
Abstract

Keywords
Peripheral artery disease (PAD) affects more than 8–10 million Americans and 200 million worldwide. 1 PAD has a dramatic impact on quality of life and greatly increases the risk of cardiovascular mortality. In its most advanced form, PAD is known as critical limb ischemia (CLI) or chronic limb-threatening ischemia (CLTI). Patients with CLTI are at high risk for major amputation and death with a 1-year mortality of nearly 25%. 2 In addition, it has been reported that these patients have a quality of life worse than cancer, chronic heart disease, and chronic kidney disease. 3 Few other conditions harbor such a dismal prognosis.
PAD remains underdiagnosed and undertreated. As an example, the PARTNERS study reported that nearly 30% of patients older than 70 years of age or between 50 and 69 years of age with diabetes or history of smoking have PAD. 4 Unfortunately, despite this alarmingly high prevalence, half of the primary care providers in that study were unaware of this diagnosis in their patients, emphasizing the ongoing need to raise PAD awareness in health care specialists. Though guideline-directed therapy has been shown to decrease amputations and cardiovascular death, 5 many patients with PAD fail to receive optimal guideline-directed medical therapy.6,7 The situation is even more dire in patients with CLTI, a group characterized by high rates of cardiovascular comorbidities, complex multivessel PAD, and limb-threatening wounds.
Disparities in sex, race, and socioeconomic status compound the complexities surrounding PAD care further. Indeed, PAD disparities relating to sex have been well recognized, and were a primary inspiration of the American Heart Association’s 2012 ‘call to action’ to better treat and diagnose PAD in women. 8 Women more often have atypical symptoms, present when they are older and in worse health, have more severe anatomical disease, and are more apt to present with ischemic rest pain or tissue loss compared to men. 9 As such, women are more likely to undergo more proximal (i.e. above the knee (AKA) versus below the knee (BKA)) amputations than men, which has a greater impact on mobility. 10 Women with PAD also have a higher in-patient mortality compared to men, irrespective of disease severity, revascularization technique, age, and co-morbidities. 11 All of these factors likely contribute to the varying treatment of women who present with CLTI. Recently, Mentias and colleagues 12 demonstrated that women presenting with CLTI are less likely to be on guideline-directed medical therapy, including high potency statins, which can adversely impact limb and cardiovascular outcomes. Women in this large cohort also received revascularization less often. Perhaps the most alarming finding of this study was that one-third of CLTI patients in this large cohort underwent major amputation without a diagnostic angiogram or trial of revascularization in the preceding 90 days regardless of sex, underscoring an enormous opportunity for improvement in CLTI care for all patients.
Racial disparities in CLTI care are also well described. In an analysis of over 2 million Medicare patients with PAD, along with diabetes mellitus and renal disease, black race was an independent predictor of lower extremity amputation. 13 This analysis also demonstrated certain geographic differences were present even after adjustment for clinical factors. Additional studies have confirmed that black patients have higher rates of amputation compared to white patients. 14 Black patients with CLTI are also less likely to receive revascularization when compared to white patients and undergo more severe amputation (AKA vs BKA). 15 Some have suggested that these racial disparities are due to socioeconomic issues and access to care. In an elegant study using data from the Veterans Affairs Administration, Arya and colleagues 14 clearly demonstrated that black race significantly increases the risk of amputation within the same socioeconomic stratum compared to white race and has an independent effect on limb loss after controlling for comorbidities, severity of PAD at presentation, and use of medications.
In this issue of Vascular Medicine, Hurst and colleagues 16 elegantly show data from Scotland that CLTI and PAD appear to be highest in socioeconomically disadvantaged areas. This represents a first step in identifying target groups for intervention in that country, especially given its socialized health care system. Disparities in CLTI care are widespread and rampant, and combating them will require multifaceted solutions (Figure 1) at the patient, provider, system, and science level. At the patient and community level, the vascular community must increase and intensify efforts to increase PAD awareness, particularly for populations that are most vulnerable. These efforts are critical to detecting the clinical manifestations of PAD earlier when interventions of all types may be more effective. We also must garner trust in these same vulnerable communities through service and education on a larger scale. On a provider level, we must learn to work together as multidisciplinary teams and not as silos of care. The care of these patients demands the expertise of numerous specialties to optimize patient outcomes on every level. No one specialty provides comprehensive CLTI care. We need to instill this team approach early in training and perhaps even formulate dedicated multidisciplinary CLTI training programs that can help develop evidence-based, protocol-driven CLTI care in an effort to minimize variances and thus optimize patient outcomes. Initiatives aimed at implementing CLTI care teams and assessing their impact are needed. Dedicated educational programs for providers engrossed in CLTI care will ensure that best revascularization practices are employed and that variations in vascular care are minimized. Scientific progress will occur through national registry development with uniform outcomes assessment, the testing of novel technologies for CLTI care, and evaluation of strategies to address disparities in clinical trials. The CLTI population is in dire need; opportunities to help are all around us. What are we waiting for?
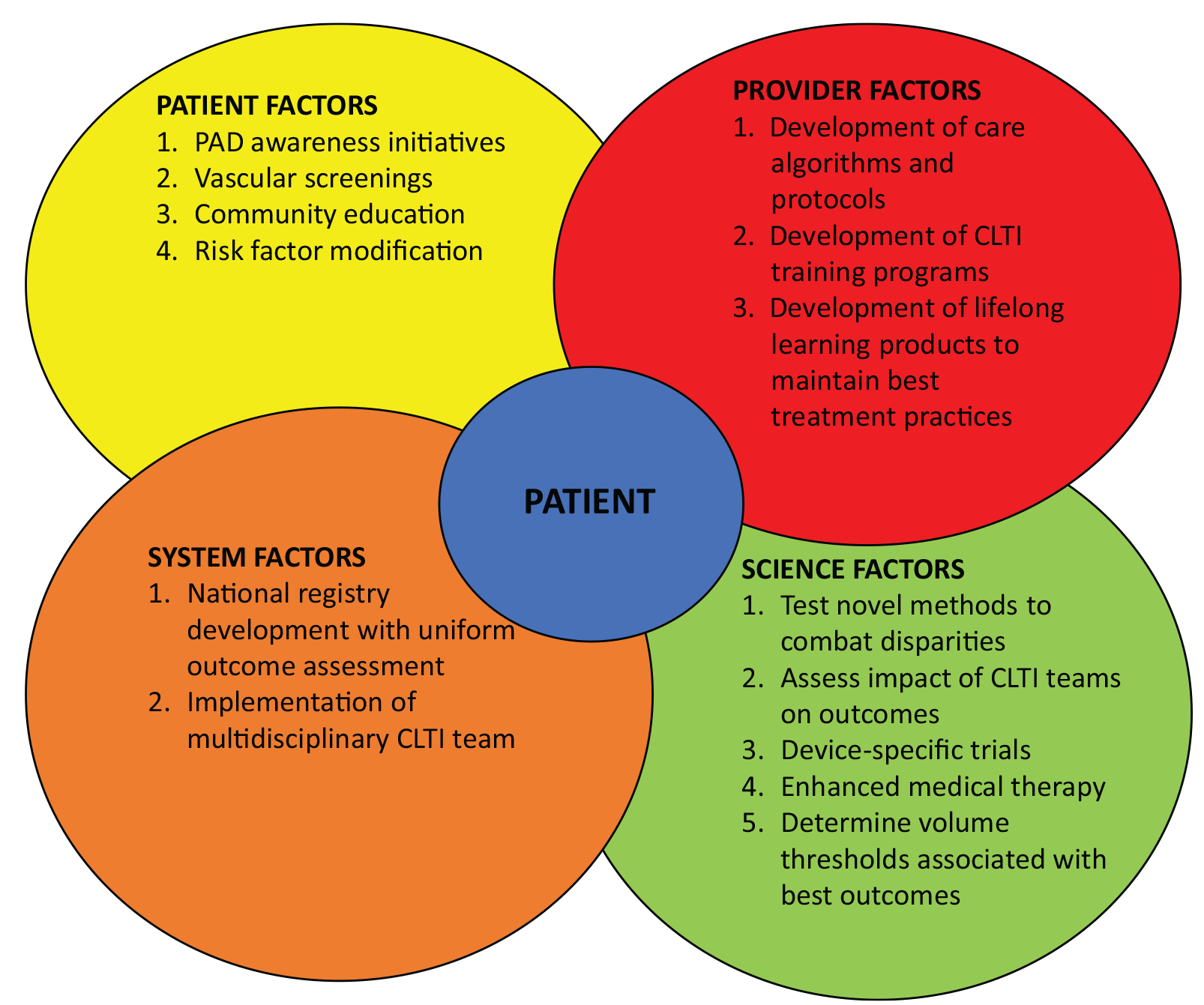
Possible strategies to combat disparities in CLTI care.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.