
Abstract
Background:
Real-world implementation of supervised exercise therapy (SET) referral for symptomatic intermittent claudication has been limited by poor provider awareness around reimbursement and low patient adherence owing to factors including limited center availability and long travel distances to sites.
Methods:
In this study, 76 of 77 consecutive male veteran patients with intermittent claudication managed at a single-center vascular specialty clinic were referred to SET prior to revascularization. Pre- and post-SET submaximal exercise treadmill testing was performed for assessment of exercise capacity in metabolic equivalents (METs).
Results:
In the 48.7% of subjects who completed 36 sessions of SET (n = 37), the average improvement in METs was 60.3%, reflecting improvement from baseline average of 3.4 METs to 5.5 METs after SET. Another 14 patients pursued self-guided exercise therapy and 25 patients declined any participation in exercise therapy. Reasons for declining participation in SET included inadequate transportation, cost of copayment, and interference with full-time work schedules. There was a nonsignificant numeric trend toward improved change in ankle–brachial index in the combined SET and self-guided exercise groups compared to those that declined exercise therapy (0.011 ± 0.124 vs –0.040 ± 0.105, p = 0.156).
Conclusion:
High acceptance of referral to SET is possible, despite the limitations to implementation. Incorporation of novel pre- and post-SET submaximal exercise treadmill testing allows for assessment of change in exercise capacity and aids in risk stratification and management of intermittent claudication symptoms.
Keywords
Introduction
Among patients with symptomatic peripheral artery disease (PAD) manifesting with intermittent claudication (IC), exercise limitation can have harmful consequences both to mobility, quality of life, and cardiovascular health. PAD can precipitate functional decline, especially in patients with the lowest ankle–brachial index (ABI) values. 1 Moreover, PAD is associated with increased risk of cardiovascular morbidity and mortality,2–4 and functional decline further increases this risk. 1 Accordingly, prevention of functional decline in addition to achievement of functional gains with supervised exercise therapy (SET) is a key component of optimal medical therapy of PAD, as supported by a Class Ia guideline recommendation. 5 Exercise has been shown to improve both walking time and quality of life.
Despite strong evidence for its use, referral rates to rehabilitation remain extremely low in the United States at 2% of eligible patients, 6 and patient completion rates are notably lower. 7 Within a real-world, single-center vascular clinic, this study aims to assess the implementation of universal referral to SET and to identify barriers to participation.
Methods
Study population
This is a prospective, cohort study of consecutive veteran patients with IC identified in a vascular specialty clinic over a 2-year period. Since institution of the MISSION Act (Maintaining Internal Systems and Strengthening Integrated Outside Networks), patients in a vascular specialty clinic at Veteran Health Administration (VHA)-Connecticut have been referred for guideline-directed SET at civilian centers. One patient received direct referral for peripheral vascular intervention prior to SET due to severe, limiting IC which impacted his ability to work. The remaining 76 patients underwent ABI measurement at initial evaluation along with the offer of referral to community-based SET. Among those patients accepting SET referral, submaximal claudication symptom-limited exercise treadmill testing (ETT) according to modified Bruce protocol was performed prior to initiation of SET and at completion of the 36 sessions of SET over the 12-week intervention. Those patients who completed self-guided exercise or declined did not undergo repeat submaximal ETT. Patients were classified into three categories: completed SET, self-guided exercise therapy according to physician prescription, and declined any exercise therapy.
Regarding the specific modalities of the SET programs, veterans were referred across the state to local centers. In total, patients were referred to 16 different facilities. Importantly, there was site-level variation in SET protocols and reporting. Some performed pre- and post-modified Gardner–Skinner stress tests, others performed submaximal Bruce protocol stress testing, and others performed no pre- or postevaluation. Despite the reporting differences between the centers, they all reported METs per session over the 36-session therapy, which is why we chose to employ a pre- and post-submaximal ETT measured in METs for uniform comparison.
Patients were followed closely throughout the study period. At initial consultation for IC, patients were counseled regarding the importance of medical optimization, smoking cessation, and exercise therapy, and they were referred for ABI, submaximal exercise stress testing, and SET. Patients were seen again within 6 weeks to ensure that referrals were processed and to address any patient concerns. Subsequent visits included one halfway through SET at 6–8 weeks postinitiation, at the conclusion of SET, and followed every 6 months thereafter. A similar follow-up protocol was in place for those pursuing self-guided exercise. For those who declined SET, they underwent initial consultation and referral, return within 6 weeks to discuss reasons for nonadherence, followed by a 3-month follow-up for symptom assessment and then every 6 months thereafter. This study was deemed exempted by the Institutional Review Board because it was approved by VHA-Connecticut as a quality improvement study for implementation of standard of care practices.
Outcomes
The primary outcomes of interest were rates of completion of SET and self-guided exercise. Secondary outcomes included percent change in METs (calculated as change in pre- to post-SET referral) and change in ABI (calculated as the difference between average of left and right ABI pre- and post-SET referral). Additionally, patients who declined SET were surveyed on barriers to adherence to SET referral, including requirement of copayment. Within the Veterans’ Affairs Health System, veterans who have a service-connected disability rating of 10% or higher are not required to pay a copayment. Those with supplemental Medicare insurance also had no copayment requirement.
Statistical analyses
Continuous data are presented as means ± SDs and compared with the nonparametric Wilcoxon test. Categorical data are presented as frequencies and percentages and compared with Fisher’s exact test. Nonparametric and exact tests were used due to the limited sample size; however, there was no evidence to suggest that continuous variables did not originate from a normal distribution. Baseline characteristics were compared between the completed and self-guided versus the declined groups. A p-value less than 0.05 was considered statistically significant without adjustment for multiplicity. All analyses were conducted using SAS version 9.4 (Cary, NC, USA).
Results
Of the 77 consecutive patients with IC between March 2019 and March 2021, all were male veterans with an average age of 71. Among these, 76 patients (98.7%) were referred for SET prior to any revascularization. Nearly half of all patients (48.7%) completed 36 sessions of SET and 67.1% completed either SET or physician-prescribed self-guided exercise. Baseline demographic findings of the completed SET (n = 37), self-guided exercise (n = 14), and declined (n = 25) cohorts are shown in Table 1. There were similar baseline characteristics among the three groups, except for a higher prevalence of diabetes in those that declined any type of exercise therapy. Patients that declined participation in any exercise therapy tended to be older and were more likely to report current tobacco use. Although rates of hypertension and hyperlipidemia were high in all patients, those who declined SET showed lower rates of hypertension than those who exercised. A prior lower-extremity bypass was rare, though those who declined any exercise therapy tended to a higher rate of prior peripheral vascular interventions (PVI). Nearly all patients were on a high-dose statin and 83% were on guideline-directed medical therapy to include a high-dose statin and either antiplatelet or anticoagulant. Fewer patients (66.2%) were prescribed angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blocker (ARB) agents. There were no significant differences in rates of medical therapy prescription between the groups (online Supplemental Table 1).
Patient demographics, comorbidities, procedural characteristics, and clinical presentation by supervised exercise therapy completion status (n = 76).
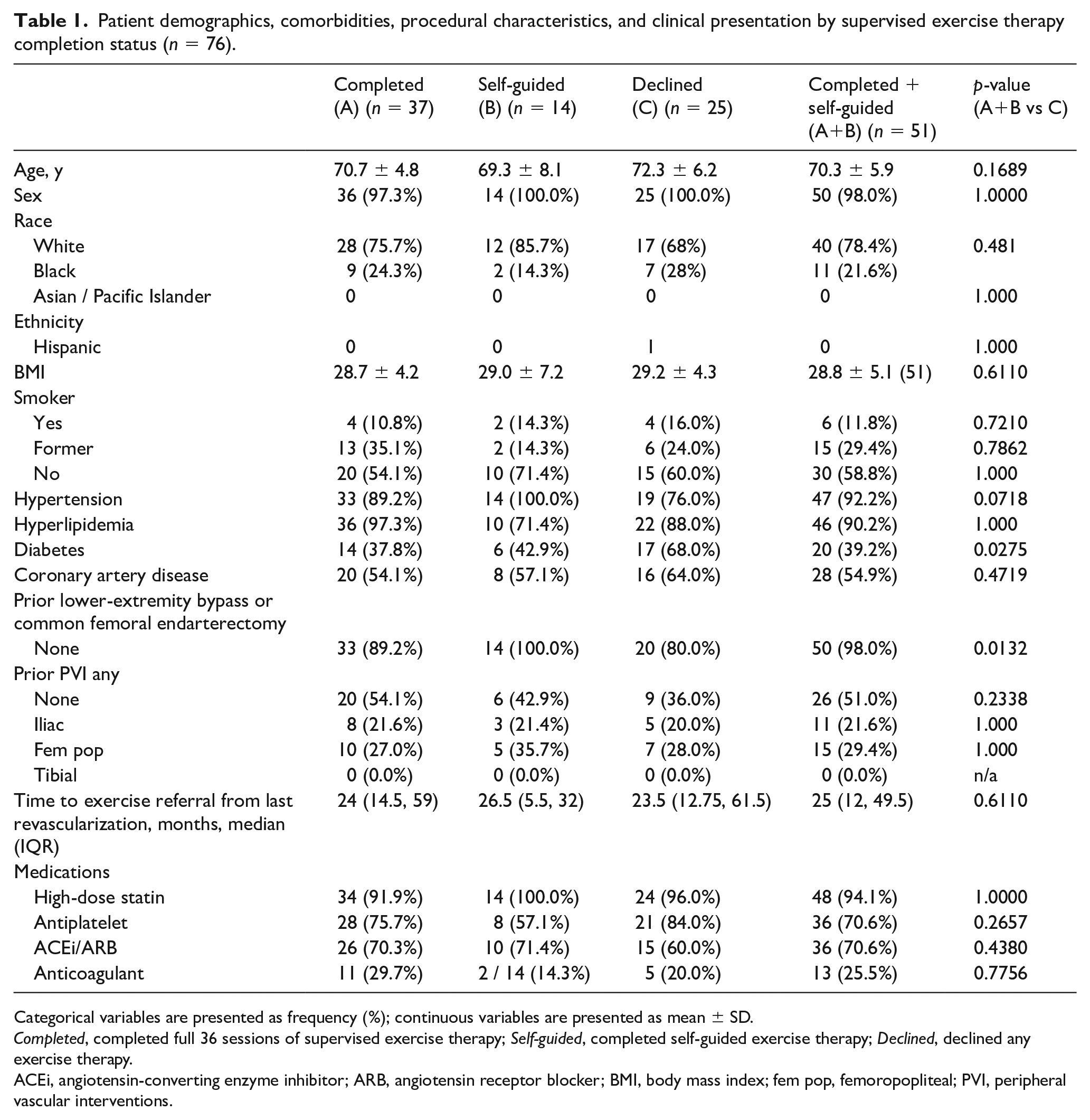
Categorical variables are presented as frequency (%); continuous variables are presented as mean ± SD.
Completed, completed full 36 sessions of supervised exercise therapy; Self-guided, completed self-guided exercise therapy; Declined, declined any exercise therapy.
ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; fem pop, femoropopliteal; PVI, peripheral vascular interventions.
Among patients declining SET, nearly one-third cited inadequate transportation or no facility close enough and nearly one-quarter cited copayment requirement as barriers (Table 2). Other notable reasons for declining SET were interference with a full-time work schedule (10.3%), concomitant musculoskeletal pain that limited participation (10.3%), and desire to exercise alone (10.3%). Of the patients who successfully completed SET, none had a copayment requirement.
Reasons for nonadherence to referral to SET.
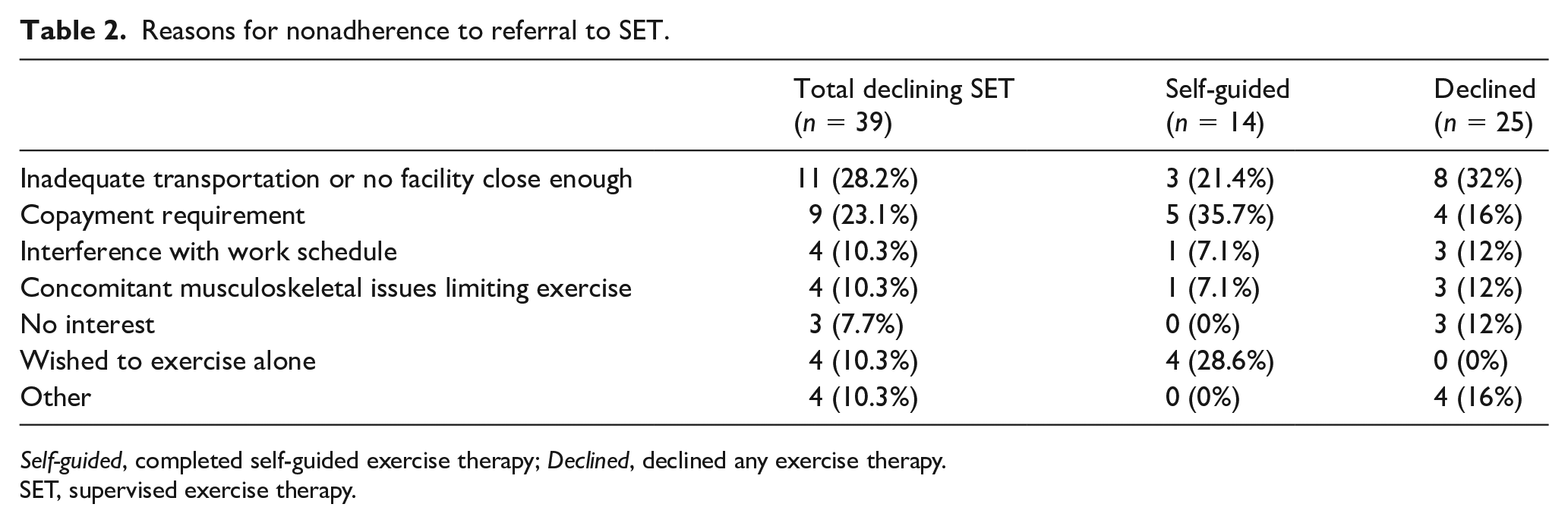
Self-guided, completed self-guided exercise therapy; Declined, declined any exercise therapy.
SET, supervised exercise therapy.
For patients completing SET, the average percent change in metabolic equivalents (METs) as assessed by submaximal, claudication symptom-limited ETT was 60.3% (Table 3). The average exercise capacity was 3.4 METs pre-SET, improving to 5.5 METs post-SET. All patients underwent ABI testing pre- and post-SET referral. Patients who completed SET or self-guided exercise tended towards an improved average ABI compared to those who declined SET.
ABI measurements and submaximal exercise treadmill testing METs pre- and post-referral to SET.
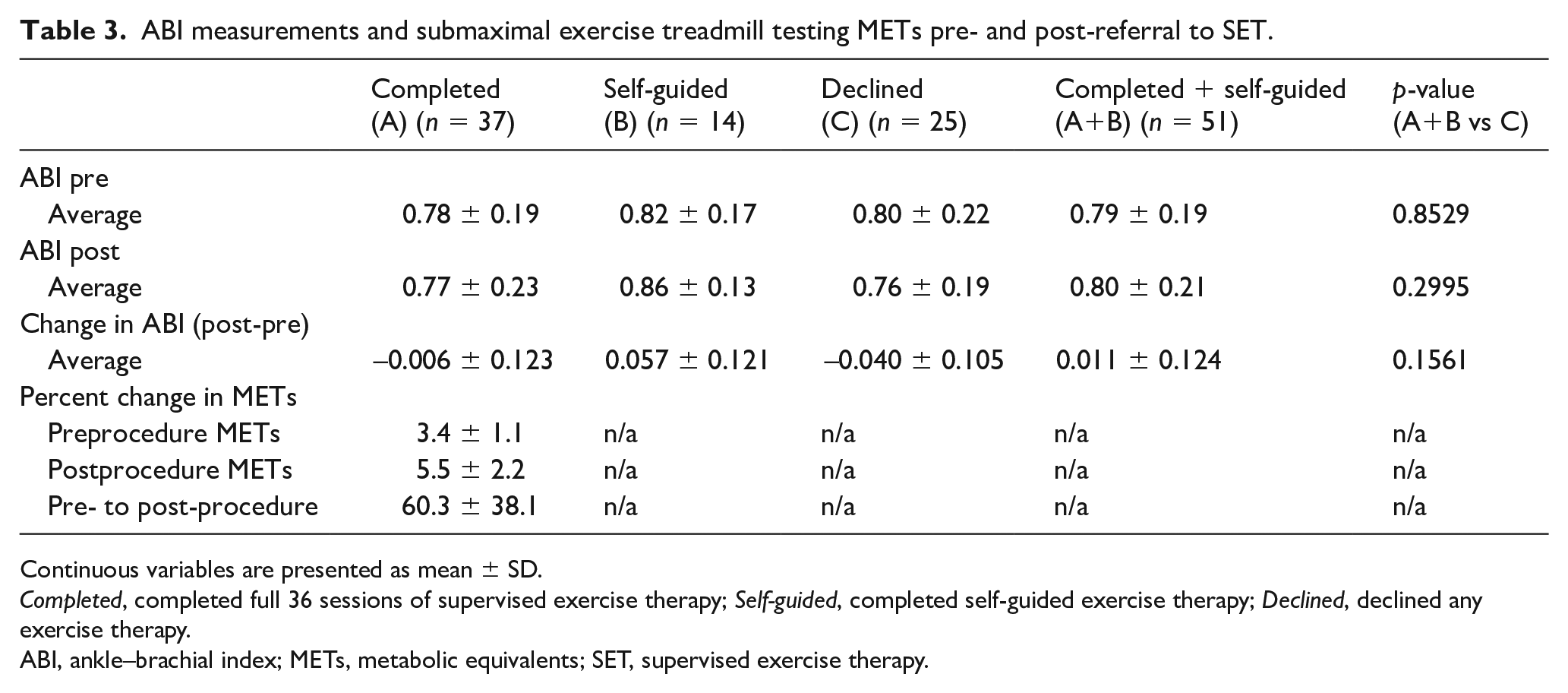
Continuous variables are presented as mean ± SD.
Completed, completed full 36 sessions of supervised exercise therapy; Self-guided, completed self-guided exercise therapy; Declined, declined any exercise therapy.
ABI, ankle–brachial index; METs, metabolic equivalents; SET, supervised exercise therapy.
During the follow-up period of 18 months, a total of six patients died (7.8%): two from the group that completed SET, four from the declined SET group, and none from the self-guided exercise group.
Discussion
This real-world implementation study shows that routine referral to SET in patients with PAD presenting with IC is feasible, with a high percentage of patients accepting referral and subsequent significant increases in exercise tolerance. Additionally, in this elderly population of veterans with comorbid hypertension, hyperlipidemia, diabetes, and coronary artery disease, two-thirds completed either SET or physician-prescribed self-guided exercise, and nearly half of all patients (48.7%) successfully completed 36 sessions of SET with average improvement in METs of 60.3%. Finally, the most common primary barrier to enrollment and completion of SET was copayment requirement per session and lack of transportation to the facility.
Despite a multispecialty guideline Class Ia recommendation for SET since 2005, 8 only since 2017 has Centers for Medicare and Medicaid Services (CMS) provided reimbursement. Additionally, specifically to the veteran population, the 2018 passage of the Veterans’ Affairs Maintaining Internal Systems and Strengthening Integrated Outside Networks (VA MISSION) Act made possible the referral to SET centers outside of the VA. Referrals to SET among Medicare beneficiaries have been sluggish, with around 1% of eligible patients referred between June 1, 2017 and December 31, 2018, similar to prior registry data showing United States referral rates at around 2%. 9 Notably, in this study, only 89 Medicare beneficiaries nationally completed SET, representing less than a tenth of a percent of eligible patients. In general, factors influencing these low referral rates include lack of provider awareness around CMS reimbursement, lack of available programs, and travel distance to those centers. 10
Although the present study population is small, with 76 patients referred and 37 completing SET, it represents a near-100% referral rate to SET in claudicants and a high rate of patient completion approaching 50%. Several reasons for higher referral and completion rates in this study include strict implementation of SET prior to revascularization strategy as clinically relevant, numerous referral sites offering SET, as well as the novel implementation of routine pre- and post-submaximal ETT. This likely improved completion rates for several reasons: (1) patients were able to assess their own exercise tolerance within the clinic setting prior to SET; (2) patients were motivated to show improvement on their post-ETT by completion of SET; and (3) frequent follow-up visits and discussions around the importance of exercise likely underscored the therapeutic nature of these interventions.
This study’s key finding of a 60% improvement in METs with SET is hypothesis-generating around whether there may be more long-term benefits to exercise than improvement in walking distance and symptomatic relief of IC. A study of fitness-related mortality risk in veterans suggests that the improvement seen from a baseline of 3.4 METs to 5.5 METs represents an approximate 3% improvement in 5-year mortality and 5–7% improvement in 10-year mortality risk. 11 For all-comers referred to ETT, patients with reduced exercise capacity were at higher risk of mortality, 12 and in those patients with stable coronary heart disease, acute coronary syndrome, and heart failure, the improvement in exercise capacity with cardiac rehabilitation is associated with reduced all-cause mortality.13–16 Specifically, in PAD patients, declining exercise performance has also been shown to increase mortality,17,18 and there are some data showing decreased mortality rates in those patients completing SET, 19 although a meta-analysis of limited randomized clinical trials shows no change in mortality over the study periods. 20 Whether participation in SET among patients with IC in conjunction with medical therapies improves mortality requires prospective randomized studies for further evaluation.
The breadth of clinical trial data overwhelmingly supports routine referral to supervised exercise therapy for patients presenting with IC.20,21 However, uptake has been sluggish, both in the United States and internationally,6,22 with some outliers showing high rates of referral in areas with widespread availability of centers.23,24 Successful implementation of SET requires both physician referral and patient adherence. Physician perceptions of barriers to referral include lack of availability of SET programs and that, when available, they are largely administered through cardiac rehabilitation programs with protocol variations from PAD-focused programs. 10 Indeed, in our study where veterans were referred across the state to 16 distinct centers, we found heterogeneity in protocols and outcome measurements, potentially reflecting these programs’ outgrowth from existing cardiac rehabilitation centers. From the patient side, barriers to walking in patients with IC have been well documented and include comorbid health concerns, walking-induced pain, poor exercise capacity, and lack of knowledge around PAD disease pathology. 25 Formal SET addresses many of these barriers; however, adherence to this regimen is also difficult for patients. A meta-analysis of SET studies reporting reasons for screen failures among study-eligible patients revealed limited symptoms when walking was formally quantified, lack of patient interest in SET, medical comorbidities affecting participation, and distance and timing of sessions. 26 This study additionally looked at causes of incomplete adherence with lack of motivation and medical comorbidities as most common causes. 26 In a smaller European study of 52 patients who reported barriers to SET completion, the most common were inability to keep up with the exercise regimen, no interest, transportation issues, social factors, and wanting to exercise alone. 27 This present study adds to the literature by identifying similar barriers in a predominantly male, veteran cohort with the principal barriers of inadequate transportation, no nearby facilities, and copayment requirement. To improve referral and adherence rates to SET, it will be necessary to either expand centers or innovate mobile health technologies to improve access to care.
Study limitations
This study is limited by single-center analysis and a small, real-world sample size that affects the ability to determine true differences between these groups. Additionally, this male veteran sample limits generalizability. Rates of adherence and barriers to SET may be different by gender, which this study cannot detect.
Conclusions
SET is a key component of optimal medical therapy for patients with PAD presenting with IC. In this study, routine referral to SET is feasible and completion rates in this study approach 50%, exceeding previously reported results. In patients completing SET, the average improvement in METs was 60%. Whether functional improvement in exercise capacity correlates to long-term mortality reduction in patients with IC requires further study. The most important barriers to SET adherence include inadequate transportation and copayment requirement. Widespread adoption of SET referral and adherence will require further investigation into the patient-level impediments.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X211073622 – Supplemental material for Implementation of supervised exercise therapy in a veteran population with symptomatic claudication
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X211073622 for Implementation of supervised exercise therapy in a veteran population with symptomatic claudication by S Elissa Altin, Marabel D Schneider, Helen Parise, Subhash Banerjee, Wen-Chih Wu, Judith L Meadows, Steven Pfau, Heidi Keefe and Ehrin J Armstrong in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.