
Abstract

What is the subclavian artery?
There are two subclavian arteries: one on the left and one on the right. These large blood vessels supply blood to the left and right arms. The subclavian arteries are located just under the clavicle (collarbone) on each side of the body, which is why they are called subclavian. As shown in Figure 1, the left and right subclavian arteries are not identical. The left subclavian artery branches off directly from the aorta, the largest artery of the body that leads away from the heart. As a result, this artery is more commonly affected by problems than the right subclavian artery. The right subclavian artery usually arises as a branch off the brachiocephalic (or innominate) artery. Both the right and left subclavian arteries give rise to important branches called the vertebral arteries, which supply blood flow to the brain.
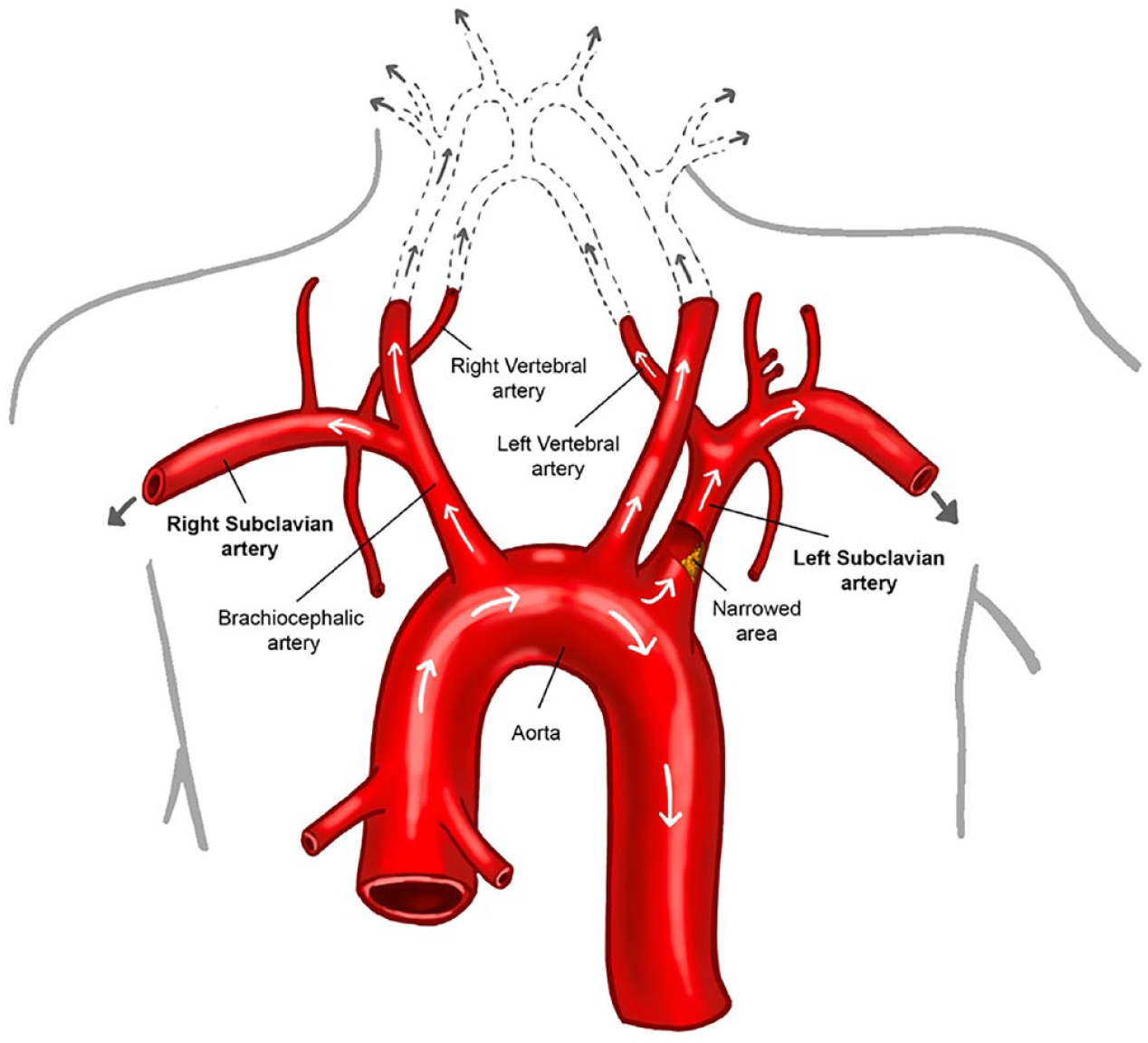
The anatomy of the subclavian arteries. The left subclavian artery branches directly from the aorta, whereas the right subclavian artery is a branch of the brachiocephalic artery. The subclavian arteries supply the arms with blood. The left and right subclavian arteries give rise to the left and right vertebral arteries, which supply the brain with blood.
What problems can occur with the subclavian artery?
Several conditions can cause problems with the subclavian arteries. Peripheral artery disease (PAD), which is common in leg arteries, also occurs in the upper body. PAD and most other artery blockages are caused by atherosclerosis, which is thickening and hardening of arteries due to cholesterol plaque build-up. Figure 2 illustrates atherosclerosis. Patients with PAD may have stenosis (i.e., narrowing) of the subclavian artery. 1
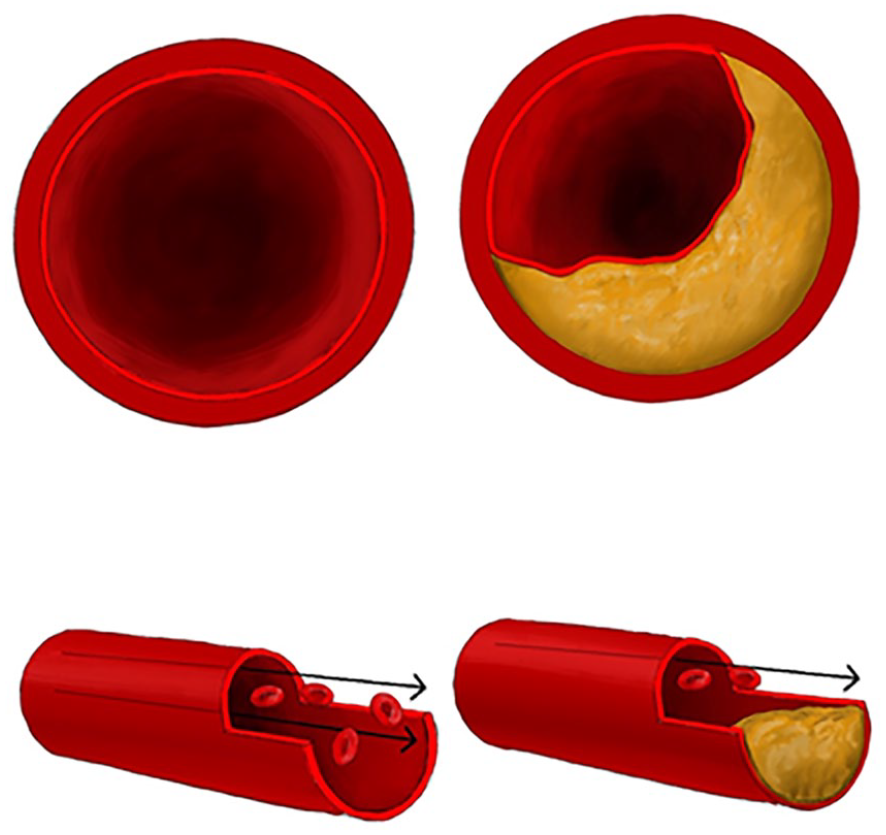
With atherosclerosis, arteries become narrowed or blocked by cholesterol plaque, limiting blood flow. Blood can flow freely in the artery shown on the left; however, the artery shown on the right is partially blocked by plaque.
Although atherosclerosis is the most common cause of blockage in the subclavian artery, other rare disorders, such as vasculitis, can also cause problems. Vasculitis (or arteritis) refers to inflammation of the blood vessels, which can lead to artery thickening, narrowing, obstruction, or an aneurysm (i.e., bulging) of the vessel wall over time. There are many types of vasculitis, such as Takayasu arteritis and giant cell arteritis, which cause inflammation of the aorta and other major blood vessels.
In some cases, chest radiation for cancer treatment can result in scarring of the vessel wall, which can cause narrowing of the subclavian artery. The subclavian arteries can also be compressed in vascular thoracic outlet syndrome, in which the uppermost rib and surrounding muscles compress the vessels and nerves. Thoracic outlet syndrome is more common in younger patients and can be provoked by repetitive arm movements, such as in athletes or instrumental musicians.
What are the symptoms of subclavian artery stenosis?
With significant narrowing of the subclavian artery, a common symptom is muscle cramping with arm use due to insufficient blood flow (known as claudication). The arm muscles may become painful or fatigued with physical activity. Symptom severity can depend on whether a person is left- or right-handed, and which arm is used more in daily life. Rare symptoms include dizziness, vertigo (room spinning), or fainting. In patients who have had prior coronary artery bypass surgery, subclavian artery stenosis can cause chest pain if the bypass graft was a branch of the subclavian artery. In general, if the narrowing is mild, then it may not cause any symptoms. If a portion of plaque or blood clot breaks free and travels down the arm vessels (embolizes), it can become lodged in a smaller vessel, causing finger pain and discoloration.
How is subclavian artery stenosis diagnosed?
The first step in diagnosis is the physical exam. The blood pressure may be different between the left and right arms, with the affected arm having a falsely low reading. The pulses throughout the affected arm may also be reduced.
The blood pressures measured in the left and right arms should normally be within about 10–15 mmHg of one another. Larger differences between the left and right arm readings may indicate subclavian artery stenosis. If the subclavian artery is blocked or narrowed, then the lower blood pressure from that arm is not accurate. Any medications for high blood pressure should be adjusted to treat the blood pressure on the unblocked arm (i.e., the arm with higher blood pressure readings). Irregular heart rhythms such as atrial fibrillation can also impact blood pressure readings.
When significantly different arm blood pressures are identified, further testing can be done to help clarify the problem and guide potential treatments. The test of choice depends on the symptoms, medical situation, and other risk factors a patient may have.
A handheld ultrasound device (Doppler) can be used to listen to the arterial blood flow in the doctor’s office. More detailed, noninvasive ‘physiologic’ testing of the arms can be performed in the vascular laboratory to check for differences in blood flow at different sites in the arms. With pulse volume recordings (PVRs) and segmental pressure analyses, a series of blood pressure cuffs and an ultrasound device are used to obtain more specific information about blood flow in the arteries. 3 Arterial duplex is another noninvasive ultrasound test used to visualize the arteries and blood flow directly to determine the location and degree of narrowing or blockage. High-velocity blood flow can indicate a narrowed vessel. 3
A carotid duplex of the neck arteries is often helpful when subclavian artery stenosis is suspected. This ultrasound test allows direct visualization of the neck arteries, including the vertebral arteries, and it can establish whether the blood is flowing in the correct direction from the subclavian arteries into the vertebral arteries or whether subclavian artery stenosis is causing ‘steal’ (see below).
Two other noninvasive, advanced imaging tests can be helpful to produce more detailed pictures: computed tomographic angiography (CTA) and/or magnetic resonance angiography (MRA). The images from CTA (Figure 3) or MRA can reveal narrowing, tears, dilation, aneurysms, or other damage in the artery.
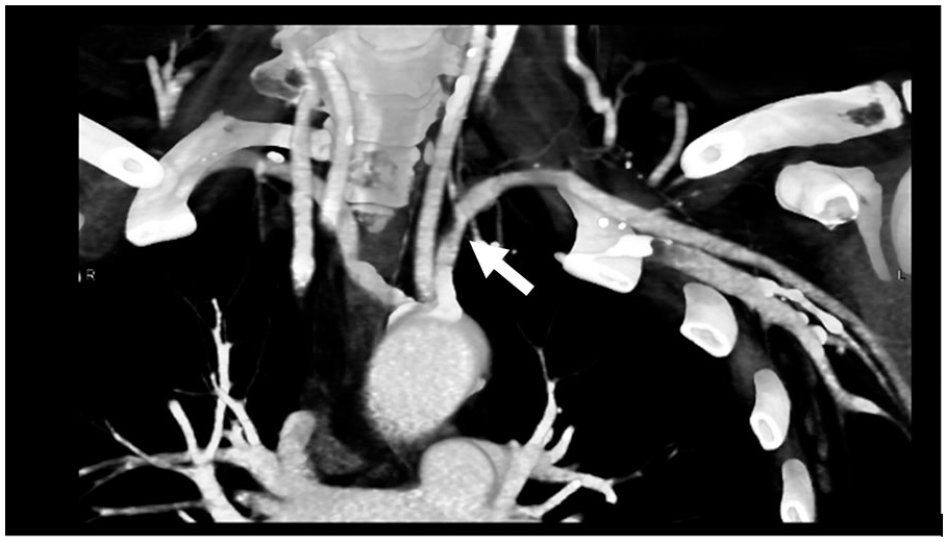
Computed tomographic angiography highlights the arteries and reveals the narrowing of the left subclavian artery (arrow).
An angiogram test is more invasive. A catheter is inserted into an artery, and dye (contrast) is injected to follow and visualize the path of the blood flow to reveal the location and severity of an artery blockage.
What is ‘subclavian steal’? How is this different from subclavian stenosis?
In subclavian stenosis, the artery is simply narrowed, leading to decreased blood flow beyond the area of blockage. When the subclavian blockage is severe, or if the artery is completely blocked, a condition called ‘subclavian steal’ can occur (Figure 4).
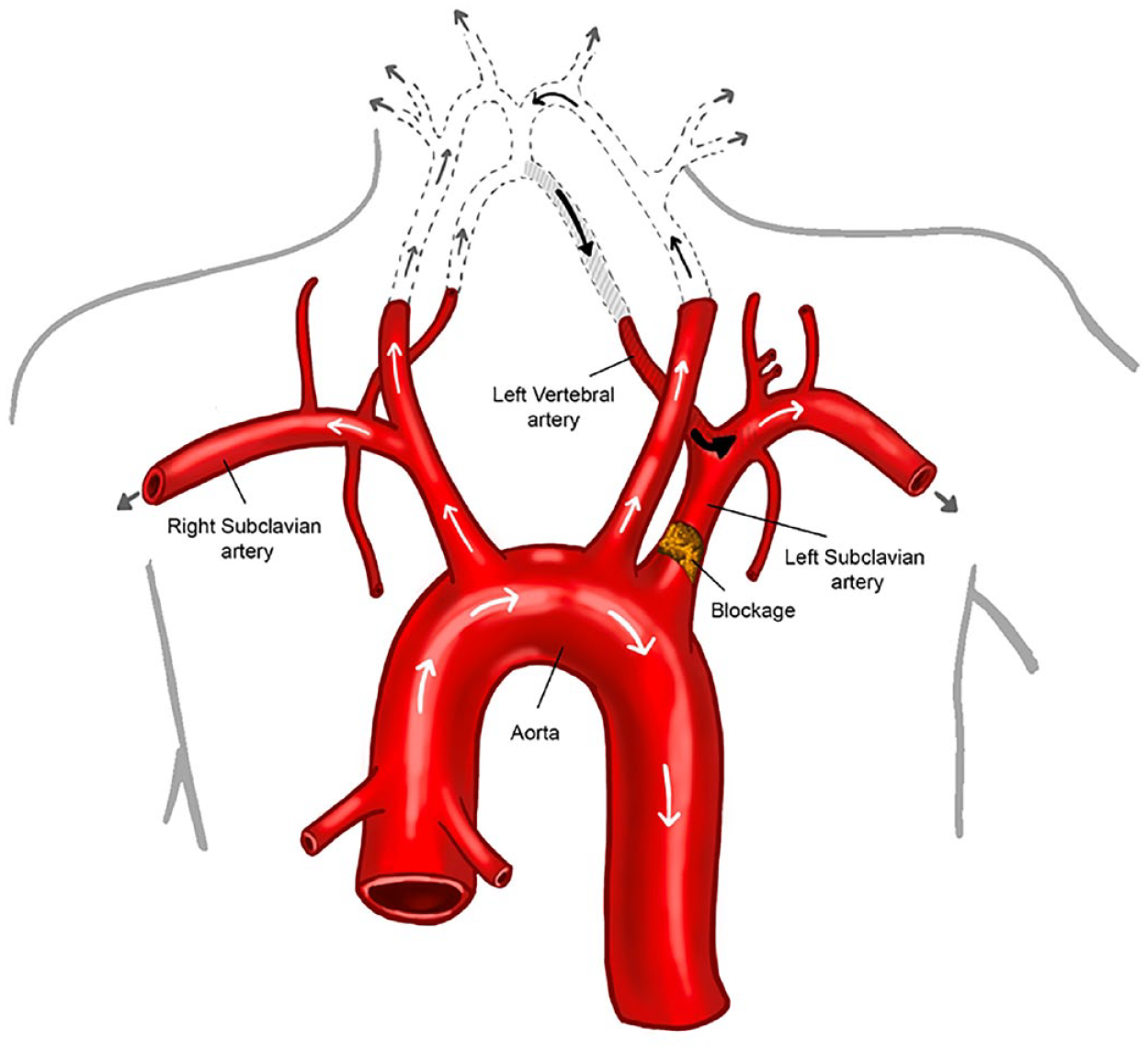
When the subclavian artery is blocked or severely narrowed, blood cannot flow into the subclavian artery from the aorta. Instead, the subclavian artery sometimes ‘steals’ blood from the vertebral artery above it (shaded), which should normally supply the brain. This abnormal reversal of blood flow is called ‘subclavian steal’.
Instead of flowing normally from the aorta into the subclavian artery and then upward into the vertebral artery, blood is diverted. In subclavian steal, the subclavian artery receives flow from the vertebral artery rather than supplying flow to the vertebral artery. The vertebral arteries normally supply blood flow to the brain, but in the case of steal, the subclavian artery ‘steals’ blood from the brain to supply the arm. This abnormal reversal of blood flow in the vertebral artery can be seen by ultrasound (Figure 5).
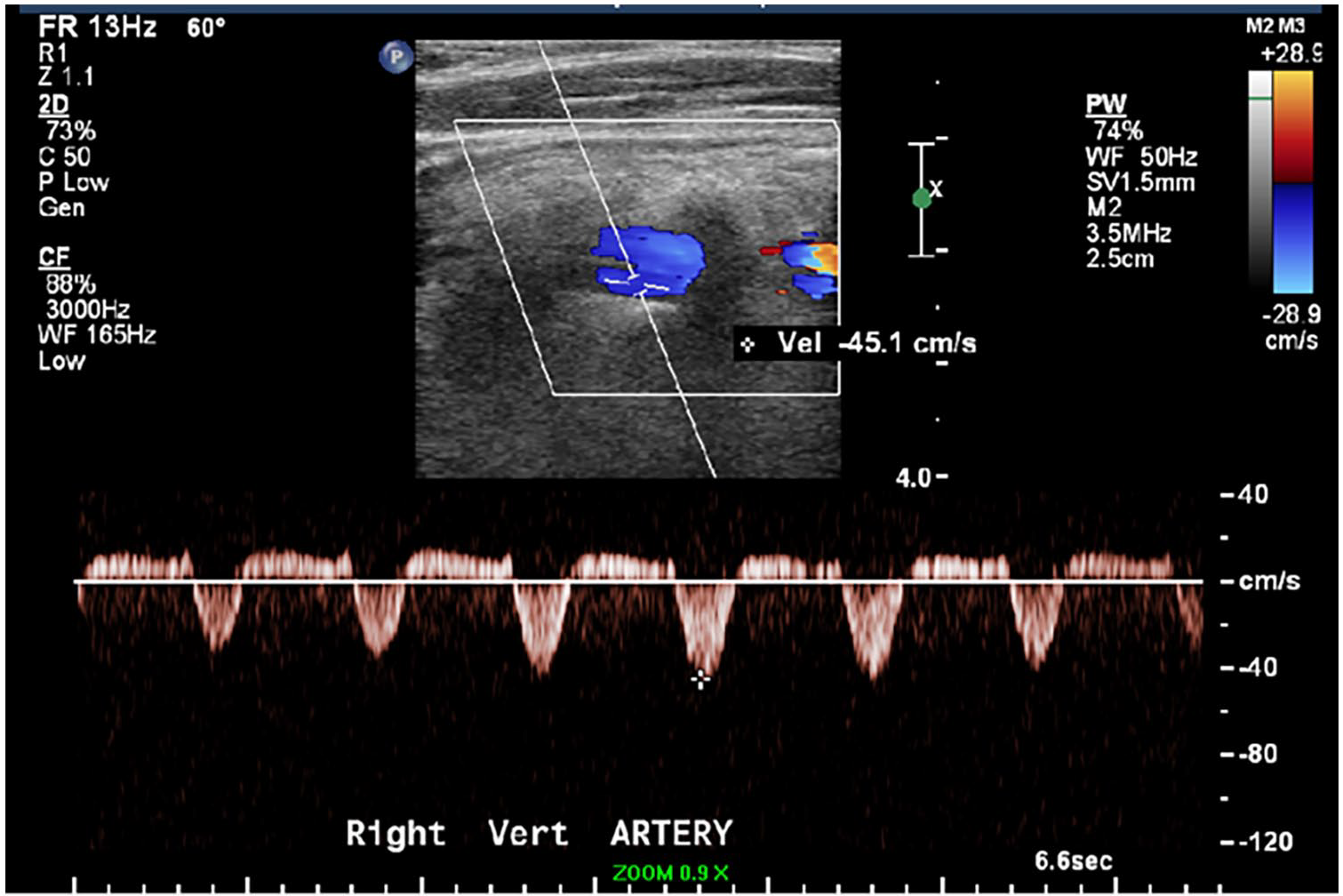
In this ultrasound image, the blood in the right vertebral artery (shown in blue) is flowing in the wrong direction, away from the brain. The Doppler waveform (below ultrasound image) shows blood flow both to the brain and to the arm, consistent with subclavian steal.
The term ‘subclavian steal syndrome’ is used when the stealing of blood flow from the brain causes symptoms, which may include vertigo, double vision, or passing out. Sometimes the symptoms occur only during arm exercise – when the arm requires more blood flow. Subclavian stenosis is more common than subclavian steal (flow reversal), and subclavian steal syndrome (with symptoms) is quite rare.
If there are no symptoms, is treatment of subclavian artery stenosis necessary?
Sometimes plaque in the subclavian artery is found incidentally on images or tests done for other medical reasons. Treatment depends on the type and severity of the problem. Among patients who have subclavian artery plaque (i.e., atherosclerosis), many will also have atherosclerosis in the arteries that supply blood flow to the heart or brain. Therefore, medical treatment and lifestyle adjustments should focus on reducing the risk of future heart attack, stroke, or worsening subclavian artery problems.
What medications are used to treat subclavian artery stenosis?
Treatment of atherosclerosis includes lifestyle changes such as avoiding tobacco, improving nutrition, and increasing physical activity. Smoking is a key risk factor for PAD, including subclavian artery stenosis, and medications such as nicotine replacement or varenicline may aid in efforts to quit.
Medications are also sometimes needed to reduce the risk of heart disease and vascular disease progression as well as future heart attack or stroke. Medications often include blood thinners such as aspirin, cholesterol-lowering medications such as statins, and/or blood pressure medications. To learn more about statins and/or high blood pressure, read the Vascular Disease Patient Information Pages on ‘Statins’ and ‘Hypertension’.4,5 As mentioned above, blood pressure medications should be adjusted based on the higher blood pressure reading (in the arm without subclavian stenosis).
If the subclavian artery stenosis is due to vasculitis, medical treatment focuses on controlling inflammation to prevent further damage to the blood vessels.
When is invasive treatment required for subclavian artery stenosis?
Invasive treatment is rarely required for subclavian artery stenosis. If the stenosis is limiting arm function or activities in daily life, or if there are symptoms of subclavian steal or chest pain in patients with prior coronary artery bypass, then procedures or surgery can be considered.
If intervention is needed, the minimally invasive treatment option is called balloon angioplasty. A catheter with a small balloon is directed into the blocked vessel. The balloon is inflated to open the vessel and restore blood flow (Figure 6). This procedure is usually combined with a stent to keep the vessel open. In rare cases, open surgery is needed to bypass a subclavian artery blockage completely.
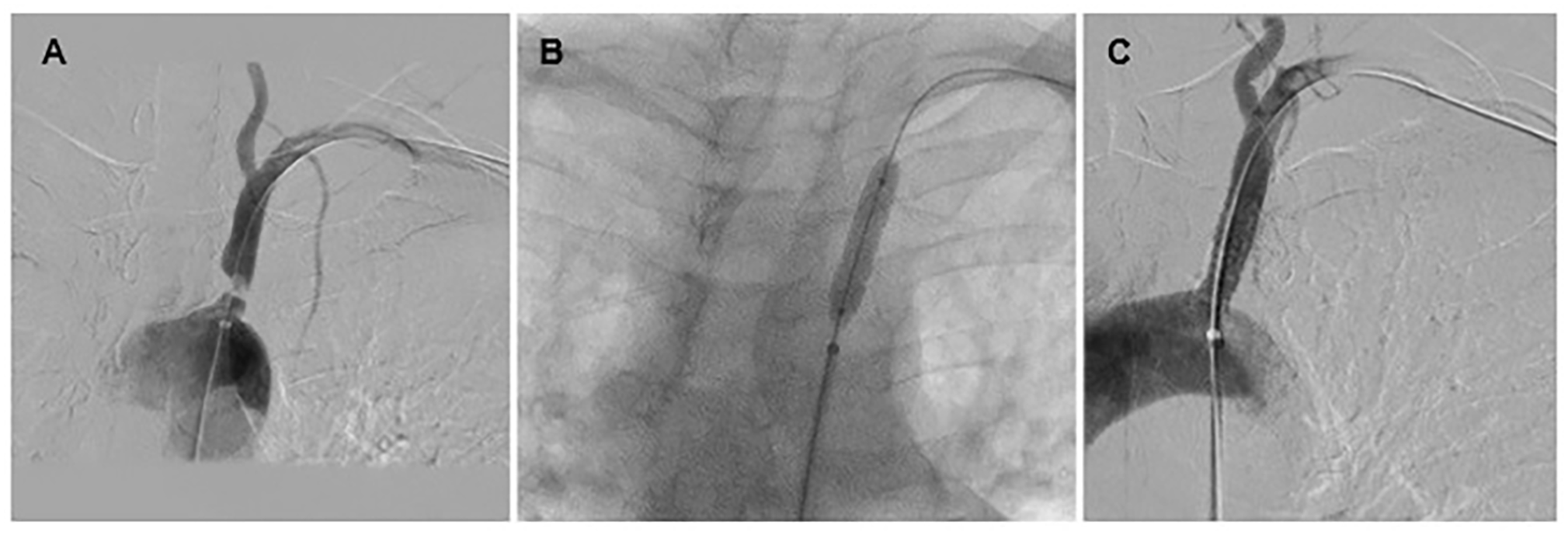
With an angioplasty procedure, a narrowed subclavian artery (A) can be re-opened with a balloon (B). A stent (metal scaffold, C) is then placed to prop open the artery.
How can subclavian artery problems be prevented?
The most important way to prevent atherosclerosis and PAD, including in the subclavian arteries, is to work toward a healthy lifestyle. Steps include good nutrition, regular exercise, maintaining a healthy body weight, and avoiding all forms of smoking and tobacco. It is also important to manage other medical problems carefully. For example, the risk of vascular problems can be reduced by treating high blood pressure, lowering cholesterol levels, maintaining healthy blood sugars in diabetes, and taking medications such as aspirin or statins as prescribed.
Summary
Stenosis (narrowing) of the subclavian artery is most commonly caused by atherosclerosis, and it usually affects the left subclavian artery. It may be suspected if a large difference in blood pressure readings is found between the arms. Imaging tests can confirm the diagnosis, and treatments aim to address the root cause. Prevention and treatment include lifestyle modification, risk factor management, and sometimes medications. Surgical procedures and minimally invasive vascular procedures are available to re-open or bypass blocked arteries to restore blood flow when needed.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage
The Vascular Disease Patient Information Page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.