
Abstract
Background:
Thrombosis of the left internal jugular vein in an astronaut aboard the International Space Station was recently described, incidentally discovered during a research study of blood flow in neck veins in microgravity. Given this event, and the high incidence of flow abnormalities, the National Aeronautics and Space Administration (NASA) instituted an occupational surveillance program to evaluate astronauts for venous thrombosis.
Methods:
Duplex ultrasound of the bilateral internal jugular veins was conducted on all NASA astronauts terrestrially, and at three points during spaceflight. Respiratory maneuvers were performed. Images were analyzed for thrombosis and certain hemodynamic characteristics, including peak velocity and degree of echogenicity.
Results:
Eleven astronauts were evaluated with matching terrestrial and in-flight ultrasounds. No thrombosis was detected. Compared to terrestrial ultrasound measurements, in-flight peak velocity was reduced and lowest in the left. Six of 11 astronauts had mild–moderate echogenicity in the left internal jugular vein during spaceflight, but none had more than mild echogenicity in the right internal jugular vein. Two astronauts developed retrograde blood flow in the left internal jugular vein.
Conclusion:
Abnormal flow characteristics in microgravity, most prominent in the left internal jugular vein, may signal an increased risk for thrombus formation in some individuals.
See Commentary: Drudi LM, Grenon SM. The Vascular Frontier: Exploring the Diagnosis and Management of Vascular Conditions in Spaceflight. Vasc Med2022; 27: 373-374.
Introduction
Thrombosis of the left internal jugular vein (IJV) in an astronaut aboard the International Space Station was recently described, detected during a research study of microgravity-induced changes in intra- and extravascular fluid distribution in the neck vessels of 11 individuals.1,2 Five of the 11 subjects exhibited signs of flow stasis in the left IJV, based on the characteristics of Doppler spectra; the right IJVs were not examined. 1
Given the absence of a hydrostatic pressure gradient in microgravity, and the fact that stasis is one component of Virchow’s triad of venous thrombosis pathophysiology, 3 the findings of slow flow and thrombosis in the left IJV raise the possibility that the risk for deep vein thrombosis (DVT) is increased during spaceflight. Terrestrially, slow flow on venous ultrasound imaging appears to be associated with thrombosis in patients with risk factors for DVT, such as malignancy, and slow venous flow – related to limited mobility – is thought to contribute to an increased DVT risk following long duration air travel.4,5
Whether such slow flow predisposes healthy individuals, like astronauts, to thrombosis has not been well studied. However, the discovery of one asymptomatic DVT during spaceflight in a data set of 11 unilateral jugular vein evaluations is concerning. If sequelae of microgravity-related thrombosis are similar to those on Earth, outcomes of DVT and venous thromboembolism (VTE) in spaceflight could be poor, given the limited availability of medical supplies and distance from definitive care.
Therefore, the National Aeronautics and Space Administration (NASA) instituted an occupational surveillance program to screen for DVT in astronauts and better characterize the incidence, prevalence, outcome, and risk factors for venous thrombosis in spaceflight. We report here the Doppler ultrasound findings of the bilateral IJV evaluations and discuss their relevance to a possible prothrombotic state.
Methods
Use of de-identified data from bilateral IJV ultrasound exams and from nutritional surveys during an occupational surveillance program for venous thrombosis in NASA astronauts was approved by NASA’s Lifetime Surveillance of Astronaut Health Advisory Board and determined to be nonhuman subjects’ research by the NASA Institutional Review Board. Data that could potentially identify a specific astronaut subject or mission are withheld.
Ultrasound protocol
Ultrasound of the deep veins is collected on active NASA astronauts on Earth (‘terrestrial baseline’) and during spaceflight (‘in-flight’). For the IJV exam, terrestrial baselines were collected with the subject’s head and torso elevation not exceeding 10 degrees from horizontal. In the early development phase of the surveillance program, some terrestrial baselines were collected after spaceflight. In-flight venous ultrasound exams were collected approximately 30 and 60 days after launch, and 6 weeks before return to Earth (referred to as ‘first, second, and third in-flight’ exams). Additional in-flight and postflight venous ultrasounds, and multispecialty conferences to discuss appropriate response, were scheduled in the eventof abnormality. All images were sent for radiologist interpretation.
Terrestrial baseline imaging was performed by a registered vascular sonographer with a Logiq E10 system, ML6-15 linear array transducer (General Electric, Milwaukee, WI, USA). In-flight ultrasound examinations were self-administered with a Vivid q system, L12-5 linear array transducer (General Electric) with real-time guidance from the NASA Johnson Space Center’s vascular team. For terrestrial exams, a sonography machine setting of ‘upper extremity venous’ was used. Early in-flight exams were completed in either the ‘upper extremity venous’ or a customized ‘small part’ preset; as the protocol developed, settings were standardized to improve visualization of blood echogenicity.
Following collection of resting-state 2D imagery and Doppler spectra during normal-effort respiration, subjects were asked to perform respiratory maneuvers for approximately 10 seconds each to record their effect on IJV flow. A Valsalva maneuver was performed to evaluate the effect of increased intrathoracic pressure. A modified Mueller maneuver, which involves slow and steady inspiration through tightly pursed lips, was performed to observe the effect of reduced intrathoracic pressure. In subjects with retrograde IJV flow in the resting state, manual compression of the contralateral IJV was also performed and its effect on ipsilateral flow documented.
Fluid intake
To approximate hydration status, average daily fluid intake data in milliliters per kilogram bodyweight were derived from self-reporting of food and fluid intake aboard the International Space Station, a standard activity downlinked weekly.
Image analysis
Image analysis was undertaken by a vascular team consisting of two radiologists (DB, AS), one aerospace medicine specialist (JP), and one vascular sonographer (AE); the remote guider always participated in the review. The following measurements were obtained: IJV cross-sectional area (IJV-CSA), right-to-left IJV-CSA ratio, peak flow velocity (IJV-PV), flow direction (antegrade or retrograde), and grade of spontaneous echo contrast (SEC), which was defined as blood echogenicity on real-time grayscale imaging. The IJV-CSA was measured at the level of the inferior thyroid, and IJV-PV was measured approximately 3–4 cm cephalad of the clavicle using manual angle correction, which approximated 60 degrees in most examinations. Measurements were made using Fujifilm Synapse Cardiovascular software, version 6.2.
Grade of IJV SEC was rated by the vascular team’s consensus on an ordinal scale of 1 through 5 following a nonblinded review of all available longitudinal and transverse cine loops. Definitions of each SEC grade (Table 1) were modified from definitions developed for the left atrium. 6 Examples of SEC grades 1–4, as seen on longitudinal imaging, are presented in Figure 1; an example of SEC visualized as a compressible, ring-like layer of echogenicity is presented in Figure 2.
Spontaneous echo contrast grades.
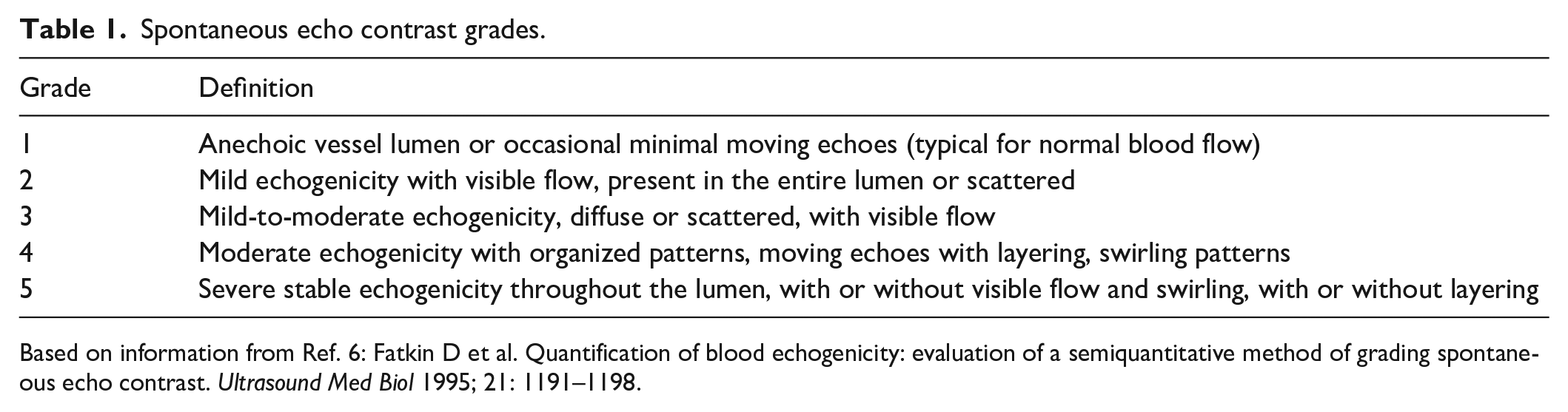
Based on information from Ref. 6: Fatkin D et al. Quantification of blood echogenicity: evaluation of a semiquantitative method of grading spontaneous echo contrast. Ultrasound Med Biol 1995; 21: 1191–1198.
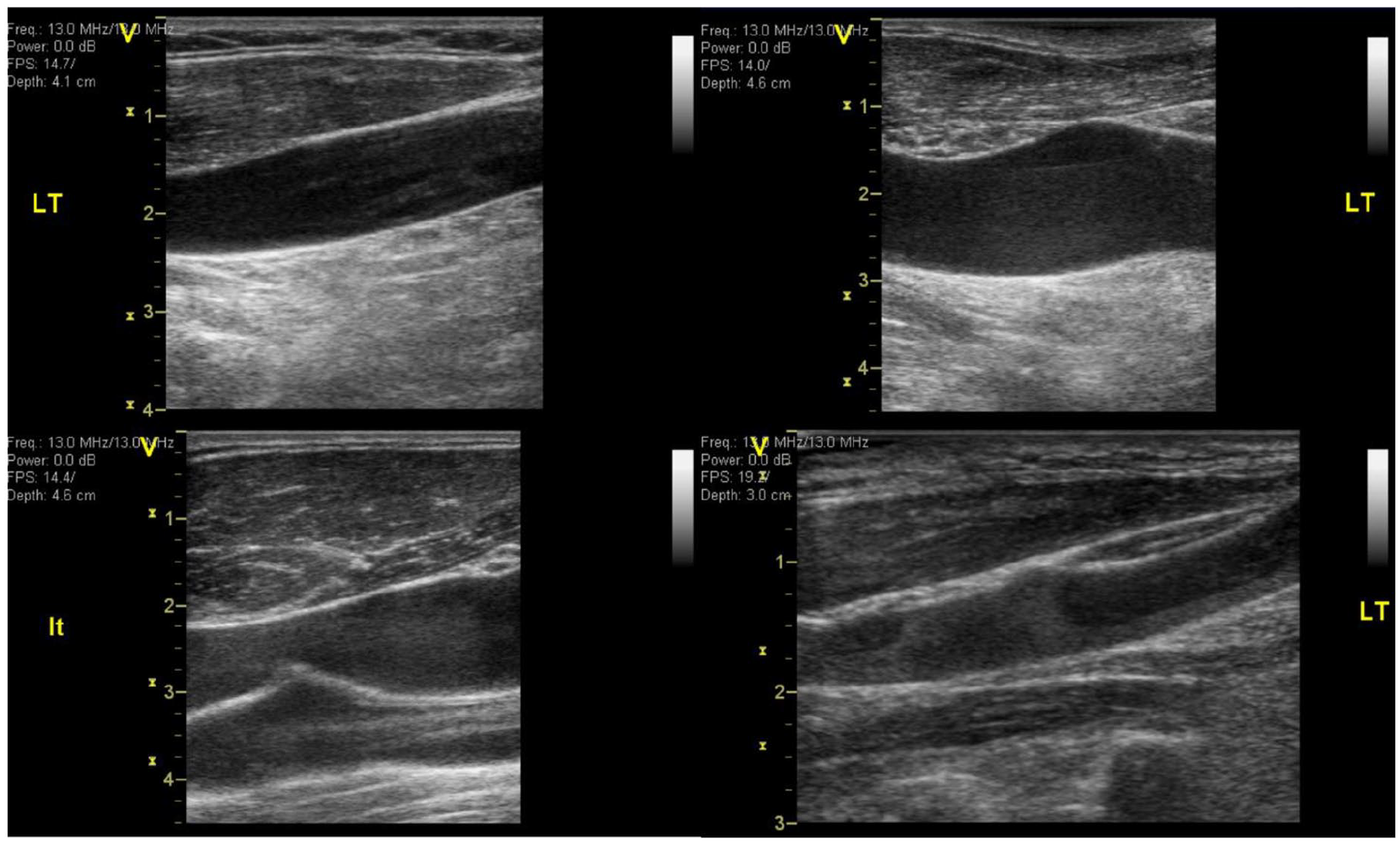
Spontaneous echo contrast (SEC) grades 1–4. Longitudinal sonographic images of the left internal jugular vein with differing flow patterns recorded during in-flight exams.
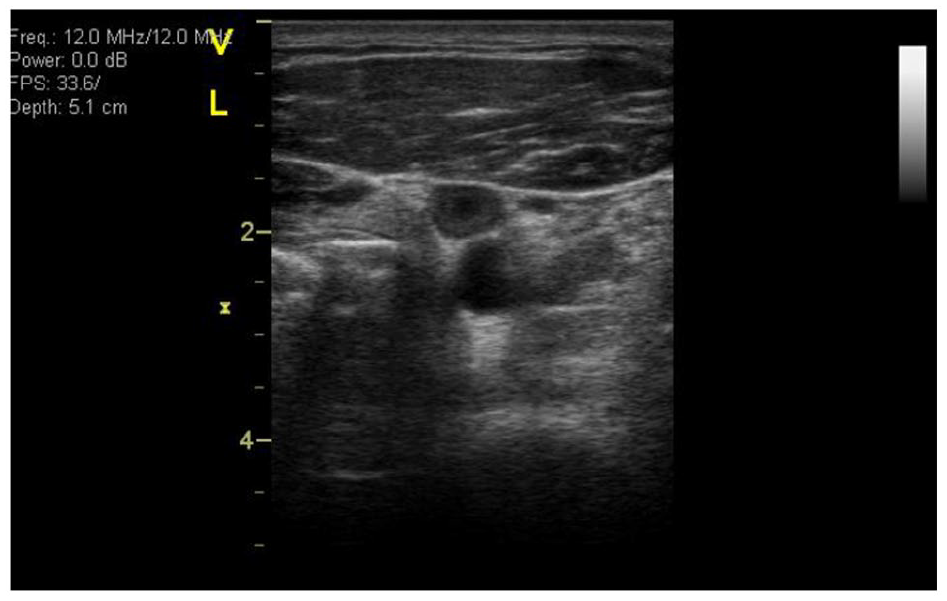
Spontaneous echo contrast (SEC) grade 3 with peripheral echogenicity. Transverse sonographic image of the left internal jugular vein showing ring-like peripheral echogenicity, seen here in an exam with SEC grade 3 flow.
Statistical analysis
The distributions of IJV measurements were described using means, SDs, medians, and IQRs. Right and left IJV-CSA and IJV-PV measurements were compared with the Wilcoxon test. Separate mixed-effects generalized linear models were used to assess the association of mission phase with IJV-CSA and IJV-PV. Each model was fit with a subject-specific random intercept to account for the repeated measurements within each subject, and with and without a sex main effect.
Univariable linear regression models were fit at each cross-sectional exam time point to assess the associations of reported fluid intake, IJV-CSA, and right-to-left IJV-CSA ratio with IJV-PV. Univariate proportional odds logistic regression models were used to assess the association between first in-flight SEC grade and terrestrial baseline measurements for the left IJV. A type I error of 5% was used for all CIs and hypothesis tests. R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria) was used for statistical modeling.
Results
Eleven NASA astronauts (six male, five female) had terrestrial baseline exams and at least one in-flight exam. Total person-time in microgravity was approximately 2150 days. Six terrestrial baseline exams were conducted preflight and five were conducted postflight. The average mission days of the first, second, and third in-flight exam were 27, 80, and 168, respectively.
No IJV DVT was diagnosed. Additional exams and multispecialty conferences were scheduled for two individuals who demonstrated slow (absolute PV < 10 cm/s) retrograde blood flow and increased echogenicity in the left IJV during spaceflight (online Supplemental Video 1). One individual (Subject 1) demonstrated retrograde flow on all in-flight exams; the other (Subject 3) demonstrated retrograde flow only on the third exam. Subject 3 also had increased echogenicity near the anterior IJV valve leaflet (online Supplemental Video 2).
Clinically recommended postflight ultrasound exams, performed 3 days after return to Earth, demonstrated antegrade IJV flow direction in both individuals; echogenicity and PV at the level of the IJV valve did not completely normalize. Subject 1 had a 3 cm segment of increased echogenicity and stagnant flow in the left IJV between the level of the bulb of the carotid artery superiorly and an in-flowing tributary vein inferiorly (online Supplemental Figure S1). Valsalva maneuver temporarily restored flow through the stagnant segment.
Measurements of IJV-PV, IJV-CSA, and right-to-left CSA ratio at baseline and at each scheduled in-flight ultrasound exam are presented in Table 2. PV was significantly lower in the left IJV than in the right IJV on all in-flight exams (p < 0.001, 0.04, < 0.001), but not at terrestrial baseline (p = 0.5). Compared to terrestrial baseline, both right and left IJV-PV were decreased in-flight, and flattening of the spectral waveform, especially on the left, was evident on the in-flight exams; some in-flight left IJV spectral waveforms appeared more peripheral than central (online Supplemental Figures S2 and S3). Mean reported daily fluid intake per kilogram of body weight was not associated with in-flight measures of left or right IJV PV (p > 0.2 for all comparisons).
Internal jugular vein measurements by exam.
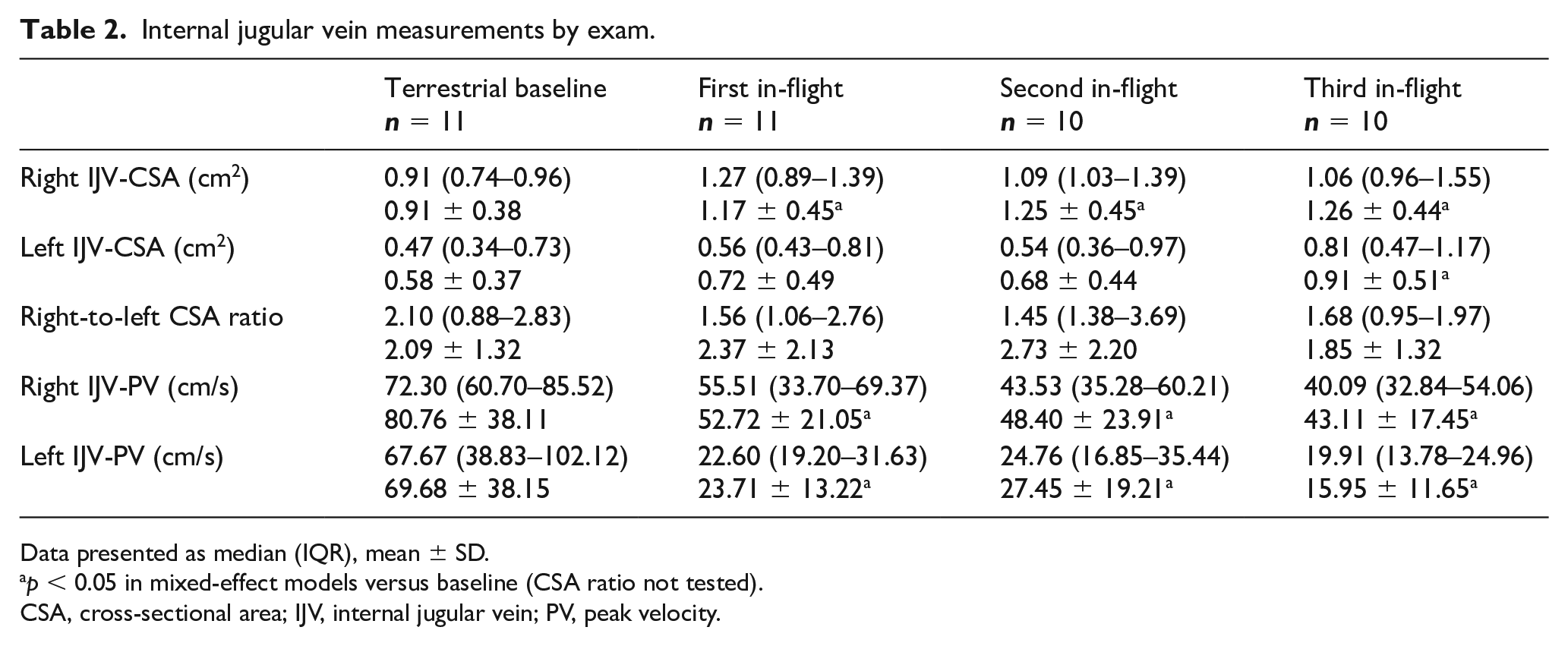
Data presented as median (IQR), mean ± SD.
p < 0.05 in mixed-effect models versus baseline (CSA ratio not tested).
CSA, cross-sectional area; IJV, internal jugular vein; PV, peak velocity.
The left IJV was significantly smaller than the right IJV at terrestrial baseline and first and second in-flight exams (p = 0.04, 0.02, 0.01, 0.2). Compared to terrestrial baseline, the in-flight right IJV-CSA was significantly increased on all exams, and the left IJV-CSA was significantly increased on the third exam (online Supplemental Tables 1–4). Ipsilateral measurements of IJV-CSA were not associated with the respective IJV-PV. The right-to-left CSA ratio was inversely correlated with the left IJV-PV only for the first in-flight exam.
Distributions of SEC grades are presented in Table 3. The right IJV did not have a SEC grade > 2 on any examination. The left IJV had grades 3 or 4 SEC on the first in-flight evaluation in five subjects. Three of these subjects had a decrease in SEC grade on subsequent evaluations; two had at least one subsequent evaluation with grades 3 or 4. There was no association between terrestrial baseline parameters (left IJV-PV, left IJV-CSA, or right-to-left IJV-CSA ratio) and first in-flight left IJV SEC grade. The left IJV-PV was inversely associated with the left IJV SEC grade on the first and third exam.
Spontaneous echo contrast distribution by exam.
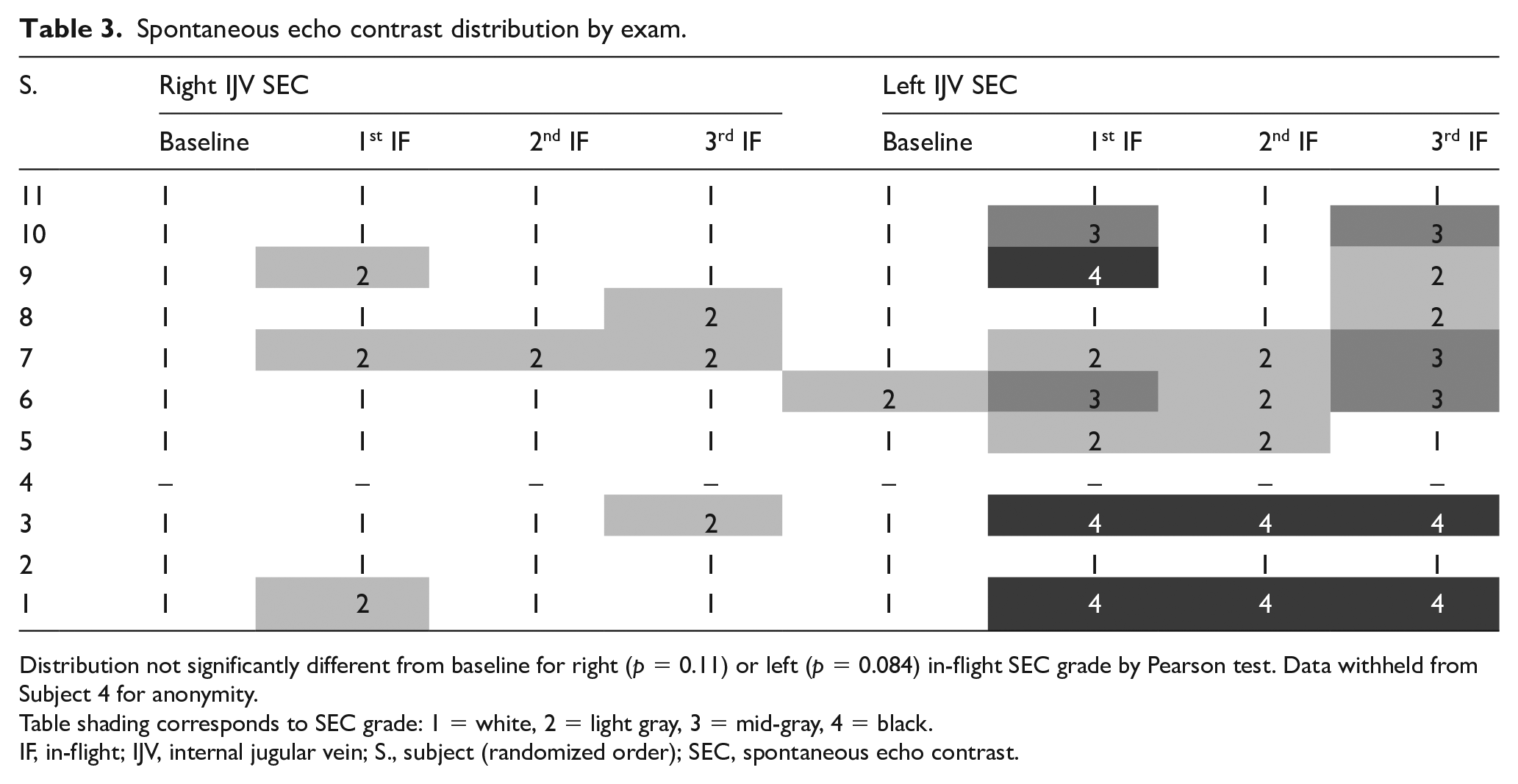
Distribution not significantly different from baseline for right (p = 0.11) or left (p = 0.084) in-flight SEC grade by Pearson test. Data withheld from Subject 4 for anonymity.
Table shading corresponds to SEC grade: 1 = white, 2 = light gray, 3 = mid-gray, 4 = black.
IF, in-flight; IJV, internal jugular vein; S., subject (randomized order); SEC, spontaneous echo contrast.
Flow response to respiratory maneuvers appeared as expected for the respective maneuver. The Valsalva maneuver decreased apparent blood flow velocity; in some cases it resulted in complete loss of flow spontaneity, and often produced a temporary increase in blood echogenicity. The modified Mueller maneuver increased apparent blood flow velocity in all individuals and reduced echogenicity. In two individuals with retrograde blood flow, both the modified Mueller maneuver and the contralateral manual compression (Figure 3) of the right IJV reversed the flow direction to antegrade while the maneuver was performed.
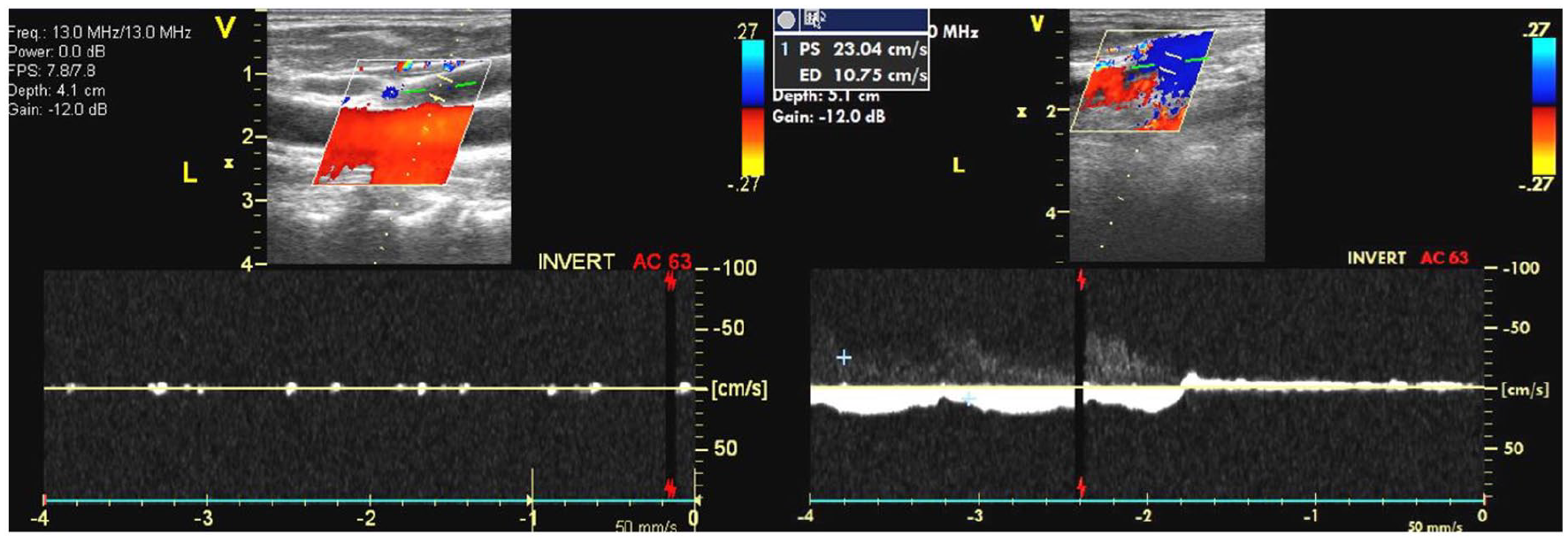
Flow augmentation in left IJV by right IJV compression.
Discussion
Recent observations of stagnant IJV flow patterns in several astronauts and an asymptomatic case of left IJV DVT have raised concerns about whether spaceflight may lead to a prothrombotic state. 1 Differentiating expected and clinically not relevant flow abnormalities from those that may signify a prothrombotic state or asymptomatic or symptomatic DVT is necessary for a meaningful, evidence-based assessment of risk, prevention, and management.
In this review, no cases of IJV DVT were diagnosed in 11 astronauts with approximately 2150 person-days of spaceflight. Two cases of left IJV retrograde flow and intravascular imaging abnormalities were identified, striking enough for clinical concerns to be raised, prompting a multispecialty review and additional, previously-not-scheduled ultrasound examinations. However, no diagnoses of DVT were made, and the use of anticoagulation was not recommended in either case.
Compared to measurements on Earth, we observed decreased PV in both the right and left IJV, an increased CSA with a wide range in asymmetry, increased blood echogenicity in some individuals (most frequently in the left IJV), and slow, retrograde left IJV blood flow in two individuals. Because no DVT was diagnosed, the relationship between these variables and thrombosis is not certain. However, their trends relative to terrestrial baseline justify further attention.
Qualitative slow flow – defined as an increase in echogenicity on grayscale ultrasound – has been shown to be a weak risk factor for development of lower-extremity DVT in patients with malignancy. 4 More broadly, stagnant blood flow secondary to prolonged immobilization is thought to be one mechanism by which VTE risk approximately doubles during long airline flights. 5 Because the hydrostatic pressure gradient in the venous circulation is always zero in microgravity irrespective of body position (i.e., there is no head ‘up’, supine, or head ‘down’ positions in microgravity), astronauts who develop slow flow in some veins may do so for a prolonged period. On Earth, risk for airline flight-associated VTE is increased with hereditary thrombophilia and oral contraceptive use, raising the question whether screening for thrombophilia before spaceflight, and appropriate counseling and modification of estrogen use, are warranted.5,7
Slow blood flow was most prominent in the left IJV, and left IJV-CSA was generally smaller than the right IJV-CSA. These findings are consistent with prior literature that the right IJV is dominant in terms of area, average velocity, and overall flow. However, we did not find that IJV-CSA was associated with peak velocity on univariate analysis, which suggests that IJV area – at least measured at one point – is not explanatory. Extrinsic factors affecting IJV flow but not measured in this surveillance include anatomic asymmetry of the transverse sinuses and possible compression of the left brachiocephalic vein between the aortic arch and the sternum, which can cause IJV reflux in some individuals.8,9 IJV compression may also occur in the neck by the styloid process and the carotid artery. 10 It has also been hypothesized that, in microgravity, the IJV may not shift away from a potential compression point between the sternocleidomastoid muscle and the carotid artery due to the lack of blood weight. 11
Lower PV was associated with increased SEC in the left IJV in-flight. This is consistent with findings of increased SEC in patients with nonvalvular atrial fibrillation with low left atrial emptying velocity, and consistent with the understanding that SEC reflects red blood cell (RBC) aggregation, a normal and reversible occurrence under conditions of low shear rates, and an anomalous occurrence in inflammatory states.12 –14 Increased RBC aggregation is a mechanism for the development of anomalous whole blood viscosity, further increasing resistance to flow, potentiating a vicious cycle. In our surveillance, SEC grade 1 was consistently associated with antegrade flow with generally laminar characteristics, whereas SEC grades 3 and 4 were seen during relative stasis.
Apart from reduced flow velocity, other changes associated with spaceflight may contribute to the finding of increased SEC in some individuals. For example, exposure to microgravity leads to an acute plasma volume reduction of approximately 17% within 24 hours, which is only partially compensated by a hemolytic reduction of RBC mass, resulting in a chronic increase in hematocrit by up to 10%.15 –17 Increased hematocrit would further exacerbate a rise in localized whole blood viscosity and may be independently associated with thrombosis risk. 18
Whether higher SEC grades in the left IJV of healthy subjects signify a prothrombotic state remains unclear. In nonvalvular atrial fibrillation, a higher-grade SEC is correlated with an increased risk for stroke, even accounting for other high-risk features.12,19 Small studies suggest there may be similar associations in the venous circulation. SEC in the IJVs is positively correlated with a higher plasma fibrinogen level, high-sensitivity C-reactive protein, and prior stroke, and in those critically ill with coronavirus disease, the presence of venous SEC was associated with ‘clotting events’.20,21
Most subjects maintained the normal antegrade direction of IJV flow bilaterally. However, slow retrograde flow was observed in two individuals during spaceflight. Both modified Mueller and contralateral compression reversed flow to antegrade and reduced the severity of SEC. Induced flow normalization argues against fixed intravascular obstruction by an anechoic or occult obstructive blood clot. Restoration of flow during contralateral pressure also suggests that some venous return is shunted to the right side in these individuals. Given the decrease in SEC appearance following the Mueller maneuver, its intermittent use may help break up layering RBC aggregates.
In one individual with retrograde flow (Subject 1), a segment of stagnant flow was observed postflight between the level of the carotid bulb and an inflowing tributary vein, suggesting a venous bypass circuit around compression. Paradoxically, sustained Valsalva maneuver temporarily restored antegrade flow through the stagnant segment – as pressure and volume increased, the inward compression placed on the jugular vein was relieved, and flow restored. However, this bypass circuit was insufficient to sustain antegrade flow in microgravity; tributary vein inflow was present during spaceflight, but overall flow remained retrograde.
In the other individual with retrograde flow (Subject 3), a small poorly defined and weakly hypoechoic focus with stronger central echogenicity was seen just caudal to the ventral cusp of the IJV valve, which was initially suspicious for an early incipient thrombus upon image review (online Supplemental Video 2). However, the final impression favored the interpretation that the structure represented a cluster of stable macro-aggregates with minimal or no fibrinous stroma. In this individual, the IJV lumen at the level of the carotid bulb was not compressed, which suggests that retrograde flow in microgravity has diverse etiologies.
Ultimately, a reversed pressure gradient must be the cause of retrograde venous flow; it also implies preexisting or newly developed IJV valve incompetence, as the IJV valve works to prevent the cerebral circulation from transient increases in pressure. 22 The prevalence of IJV valve incompetence in the general population is not well known; studies have reported rates between 0 and 90%.22,23 Chronic dilation of the IJV in microgravity may contribute to the development of valve incompetence, and it may also be possible that slow monophasic flow does not impart sufficient force on the cusps to effect their full approximation.
Study limitations
There are several limitations associated with this review of occupational surveillance data. Firstly, as an occupational surveillance project, data collection was primarily focused on evaluation for presence of thrombus, was time-constrained by work schedule, and did not control environmental variables prior to examination (e.g., hydration).
Secondly, the absence of DVT in these 11 subjects prevents firm conclusions about flow abnormality as a risk for DVT. However, the finding that spontaneous flow had not recovered even after thrombus recanalization in the aforementioned case of IJV DVT in an astronaut suggests that stasis in the jugular vein – potentially exacerbated by an available venous bypass circuit – may have preceded and contributed to thrombus formation.
Thirdly, astronauts are not experienced sonographers, and acting as their own probe operators for the in-flight exams may introduce variability in probe pressure, position, and angle between subjects; focus should be placed on standardization including a spectral Doppler angle of 60 degrees when possible.
Fourthly, differences in ultrasound machine model and mode may account for some variability in SEC grade. Going forward, standardization between terrestrial and in-flight ultrasound frequency, among other settings, should be pursued, as SEC visualization depends on the combination of ultrasound wavelength and the size of cellular aggregates. These differences may have affected the sensitivity for lower-grade SEC, which reflects the presence of smaller RBC aggregates. However, ultrasound settings were consistent within each exam, and increased SEC grade in-flight was observed mostly on the left side – suggesting a true underlying difference.
Fifthly, classifying postflight exams as terrestrial baseline may be confounding if microgravity exposure induces persistent changes. However, prior investigations have demonstrated normalization of Doppler spectra after landing in most individuals. 1 In our surveillance, two individuals with retrograde flow had preflight and postflight exams for comparison; postflight, we observed antegrade flow and higher PV versus that in-flight, but lower PV versus that preflight. This finding suggests that classifying postflight data as baseline may bias our result in the null direction.
Lastly, IJV measurements are influenced by multiple variables, including hydration status, heart rate, breathing effort, and positioning. 24 Average daily fluid intake did not correlate with our in-flight measurements, but our estimate may not be granular enough to reflect status at the time of the exam, and it is possible that there was a difference between in-flight and baseline hydration status. Heart and respiratory rate were not monitored during these exams; however, measurements occurred under normal respiratory effort.
Regarding positioning, all in-flight exams were standardized for postural effects by the factor of weightlessness (i.e., the absence of hydrostatic pressure). However, our terrestrial baseline IJV data were subject to hydrostatic pressure, and subject positioning may influence some difference between our baseline and in-flight measurements. 25 Unfortunately, the exact angle at which to position subjects terrestrially to best approximate microgravity for IJV evaluation is unknown; studies utilizing the supine position as baseline have reported discordant results.1,26 Research-driven projects could consider use of parabolic aerial flight – which is not used for training and thus not part of this occupational surveillance – to simulate microgravity for brief periods of time (approximately 20 seconds per parabola, preceded and followed by hyper-gravity) to gain insight into changes in venous dynamics as the hydrostatic gradient is removed. However, acute changes during parabolic flight may be dissimilar to the steady-state changes seen in sustained weightlessness, which cannot be reproduced on Earth.
Conclusion
No IJV venous thrombosis was observed during this occupational surveillance study. Abnormal flow characteristics in microgravity, predominantly observed in the left IJV, including reduced peak velocities, retrograde flow, and increased blood echogenicity, may signal an increased risk for thrombus formation in individuals with the most extreme aberrations. Anatomical variants in the cerebral venous outflow pathways may predispose the left IJV to abnormal flow in microgravity. Slow and echogenic flow can be temporarily improved with respiratory maneuvers and manual compression of the contralateral internal jugular vein, suggesting their use as diagnostic and preventive measures. Continued venous surveillance of astronauts during spaceflight, its enhancement with appropriate biomarker assays, and review of the biophysical aspects of craniocervical drainage in microgravity is warranted.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221086619 – Supplemental material for Surveillance for jugular venous thrombosis in astronauts
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221086619 for Surveillance for jugular venous thrombosis in astronauts by James Pavela, Ashot Sargsyan, Deepak Bedi, Aaron Everson, Jacqueline Charvat, Sara Mason, Benjamin Johansen, Karina Marshall-Goebel, Sarah Mercaldo, Ronak Shah and Stephan Moll in Vascular Medicine
Footnotes
Acknowledgements
The authors acknowledge NASA’s Nutritional Biochemistry Laboratory, for their collection and maintenance of fluid intake records.
Data availability
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Institutional support was provided by NASA.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.