
Abstract
This study evaluated the incidence, predictors, and impact of bleeding requiring hospitalization following successful endovascular therapy (EVT) for peripheral artery disease. Platelet inhibition after EVT reduces the risk of major adverse limb events but increases the risk of bleeding. The incidence of post-discharge bleeding after EVT, its independent predictors, and its prognostic importance in clinical practice have not been fully addressed. We evaluated 779 consecutive patients who underwent EVT. We found that 77 patients (9.9%) were hospitalized for major bleeding during follow-up after EVT (median 39 months, range 22–66 months), with almost half (48.1%) of the bleeding categorized as gastrointestinal bleeding. Significant predictors of post-discharge bleeding were hemodialysis (hazard ratio (HR), 3.12; 95% CI: 1.93 to 5.05; p < 0.001) and dual antiplatelet therapy (DAPT) use (HR, 1.87; 95% CI: 1.03 to 3.41; p = 0.041). During follow-up, the all-cause mortality-free survival rate was significantly worse in patients who had experienced major bleeding than in those who had not (log-rank test χ2 = 54.6; p < 0.001). Cox proportional hazards analysis showed that major bleeding (HR, 2.78; 95% CI: 1.90 to 4.06; p < 0.001) was an independent predictor of all-cause death after EVT. Hospitalization for post-discharge bleeding after EVT is associated with a substantially increased risk of death, even after successful EVT. We concluded that patients’ predicted bleeding risk should be considered when selecting patients likely to benefit from EVT, and that the risk should be considered especially thoroughly in hemodialysis patients.
Introduction
Recent advances in antithrombic and mechanical therapy have resulted in significant improvements in the clinical outcome of patients with peripheral artery disease (PAD).1,2 However, the reduction in risk of fatal and nonfatal ischemic events associated with advancements in technology has been paralleled by an increase in the incidence of bleeding events. Major bleeding is currently the most important nonischemic side effect of therapy for patients with PAD.
There are many retrospective and registry data indicating that major bleeding is associated with mortality in patients with ischemic heart disease undergoing percutaneous coronary intervention (PCI), emphasizing the potential importance of minimizing bleeding, as well as ischemic events.3–7 However, there are no data available describing the incidence, risk factors, and outcomes of major bleeding events in patients with PAD after endovascular therapy (EVT). The identification of demographic, clinical, and treatment characteristics associated with increased risk of bleeding after EVT may help us find ways of decreasing the frequency of major bleeding both through clinical interventions and appropriate patient selection. Therefore, we sought to evaluate the incidence, predictors, and impact of clinically significant bleeding occurring after hospital discharge following successful EVT for PAD.
Methods
Study population
This retrospective study included 779 consecutive patients with Rutherford category 8 2 to 6 ischemia who underwent EVT for PAD between January 2012 and April 2017 at Yokosuka Kyosai Hospital, Kanagawa, Japan. All patients successfully treated with EVT and who were adequately loaded with aspirin and clopidogrel were eligible for enrollment, regardless of clinical presentation or lesion complexity. The only major exclusion criterion was the occurrence of mortality during hospitalization because our goal was to examine post-discharge bleeding (PDB). After EVT, patients were treated with aspirin indefinitely, and clopidogrel was recommended for at least 6 months. All other treatments were per standard of care. For patients who had multiple EVT procedures during the study period, the first EVT was considered the index procedure. The hospital’s ethics committee approved the study protocol, and the study was performed in accordance with the Declaration of Helsinki. Every patient provided written informed consent. For the present study, patients were grouped by whether PDB had occurred or not during the follow-up period.
Study objectives and definitions
The objectives of the present study were to: (1) determine the incidence of PDB after EVT for PAD; (2) identify risk factors associated with the occurrence of PDB; and (3) evaluate the time-dependent, multivariable adjusted effect of PDB on mortality after the index procedure.
PDB was defined as Bleeding Academic Research Consortium (BARC) type 3 bleeding or greater by hemoglobin decrease > 3 g/dL, overt bleeding requiring transfusion, or intracranial/intraocular bleeding, as in a previous study. 9 The following pre-specified categories were used to group the sites of bleeding: gastrointestinal, neurologic, pulmonary, genitourinary, peripheral, retroperitoneal, and other. The endpoint evaluated in the present study was all-cause mortality.
Statistical analysis
Categorical data were expressed as absolute frequencies (percentages) and were compared using the chi-squared or Fisher’s exact test, as appropriate. Continuous variables were expressed as the means ± SD if they were normally distributed and as medians with IQR if they were nonparametric; they were compared using the Student t-test or the Mann–Whitney U test, respectively.
Baseline predictors of PDB were identified using multivariable analysis based on the intent to-treat population. Baseline variables assessed in the logistic regression model included demographic features, clinical history, clinical and laboratory parameters, and medications. Multivariable analysis of predictors of PDB was then performed. The relationship between PDB and mortality was assessed using multivariable logistic regression modeling. Variables in this model included demographic features, clinical history, and clinical and laboratory parameters. All variables achieving p < 0.1 in the univariate analysis were entered into a multivariate Cox regression model. A p < 0.05 indicated statistical significance for all analyses. Data from the models are presented as hazard ratios (HR) with CIs. Data were analyzed using IBM SPSS software, version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Characteristics of patients with and without hospitalization for bleeding
Among the 779 patients enrolled in the study who underwent EVT for symptomatic PAD, no patients died during hospitalization for EVT, resulting in all patients being included in the current analysis. Median follow-up was 39 months (22–66 months). During follow-up, 77 patients (9.9%) had PDB events. The mean age of our cohort was 72.7 years, 29.3% were women, and 27.6% had critical limb ischemia (CLI) (Table 1). Roughly 40% of patients had previous EVT. Baseline clinical characteristics associated with belonging to the major bleeding group were history of hypertension, coronary artery disease, myocardial infarction, and hemodialysis. Patients who had bleeding episodes also were more likely to be prescribed aspirin, either of ticlopidine or clopidogrel, cilostazol, dual antiplatelet therapy (DAPT), and β-blockers (Table 1).
Patient characteristics.
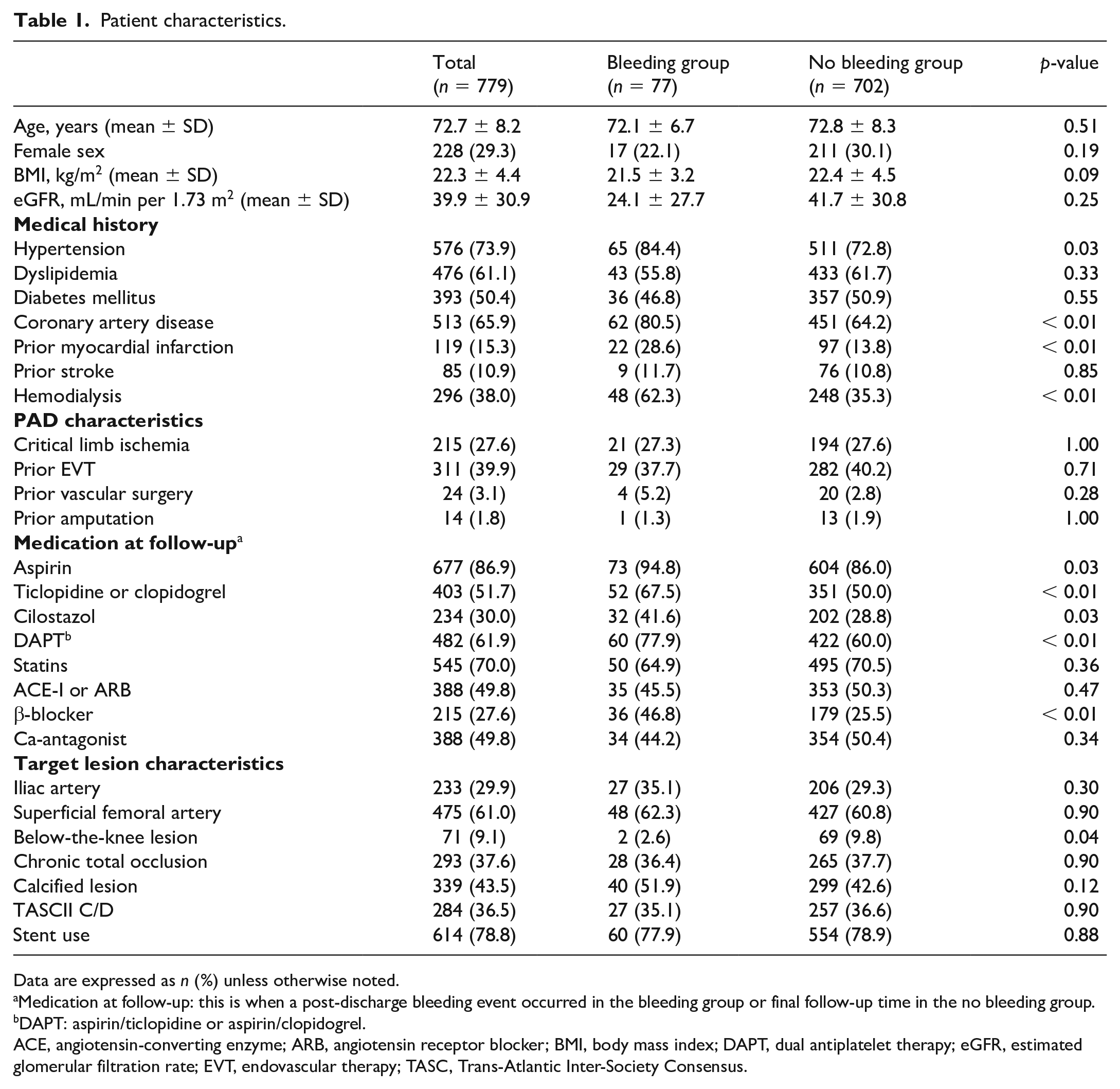
Data are expressed as n (%) unless otherwise noted.
Medication at follow-up: this is when a post-discharge bleeding event occurred in the bleeding group or final follow-up time in the no bleeding group.
DAPT: aspirin/ticlopidine or aspirin/clopidogrel.
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BMI, body mass index; DAPT, dual antiplatelet therapy; eGFR, estimated glomerular filtration rate; EVT, endovascular therapy; TASC, Trans-Atlantic Inter-Society Consensus.
Sites of post-discharge bleeding
The most common bleeding site was gastrointestinal (48.1%) followed by neurologic (14.3%). Peripheral bleeding and retroperitoneal bleeding accounted for 6.5% of bleeding episodes, pulmonary for 5.2%, while genitourinary bleeding was observed in 3.9% (Figure 1).
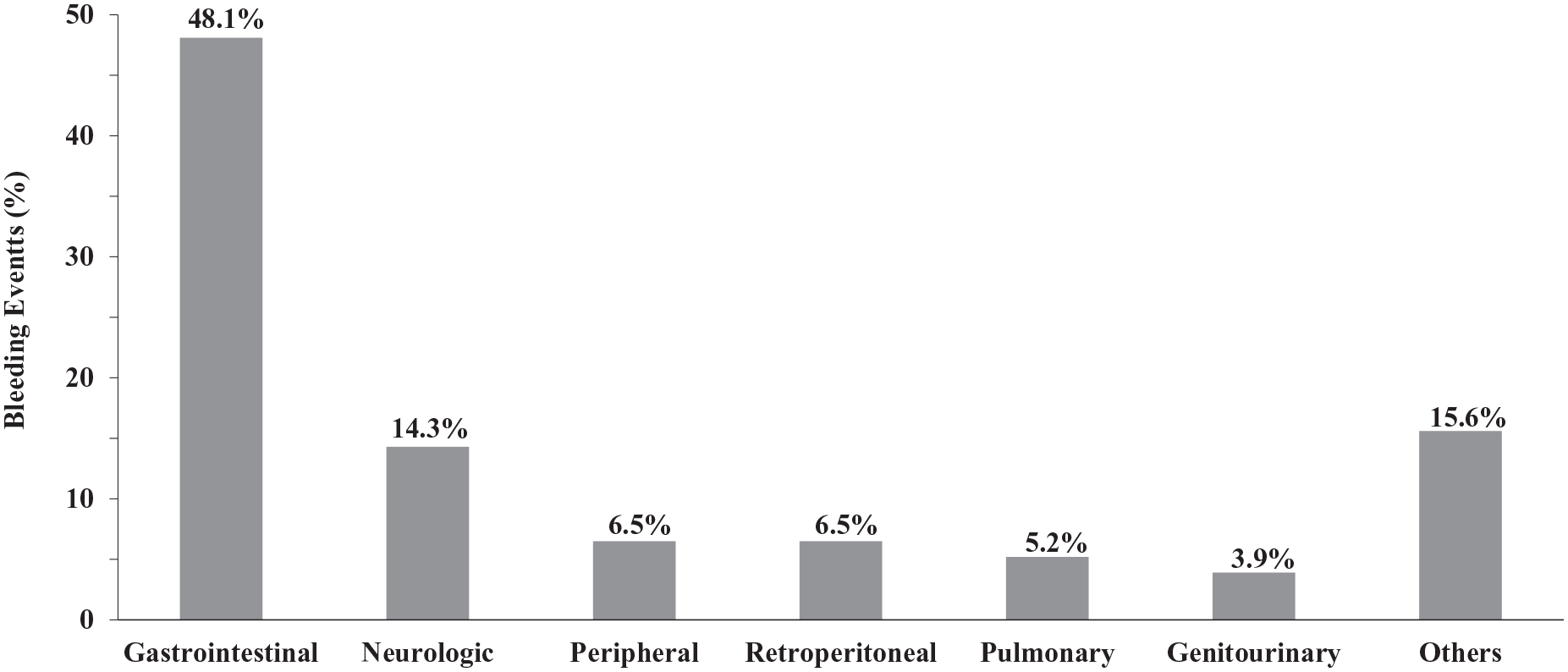
Site of post-discharge bleeding (PDB). Among 77 patients with major bleeding and identified source, gastrointestinal bleeding was the predominant cause of PDB.
Independent predictors associated with late major bleeding after endovascular therapy (EVT)
Factors associated with increased hazard of PDB are shown in Table 2. Out of five factors with p < 0.1 in univariate analysis, two factors remained as independent predictors in multivariate analysis: hemodialysis and DAPT use. Among these factors, hemodialysis was associated with the greatest hazard of PDB, with a 3.12-fold increased risk (95% CI: 1.93–5.05; p < 0.001), followed by DAPT use (HR 1.87; 95% CI: 1.03–3.41; p = 0.041).
Analysis of factors related to major bleeding.
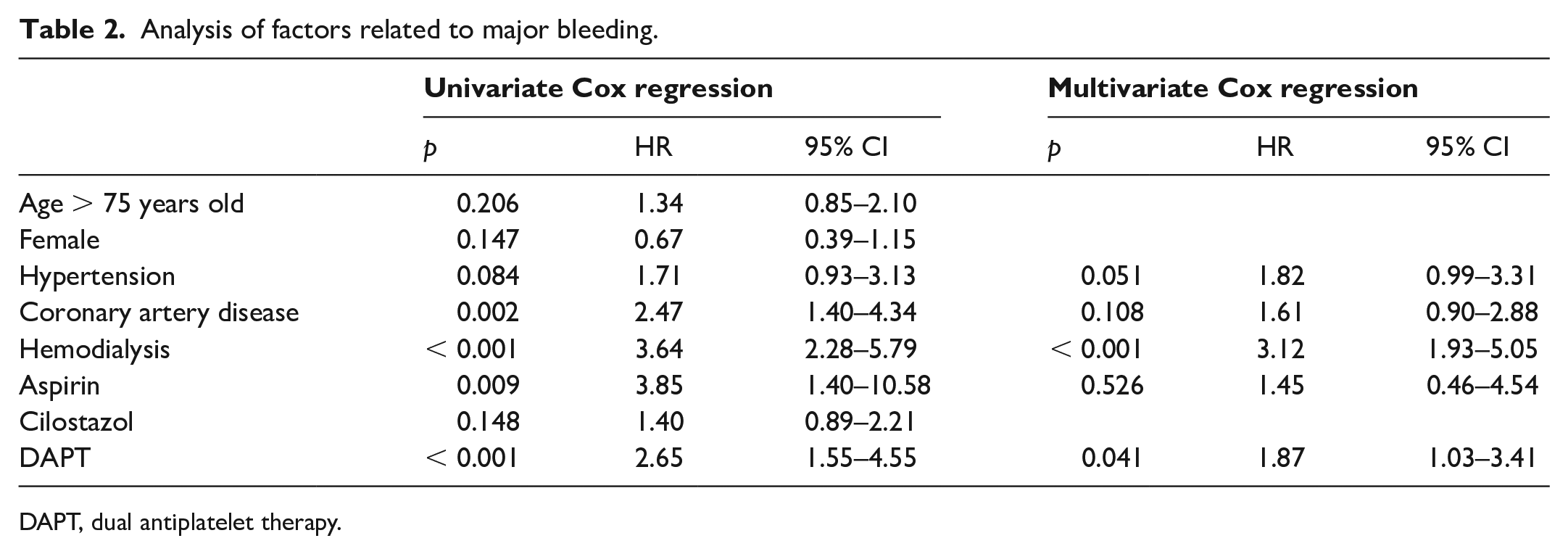
DAPT, dual antiplatelet therapy.
Relation between post-discharge bleeding and mortality after EVT
During follow-up, the all-cause mortality rate was significantly worse in patients with PDB compared to patients without PDB (57.1% vs 18.2%, p < 0.001) (Figure 2).
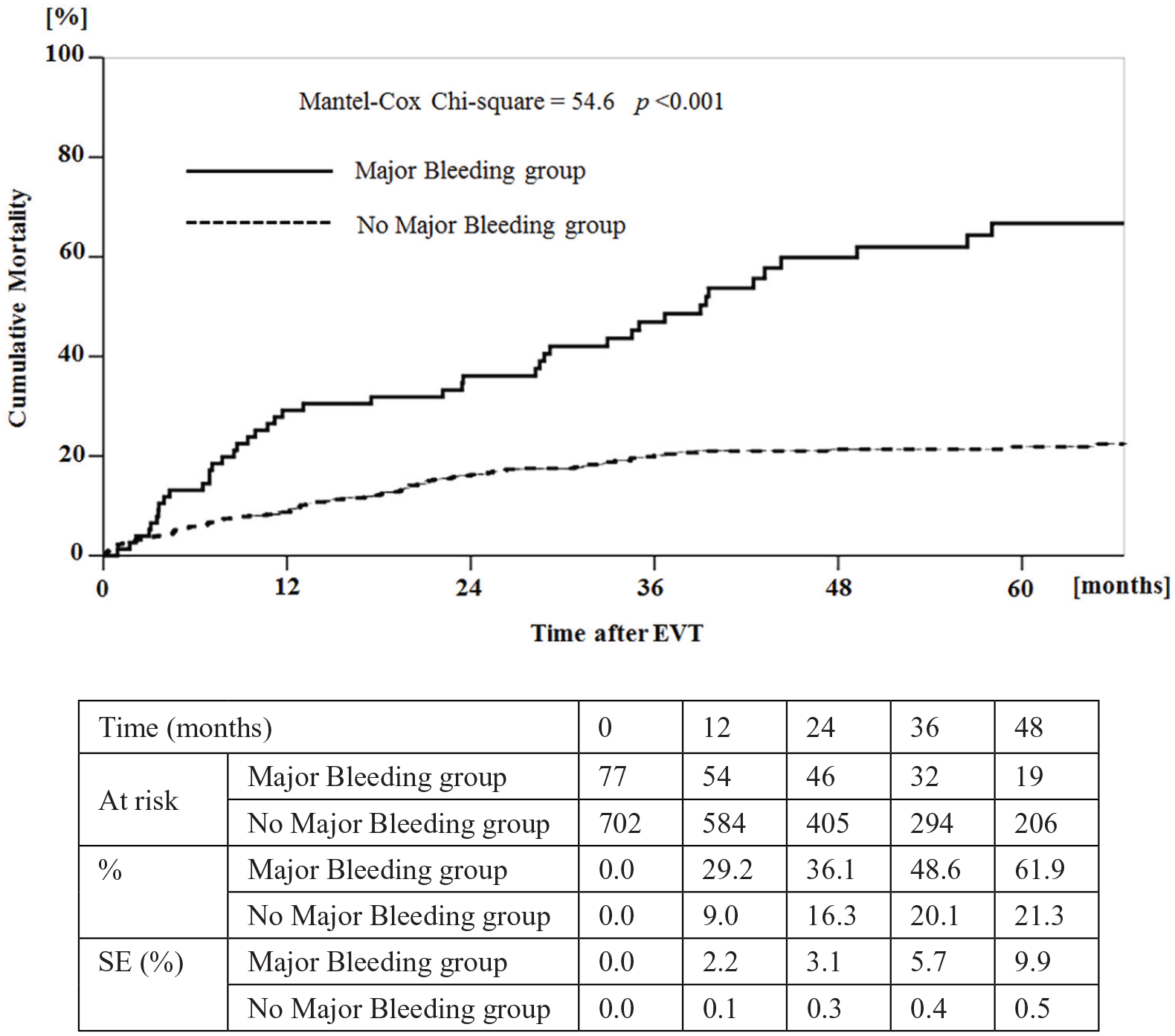
Cumulative risk of all-cause death in patients with and without major bleeding. Cumulative probability of all-cause death was significantly different between the two groups.
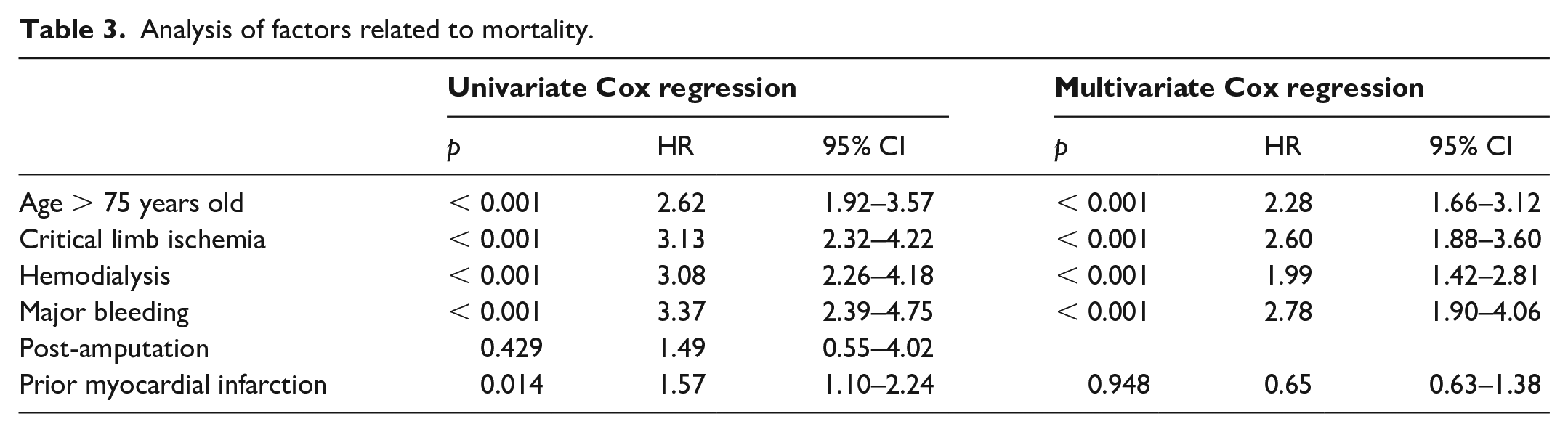
Multivariate analysis demonstrated four independent predictors of mortality: PDB, critical limb ischemia, age > 75 years, and hemodialysis. PDB was the strongest predictor of mortality, with a HR of 2.78 (95% CI: 1.90 to 4.06; p < 0.001) (Table 3). Whether or not blood had been transfused for PDB did not affect mortality (not shown).
Analysis of factors related to mortality.
Discussion
This is the first study to evaluate the incidence, predictors, and impact on prognosis of PDB events after EVT for PAD patients. The major results of this analysis were: (1) PDB events occurred in 9.9% of PAD patients after EVT during follow-up (median 39 months, range 22–66 months) and was associated with strikingly higher rates of mortality; (2) several factors were associated with an increased risk of PDB, but only hemodialysis and DAPT therapy were independent predictors of PDB after EVT in multivariate analysis.
In our study, the distribution of bleeding sites in our overall patient population was similar to that of a published study of patients undergoing PCI. 10 Almost half (48.1%) of these hospitalizations for late major bleeding after EVT were due to gastrointestinal bleeding. Importantly, PDB was associated with a threefold increased risk hazard of all-cause mortality after EVT. Several independent predictors of PDB were identified that may allow physicians to identify patients at high risk for PDB. Most notably, physicians should be aware that hemodialysis was the strongest predictor of PDB and led to a greater than threefold increased hazard of PDB after EVT.
A previous study showed that 2.5% of 22,798 patients who underwent PCI were hospitalized for late major bleeding within a year, with 56% of bleeding episodes due to gastrointestinal bleeding. 11 Kolte et al. found that 20.4% of patients hospitalized for CLI and undergoing revascularization were readmitted within 30 days, and bleeding was responsible for 4.8% of 30-day readmissions in a Nationwide Readmissions Database analysis of 60,998 patients. 12 Our higher bleeding rate of 9.9% during the median follow-up of 39 months is likely a reflection of our real-world EVT cohort compared to patients typically enrolled in PCI trials. Our patients had high rates of hypertension, dyslipidemia, diabetes mellitus, and multiple comorbidities, including end-stage renal disease requiring hemodialysis. Previous studies included many chronic kidney disease patients, but not so many hemodialysis patients.11,12 The high comorbidity rate may explain the higher bleeding episode rate for the study participants.
To the best of our knowledge, this is the first study that has examined the strong prognostic importance of PDB after EVT for all-cause mortality in routine clinical practice. We lacked data to categorize causes of death and were unable to identify mechanisms underlying these adverse events. Although a greater burden of comorbidities among patients who had bleeding may have played a role, the association of late major bleeding with all-cause mortality remained significant after adjustment for comorbidities. We believe the mechanism behind the high rates of mortality in our patients who experienced bleeding to be multifactorial. First, these patients with PDB had a more unfavorable baseline clinical profile that included higher prevalence of hypertension, coronary artery disease, and chronic renal insufficiency, all factors known to worsen the prognosis of patients with atherosclerotic diseases.13–16 Second, the bleeding itself is associated with morbidity and mortality by means of its location and the extent of blood loss. 17 Bleeding-related hemodynamic instability may provoke or aggravate ischemia, resulting in adverse outcomes. Third, major bleeding is a well-known cause of premature cessation of antiplatelet therapy, which poses additional risk for ischemic outcomes in patients with atherosclerotic diseases.18–23
Given the strong association of late major bleeding with poor adverse outcomes, an improved understanding of the determinants of late major bleeding may promote strategies to reduce bleeding and may lead to improved clinical outcomes of PAD after EVT. We found hemodialysis and DAPT therapy to be strongly associated with the adjusted hazard for late major bleeding after EVT. A shorter DAPT duration may result in improved survival compared to prolonged DAPT, presumably by reducing the late major bleeding events after EVT. Nonetheless, some patients at high risk for thrombotic events, such as those with prior myocardial infarction, might still benefit from more potent and prolonged DAPT.24,25 Antiplatelet therapy is generally recommended for all patients with PAD to improve event-free survival, both as a primary and secondary prevention measure upon EVT.26–30 The available data regarding safety and efficacy of different antiplatelet agents in the treatment of PAD are very heterogeneous. Despite the increasing number of patients receiving endovascular stents due to progressive PAD, knowledge regarding post-interventional management, and more specifically DAPT after EVT, is still markedly limited. The DAPT routinely used for PAD treatment was mainly extrapolated from data on DAPT after coronary artery intervention.31,32 Choosing between shorter versus longer DAPT requires balancing the risk of future atherothrombotic events and major bleeding, and large-scale randomized trials are required to determine the optimal duration of DAPT therapy after EVT for PAD patients.
Study limitations
Our study has several limitations. First, bleeding events were not independently adjudicated by a blinded clinical events committee, introducing potential reporting bias. Second, we were unable to identify the site of bleeding in some patients in this retrospective study. Third, information on other drugs known to increase the risk of major bleeding, including anticoagulant drugs (anticoagulant drugs are not recommended or sometimes contraindicated for hemodialysis patients according to the Japanese Society for Dialysis Therapy), nonsteroidal anti-inflammatory drugs, corticosteroids, and spironolactone, was not collected. Our analysis also lacks data on treatment with proton pump inhibitors. Finally, although we found a strong association between late major bleeding and adverse clinical outcomes after EVT, our study cannot definitively prove a causal relationship given the complex interplay among comorbidities, late major bleeding, and adverse clinical outcomes.
Conclusions
In conclusion, in this population-based cohort of PAD patients who underwent EVT, hospitalization for PDB after EVT was associated with a substantially increased risk of all-cause mortality in the long term. Clinicians should identify patients at risk for PDB after EVT and implement strategies and appropriate risk-based patient selection to reduce the overall risk of PDB to improve patient outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.