital and 30-day outcomes were compared between cohorts using univariate analysis. Ordinal regression was then utilized to determine if ethnicity was a predictor of higher PE severity on presentation. Binary logistic regression was utilized to determine if ethnicity was associated with receipt of PE-specific intervention and in-hospital and 30-day outcomes. Unadjusted models were created as well as models adjusted for clinical characteristics (age, sex, BMI ⩾ 35 mg/kg, recent surgery, and prior VTE). 5 Given ethnicity was associated with PE severity, subgroup analyses of high-risk and intermediate-risk PEs were performed to determine if ethnicity was associated with receipt of targeted or systemic intervention within each risk category. Following this initial analysis, a supplemental analysis utilizing the same univariate and multivariate methods described above was performed to compare PE severity, treatment strategy, and outcomes between Black and White patients in the study population.
Results
Baseline characteristics
A total of 1265 patients were included in the study population; 474 patients (37%) identified as Hispanic or Latino (Table 1). The majority (63%) of Hispanic or Latino patients either opted to not report their race or identified as two or more or other races. When compared to non-Hispanic or Latino patients, Hispanic or Latino patients had a significantly higher proportion of diabetes (28% vs 18%, p < 0.0001), heart failure (14% vs 10%, p = 0.02), and prior CVA (11% vs 7.1%, p = 0.01), and a lower proportion of chronic lung disease (17% vs 22%, p = 0.04). The frequency of VTE risk factors did not significantly differ between the two cohorts (Table 1). A comparison of baseline characteristics between Black and White patients in the study population can be found in the online supplemental material (Table S1).
Baseline characteristics of the study population.
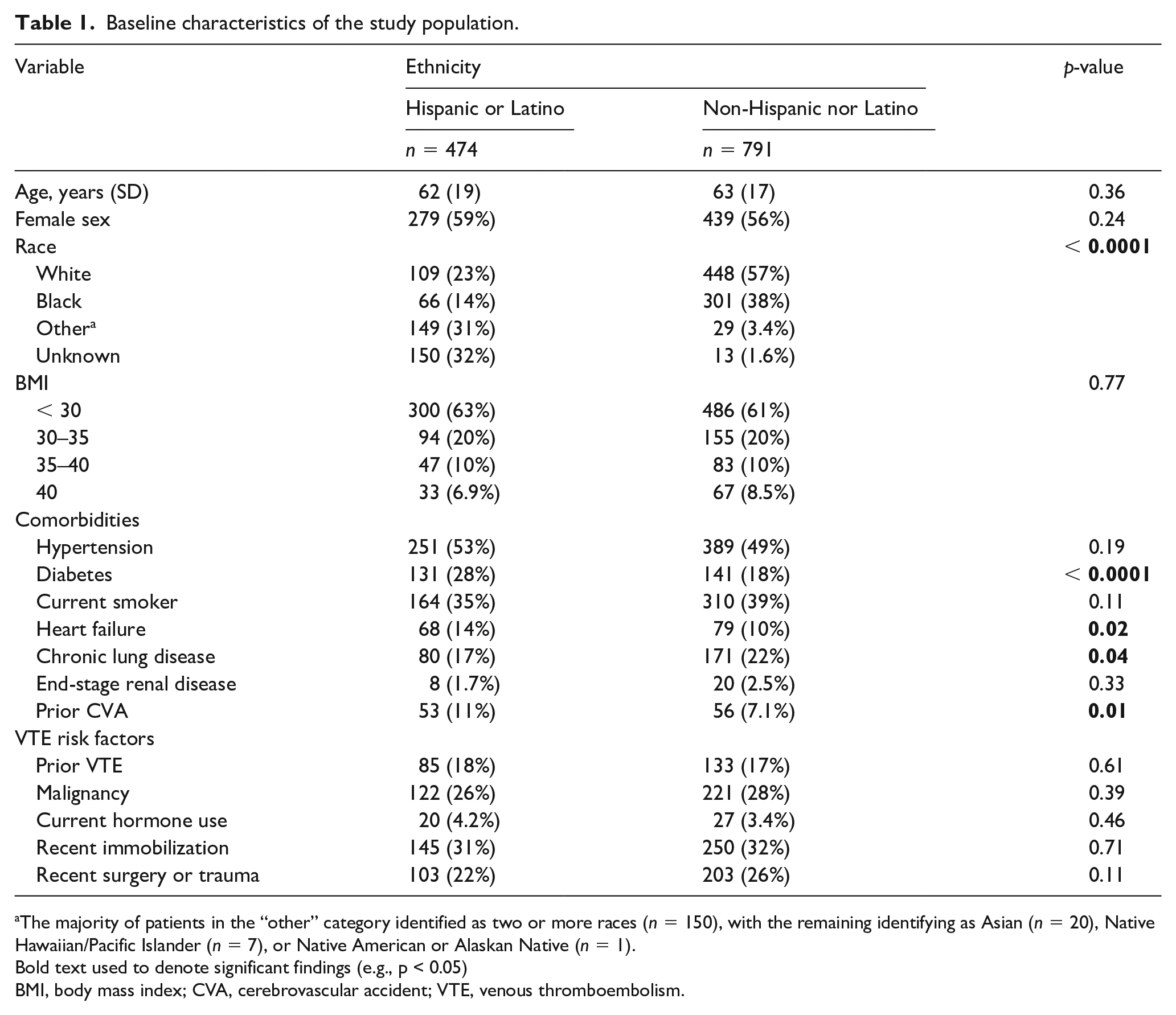
The majority of patients in the “other” category identified as two or more races (n = 150), with the remaining identifying as Asian (n = 20), Native Hawaiian/Pacific Islander (n = 7), or Native American or Alaskan Native (n = 1).
Bold text used to denote significant findings (e.g., p < 0.05)
BMI, body mass index; CVA, cerebrovascular accident; VTE, venous thromboembolism.
Presenting characteristics
Hispanic or Latino patients had a lower frequency of hemodynamic instability (19% vs 25%, p = 0.02) and supplemental oxygen need on presentation (44% vs 53%, p = 0.001) (Table 2). PESI and sPESI classes did not differ significantly between ethnicities. On TTE, Hispanic or Latino patients had a higher frequency of normal RV size (59% vs 49%, p = 0.0006) and function (61% vs 55%, p = 0.28), and a lower frequency of RV volume overload (11% vs 16%, p = 0.04) and intracardiac thrombus (0.5% vs 2.5%, p = 0.02). When analyzing cardiac biomarker elevations, the frequency of BNP elevation in Hispanic and Latino patients was significantly lower (69% vs 80%, p = 0.0002) and the frequency of troponin elevation in Hispanic and Latino patients was substantially lower (43% vs 50%, p = 0.06). There were no differences in the frequency of biomarker testing between ethnicities. PE location also did not differ significantly between ethnicities (Table 2). After presentation, Hispanic or Latino patients had lower rates of vasopressor support and ICU disposition (10% vs 16% and 27% vs 38%, respectively) as well as lower rates of ECMO use (1.3% vs 3.3%) (all p < 0.01). A comparison of presenting characteristics and illness severity between Black and White patients can be found in the online supplementary material (Table S2).
Presenting characteristics and illness severity compared by patient ethnicity.
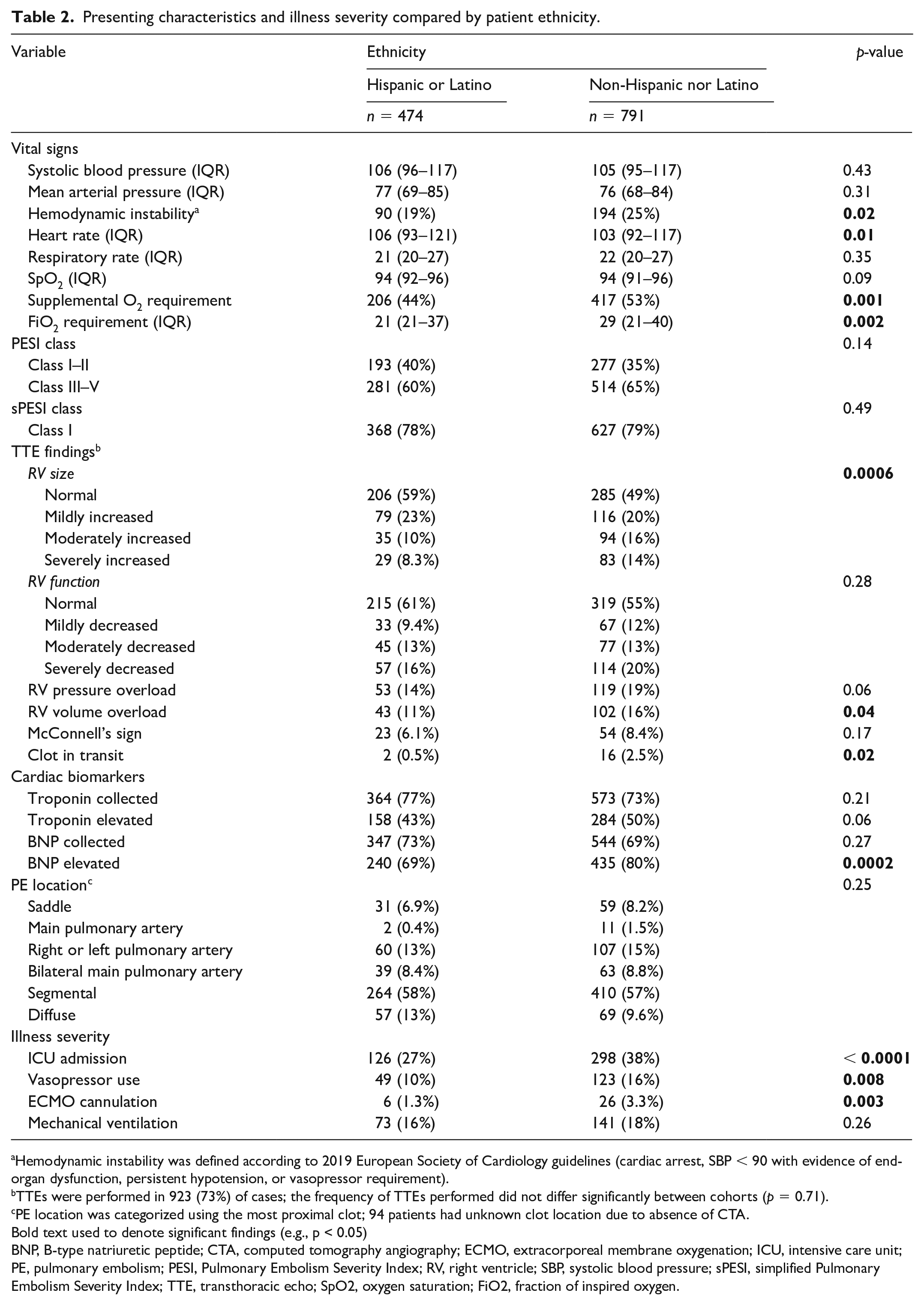
Hemodynamic instability was defined according to 2019 European Society of Cardiology guidelines (cardiac arrest, SBP < 90 with evidence of end-organ dysfunction, persistent hypotension, or vasopressor requirement).
TTEs were performed in 923 (73%) of cases; the frequency of TTEs performed did not differ significantly between cohorts (p = 0.71).
PE location was categorized using the most proximal clot; 94 patients had unknown clot location due to absence of CTA.
Bold text used to denote significant findings (e.g., p < 0.05)
BNP, B-type natriuretic peptide; CTA, computed tomography angiography; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; PE, pulmonary embolism; PESI, Pulmonary Embolism Severity Index; RV, right ventricle; SBP, systolic blood pressure; sPESI, simplified Pulmonary Embolism Severity Index; TTE, transthoracic echo; SpO2, oxygen saturation; FiO2, fraction of inspired oxygen.
Risk categorization and receipt of PE-specific intervention
When compared to non-Hispanic or Latino patients, Hispanic or Latino patients presented with high-risk PE significantly less often (19% vs 25%, p = 0.03) and had a significantly lower frequency of PE-specific intervention (15% vs 19%, p = 0.03) (Table 3). On ordinal regression analysis, Hispanic or Latino patients were significantly less likely to present with a higher-risk PE (OR 0.69, 95% CI 0.54–0.89, p = 0.003) than non-Hispanic or Latino patients, even after correcting for baseline clinical characteristics (OR 0.71, 95% CI 0.56–0.91, p = 0.007) (Table 4). Hispanic or Latino patients were also significantly less likely to receive any PE-specific intervention (OR 0.71, 95% CI 0.52–0.97, p = 0.03) or any targeted intervention (OR 0.55, 95% CI 0.36–0.85, p = 0.007) than non-Hispanic or Latino patients. These differences persisted even after adjustment for clinical characteristics (Table 4). On subgroup analysis within each PE risk category, however, ethnicity was not associated with a difference in likelihood of PE-specific intervention for high-risk or intermediate-risk PE (Table 5).
Risk categorization, treatment modality, and outcomes compared by patient ethnicity.
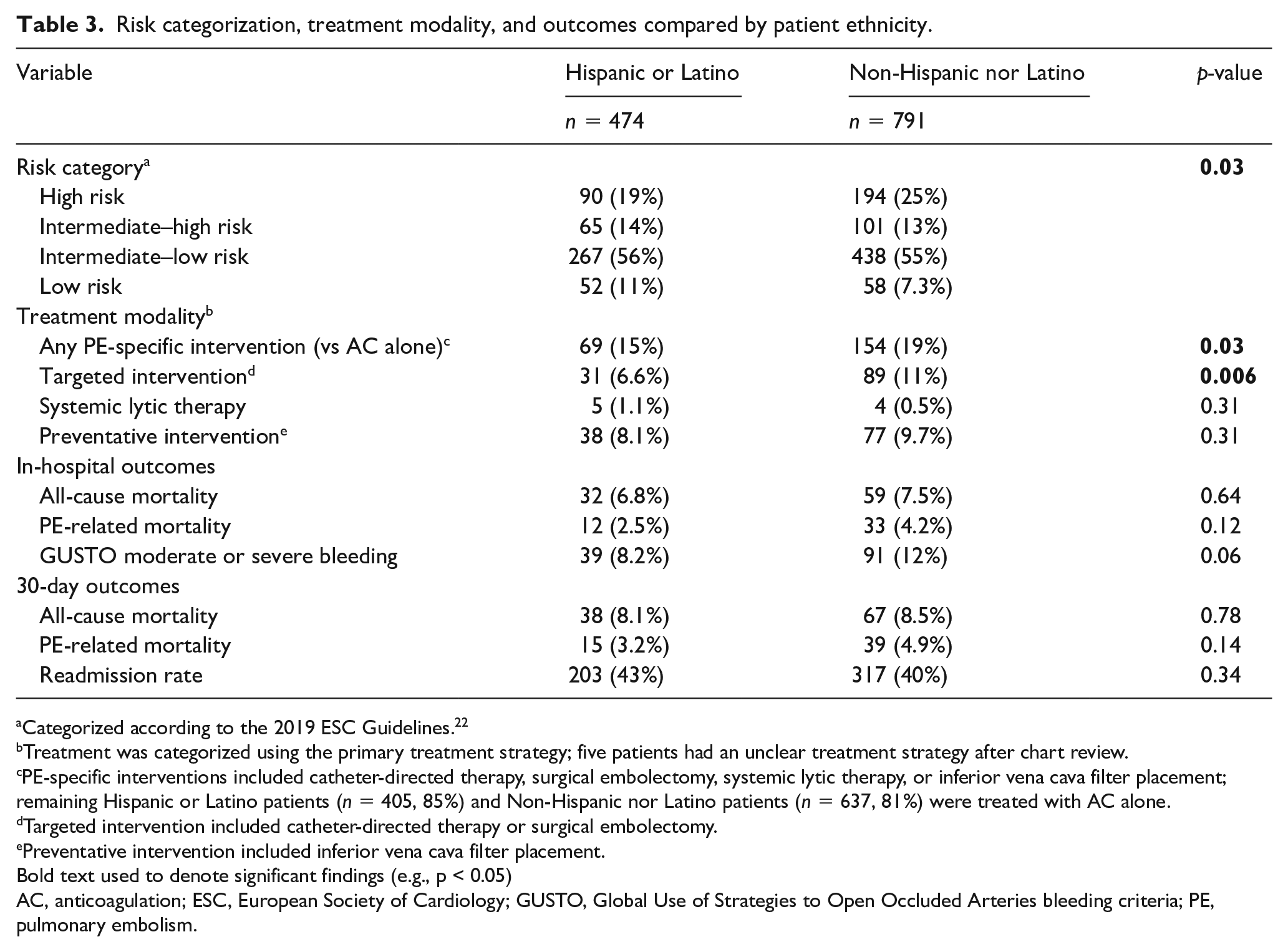
Categorized according to the 2019 ESC Guidelines. 22
Treatment was categorized using the primary treatment strategy; five patients had an unclear treatment strategy after chart review.
PE-specific interventions included catheter-directed therapy, surgical embolectomy, systemic lytic therapy, or inferior vena cava filter placement; remaining Hispanic or Latino patients (n = 405, 85%) and Non-Hispanic nor Latino patients (n = 637, 81%) were treated with AC alone.
Targeted intervention included catheter-directed therapy or surgical embolectomy.
Preventative intervention included inferior vena cava filter placement.
Bold text used to denote significant findings (e.g., p < 0.05)
AC, anticoagulation; ESC, European Society of Cardiology; GUSTO, Global Use of Strategies to Open Occluded Arteries bleeding criteria; PE, pulmonary embolism.
Univariate and multivariate regression analyses evaluating the impact of patient ethnicity on PE risk categorization, likelihood of intervention, and outcomes.
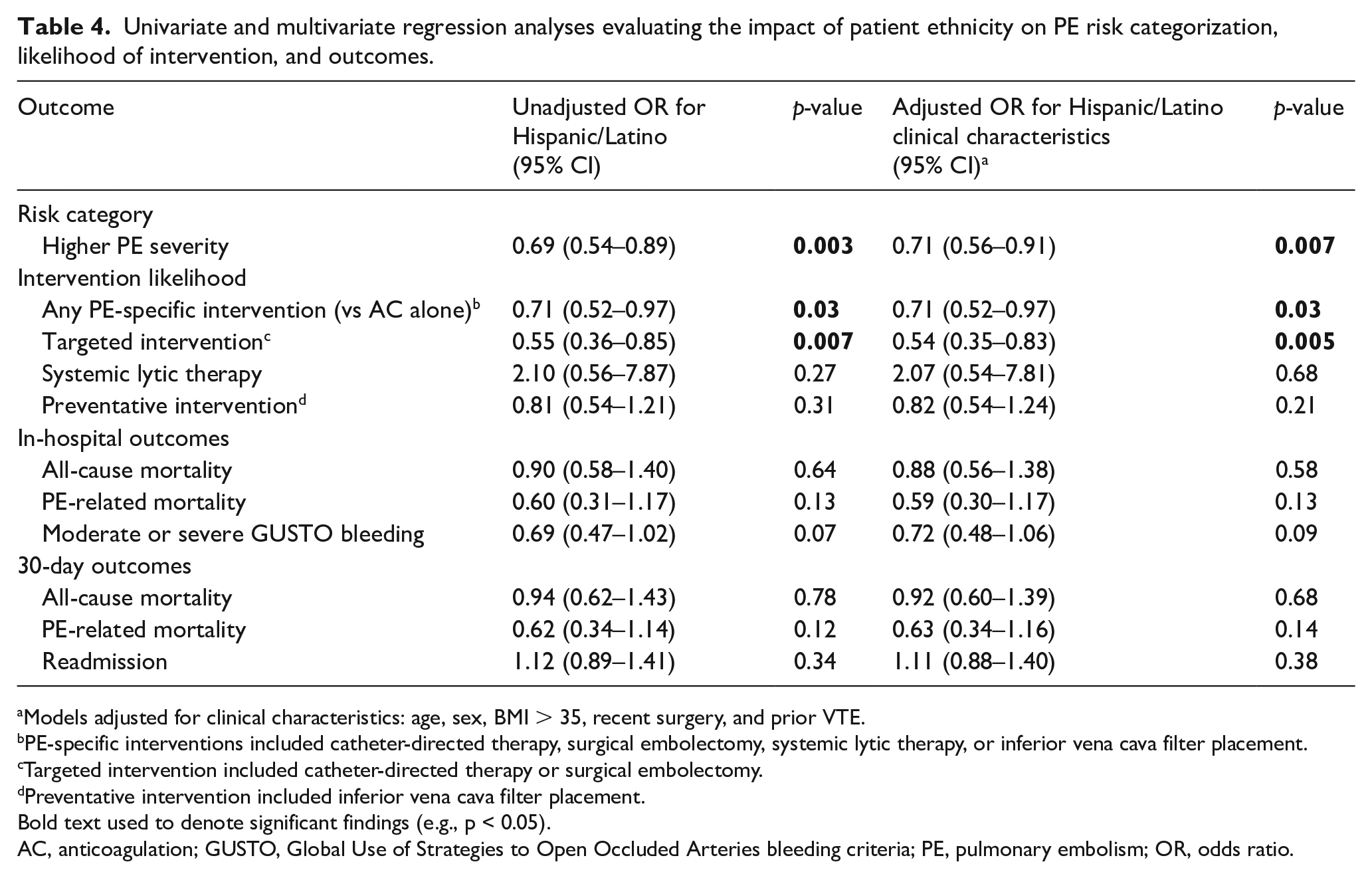
Models adjusted for clinical characteristics: age, sex, BMI > 35, recent surgery, and prior VTE.
PE-specific interventions included catheter-directed therapy, surgical embolectomy, systemic lytic therapy, or inferior vena cava filter placement.
Targeted intervention included catheter-directed therapy or surgical embolectomy.
Preventative intervention included inferior vena cava filter placement.
Bold text used to denote significant findings (e.g., p < 0.05).
AC, anticoagulation; GUSTO, Global Use of Strategies to Open Occluded Arteries bleeding criteria; PE, pulmonary embolism; OR, odds ratio.
Subgroup analysis of high-risk and intermediate-risk PE comparing the likelihood of intervention by patient ethnicity.
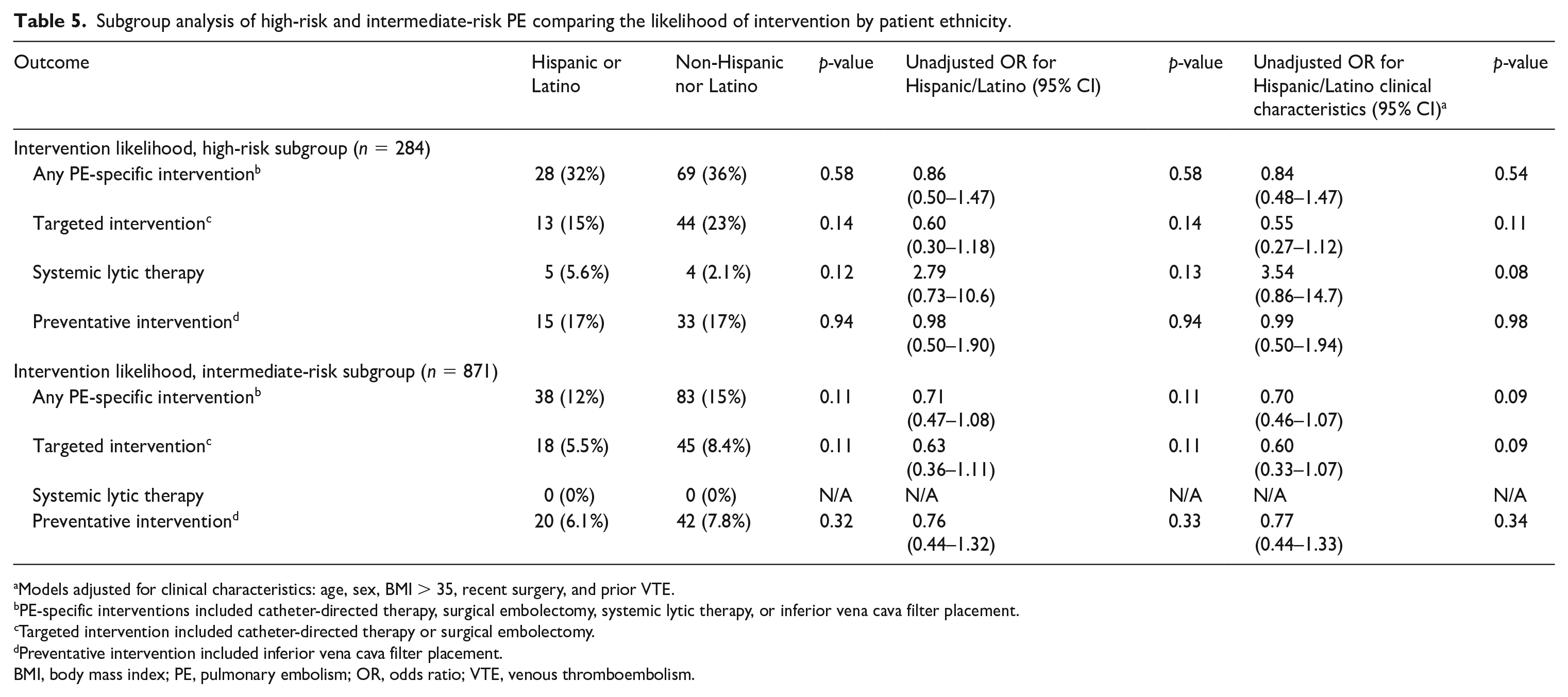
Models adjusted for clinical characteristics: age, sex, BMI > 35, recent surgery, and prior VTE.
PE-specific interventions included catheter-directed therapy, surgical embolectomy, systemic lytic therapy, or inferior vena cava filter placement.
Targeted intervention included catheter-directed therapy or surgical embolectomy.
Preventative intervention included inferior vena cava filter placement.
BMI, body mass index; PE, pulmonary embolism; OR, odds ratio; VTE, venous thromboembolism.
Univariate and multivariate analyses comparing PE severity and treatment modality between Black and White patients in the study population were also performed (Tables S3 and S4). When compared to White patients, Black patients were significantly less likely to present with a higher-risk PE (OR 0.67, 95% CI 0.50–0.88, p = 0.005), even after correcting for baseline clinical characteristics (OR 0.73, 95% CI 0.55–0.98, p = 0.03). Race was not included in multivariate models evaluating the impact of ethnicity on PE severity because the majority of Hispanic or Latino patients did not identify as White or Black and 32% did not report their race at all.
In-hospital and 30-day outcomes
While hospitalized, Hispanic or Latino patients faced similar rates of all-cause inpatient mortality (6.8% vs 7.5%, p = 0.64), PE-related inpatient mortality (2.5% vs 4.2%, p = 0.12), and GUSTO moderate or severe bleeding (8.2% vs 12%, p = 0.06) to non-Hispanic or Latino patients (Table 3). Within the 30-day interval after hospitalization, all-cause mortality, PE-related mortality, and readmission rates did not differ significantly between Hispanic or Latino and non-Hispanic or Latino patients (Table 3; all p > 0.1). Notably, PE-related mortality accounted for < 40% of all-cause mortality for Hispanic or Latino patients both in-hospital and at 30 days. No significant differences in in-hospital or 30-day outcomes were identified between ethnicities on regression analysis, even after correcting for differences in clinical characteristics (Table 4). Univariate and multivariate analyses comparing in-hospital and 30-day outcomes between Black and White patients in the study population can be found in the online supplementary material (Tables S3 and S4).
Discussion
There is a growing body of evidence which demonstrates that disparities in access to care and quality of care received for PE exist in the US.5–9 Much of the existing body of literature has focused on Black and White patients and has been underpowered to evaluate healthcare disparities based on ethnicity.7,10–13 Results of this study demonstrate that Hispanic or Latino patients are less likely to present with high-risk PE. However, after adjusting for differences in PE severity, they are equally likely to receive PE-specific intervention and suffer in-hospital and 30-day mortality as non-Hispanic or non-Latino patients.
To the authors’ knowledge, this is the first study of its kind to investigate disparities in PE care using a representative sample of Hispanic or Latino patients. Although Hispanic patients are expected to make up a third of the US population by 2060, 27 representation in national cohort studies is often disproportionately low due to underrepresentation in national databases.28,29 This has been hypothesized to stem from under-reporting, lack of access to medical care, and lack of patient outreach.28,29 Consequently, study on an institutional or hospital-system level becomes critical, noting that Hispanic or Latino patients are distributed in much greater frequency in metropolitan areas of New York and New Jersey along with the Southwestern and Southeastern US. 30 A strength of this study was the location of the primary institution and the patient population it serves, which allowed for a study population that included 37% Hispanic or Latino-identifying patients. The decision to consider ethnicity separate from race was made intentionally given that Hispanic or Latino patients may identify as any race. This plurality is well demonstrated in our study population, as 23% of Hispanic or Latinos identified as White and 14% identified as Black. Notably, the majority of Hispanic or Latino patients selected to either not report their race or identified as two or more or other races, consistent with US Census data. 11
Hispanic or Latino patients living in the US bear a disproportionate burden of chronic conditions like diabetes, cardiovascular disease, and stroke, which was demonstrated in our study population. In the US, Hispanic men and women face the highest estimated lifetime risk of diabetes of all racial and ethnic groups at 45.4% and 52.5%, respectively, and have almost twice the prevalence of diabetes when compared to age-matched White, non-Hispanic patients.31,32 Level of blood sugar control for those with diabetes also differs, with Hispanic patients facing significantly higher rates of microvascular complications like retinopathy and nephropathy when compared to non-Hispanic patients.18,19 In the American Heart Association’s 2021 Update of Heart Disease and Stroke Statistics, Hispanic patients were shown to have an overall incidence rate ratio for ischemic stroke of 1.34 when compared to non-Hispanic White individuals and have higher incidence rates of heart failure when compared to non-Hispanic White individuals. 1 These differences are likely underestimated due to high rates of underdiagnosis; in the Echocardiographic Study of Latinos, half of middle-aged or older Hispanic individuals had some form of systolic or diastolic dysfunction on echocardiogram but less than 5% of these patients had clinically recognized heart failure. 33 Though unmodifiable factors like genetics may play a role in these differences, socioeconomic factors such as poor health insurance access, 34 less access to care, 35 and difficulty affording medical care regardless of insurance access 36 also play a large role and provide areas to target for improvement of medical care delivery to Hispanic populations in the US.
Though results of this study suggest that Hispanic patients are less likely to present with high-risk PE, the cause of this finding is likely multifactorial. Existing research suggests that this is not because Hispanic patients with high-risk PE are not making it to the hospital. In a study performed by Tang et al. examining 578 consecutive out-of-hospital fatal PE cases in New York City, the adjusted incidence of out-of-hospital PE among Hispanic patients was the lowest of all groups at 0.93 per 100,000 people per year. 37 The difference may in part lie in disparities in the care that is received while in the hospital. The differentiating factor that drives cases into the high-risk category of PE is hemodynamic instability. In the 2019 ESC Guidelines, this is defined by both objective measures (sustained systolic blood pressure (SBP) < 90 mmHg, end-organ damage, cardiac arrest) and subjective measures such as need for vasopressor initiation. In our study population, presenting SBP and mean arterial pressure (MAP) ranges did not differ between cohorts, yet rates of vasopressor initiation were 6% lower in Hispanic or Latino patients when compared to non-Hispanic or Latino patients. Though it is possible that this was driven by clinical judgment from differences in TTE findings (e.g., RV volume overload) and perceived fluid tolerance, it is also possible that vasopressors were initiated at higher SBPs or after shorter lengths of hypotension or fluid trials for non-Hispanic or Latino patients. Further research should investigate whether length of hypotension tolerated prior to vasopressor initiation and SBP at which vasopressors are initiated differs by patient race or ethnicity. Lower rates of biomarker elevation and RV dysfunction on TTE suggest that there may also be a physiologic difference (e.g., hereditary predisposition, less aggressive disease processes) that this study was not able to analyze, which are driving differences in PE severity. Measurements of RV size and function were determined qualitatively, however, and future research should evaluate more granular and quantifiable signs of RV dysfunction such as tricuspid annular plane systolic excursion (TAPSE) and RV fractional area change (FAC).38,39
On the surface, results of this study suggest that Hispanic patients have a lower likelihood of PE-specific intervention. This follows a study in Pennsylvania by Phillips et al. which found that Black patients were less likely to receive PE-specific intervention than White patients. 5 In this study, however, the difference in likelihood of intervention did not retain significance after adjusting for differences in PE severity. As discussed above, potential disparities in treatment can lead to misclassification of PE severity, and as such subtle differences in likelihood of intervention may exist despite absence of statistical significance in this cohort. It is important to note that the frequency of intervention in this study cohort was also substantially higher than what has been seen in previous literature. 5 The primary institution for this study serves as a quaternary care center with a dedicated pulmonary embolism response team that often receives hospital transfers for intervention. This can likely explain these differences in frequency and may mask race- and ethnicity-based differences in the administration of PE-specific intervention. This has the potential the produce perceived differences in PE severity as well if the majority of the cohort of patients being transferred with high-risk PE is non-Hispanic or Latino.
Despite lower classifications of PE severity, this study failed to demonstrate a difference in in-hospital or 30-day all-cause or PE-related mortality for Hispanic or Latino patients presenting with PE. When comparing rates of all-cause mortality and PE-related mortality within ethnicities, it is evident that the majority of inpatient and 30-day mortality for Hispanic or Latino patients is not PE-related. On chart review, non-PE-related mortalities which led to the high rates of all-cause mortality for Hispanic or Latino patients were driven by decompensation of chronic conditions. This is a reflection not only of the disproportionate burden of chronic conditions Hispanic or Latino patients bear, but also of the difference in disease control. Factors such as institutional and systemic racism may also play a role in contributing to higher-than-expected rates of in-hospital and 30-day mortality.
Study limitations
An important limitation of this study was the lack of adjustment for race in multivariate models evaluating the association between ethnicity and PE severity. Whereas this analysis found that White and Black patients have different likelihoods of high-risk PE, the majority of Hispanic or Latino patients did not identify as White or Black. In this study, 31% of Hispanic or Latino patients identified as two or more or other races and 32% decided not to identify their race at all. This is representative of a national trend; in the US, < 25% of Hispanic or Latino individuals identify as White or Black. 11 Given the majority of Hispanic or Latino patients identify as two or more or other races, and 32% chose not to provide data on their race, race was not adjusted for in the multivariate models.
This study had several additional limitations that must be acknowledged. The population for this study comes from a single academic medical center, which may limit the generalizability of the study results. Future research should focus on replicating this study utilizing national databases, paying particular attention to using databases with more representative populations of Hispanic or Latino patients. The retrospective nature of this study led to limitations in terms of assigning PE severity. The study population comes from 2013 through June 2019, which was prior to the release of the 2019 ESC Guidelines which re-classified PE severity. Patients were retrospectively assigned a PE severity according to the 2019 ESC Guidelines using retrospective review of blood pressure data, medication administration, imaging findings, and labs, which has the potential to lead to inaccurate classification. This method also is unable to evaluate for differences in measurement bias and provider decision-making behind vasopressor initiation, which may lead to differences in PE severity. This study was also unable to adjust for genetic differences in clotting predisposition (e.g., prothrombin 20210, Factor V Leiden) and hemostatic factors that could be leading to differences in PE severity. Finally, this study was also unable to adjust for differences that may contribute to the likelihood of PE-specific intervention, including patient preference, presence of bleeding disorders, and chronicity.
Conclusions
This is the first study to utilize a population with a representative cohort of Hispanic or Latino patients to evaluate disparities in PE presentation, management, and outcomes. Results of this study suggest that Hispanic or Latino patients are less likely to present with high-risk PE but equally likely to receive PE-specific intervention and experience in-hospital and 30-day mortality when compared with non-Hispanic or Latino patients. Future research is needed to determine if disparities in in-hospital care are driving a perceived difference of lower PE severity and what addressable systematic factors are driving higher-than-expected in-hospital mortality for Hispanic or Latino patients.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231157441 – Supplemental material for Association between Hispanic or Latino ethnicity and pulmonary embolism severity, management, and in-hospital outcomes
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231157441 for Association between Hispanic or Latino ethnicity and pulmonary embolism severity, management, and in-hospital outcomes by Daniel J Snyder, Robert S Zilinyi, Mahesh V Madhavan, Marissa Alsaloum, Danial Saleem, John J Buyske, Emma W Healy, Maxine J McGredy, Bernardo T Da Silva, Erika B Rosenzweig, Koji Takeda, Daniel Brodie, Cara Agerstrand, Andrew Eisenberger, Ajay J Kirtane, Sahil A Parikh and Sanjum S Sethi in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Daniel Brodie receives research support from and consults for LivaNova. He has been on the medical advisory boards for Abiomed, Xenios, Medtronic, Inspira, and Cellenkos. Ajay Kirtane reports institutional funding to Columbia University and/or the Cardiovascular Research Foundation from Medtronic, Boston Scientific, Abbott Vascular, Amgen, CSI, Philips, ReCor Medical, Neurotronic, Biotronik, Chiesi, Bolt Medical, Magenta Medical, Canon, SoniVie, and Merck. In addition to research grants, institutional funding includes fees paid to Columbia University and/or the Cardiovascular Research Foundation for consulting and/or speaking engagements in which Dr Kirtane controlled the content. He has also received consulting fees from IMDS and travel expenses/meals from Medtronic, Boston Scientific, Abbott Vascular, CSI, Siemens, Philips, ReCor Medical, Chiesi, OpSens, Zoll, and Regeneron. Sahil Parikh receives institutional grants/research support from Abbott Vascular, Shockwave Medical, TriReme Medical, SurModics, Silk Road Medical, and the National Institutes of Health. He has received consulting fees from Terumo and Abiomed and served on the advisory boards of Abbott, Medtronic, Boston Scientific, CSI, Janssen, and Philips. Sanjum Sethi reports honoraria from Janssen and Chiesi. All other authors have no conflicts of interest to report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.