
Abstract

Keywords
Transcutaneous oxygen pressure (TcPO2) is measured to diagnose critical limb-threatening ischemia (CLTI)1–3 in patients with peripheral artery disease (PAD) but highly depends on the applied method.4,5 The Undersea and Hyperbaric Medical Society is the only professional society that endorsed guidelines focusing on the prognosis of healing using TcPO2 values for hyperbaric oxygen therapy. 6 Real-world practices are unknown. The aim of this study was to describe real-world practices in the field and general knowledge on TcPO2 measurement.
An anonymous survey (online Supplemental Table 1) was made available online in December 2020 to all members of the Société Française de Médecine Vasculaire (SFMV) (French Society of Vascular Medicine) (n = 2143) and the Société de Chirurgie Vasculaire et Endovasculaire de Langue Française (SCVE) (French Speaking Society of Vascular and Endovascular Surgery) (n = 350), through a Google form. Quantitative variables were presented as the number of cases. The mean differences in mean values between groups were assessed using the analysis of variance (t-test). Categorical variables were compared using the Fisher test. Data were processed and analyzed using R package version 3.4.3 (R Foundation for Statistical Computing, Vienna, Austria). This survey on medical practices was exempt from ethical approval.
The survey was completed by 197 members of the SFMV and by 119 vascular surgeons of the SCVE. The baseline characteristics of respondents are reported in Table 1. The most frequent indication for TcPO2 measurement was the determination of amputation level (n = 264, 83.5%) followed by evaluation of PAD severity (195, 61.7%). On a 0–10 scale (0 = no confidence and 10 = absolute confidence), the mean confidence score in TcPO2 measurements was 6.9 (range: 0–10) (online Supplemental Table 2).
Baseline characteristics of respondents.
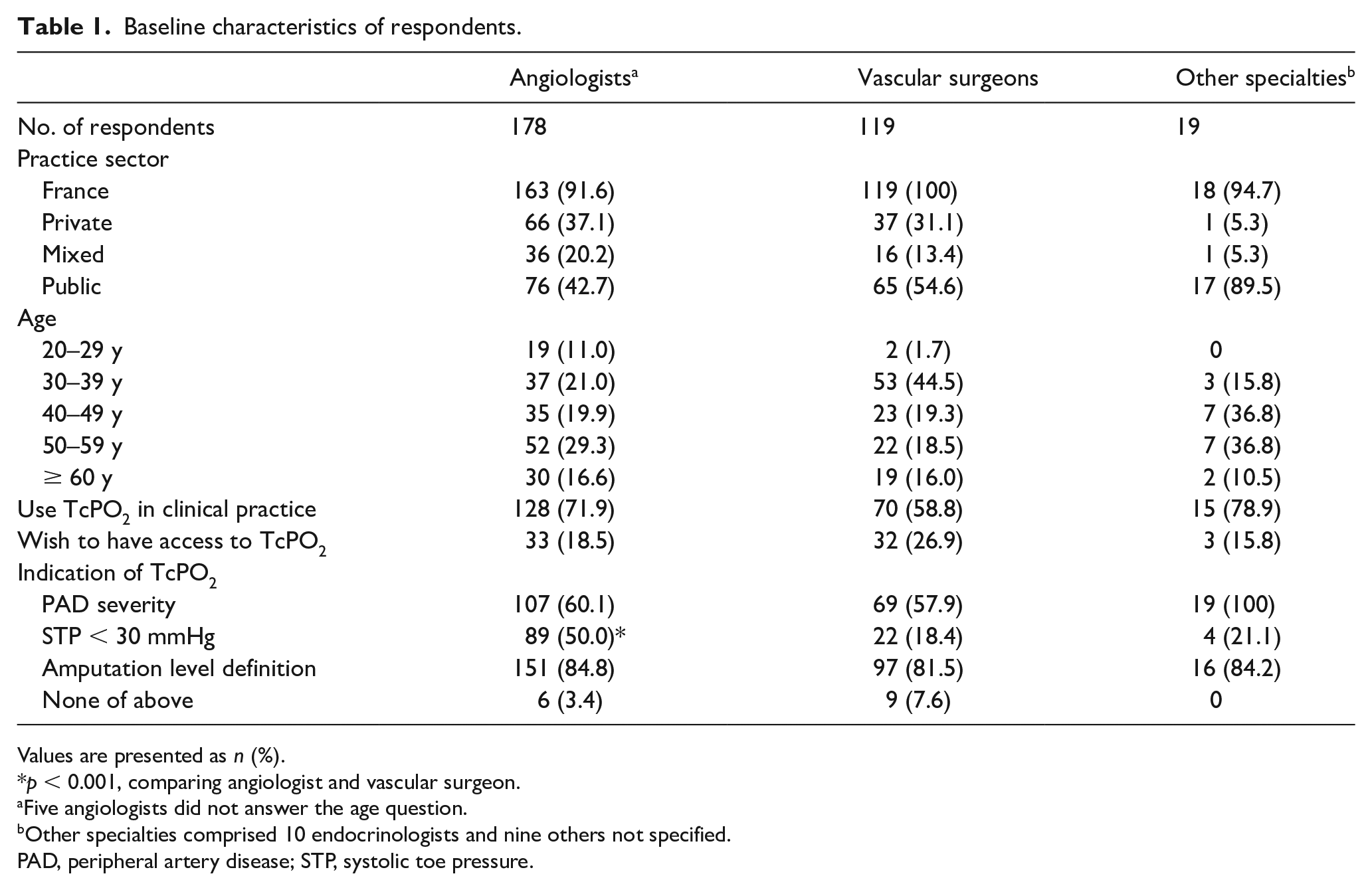
Values are presented as n (%).
p < 0.001, comparing angiologist and vascular surgeon.
Five angiologists did not answer the age question.
Other specialties comprised 10 endocrinologists and nine others not specified.
PAD, peripheral artery disease; STP, systolic toe pressure.
TcPO2 measurement was well correlated with wound healing (277, 87.7%) and amputation healing (267, 84.5%). To a lesser degree, some participants also agreed with correlation with systolic toe pressure (187, 59.2%), PAD severity according to Fontaine classification (117, 37.0%), Doppler waveforms (77, 24.4%), and ankle pressure (74, 23.4%).
Survey respondents reported that confounding factors in TcPO2 measurement are mainly edema (292, 92.4%) and local infection (216, 84.2%). Other factors include comorbidities (anemia, heart failure, respiratory failure, sleep apnea) (189, 58.9%), skin thickness (189, 58.9%), smoking, caffeine consumption (within 2 hours before measurement) (152, 48.1%), PAD severity (77, 24.4%), and age (36, 11.3%).
Concerning controllable confounding factors, respondents agreed with the importance of room temperature (244, 77.2%), patient resting > 15 minutes before measurement (208, 65.8%), stable TcPO2 value ⩾ 20 minutes (180, 56.9%), hanging legs on a footboard (102, 32.3%), covered limbs (92, 29.1%), fasting examination (66, 20.9%), closing the door (61, 19.3%), and staying quiet (41, 13.0%).
Placement of the TcPO2 electrode was investigated. Absence of edema was the most common requirement for placement of electrodes. Medial face of the leg (15.9% and 17.0%), posterior face of the leg (8.3% and 13.0%), and above artery (10.4% and 7.2%) were the least chosen positions for electrode placement, for all indications and before amputation, respectively (online Supplemental Table 3).
Regarding measurement time, the majority of respondents reported a time of 20 minutes and until stabilization (149, 53.0%). Other responders proposed a measurement time until stabilization (89, 31.7%), 20 minutes (28, 10.0%), 10 minutes (11, 3.9%), or 5 minutes (4, 1.4%). If a patient has hanging legs, the majority of responders proposed a measurement time until stabilization (188, 68.2%). Other respondents proposed a measurement time of 20 minutes (33, 12.0%), 10 minutes (34, 12.3%), or 5 minutes (21, 7.6%). Among regular users of TcPO2, minority practices of other measurement times were reported, including rising leg (15, 7.3%), 100% oxygen inhalation (29, 14.3%), thorax reference (36, 17.7%), and occlusion test (8, 3.9%).
After revascularization, respondents selected a delay of 1 day (56, 19.7%), 3 days (74, 26.1%), 7 days (56, 19.7%), 15 days (40, 14.1%), and 30 days (58, 20.4%) to obtain a reliable TcPO2 result.
Among respondents, the majority (165, 56.7%) considered TcPO2 as important as other factors to select amputation level. Ten (3.1%) respondents considered only TcPO2 to select amputation level, and 72 (22.7%) respondents considered TcPO2 as the most important factor, whereas 44 (15.1%) respondents did not consider TcPO2 (but considered other factors) to determine amputation level (online Supplemental Table 4).
Other factors were proposed by responders for determining amputation level and can be considered in four major categories: comorbidities and general status (n = 72); functional status, autonomy, and mobility (n = 91); clinical examination (n = 121); and lower limb vascularization quality (n = 131). Four responders proposed to ask for the patient’s opinion about level of amputation.
The mean value of TcPO2 proposed to expect good healing after amputation in a nondiabetic patient was higher than the mean value proposed to define CLTI (33.5 vs 25.9 mmHg, p < 0.001) (online Supplemental Tables 5 and 6).
Gathering 316 vascular practitioners in France, this study highlights large variation in real-world practices and interpretations that could alter the quality of TcPO2 measurements, despite having an overall good level of confidence among respondents.
Generalizability of our results may be limited given that these data reflect practices only in France. The variability of real-world practices may be explained by the lack of consensus in France. The only clinical practice guidelines regarding TcPO2 measurements come from the Undersea and Hyperbaric Medical Society using a Delphi method with six experts in the field of hyperbaric oxygen therapy. 6 However, Leenstra and colleagues recently showed that there is still a large variation of methods applied in the different studies. 4 A potential new expert consensus including vascular practitioners and which covers TcPO2 use across all indications should be more precise concerning the placement of electrodes (i.e., location, number), the necessity of using additional maneuvers with TcPO2 testing (e.g., oxygen challenges, leg dependency, occlusion test), and should provide an interpretation algorithm. Such a document would be helpful to ensure that all clinicians who use TcPO2 will apply the same protocol and follow the same standards for interpretation.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221094080 – Supplemental material for Real-world practices of TcPO2 measurements: A French national survey
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221094080 for Real-world practices of TcPO2 measurements: A French national survey by Judith Catella, Nellie Della Schiava, Luca Calanca, Eric Steinmetz, Antoine Millon, Guillaume Mahé, Anne Long and Lucia Mazzolai in Vascular Medicine
Supplemental Material
sj-pdf-2-vmj-10.1177_1358863X221094080 – Supplemental material for Real-world practices of TcPO2 measurements: A French national survey
Supplemental material, sj-pdf-2-vmj-10.1177_1358863X221094080 for Real-world practices of TcPO2 measurements: A French national survey by Judith Catella, Nellie Della Schiava, Luca Calanca, Eric Steinmetz, Antoine Millon, Guillaume Mahé, Anne Long and Lucia Mazzolai in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.