
Abstract
Although an association between serum ferritin and atherosclerosis has been suggested, limited epidemiologic data are available regarding the association between ferritin and arterial stiffness in healthy adults. A total of 2932 healthy subjects were enrolled in this study. Anthropometric and biochemical profiles including ferritin were measured. The arterial stiffness was measured using brachial–ankle pulse wave velocity (baPWV). Serum ferritin levels were classified into quartiles and baPWV values gradually increased with each ferritin quartile. Multiple regression analysis showed that ferritin levels were independently correlated with baPWV. After adjusting for multiple risk factors, as compared with the lowest quartile, the odds ratios for high baPWV (>75th percentile) were 1.15 (0.84–1.56), 1.37 (0.97–1.73), and 1.46 (1.29–2.17) among men (p for trend < 0.05) and 1.24 (0.87–1.79), 1.53 (1.09–2.16), and 1.80 (1.25–2.82) among women (p for trend < 0.05), for the second, third, and fourth quartiles of ferritin, respectively. In conclusion, serum ferritin levels are independently associated with arterial stiffness in healthy Korean adults.
Introduction
Ferritin is a ubiquitous intracellular protein that regulates iron homeostasis, and the serum ferritin level reflects the amount of iron stored. Recently, several studies have reported that an increased serum ferritin concentration is associated with various metabolic risk factors, including diabetes,1,2 hypertension, 3 dyslipidemia,4,5 and metabolic syndrome.6–8 In addition, growing evidence has suggested that ferritin is associated with cardiovascular diseases.9–11
Brachial–ankle pulse wave velocity (baPWV) is a non-invasive method widely used to assess arterial stiffness, which is strongly associated with cardiovascular diseases,12–14 and recent studies have found it to be an independent predictor of not only cardiovascular events, but also cardiovascular mortality. 15
Few studies have examined the relationship between serum ferritin level and arterial stiffness, and results have been inconsistent.16,17 Therefore, we investigated the relationship between serum ferritin level and arterial stiffness in healthy Korean adults.
Methods
Study population
This study population consisted of 5217 Korean subjects who participated in a comprehensive health examination, including measurements of baPWV, as part of a self-referred health checkup program at the Gangnam Severance Hospital Health Promotion Center from January 2008 to February 2013. We excluded subjects who had any malignancy, acute inflammatory disease, infectious disease, or increased WBC counts (⩾10,000 cells/mm3). We also excluded subjects with a history of angina, myocardial infarction or cerebrovascular accidents, hypertension, diabetes, renal disease, excessive alcohol consumption (⩾20 g/day), or hepatic disease. Subjects with anemia (Hb <13 g/dL for men, <12 g/dL for women) or those with iron deficiency (ferritin <10 μg/L) were also excluded. After these exclusions, 2932 subjects were ultimately enrolled in our final analysis. The study protocol was approved by the Institutional Review Board of Yonsei University College of Medicine.
Clinical characteristics
Height and weight were measured, and body mass index (BMI) was calculated by dividing the weight (kg) by the square of the height (m2). Lifestyle, personal medical history of acute and chronic illnesses, and medication history were assessed with a standard questionnaire. Systolic and diastolic blood pressures (SBP, DBP) were measured by an experienced technician by placing the arm at heart level after a 5-minute rest period. Current smokers were defined as those who reported having smoked cigarettes regularly over the previous 6 months.
Biochemical parameters
Blood samples were taken from all subjects after 8 hours of fasting. Samples were immediately centrifuged, and serum samples were stored at −70°C until analysis. Fasting plasma glucose (FPG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), and C-reactive protein (CRP) levels were determined using enzymatic methods with a Hitachi 7600-120 automated chemistry analyzer (Hitachi, Tokyo, Japan). Low-density lipoprotein cholesterol (LDL-C) was calculated according to the Friedewald formula. Fasting serum insulin was determined by means of chemiluminescence (RIA kit; Daiichi, Japan), and insulin resistance was estimated using the homeostasis model assessment of insulin resistance (HOMA-IR) index calculated from the following formula: HOMA-IR = fasting insulin (μU/mL) × fasting plasma glucose (mmol/L) / 22.5. Serum ferritin was measured using a chemiluminescence immunoassay (DxI; Beckman Coulter, Brea, CA, USA).
Pulse wave velocity
Arterial stiffness was measured using an automatic plethysmographic instrument (VP-1000; Colin, Komaki, Japan) as previously described. 18 Electrodes were placed on both wrists, and cuffs were wrapped around both the upper arms and the ankles. After simultaneous measurement of blood pressure and waveforms in all four limbs, the time interval between the brachial and ankle waveforms (ΔTba) was determined. The distance between the brachium and the ankle (La – Lb) was estimated automatically according to the subject’s height. After these data were collected, baPWV was calculated using the following equation: baPWV = (La − Lb) / ΔTba (in cm/s). Both baPWV values were measured after allowing the patient to rest in the supine position for at least 5 minutes. We used the mean of the right and left baPWV as a marker of arterial stiffness.
Statistical analysis
Continuous variables with normal distributions are expressed as means ± SD, whereas continuous variables with skewed distributions are presented as median (interquartile range) and were log transformed for analysis. The intergroup comparisons were performed using ANOVA tests. Chi-squared tests were used to compare categorical variables with percentages. The relationships between ferritin and various clinical parameters were examined using Pearson’s correlation. Multiple linear regression analysis was used to assess the independent factors affecting the ferritin. The odds ratios (OR) and corresponding 95% confidence intervals (CI) for high PWVs were estimated using a multivariate logistic regression analysis after adjusting for confounding variables across ferritin quartiles. Because an absolute cut-off value of normal baPWV was not available, high baPWV was arbitrarily defined as a value greater than the cut-off level between the third and fourth quartiles (>75th percentile), which was 1431.5 cm/s for men and 1412.0 cm/s for women. Statistical analysis was carried out using IBM SPSS for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA). P-values less than 0.05 were considered statistically significant.
Results
This study included 1649 men and 1283 women. Subjects were stratified into four groups according to their ferritin levels. There were significant differences in metabolic parameters among the groups. Age, SBP, DBP, BMI, FPG, TG, insulin, HOMA-IR, and CRP levels increased with ferritin quartiles in ascending order in both men and women. TC and LDL-C levels increased progressively across the ferritin quartiles in women while the HDL-C level decreased in both sexes (Tables 1 and 2).
Clinical characteristics of male subjects divided into ferritin quartiles.
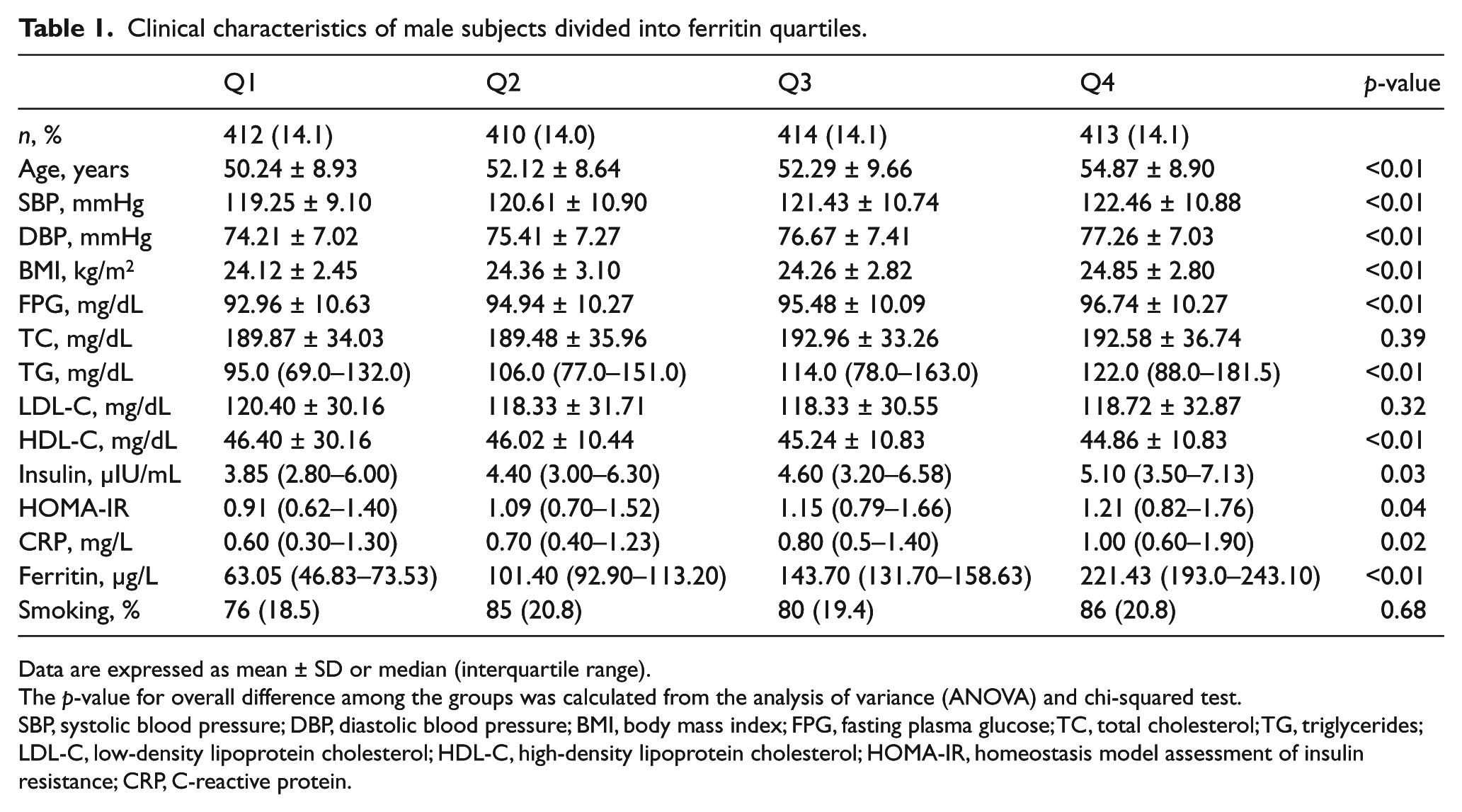
Data are expressed as mean ± SD or median (interquartile range).
The p-value for overall difference among the groups was calculated from the analysis of variance (ANOVA) and chi-squared test.
SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; FPG, fasting plasma glucose; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment of insulin resistance; CRP, C-reactive protein.
Clinical characteristics of female subjects divided into ferritin quartiles.
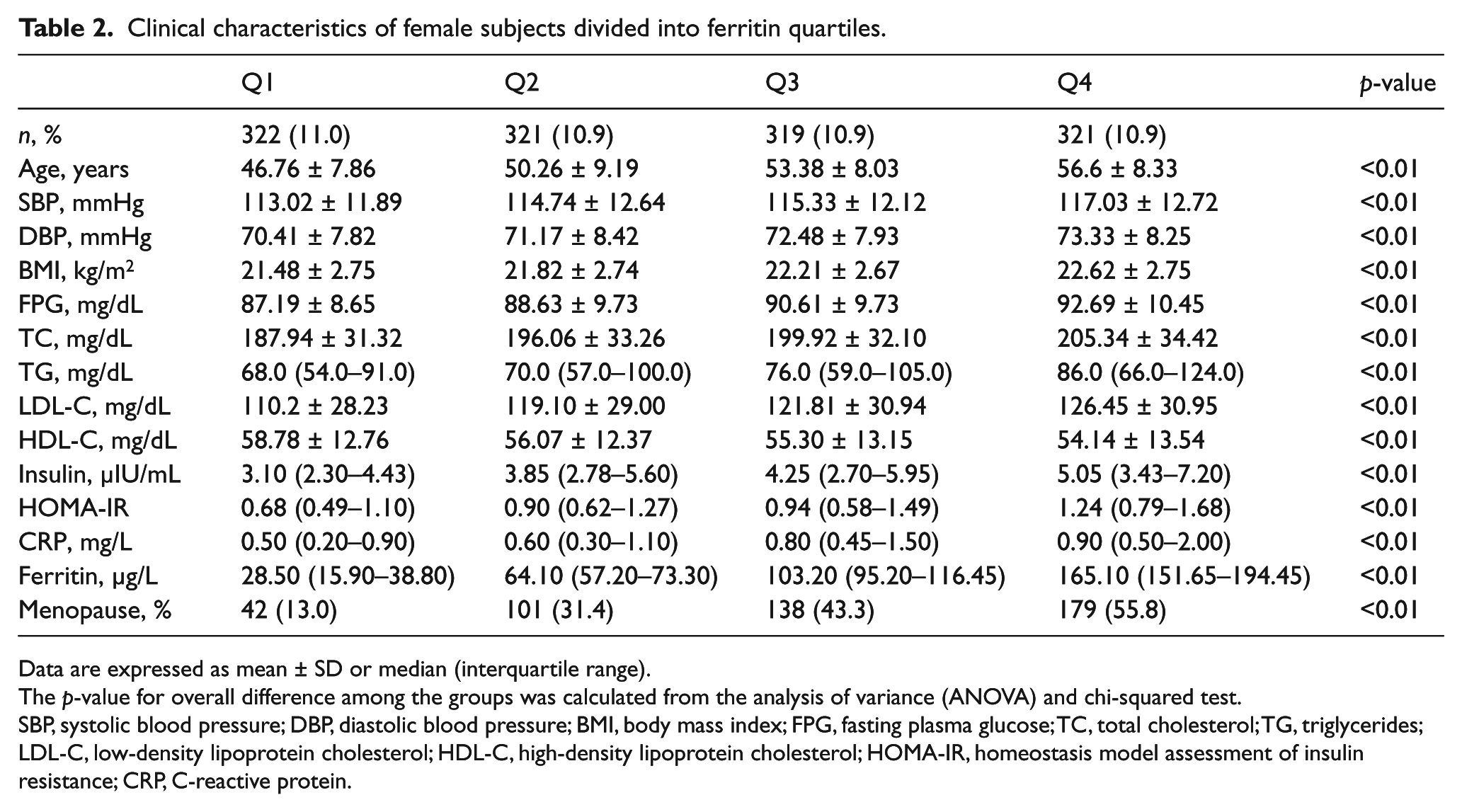
Data are expressed as mean ± SD or median (interquartile range).
The p-value for overall difference among the groups was calculated from the analysis of variance (ANOVA) and chi-squared test.
SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; FPG, fasting plasma glucose; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment of insulin resistance; CRP, C-reactive protein.
The baPWV gradually increased with each ferritin quartile (Figure 1): Q1 = 1319.7, Q2 = 1345.7, Q3 = 1358.4 and Q4 = 1381.4 cm/s in men (p < 0.01) and Q1 = 1250.7, Q2 = 1291.3, Q3 = 1328.5 and Q4 = 1380.4 cm/s in women (p < 0.01).
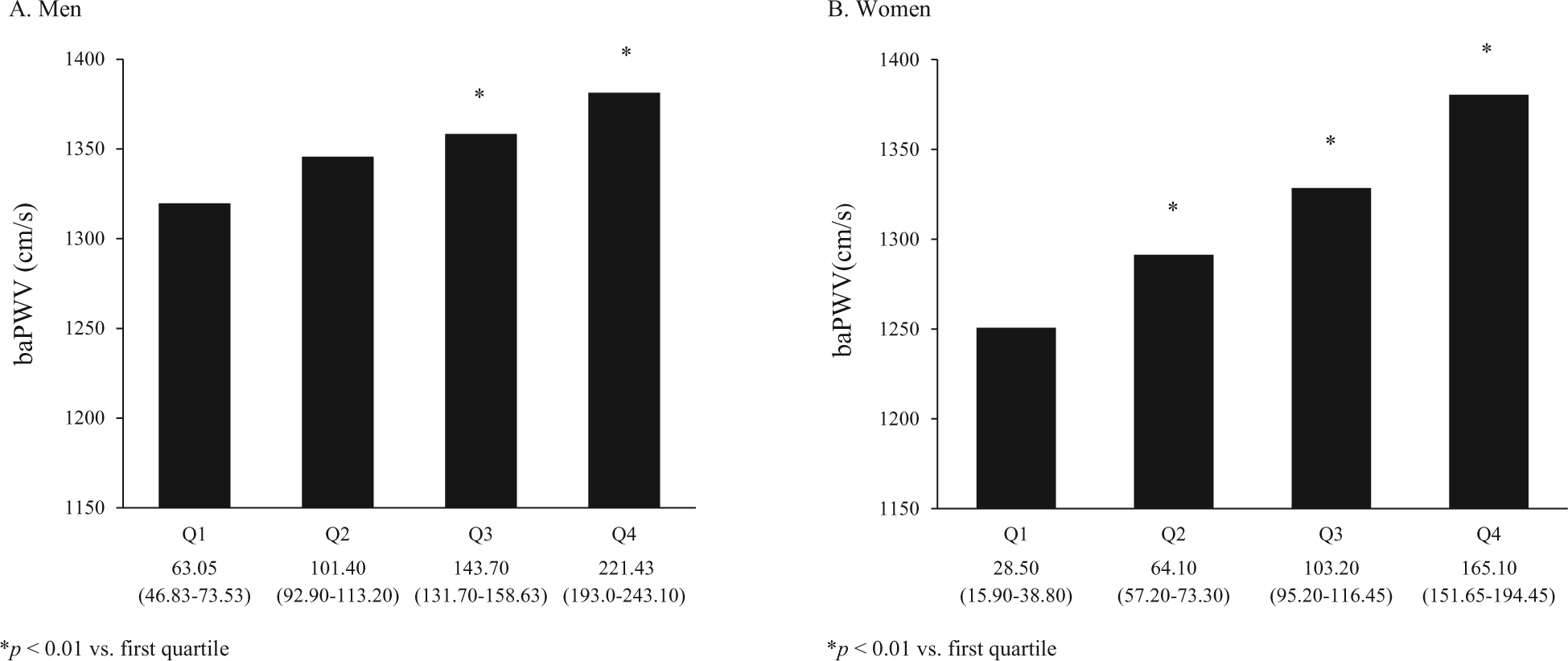
Relationship between baPWV and ferritin quartile in men (A) and women (B).
Age, SBP, BMI, FPG, TG, insulin, HOMA-IR, CRP, and baPWV were positively correlated with ferritin in both sexes, and DBP, TC, and LDL-C were positively correlated with ferritin in women, while HDL-C was inversely associated with ferritin in women (Table 3). In multiple regression analysis, using ferritin as the dependent variable, age, FPG, TG, insulin, HOMA-IR, and baPWV were independently correlated with ferritin (R2=0.221, β=0.13, 0.10, 0.12, 0.09, 0.10, and 0.07, all p < 0.01) in men; age, BMI, FPG, TG, LDL-C, insulin, HOMA-IR, and baPWV (R2=0.243, β=0.21, 0.13, 0.15, 0.18, 0.09, 0.17, 0.18, and 0.13 all p < 0.01) were significantly associated with ferritin in women.
Correlations between ferritin and other metabolic variables.
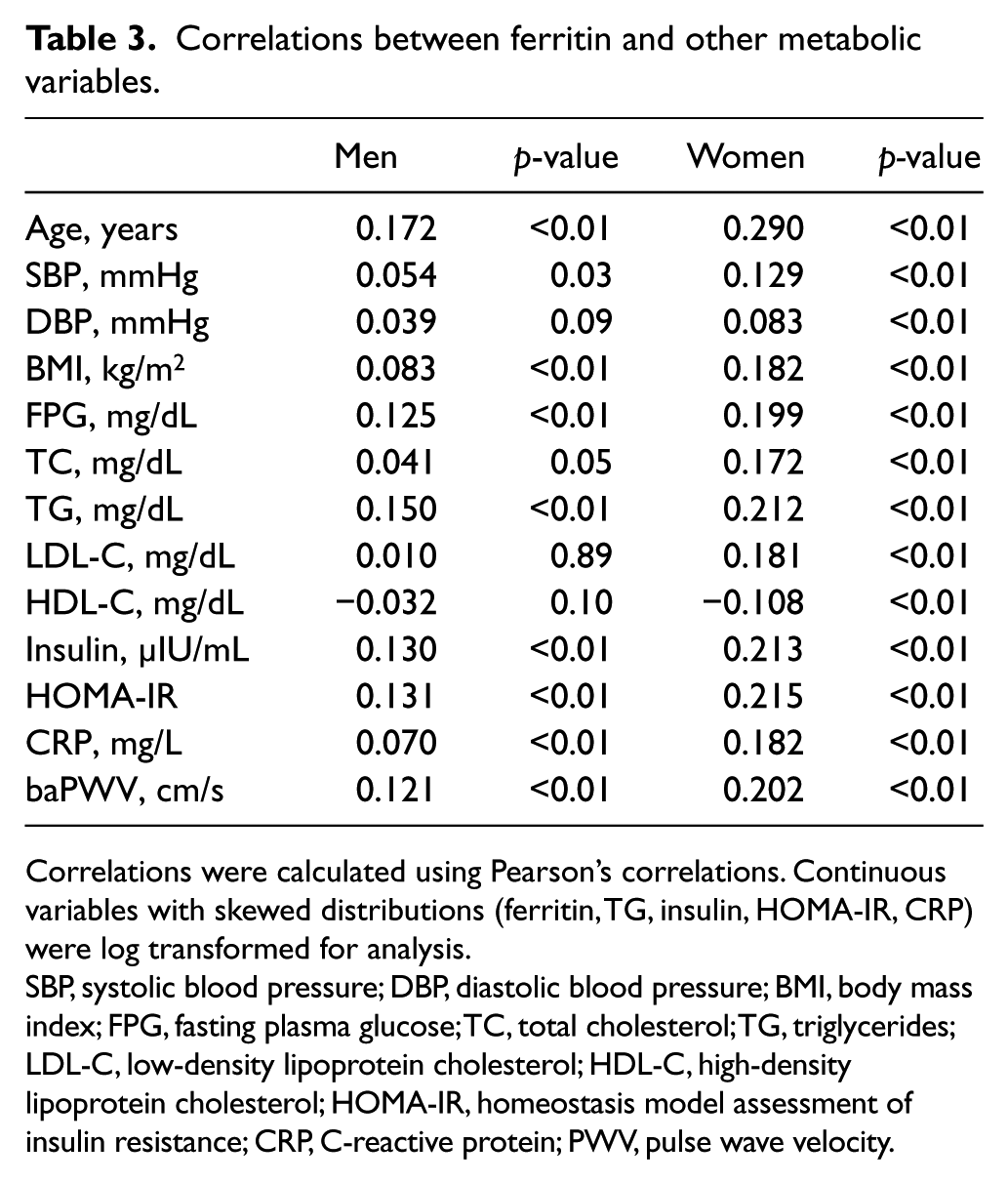
Correlations were calculated using Pearson’s correlations. Continuous variables with skewed distributions (ferritin, TG, insulin, HOMA-IR, CRP) were log transformed for analysis.
SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; FPG, fasting plasma glucose; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment of insulin resistance; CRP, C-reactive protein; PWV, pulse wave velocity.
Table 4 demonstrated the ORs and 95% CIs for high baPWV according to ferritin quartile. The association between ferritin and high baPWV was further explored by categorizing ferritin levels into quartiles and using the first quartile as the reference. From an unadjusted multivariable logistic regression analysis, with Q1 set as a reference, ferritin levels for Q2, Q3, and Q4 were found to have increased ORs for high baPWV in all subjects. After adjusting for confounding variables, this relationship remained statistically significant.
Odds ratios and 95% confidence intervals for high baPWV according to ferritin quartile.
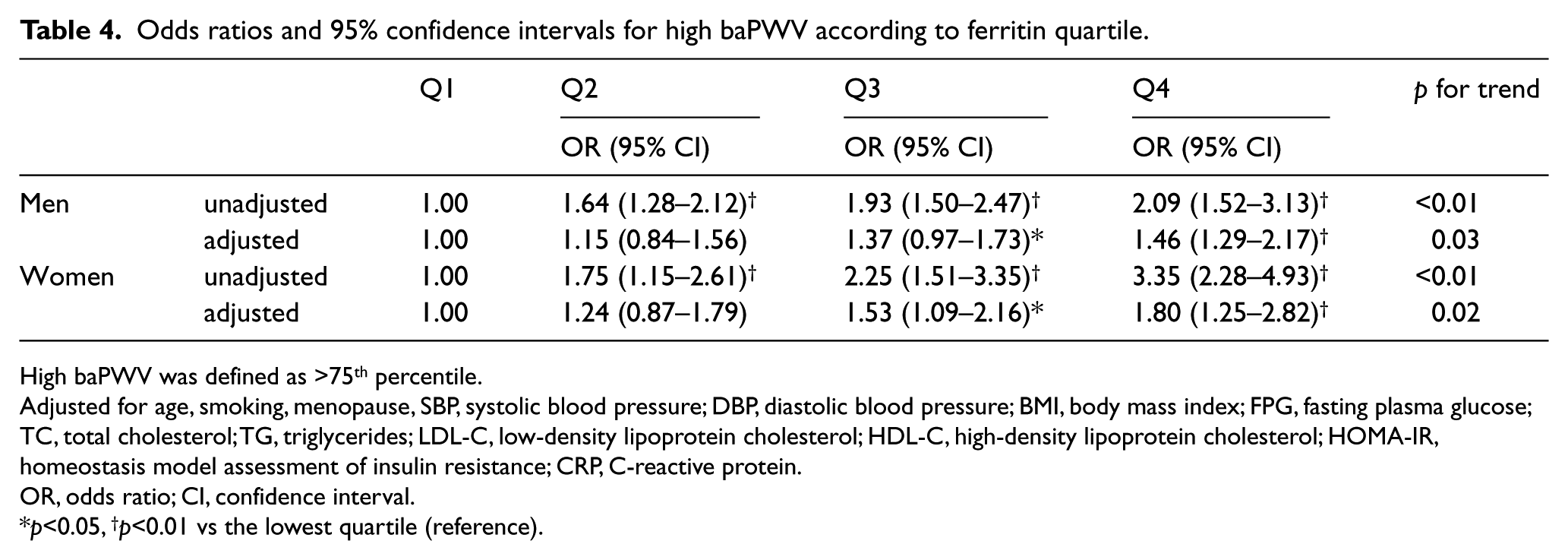
High baPWV was defined as >75th percentile.
Adjusted for age, smoking, menopause, SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; FPG, fasting plasma glucose; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment of insulin resistance; CRP, C-reactive protein.
OR, odds ratio; CI, confidence interval.
p<0.05, †p<0.01 vs the lowest quartile (reference).
Discussion
In this study, we investigated the relationship between serum ferritin level and arterial stiffness, a marker of preclinical atherosclerosis, in healthy Korean adults. Even after adjusting for cardiovascular risk factors, an independent positive association was identified between serum ferritin and increased baPWV. To the best of our knowledge, this is the largest cross-sectional study to demonstrate the positive association between serum ferritin and arterial stiffness in healthy adults.
Our results showed that most of the metabolic parameters increased or decreased as expected according to the ferritin quartiles. Moreover, significant correlations were observed between serum ferritin and metabolic parameters. These findings are similar to those of other studies.1–8 Although the exact pathophysiological mechanism has not been clarified, recent studies suggest iron overload may contribute to adipocyte insulin resistance in the pathogenesis of metabolic syndrome and type 2 diabetes.19–22
Recently, several studies have investigated the relationship between serum ferritin and subclinical atherosclerosis; however, the results have been inconsistent. A study by Sung et al. reported that serum ferritin was associated with coronary artery calcification in men. 23 Other studies found an association between serum ferritin and carotid atherosclerosis.24,25 In contrast, Yunker et al. found no association between serum ferritin and carotid atherosclerosis. 26 To date, only three studies have examined the associations between serum ferritin level and arterial stiffness, which is another marker for subclinical atherosclerosis. A study conducted by Lee et al. indicated that ferritin was independently associated with arterial stiffness in healthy subjects even after adjusting for age, sex, and blood pressure, but this association was positive only in women and was in fact negative in men. 16 However, the number of study subjects was small (n = 196), and the observed gender difference could not be explained. Recently, Valenti et al. investigated the association between serum ferritin and PWV in subjects with essential hypertension and found that the serum ferritin level was independently associated with increased aortic stiffness. 17 In addition, findings in Lin et al. were supported by a study among 53 hemodialysis patients with 3 years of follow-up. 27
We defined high baPWV as >1431.5 cm/s in men and >1412.0 cm/s in women. These cut-off values may be surrogates for increased arterial stiffness because baPWV >1400 cm/s has been found to predict cardiovascular diseases, 15 and we found that serum ferritin was an independent determinant of increased arterial stiffness in both men and women, a result that is consistent with the hypothesis that iron stores are associated with atherosclerosis.9–11 Although the exact mechanism has not been fully elucidated, several explanations exist regarding the relationship between serum ferritin and arterial stiffness,28,29 and oxidative stress is one possible mechanism for this association.
Ferritin is an acute-phase protein that reflects stored iron, which has significant oxidative capacity and can cause tissue damage by oxidative stress,30,31 and several studies reported that increased serum ferritin was associated with markers of oxidative stress.32,33 Several mechanisms have been proposed to explain the pro-atherogenic role of iron via oxidative stress catalysis, including decreased plasma antioxidant activity, increased LDL oxidation, and enhanced macrophage activation determining oxidized LDL uptake.34–36 In addition, arterial stiffness measured by PWV has been reported to be significantly associated with oxidative stress. 37 Therefore, although the mechanism underlying the relationship of ferritin with arterial stiffness is not completely understood, oxidative stress might provide a link between ferritin and arterial stiffness.
Limitations
Several limitations of our study need to be considered. First, the cross-sectional design could not confirm causality, and more prospective studies are necessary to confirm the relationships we observed. Second, participants in the current study were enrolled in the same health promotion center; therefore, generalizability may be limited. Third, serum ferritin is an acute phase protein and may be elevated under conditions of inflammation or infection. Thus, we excluded individuals with a WBC count of ⩾10,000 cells/mm3 to minimize the possibility of including individuals with active infections and adjusted CRP to control for this confounding factor. Fourth, we measured only hemoglobin and ferritin as a marker of body iron status; other iron-related markers were not measured. Finally, as a cut-off value for baPWV has not been determined, the results can change depending on the subjects enrolled. Despite these limitations, the present study was meaningful in demonstrating the association between serum ferritin and arterial stiffness in healthy adults.
Conclusion
In conclusion, we demonstrated that the serum ferritin level is significantly associated with arterial stiffness in healthy adults. Further community-based, prospective, large-scale research is required to investigate whether serum ferritin is associated with an increased risk of cardiovascular events.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.