
Abstract
Keywords
Introduction
May-Thurner syndrome (MTS) is a condition in which the right common iliac artery, which supplies blood to the right leg, compresses the left common iliac vein, which returns blood from the leg to the heart. Most patients with this anatomy have no symptoms, but some can develop blood clots in the vein related to this compression. MTS can be diagnosed using ultrasound and other non-invasive imaging tests. Treatments are aimed at dissolving blood clots and relieving the compression that caused them to form.
What is May-Thurner syndrome?
May-Thurner syndrome (MTS) is a relatively rare vascular condition that involves narrowing of the left common iliac vein, which runs between the right common iliac artery and the lower part of the spine. The arteries are the tubes that take blood from the heart to the body (including the limbs), and the veins are the tubes that return blood from the body to the heart. Sometimes the vein can become compressed between the artery and spine, leading to highly variable symptoms. The syndrome is named after the doctors who first described the condition in the 1950s. 1
Most people who have left common iliac vein compression have no symptoms, but sometimes MTS may cause symptoms and may lead to the formation of blood clots known as deep vein thrombosis (DVT) and pulmonary embolism (see Vascular Disease Patient Information Page on venous thromboembolism 2 ). DVT and pulmonary embolism can be serious medical conditions if not recognized and treated in a timely and effective fashion.
Who is at risk for May-Thurner syndrome?
Significant compression of the left common iliac vein is thought to be present in up to one-third of the general population. MTS is primarily seen in people aged 18–50 years old, and women are five times more likely than men to have MTS. Surgery, pregnancy, oral contraceptive use (birth control pill), dehydration, cancer, and infection may predispose individuals with MTS to blood clot formation (DVT).
What are the signs and symptoms of May-Thurner syndrome?
Many people with MTS anatomy have no symptoms; however, progression to significant narrowing or complete closure (occlusion) of the vein can occur. Occlusion of the left common iliac vein may lead to swelling of the left leg and other symptoms including skin color changes, hardening or thinning of the skin, and even development of sores on the lower part of the leg called venous stasis ulcers.
Symptomatic MTS most commonly occurs in women in their 20s and 30s, when they develop left leg swelling, heaviness, and pain, also known as venous congestion. The symptoms may come on gradually (over weeks to months) or suddenly (over hours to days). Symptoms may come and go or worsen through the course of the day, particularly after prolonged standing or sitting, causing significant leg swelling or tenderness. Symptoms typically affect the left leg or pelvis, but right-sided and both-sided symptoms of MTS have been reported. Swelling usually involves the entire affected leg; often it is noticeably larger than the opposite leg. The swelling may or may not be associated with the formation of a blood clot (DVT). A significant number of patients with MTS also experience venous claudication, which is defined as thigh or leg pain and tightness that comes on with exercise and subsides with rest or elevation of the leg.
How is May-Thurner syndrome diagnosed?
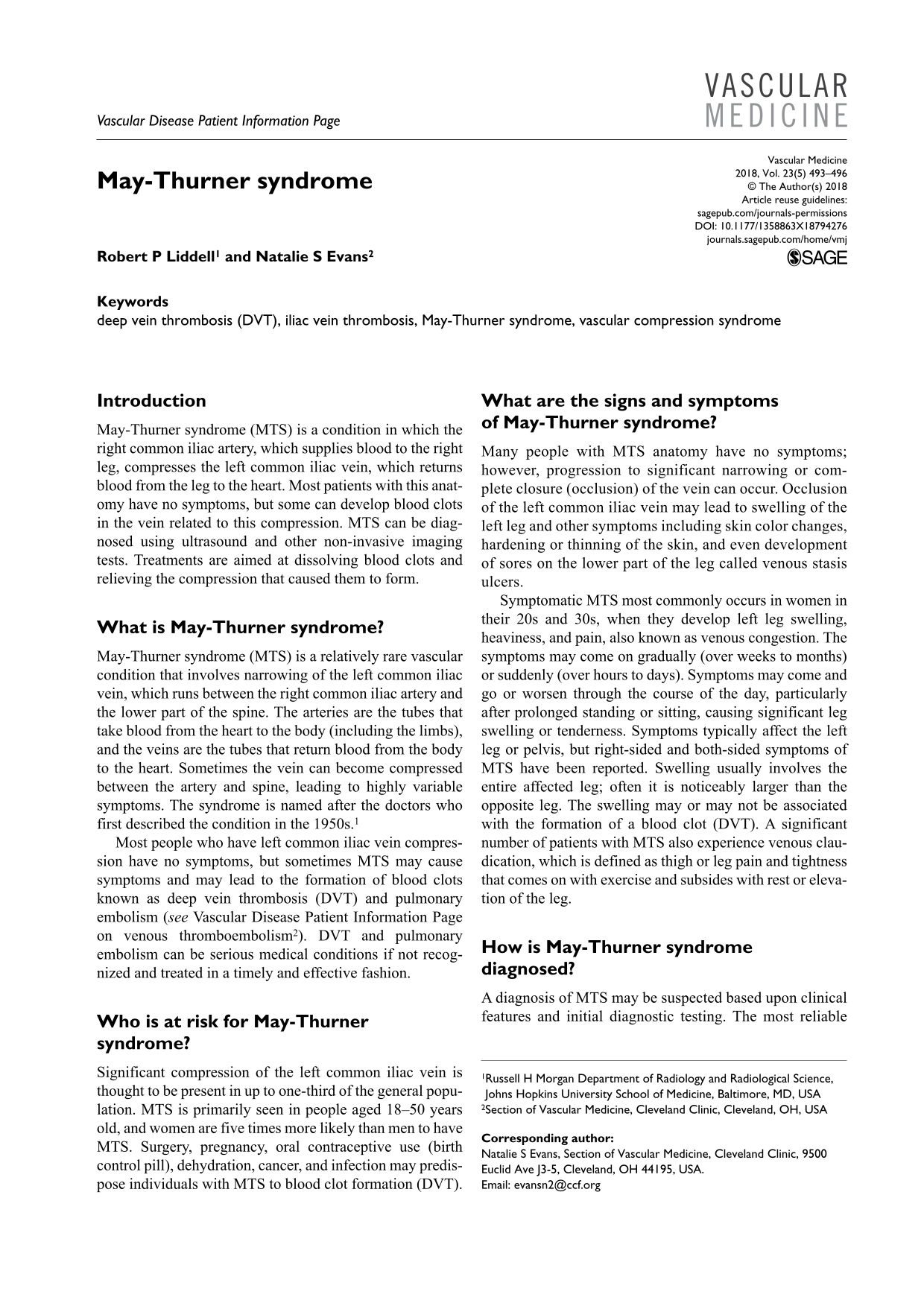
A diagnosis of MTS may be suspected based upon clinical features and initial diagnostic testing. The most reliable initial test to evaluate leg swelling is a venous duplex ultrasound (sometimes called a ‘Doppler’ study; see Vascular Disease Patient Information Page on the vascular laboratory 3 ) to rule out DVT (Figure 1). Ultrasound is a non-invasive test that uses sound waves to create pictures of the leg veins; however, direct ultrasound visualization of the iliac veins is often difficult due to their relatively high location within the pelvis. Computed tomography (CT) and magnetic resonance imaging (MRI) are extremely useful non-invasive tests that can directly visualize compression of the vein by the artery, as well as DVT and collateral vessels often seen in patients with MTS. Collateral vessels are smaller veins that form to try to bypass a blocked or severely compressed or narrowed vein.
A 27-year-old woman with a history of smoking while taking oral contraceptive (birth control) pills presented with 3 days of increasing left leg swelling and pain suspicious for DVT. Doppler ultrasound examination demonstrates a blood clot within the left common femoral vein (arrow) extending to the left external iliac vein (left side of the image). This patient was ultimately found to have May-Thurner syndrome.
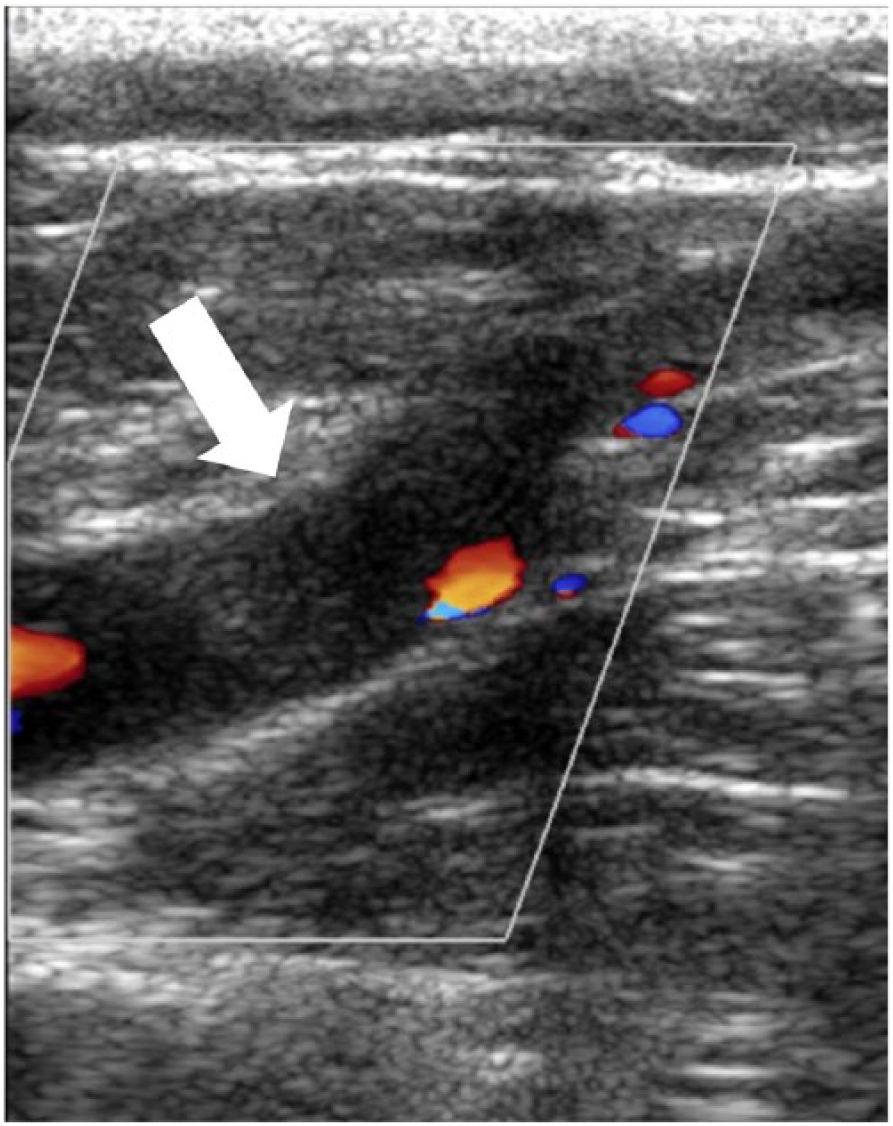
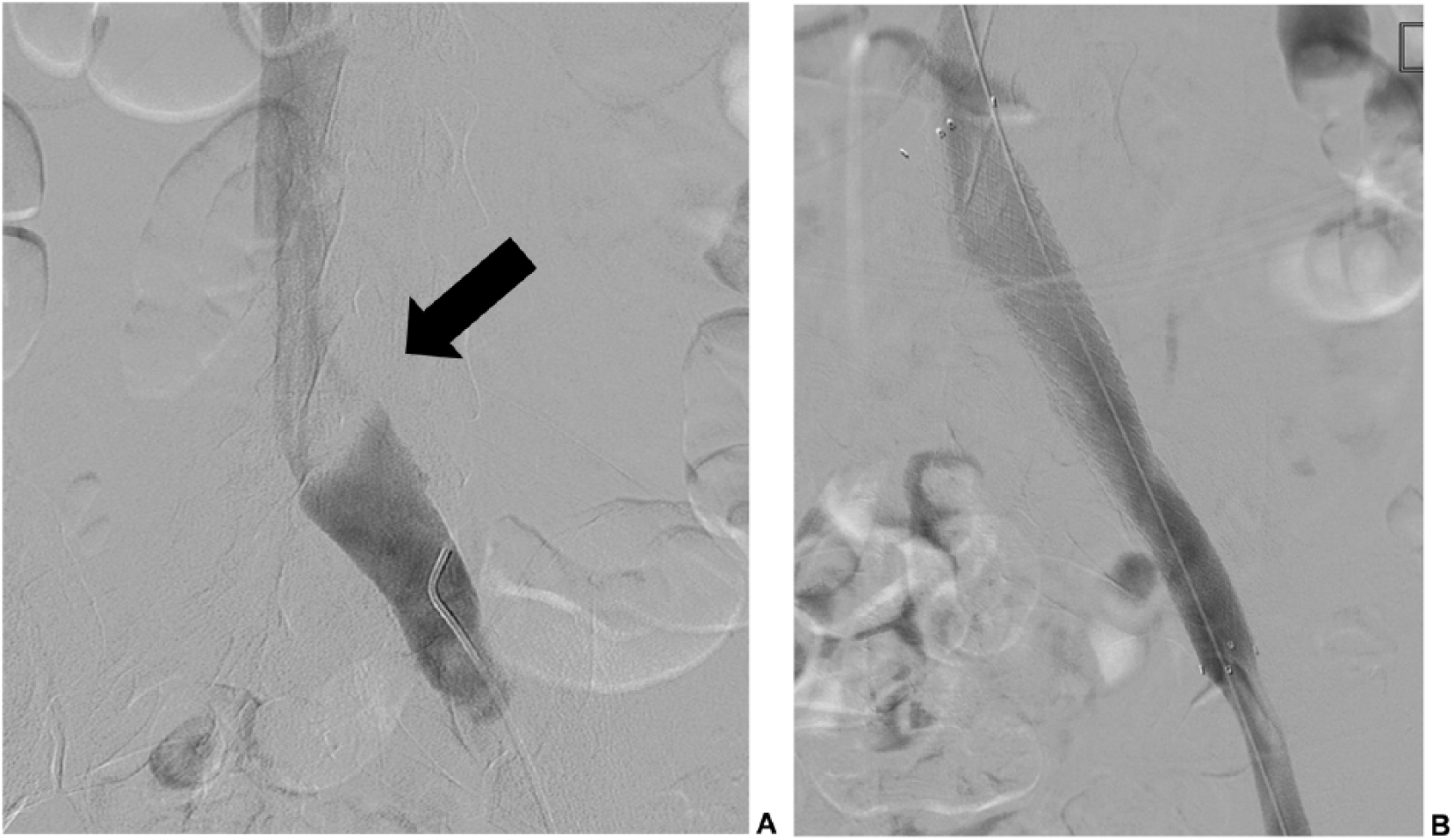
Minimally invasive imaging techniques such as venography and intravascular ultrasound (IVUS) may be more helpful in identifying left common iliac vein compression and determining its severity compared to CT and MRI. In venography, a small tube (catheter) is inserted into the vein, and dye that lights up on X-rays is injected to outline the vein (Figure 2). In IVUS, a catheter is placed in the vein and a tiny ultrasound device is used to take pictures of the vein from the inside (Figure 3). Venography and IVUS are most often reserved for cases of suspected MTS in which treatment like angioplasty or stenting are planned.
(A) Left leg venogram demonstrating narrowing (arrow) within the left common iliac vein due to compression caused by the overlying right common iliac artery. (B) Venogram after stent placement, demonstrating restoration of venous blood flow within the left common iliac vein.
(A) IVUS images before intervention, demonstrating compression of the left common iliac vein (white arrow) by the overlying right common iliac artery (black arrow). (B) IVUS after stent placement, demonstrating a wide open left common iliac vein (white arrow) and the overlying right common iliac artery (black arrow). IVUS images are created from an ultrasound catheter that is placed within the veins.
What are the treatment options for May-Thurner syndrome?
The primary goals of treatment for MTS are to restore normal blood flow in the compressed common iliac vein and to remove any clot that may have formed as a result of narrowing. Treatment for iliac vein compression is generally reserved for patients with symptoms, most commonly those with new DVT. However, a number of reports have shown promise in treating patients with older (chronic), more scar-like DVT who have increasing or new symptoms in the affected leg. 4
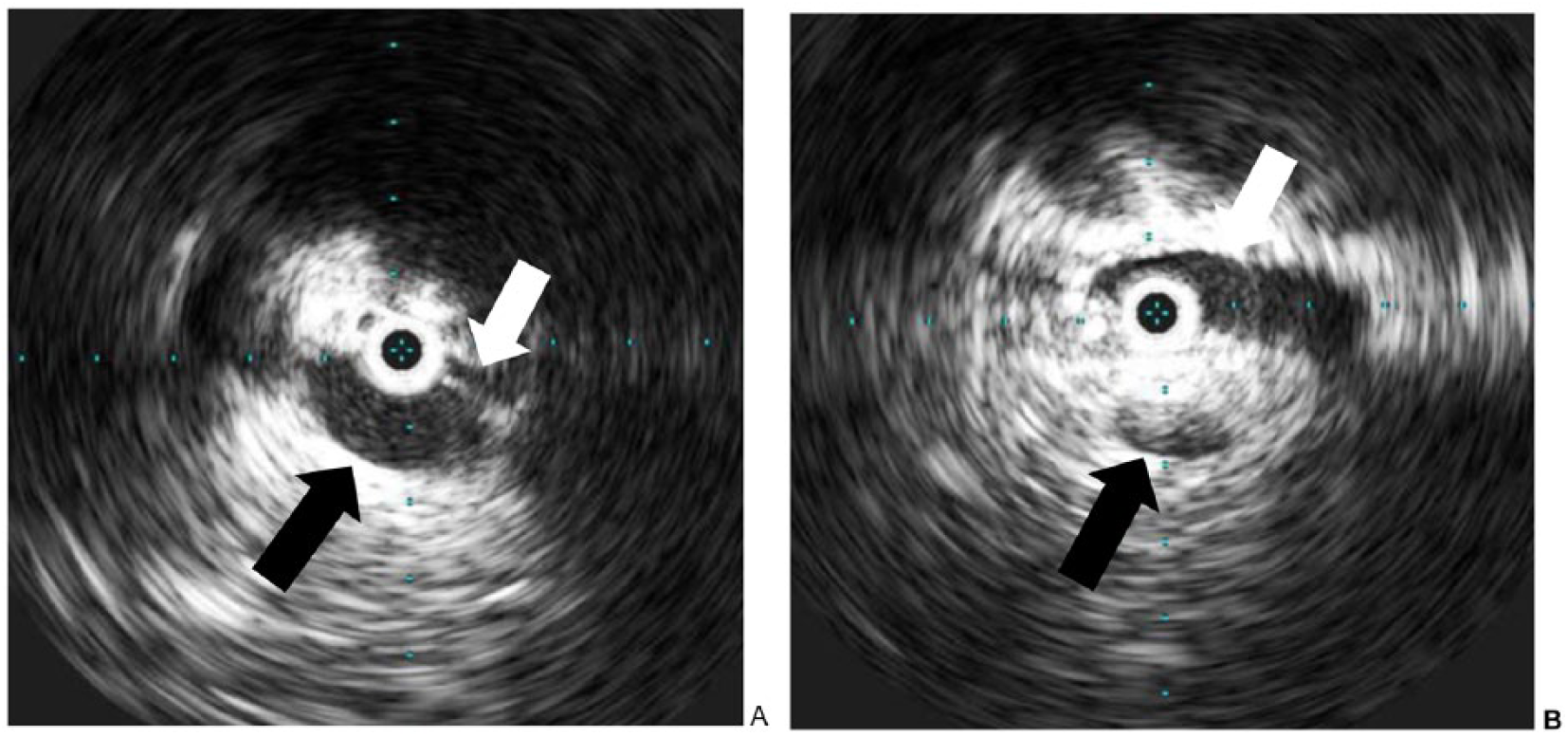
Treatment strategies have evolved from more invasive, open surgical techniques to minimally invasive therapies using catheters and imaging guidance. These new techniques often use medications known as clot-busters (thrombolytics) to dissolve the blood clot (DVT) and balloons and stents to prop open the vein (Figure 4). 5 Anticoagulant medications (blood thinners) are also considered the mainstay of treatment for DVT and are used in combination with these techniques. In general, long-term anticoagulation and elastic compression stockings are recommended following treatment to help prevent recurrent clot formation and limit the risk of post-thrombotic syndrome (PTS). PTS may occur in up to one-half of patients with extensive DVT and consists of some combination of leg pain, swelling, redness, or skin changes. Symptoms of PTS may come and go, and can be very debilitating for some patients (see Vascular Disease Patient Information Page on the post-thrombotic syndrome. 6 )
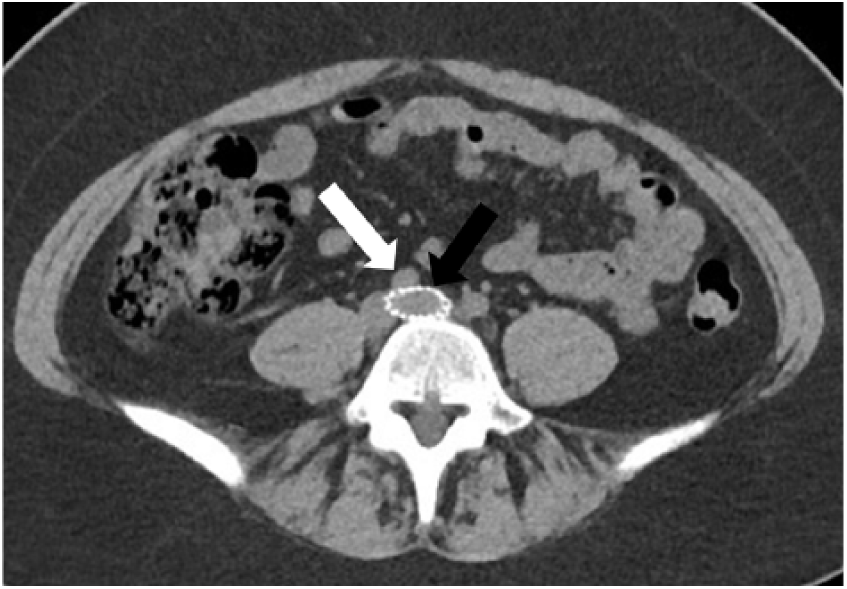
CT scan of the pelvis shows a stent within the left common iliac vein (black arrow) between the right common iliac artery (white arrow) and the lumbar spine.
Less common treatment options for MTS include open surgical clot removal (thrombectomy) with repositioning of the right common iliac artery away from the left common iliac vein, and various bypass procedures. These surgical procedures are usually reserved for cases in which minimally invasive therapies such as angioplasty and stent placement have failed.
What about May-Thurner syndrome without a blood clot?
Patients with left common iliac vein compression who do not have an associated blood clot (DVT) usually do not have any symptoms. The vein narrowing in these cases is often discovered on a CT or MRI performed for other reasons. Sometimes, patients without blood clots will have symptoms associated with the slow venous drainage from the left leg, including debilitating pain, swelling, venous claudication, varicose veins, and formation of venous stasis ulcers. The goal of treatment in these patients is to improve venous flow through the compressed iliac vein in order to relieve these symptoms and theoretically prevent future blood clot formation. Some studies have shown significant symptom improvement in patients who have undergone stent placement for iliac vein compression who have never had an associated blood clot. 4
What are the potential risks of treatment?
Overall, minimally invasive procedures such as angioplasty and stenting for iliac vein compression are safe. The early (within the first 30 days of the procedure) complication rates are very low (less than 10%). 7 Bleeding and small hematomas (blood collections in the tissue) at the site of catheter insertion are the most common complications and are generally treated with applying pressure to the affected area and monitoring. The risk of these complications has significantly decreased by using ultrasound to guide where the catheter is inserted. Delayed (after 30 days) complications most often involve the affected vein becoming narrow again or clotting off. Treatment with blood thinning (anticoagulant) medications for a short period after stenting has been shown to decrease the risk of complications.
After treatment for May-Thurner syndrome, what monitoring is needed over the long-term? What symptoms may occur?
After the blood flow has been restored, treatment is needed with blood thinners to prevent recurrence of the blood clot (DVT). How long the blood thinners are needed depends on the estimated risk of recurrence. Referral to a hematology or vascular medicine specialist should also be considered to optimize anticoagulation therapy and manage risk factors for future blood clots. Patients usually return to the office for follow-up approximately 1 month after the procedure. Imaging with ultrasound, CT, or MRI is often performed to see if the veins and any stents that were placed are still open.
Additionally, patients should be aware of the signs and symptoms which may suggest that the vein is becoming re-narrowed or blocked, which are increasing leg swelling, pain, skin discoloration, or venous claudication.
Summary
MTS, classically described as compression of the left common iliac vein by the right common iliac artery, is a relatively rare vascular disorder seen primarily in young women. Patients with MTS may either have no symptoms or have symptoms associated with left leg DVT or venous congestion. Non-invasive imaging, including duplex ultrasound, CT, and MRI, are used to confirm the diagnosis of MTS in those with symptoms, and these imaging studies play an important role in planning treatment. Minimally invasive treatment techniques such as clot-buster medications, angioplasty, and stenting provide safe and effective methods to relieve acute symptoms and prevent the development of chronic symptoms associated with PTS. Anticoagulation (blood thinners), clinical follow-up, and non-invasive imaging all play critical roles in preventing the relapse of MTS and its associated complications.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.