
Abstract
Immobility is a well-recognized risk factor for deep vein thrombosis (DVT) in surgical patients, whereas the level of DVT risk conferred by immobility is less defined in patients on medical wards. The aim of this study was to establish whether immobility and its duration are associated with the risk of DVT in acutely ill medical inpatients. We conducted a cohort study in acutely ill medical inpatients. Patients underwent whole leg ultrasound for suspected lower extremity DVT and were divided into two groups according to presence or absence of immobility, defined as total bed rest or sedentary without bathroom privileges. The endpoint was the detection of proximal DVT or isolated distal DVT (IDDVT). Among the 252 acutely ill medical inpatients with immobility (age 82.6 ± 10.3 years, female 63.9%), ultrasound showed 36 (14.3%) proximal DVTs and 39 (15.5%) IDDVTs, while there were 11 (4.4%) proximal DVTs and 26 (10.5%) IDDVTs among the 248 inpatients without immobility (age 73.6 ± 14.2 years, female 54.8%). The risk of proximal DVT was higher in immobile than in mobile patients (OR 3.59, 95% CI: 1.78–7.23, p = 0.0001), whereas the risk of IDDVT was similar between the two groups (OR 1.56, 95% CI: 0.92–2.66, p = 0.111). During the first 3 days of hospitalization, the frequency of all DVTs was similar in patients with and without immobility, but it was 0.26 ± 0.03 vs 0.18 ± 0.03, respectively, after 4 days. In conclusion, immobility for more than 3 days is a risk factor for proximal DVT in acutely ill medical inpatients.
Keywords
Introduction
Deep vein thrombosis (DVT) and pulmonary embolism (PE) are still a major health problem in the European Union, with 370,000 venous thromboembolism (VTE) related deaths per annum. 1 Hospitalization is one of the most important factors influencing the risk of VTE, as lower extremity DVT incidence is at least 10 times higher in hospitalized patients than in community residents.2,3 In surgical patients, the risk of DVT is clearly defined, but it can be high in medical inpatients as well, in whom DVT prevalence is higher than in outpatients. 4 In the Prophylaxis in Medical Patients with Enoxaparin (MEDENOX) 5 trial and in the Prospective Evaluation of Dalteparin Efficacy for Prevention of VTE in Immobilized Patients Trial (PREVENT) 6 the incidence of symptomatic DVT was 1.5% and 0.95%, respectively, in the placebo arms. The increased DVT risk in hospitalized medically ill patients may be due to the higher prevalence of DVT risk factors in such patients. Immobility or reduced independent mobility is an important and highly prevalent risk factor for DVT in hospitalized patients. A sustained period of immobility leads to vascular stasis, one of the cornerstones of Virchow’s triad in the pathology of thrombosis. 7 In surgical patients, immobility is often secondary to surgery itself and early mobilization after surgery can reduce VTE incidence. 8 In medical ward inpatients, immobility is highly prevalent as well because the diseases leading to hospitalization, such as respiratory failure, heart failure, sepsis, stroke, etc., may provoke bed confinement. A meta-analysis of epidemiological studies showed that immobility was associated with a two- to threefold increase in VTE risk in medical patients. 9 Thirty-six cohort studies were included, but only 10 studies were conducted in cohorts of patients. Among these 10 studies, seven explored only the incidence of PE without any data on DVT. Three studies evaluated the clinical scores for DVT prediction in hospitalized patients, but they enrolled patients from surgical, intensive care, and internal medicine units. Moreover, only proximal DVT was diagnosed. Three other studies reported risk factors associated with DVT in hospitalized patients, but they were cross-sectional studies.10–12 Almost all patients in the DVT group of the larger study had reduced mobility, 10 while the other two studies included a small sample size of less than 200 patients, 11 with DVT developing before hospitalization. 12 Since the level of risk for proximal and isolated distal DVT (IDDVT) conferred by immobility in acutely ill medical inpatients is not clearly defined, the purpose of this study was to evaluate how immobility and its duration can contribute independently to the risk of lower limb proximal DVT and IDDVT in acutely ill medical inpatients.
Methods
Study design
This was a cohort study performed in a tertiary care academic hospital (S. Orsola-Malpighi University Hospital, Bologna, Italy) from October 2016 to March 2017.
Symptomatic patients (with at least one of the following acute symptoms: leg pain, leg swelling, calf cramps, calf redness, calf warmth) were eligible for the study if they were hospitalized in medical wards for acute illness and developed DVT suspicion after admission. Inclusion criteria were acute congestive heart failure, acute respiratory disease, infection, acute exacerbation phase of an inflammatory disease, stroke, critical limb ischemia, acute pancreatitis, peptic ulcer disease, hepatic decompensation, and diabetic decompensation. Patients were excluded if they had DVT symptoms before hospital admission, were hospitalized for DVT and/or PE or had a diagnosis of DVT or PE in the previous 12 months, were younger than 18 years, were pregnant or during puerperium, and had undergone surgery or had a leg fracture or plaster cast within 3 months before admission – although patients with minor trauma of the symptomatic leg were included. Moreover, we excluded patients that were already receiving anticoagulants such as vitamin K antagonists or direct oral anticoagulants before admission. All consecutive eligible patients were enrolled during business days.
During the hospital stay, in case of suspected lower extremity DVT, the medical ward clinician ordered an ultrasound (Figure 1), which was performed within 24 hours as whole leg duplex ultrasound (DUS). Patients were carried to the vascular emergency room on their own hospital bed (beds have wheels in our hospital) or using a wheelchair. The vascular emergency room is the only reference unit in our hospital for patients with suspected DVT. At the vascular emergency room, patients signed the informed consent and a separate investigator reviewed the clinical files, performed a physical examination of the patient in the supine position, and elicited a personal and family history from each patient, collecting data on a standardized form. Patients were divided into two groups according to the presence or absence of immobility at the time of admission to the medical ward. The designation of immobility was made from the review of activity orders/status. Immobility was defined according to the level 1 immobility EXCLAIM eligibility criteria 13 as total bed rest or sedentary without bathroom privileges. The immobility status had to be constant from medical ward admission and the time when DUS was performed. Patients were not categorized in the immobility group in cases where they met the criteria for immobility only for a part of their hospital stay. Next, a third clinician performed and interpreted the DUS (Figure 1). The number of days from admission (day 0) to the time when suspicion of DVT arose were calculated. The endpoint of the present study was the detection of proximal and IDDVT.
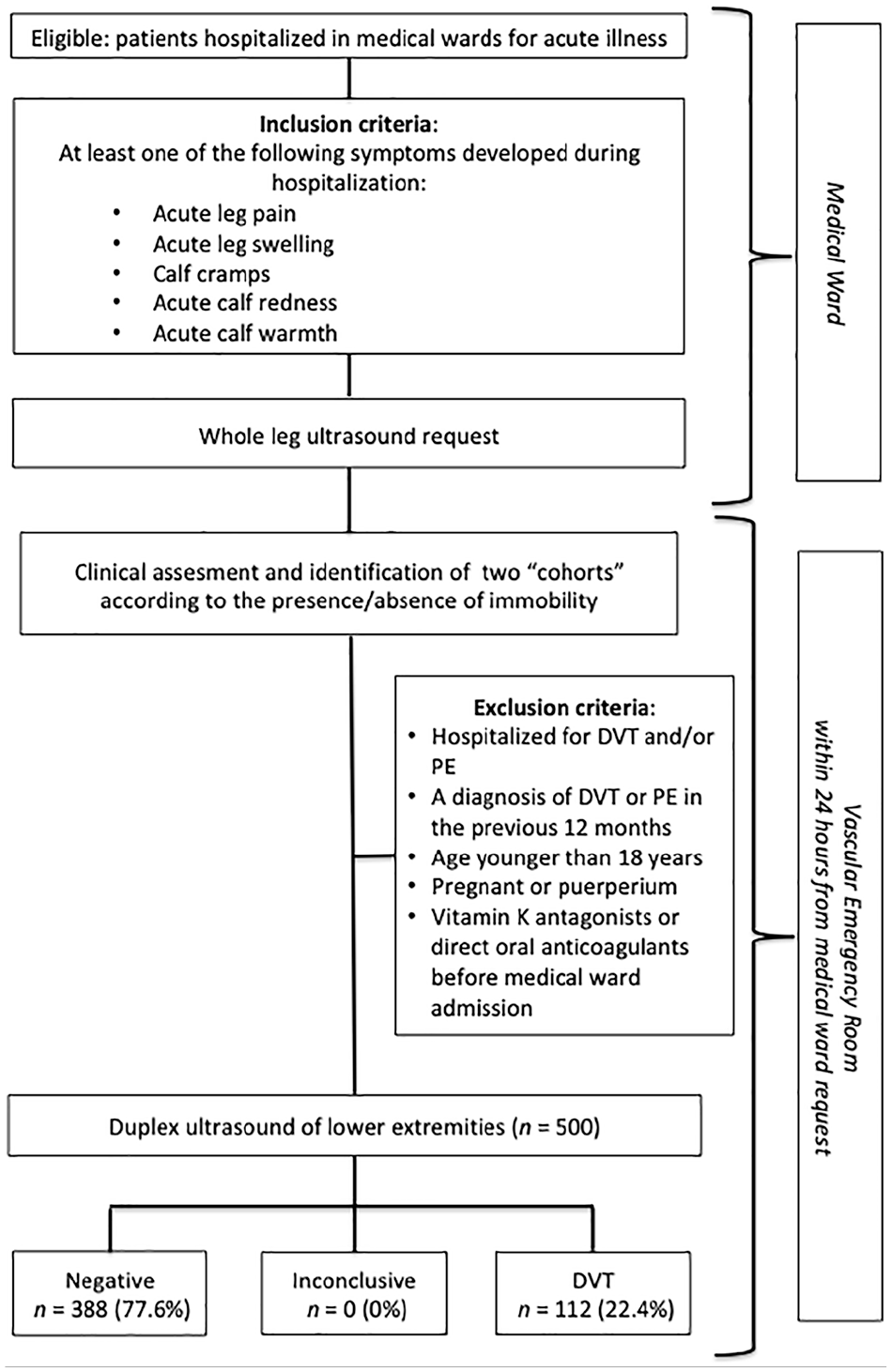
Study flow chart.
Pharmacologic prophylaxis was defined as the use of subcutaneous heparin calcium, 5000 U, two or three times daily, or subcutaneous enoxaparin sodium, 40 mg/day, or subcutaneous fondaparinux, 1.5/2.5 mg/day, between the time of hospital admission and DUS. Mechanical prophylaxis was defined as the use of anti-embolism stockings or intermittent pneumatic compression. At the time of admission, the physician in charge decided whether patients needed prophylaxis and the type of prophylaxis according to his clinical judgement. The patients enrolled in the present study were considered to have: (i) acute respiratory failure if they were admitted to the medical ward for acute hypoxemia due to lung failure; (ii) acute heart failure if they were admitted to the medical ward for rapid onset or worsening of symptoms and/or signs of heart failure as a first occurrence or as a consequence of acute decompensation of chronic heart failure.
The study was approved by the local Ethics Committee. All patients provided informed consent. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Whole leg ultrasonography investigation
In our academic hospital, hospitalized patients with clinical suspicion of DVT proceed directly to DUS within 24 h from the request. Board-certified vascular medicine physicians performed DUS of both lower extremities with an EnVisor C HD (Philips Medical System S.p.A, Monza, Italy) using a standardized examination protocol. 14 The iliac, femoral, and popliteal veins were examined first, then calf veins were evaluated with the patient seated and their legs vertical. Calf veins were studied using various views: anterior-medial, posterior, and posterior-lateral. The following veins were scanned in the transverse plane over their entire length: posterior tibial and fibular (axial veins), medial and lateral gastrocnemius, and soleal veins (muscular veins). DVT diagnosis was confirmed in case of presence of endoluminal material combined with lack of compression of the vein. IDDVT was defined as thrombosis confined to the infra-popliteal veins of the lower limbs (or calf deep vein thrombosis), whereas thrombosis that involved the popliteal vein and/or veins above was defined as proximal DVT.
Statistical analysis
Analysis was carried out using IBM SPSS (version 21; IBM Corp., Armonk, NY, USA). Relationships between variables were assessed using Pearson correlation for continuous variables and chi-squared or Fisher’s exact tests for categorical variables. Student’s t-test was used to compare means among groups for normally distributed variables. Multinomial logistic regression analysis was used to compare the frequency of inpatients that reached the endpoint according to the use of pharmacologic prophylaxis and the presence of immobility. The associations between clinical characteristics of the study population and the endpoint of the study were tested with univariate analysis followed by multivariate analysis, being the effect of the various variables on the endpoint estimated from multivariate Cox’s proportional hazard models. A parsimony model with predictors associated with a p-value less than 0.1 was presented to improve precision and avoid over-fitting. For the time-to-first-event analysis, cumulative endpoint curves were estimated with the Kaplan–Meier procedure and survival curves were tested by the log-rank test. Categorical variables were expressed as frequency and percentage; continuous variables were expressed as mean ± SD. The significance level was set at < 0.05.
The frequency for lower limb DVT (both proximal and distal) in acutely ill medical inpatients with suspected DVT without immobility was assumed to be 0.15. A sample size of 225 for each group (i.e. a total sample size of 450, assuming equal group sizes) was calculated, after applying continuity correction, to achieve a power of 80% for detecting a difference in proportions of 0.15 between the two groups (test – reference group) at a two-sided p-value of 0.05 (OpenEpi, version 3.01; www.openepi.com/).
Results
Figure 1 shows the study flow chart. Table 1 summarizes the characteristics of 500 consecutive acutely ill medical inpatients enrolled with suspected lower limb DVT during the study period. The most frequent risk factors for thrombosis were immobility (50.4%), cancer (22.4%), minor trauma at symptomatic leg within 1 month (14.4%), and previous VTE (14.0%). Pharmacologic prophylaxis was used in 279 (55.8%) patients: 236 patients were on enoxaparin, 41 patients were on fondaparinux, and two patients were on calcium heparin. Mechanical prophylaxis was used in 40 (8.0%) patients. Patients were divided into two groups as defined in the Methods section: patients with (n = 252) and patients without (n = 248) immobility within the time of DVT suspicion. The characteristics of these two groups with comorbidities, prophylaxis use, and presence of DVT risk factors are reported in Table 2. Patients with immobility were older than patients without immobility (82.6 ± 10.3 vs 73.6 ± 14.2, p = 0.0001); there were more female inpatients with immobility versus those without (63.9% vs 54.8%, p = 0.045). Comorbidities such as stroke (17.9% vs 4.5%, p = 0.0001) and respiratory failure (23.0% vs 15.7%, p = 0.042) were more frequent in patients with immobility versus those without, whereas cancer was less prevalent in patients with immobility versus those without (14.7% vs 30.2%, p = 0.001). As shown in Table 2, the percentage of subjects receiving pharmacologic prophylaxis was higher in patients with immobility than in those without (63.9% vs 47.6%, p = 0.0001). The suspicion of DVT arose after 5.31 ± 5.07 days from admission in medical ward inpatients with immobility and after 4.05 ± 4.45 days in patients without immobility (p = 0.003). DUS was performed on the same day if the request was before 14:00, otherwise the morning after. The prevalence of all DVTs (proximal and IDDVT) was higher in the immobility group than in the group without immobility (29.8% vs 14.9%, p = 0.0001): the estimated DVT risk was twofold higher among patients suspected with DVT with immobility than in those without (odds ratio (OR) 2.42, 95% CI: 1.55–3.76, p = 0.0001). There were 36 (14.3%) proximal DVTs and 39 (15.5%) IDDVTs in patients suspected of DVT with immobility, while there were 11 (4.4%) proximal DVTs and 26 (10.5%) IDDVTs in those without immobility. When only proximal DVTs were considered, the risk was three times higher among patients with immobility than in those without (OR 3.59, 95% CI: 1.78–7.23, p = 0.0001), whereas the risk of IDDVT was similar between the two groups (OR 1.56, 95% CI: 0.92–2.66, p = 0.111).
Characteristics of the study population (n = 500).

Data are presented as number (percentage) of patients unless otherwise indicated.
Days from admission to the medical ward when suspicion of DVT arose (whole leg DUS was performed on the same day if the request was before 14:00, otherwise the morning after).
use of subcutaneous heparin calcium, 5000 IU, two or three times daily, or subcutaneous enoxaparin sodium, 40 mg/day, or subcutaneous fondaparinux, 1.5/2.5 mg/day.
BMI, body mass index; DUS, duplex ultrasound; DVT, deep vein thrombosis; HRT, hormone replacement therapy; VTE, venous thromboembolism.
Characteristic of patients according to the presence or absence of immobility.

Statistical analysis was performed by chi-squared test for categorical variables and Student’s t-test for continuous variables.
Days from admission to the medical ward when suspicion of DVT arose (whole leg DUS was performed the same day if the request was before 14:00, otherwise the morning after).
use of subcutaneous heparin calcium, 5000 IU, two or three times daily, or subcutaneous enoxaparin sodium, 40 mg/day, or subcutaneous fondaparinux, 1.5/2.5 mg/day.
presence of immobility defined as total bed rest or sedentary without bathroom privileges; −, absence of immobility; BMI, body mass index; DUS, duplex ultrasound; VTE, venous thromboembolism.
Among the 279 subjects receiving pharmacologic prophylaxis, there were 22 (13.7%) proximal DVT and 22 (13.7%) IDDVT inpatients suspected with DVT with immobility, while there were four (3.4%) proximal DVTs and 11 (9.3%) IDDVTs in those without immobility (Table 3). Among the 221 subjects not receiving pharmacologic prophylaxis, there were 14 (15.4%) proximal DVT and 17 (18.7%) IDDVT inpatients with immobility, while there were seven (5.4%) proximal DVTs and 15 (11.5%) IDDVTs in those without immobility (Table 3).
Number of patients with lower extremity vein thrombosis at DUS according to the presence or absence of immobility and of pharmacological prophylaxis.

Data are presented as number (percentage).
Statistical analysis was performed by multinomial logistic regression analysis.
Immobility +, presence of immobility defined as total bed rest or sedentary without bathroom privileges; Immobility −, absence of immobility; Prophylaxis +, use of subcutaneous heparin calcium, 5000 IU, two or three times daily, or subcutaneous enoxaparin sodium, 40 mg/day, or subcutaneous fondaparinux, 1.5/2.5 mg/day; Prophylaxis −, absence of prophylaxis.
p = 0.004 vs patients with Immobility– and Prophylaxis–; bp = 0.037 vs patients with Immobility– and Prophylaxis–.
DUS, whole leg duplex ultrasound; DUS –, absence of lower extremity vein thrombosis at whole leg duplex ultrasound; DVT, deep vein thrombosis; IDDVT, isolated distal DVT.
According to Cox regression analysis, only immobility (hazard ratio (HR) 1.62, 95% CI: 1.04–2.53, p = 0.034) and the use of prophylaxis (HR 0.57, 95% CI: 0.38–0.85, p = 0.005) were associated with the endpoint (total DVTs), whereas age, sex, cancer, respiratory failure, and stroke were not (Table 4). The Kaplan–Meier estimated curves of probability for DVT in patients suspected of DVT with and without immobility according to the days from admission to the medical ward are reported in Figure 2, which shows that patients suspected of DVT with immobility had a higher risk of DVT than those without immobility (p = 0.018). The risk of DVT increased in parallel with the length of hospital stay but in the first 3 days from hospitalization the frequency of DVT was similar in patients with and without immobility: the cumulative estimated risk of DVT in patients suspected of DVT without immobility was 0.15 ± 0.02, 0.18 ± 0.03, 0.22 ± 0.04, 0.22 ± 0.04, 0.28 ± 0.06, and 0.53 ± 0.11 after 2, 4, 6, 8, 10, and 12 days from admission to the medical ward, whereas it was 0.16 ± 0.02, 0.26 ± 0.03, 0.31 ± 0.04, 0.42 ± 0.05, 0.43 ± 0.05, and 0.79 ± 0.06 in those with immobility. When only proximal DVTs were considered, the same trend was observed (Figure 2).
Factors associated with the presence of DVT in acutely ill medical inpatients suspected of DVT according to days from admission to the medical ward at Cox regression analysis.
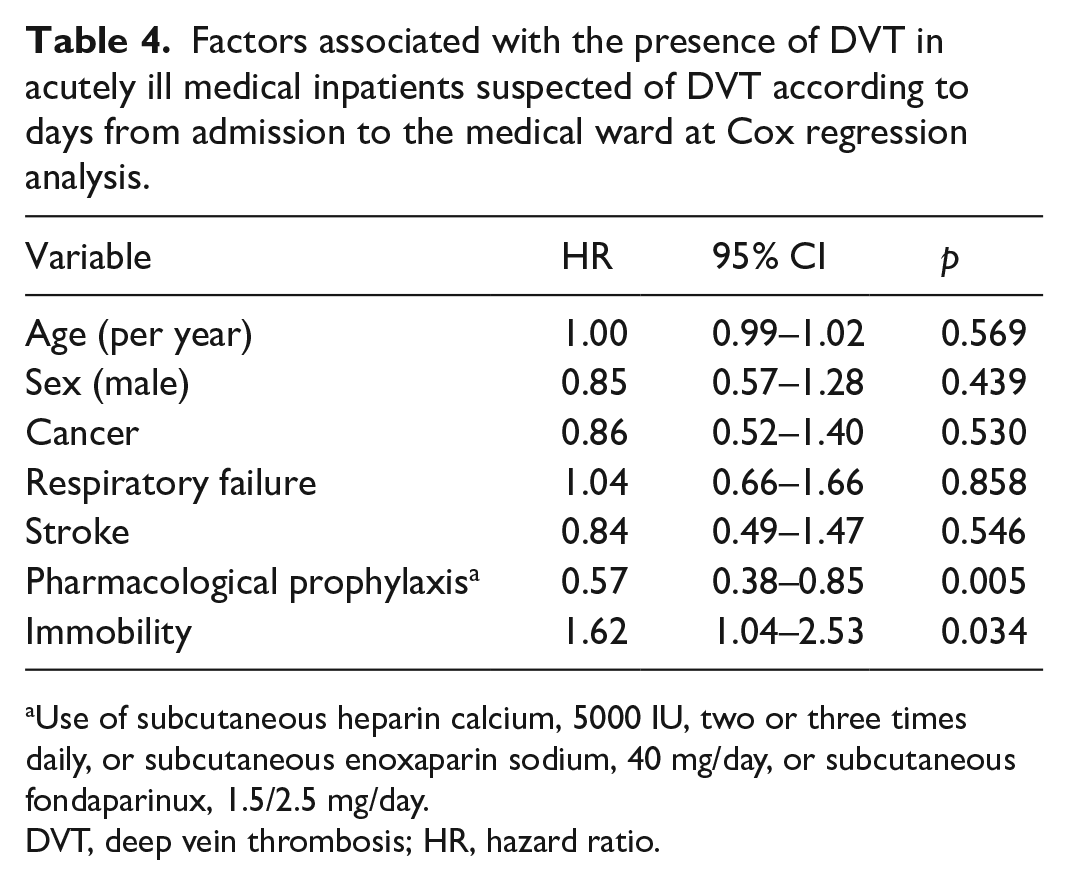
Use of subcutaneous heparin calcium, 5000 IU, two or three times daily, or subcutaneous enoxaparin sodium, 40 mg/day, or subcutaneous fondaparinux, 1.5/2.5 mg/day.
DVT, deep vein thrombosis; HR, hazard ratio.
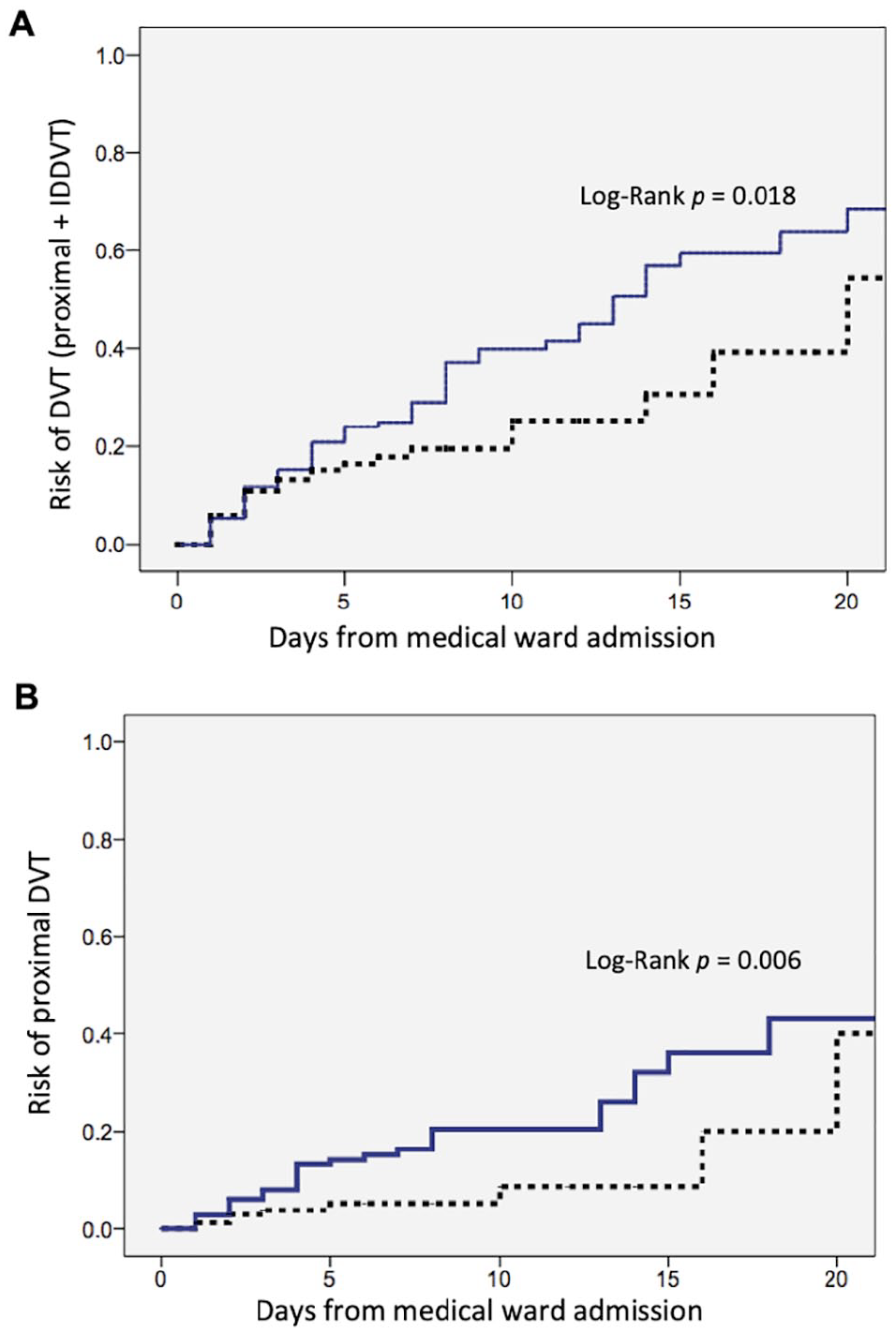
Estimated cumulative probability of all DVTs (proximal and IDDVT) (A) and of proximal DVT (B) in acutely ill medical inpatients suspected of DVT with immobility (solid line) and without (dotted line) according to the time when whole leg ultrasound was performed (day 0: admission to the medical ward).
Discussion
Our data show that immobility is a risk factor for DVT in acutely ill medical inpatients and this association is stronger with proximal DVT rather than IDDVT. Immobility for at least 3 days has a significant effect on DVT risk.
Immobility is a well-recognized risk factor for VTE in surgical patients, but it is also frequent in medically ill inpatients. In our series, immobility was present in half of our study population, suggesting that immobility is one of the most frequent DVT risk factors in the setting of medical wards. In line with our results, previous studies showed that frequency of immobility among medical ill patients might reach 50%.10,15 Medical patients tend to have a history of reduced mobility because of comorbidities that can worsen due to the acute disease that prompted their admission. As a proof of this, comorbidities leading to reduced mobility such as stroke and respiratory failure were more frequent in the immobile group of our population. It is remarkable that the frequency of patients in the immobility group that received DVT prophylaxis, either mechanical or pharmacological, was 73%. This is not surprising given that the mean age was greater than 80 years and 18% of patients had a stroke (i.e., subjects in the immobility group were at high bleeding risk). Moreover, we enrolled patients who were on single or dual antiplatelet therapy and this may constitute a contraindication to pharmacologic prophylaxis, especially concerning older subjects as were those enrolled in our study. Thus, the physician of the medical ward estimated that the risk of bleeding associated with pharmacologic prophylaxis was too high in almost 36% of the immobile patients. Nevertheless, only 10% of immobile patients received mechanical prophylaxis. There are several reasons why mechanical prophylaxis was not employed in all patients with a contraindication to pharmacological prophylaxis. Many patients had a contraindication to mechanical thromboprophylaxis as well, such as acute congestive heart failure, diabetic neuropathy, foot ulcers or other dermatological diseases of the lower extremities. Finally, some patients can refuse or not tolerate mechanical prophylaxis.
All the major clinical trials of VTE prophylaxis in medical inpatients have used different definitions of immobility. 7 As a result, a consistent definition of immobility is lacking in medical inpatients. In some studies, the terms ‘reduced mobility’ or ‘prolonged immobility’ or ‘confined to/remain in bed’ or ‘immobile with bathroom privileges’ were used but not clearly defined. 16 In the IMPROVE VTE risk assessment model validation cohort, 17 the term ‘hospital stay’ and ‘bed rest’ were used interchangeably. In our study, we clearly defined the terms ‘hospital stay’ and ‘immobility’. We dichotomized the concept of immobility by assigning different mobilization levels, as already done in previous clinical randomized trials. In the ADOPT trial, patients were categorized as moderate (allowed to walk within the hospital room or to the bathroom) or severe (confined to bed or to a chair at the bedside) reductions in mobility. 18 In the EXCLAIM study and its subgroup analyses, reduced mobility was categorized into two levels: level 1 immobility (total bed rest or being sedentary without bathroom privileges) or level 2 immobility (total bed rest or being sedentary with bathroom privileges).13,19 In the present study, patients were categorized according to the definition of level 1 immobility of the EXCLAIM trial (i.e., total bed rest or sedentary to a chair at the bedside without bathroom privileges). In other studies, the duration of immobility was specified rather than stating a level or degree of immobility. 16 Immobility has been included in the two most extensively studied risk-assessment models for medical patients: in the empirically derived Padua score, immobility was defined as bed rest with bathroom privileges for at least 3 days, 20 whereas in the IMPROVE score it was defined as confinement to a bed or chair for more than 7 days. 21 We demonstrated that DVT risk correlated with the duration of immobility and was higher from the fourth day of immobility following medical ward admission. Thus, our data support the definition of immobility as bed rest without bathroom privileges for at least 3 days.
Although immobility is an important and highly prevalent risk factor for DVT, few studies investigated the role of immobility in acutely ill medical inpatients. A multicenter case–control study with hospitalized patients older than 65 years found that restriction of mobility was an independent risk factor for VTE (OR: 1.73-5.64), 10 whereas another case–control study found that hospitalization and immobility were associated with a greater than sevenfold increased risk of venous thrombosis. 22 A meta-analysis that included nonsurgical patients showed that immobility was a risk factor for VTE with relative risk estimates ranging from 1.46 to 2.77, 9 but the DVT risk was not calculated. In fact, such meta-analysis included only three cohort studies that explored the incidence of proximal DVT but not IDDVT. Our study is the first cohort study exploring the effects of immobility per se on both proximal DVT and IDDVT risk in acutely ill medical inpatients. It has been suggested that immobility is a risk factor for both IDDVT and proximal DVT. 23 In the RIETE and in the OPTIMEV registry, the frequency of bed confinement was the same in patients with proximal DVT and in those with IDDVT.23,24 On the contrary, our study suggests that immobility is a risk factor for proximal DVT but a mild risk factor for IDDVT in medically ill patients. Such a difference may be ascribed to the different population included in the two registries: the majority of subjects were outpatients – in the RIETE registry, subjects were 10 years younger and in the OPTIMEV registry, subjects were 15 years younger than those included in our study.
Study strengths and limitations
The strengths of our study are the cohort design, the large study sample, and the analysis according to prophylaxis utilization. Immobility increased DVT risk in subjects either with or without thromboprophylaxis and it was still associated with DVT risk after Cox regression analysis. Since we did not want to detect DVTs acquired before hospitalization, we excluded patients who had DVT symptoms before hospital admission. Future studies should clearly define relationships between immobility, VTE risk, and prophylaxis for medical inpatients, and these studies would benefit from having an objective definition of immobility. However, there is no acceptable consensus on the definition of immobility. Given that DVT risk correlates with the duration of immobility and is higher from the fourth day of immobility, we suggest the use of the definition of immobility as bed rest without bathroom privileges for at least 3 days.
Some limitations of the present study should be acknowledged. We explored only the DVT risk in acutely ill medical inpatients, while we have no data on PE risk. We did not follow-up patients with negative whole leg ultrasonography examination, but several studies have shown that anticoagulant therapy can be safely withheld after negative complete compression ultrasound without further testing25,26 also in inpatients. 27 Since whole leg ultrasound was performed only in symptomatic patients, our study does not provide information on the prevalence of asymptomatic DVT in this setting. We do not know the proportion of patients with a suspicion of DVT among immobile patients admitted to the medical wards and no conclusion can be drawn on the DVT prevalence in this setting. We have no data on the mobility status before admission to the medical wards. The study was conducted in a single academic institution and may not be representative of the population in different types of hospitals.
Conclusion
Immobility defined as total bed rest or being sedentary without bathroom privileges was associated with a twofold increased risk of DVT in acutely ill medical inpatients. The relationship between immobility and thrombosis in acutely ill medical inpatients was observed only for proximal DVT, but not for IDDVT. The risk of DVT correlated with hospital length of stay and it became relevant after 3 days of immobility.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of data
The datasets used and analyzed during the current study are available from the corresponding author upon request.