
Abstract
The aim of this systematic review was to evaluate the available evidence regarding the acute effects of interrupting/breaking up prolonged sedentary behavior (SB) on vascular health among individuals at elevated risk for type 2 diabetes (T2D). Searches of MEDLINE, Embase, Web of Science, and Cochrane Library databases were conducted on April 7, 2020. Included studies: (1) examined the effect of breaking up prolonged SB in adults with or at elevated risk for T2D and (2) assessed a vascular health outcome, such as blood pressure (BP), flow-mediated dilation (FMD), pulse-wave velocity, or endothelin-1. A total of 20 articles (17 unique studies) were included. Only three studies reported adequate statistical power for the specified vascular outcome. The available evidence suggests that light and moderate intensity activity breaks are effective in acutely lowering BP when compared to prolonged sitting. The small number of studies that included FMD or other vascular outcomes prohibits conclusions regarding the impact of SB breaks on these outcomes. Few studies evaluating the impact of breaking up SB among adults at risk for T2D have included and been adequately powered to examine vascular outcomes, but our preliminary finding, that certain SB breaks improve BP, provides proof-of-concept for this line of inquiry. Future studies should examine both the acute and chronic vascular effects of breaking up SB among individuals most vulnerable to the effects of SB (e.g. older adults, those with T2D), as these individuals are both highly sedentary and at greatest risk of poor health outcomes.
Introduction
Although the terms are often used interchangeably, sedentary behavior (SB), which is defined as any waking behavior performed in a sitting or lying position and characterized by an energy expenditure ⩽ 1.5 metabolic equivalents (METs), 1 is distinct from physical inactivity (i.e. lack of achievement of physical activity guidelines 2 ). SB has significant detrimental long-term health effects, including increased risk of type 2 diabetes (T2D),3,4 cardiovascular disease (CVD), and early mortality,5,6 even among physically active individuals. 7 As harmful as SB is in otherwise healthy adults, it presents an even greater concern in individuals with T2D. T2D is a major public health problem, impacting more than 460 million adults worldwide. 8 Although numerous factors affect the development of T2D, including age, hypertension, lack of physical activity, and genetic factors, elevated body weight alone presents a significant risk factor. 9 Adults with T2D tend to engage in higher volumes of SB compared to the general population 10 and have frequent cardiovascular comorbidities. 11 The combined effects of T2D and SB appear to place individuals with T2D at particularly high risk for poor cardiovascular outcomes. 12
In addition to the health risks of engaging in a high total volume of SB, research findings suggest that accumulation of SB in prolonged bouts (vs SB broken up by bouts of physical activity (PA)) is particularly detrimental.13–18 In observational studies, prolonged SB has been linked to increased body mass index (BMI), cholesterol, and fasting glucose concentrations.13,19,20 Experimental data demonstrate that breaking up prolonged SB (SB breaks) acutely improve postprandial glucose and insulin levels.15,21–23 These benefits are more pronounced in individuals with impaired glycemia or T2D;24,25 however, the beneficial effects of SB breaks do not appear to be limited to a specific population – similar effects have been observed regardless of age, sex, or BMI.15,26,27 Importantly, these associations are observed even in people who achieve the recommended levels of moderate to vigorous physical activity (MVPA). 7
Though a growing body of research has documented the beneficial effects of breaking up SB with multiple bouts of PA on glycemic outcomes (e.g. postprandial glucose, insulin), the effects of SB breaks on vascular outcomes (e.g. blood pressure (BP), flow-mediated dilation (FMD), etc.) have received substantially less attention. A systematic review by Saunders et al. 21 synthesized studies examining the acute impact of breaking up SB on glycemic control, triglyceride responses, and vascular function; however, only six studies included vascular outcomes, and of those, BP was the only vascular outcome in five studies. A recent review by Paterson et al. 28 suggests that the vascular dysfunction of the lower limbs (as measured by FMD) caused by acute exposure to prolonged SB can be prevented by aerobic or resistance activity breaks; however, only six studies met inclusion criteria. Importantly, existing reviews included primarily healthy young adults while specifically excluding studies of individuals with known metabolic and cardiovascular diseases (e.g. T2D, hypertension). Therefore, it remains unclear if SB breaks influence vascular function in individuals with or at elevated risk for T2D (e.g. impaired fasting glucose, overweight/obesity).
The purpose of the present review is to synthesize the available literature reporting the impact of breaking up prolonged SB on vascular outcomes among adults with or at elevated risk for T2D. Specifically, we address the following research questions: (1) What is the effect of SB breaks on systemic measures (e.g. BP, heart rate), regional measures (e.g. FMD, pulse-wave velocity (PWV)), and blood biomarkers (e.g. epinephrine, endothelin-1) of vascular health? (2) Is there evidence that the type/intensity of break (e.g. standing, light activity, MVPA, resistance exercise) has differential effects? We hypothesized that SB breaks would have beneficial effects on vascular outcomes among individuals with or at elevated risk for T2D.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for the reporting of systematic reviews 29 and the review protocol was registered on PROSPERO (CRD42020183423).
Population
Studies of male and female adult participants (age 18 or older) were included. We included studies that focused on participants with T2D or at elevated risk for T2D, which we defined as individuals with impaired glucose tolerance, overweight, or obesity (sample average BMI ⩾ 25 kg/m2). Studies that focused specifically on a disease other than metabolic disease (e.g. stroke or spinal cord injury rehabilitation) were excluded due to the potential influence of the disease condition on participant physical function.
Intervention and comparison conditions
To be included in the present review, articles must have reported the results of an experimental or quasi-experimental study examining the effects of an intervention targeting breaking up SB on vascular health of human participants. Eligible study designs included randomized controlled trials (RCTs), interventions without random assignment, and cross-over designs. To be included, the comparator condition had to consist of some form of breaking up or interrupting SB, such as standing or light or moderate intensity PA. No specific limits were placed on the duration of activity or overall intervention period. Studies that examined the effects of detraining or enforced physical inactivity conditions (e.g. bed rest studies) were excluded. We also excluded studies in which the intervention targeted solely a reduction in total volume of SB and did not report specifically targeting breaking up/interrupting prolonged SB.
Outcomes
Included studies were required to report one or more indicators of central or peripheral vascular health or function, including systemic measures such as BP (systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP)), regional measures such as arterial stiffness (assessed via PWV), FMD, or cerebral blood flow, or blood biomarkers (e.g. epinephrine, endothelin-1, nitrates/nitrites, etc.). This broad strategy was used to identify the diversity of vascular measures used in the literature.
Search strategy
A systematic search was conducted of MEDLINE (via Ovid MEDLINE® and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Daily and Versions®, 1946 to present), Embase (via Elsevier, Embase.com, 1947 to present), Web of Science Core Collection (via Clarivate Analytics, including Science Citation Index Expanded and Social Sciences Citation Index, 1974 to present), and Cochrane Library (via Wiley, including Cochrane Database of Systematic Reviews and Cochrane Central Register of Controlled Trials). Articles reporting the results of intervention studies examining the effects of interrupting or breaking up SB on vascular outcomes among individuals with T2D or at risk for T2D due to impaired fasting glucose, overweight, or obesity were retrieved. The search strategy was developed with the assistance of a research librarian from the University of Colorado Strauss Health Sciences Library. Additional limits (when available) were placed on the searches to restrict the output to articles in English and those that included an adult (age 18 or older) population. No limits were placed on publication date, thus the search included articles published between January 1, 1946 and April 7, 2020. A sample search strategy used for the MEDLINE search is reported in online Supplemental Table 1. Similar strategies were used for Embase, Web of Science, and Cochrane Library. Searches of PROSPERO and the Cochrane Database of Systematic Reviews were also conducted to determine if protocols for related systematic reviews had already been published. The reference lists of the selected articles were also reviewed for additional eligible articles.
Study selection
Review and selection of articles was facilitated by the web-based software platform Covidence (Covidence.org, Melbourne, Australia). The titles and abstracts of all potentially relevant articles were initially screened by one reviewer (MOW or AB). Articles deemed to be potentially relevant were obtained for full-text review and screened by two independent reviewers (MOW and AB). Discrepancies were resolved via discussion to achieve agreement.
Data extraction
The following data were abstracted from each included article: study purpose, primary and secondary outcomes, characteristics of the study participants (stated target population, sample size, mean age, mean BMI, sex distribution), key components of the intervention (total duration of the condition(s), type of PA, duration, and frequency of breaks), and primary findings. We also extracted data on key eligibility and methodological issues in order to evaluate study rigor, including the use of objective measures to assess SB and PA, menopausal status, washout period, documentation and timing of testing in relationship to female hormonal cycle, and abstention from MVPA, alcohol, caffeine, and smoking prior to testing. Data were extracted independently by two authors (MOW and AB), with disagreements resolved by discussion to achieve consensus. Total energy expenditure (kcal/kg) was estimated for each condition based on the PA frequency, intensity, and duration data provided by the authors using the standard MET calculation procedure in the ‘2011 Compendium of Physical Activities’. 30
Determination of methodological quality and strength of the evidence
Risk of bias was assessed using Cochrane’s risk of bias assessment tool. 31 The strength of the evidence was based on assessment of the key domains (quality, quantity, and consistency) identified by the Agency for Healthcare Research and Quality. 32 Risk of bias and strength of the evidence were independently evaluated by two authors (MOW and AB). Disagreements were resolved by discussion among the reviewers to achieve consensus.
Results
A total of 7239 articles were identified through comprehensive searches of MEDLINE (n = 1260), Embase (n = 2372), Web of Science (n = 2171), and Cochrane Library (n = 1470). Five additional articles were identified via searches of the reference lists of the included articles. After removing duplicates, 5034 unique titles/abstracts were screened (Figure 1). A total of 124 articles were selected based on title/abstract for full-text screening. Of these, 20 articles33–52 representing 17 unique studies met our inclusion criteria.
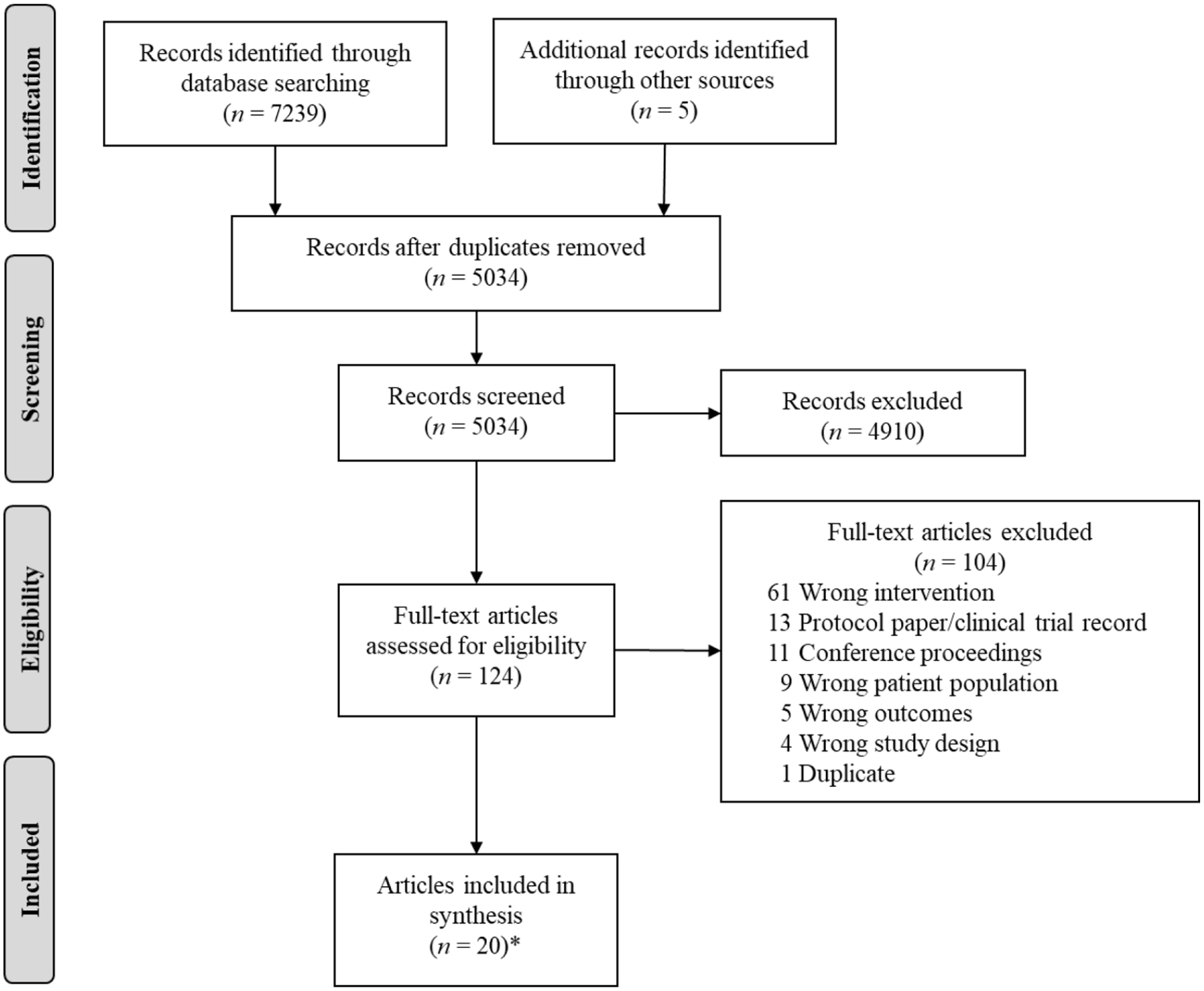
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Characteristics of included studies
Characteristics of the included studies are reported in Supplemental Table 2. Included studies were conducted primarily in the US (n = 6),34–36,43–45,52 Australia (n = 5),40,41,46,48–50 and the UK (n = 4),33,37–39,51 as well as one study each from Spain 47 and Brazil. 42
Sample characteristics
Participant demographic characteristics varied greatly across the studies. Although the majority of studies (n = 11) enrolled both young and middle-aged adults, one study included exclusively young adults (18–35 years) 33 and five studies (six articles)41,43,48–51 targeted an older adult population. The mean (SD) age of participants ranged from 24.3 (3.0) 33 to 70 (7) 50 years. Eligible studies ranged in size from 9 to 264 participants and included a total of 627 unique participants. The percent of the sample that was female varied from 17% 50 to 100%. 43 The mean (SD) BMI of participants ranged from 25.5 (3.2)37,38 to 33.0 (3.4) 41 kg/m2. Only one of the included studies specifically enrolled participants with T2D. 41 Additional studies targeted participants at elevated risk of T2D due to impaired fasting glucose (n = 2),44,52 elevated BP (n = 3),34,44,52 excess body fat (n = 1), 42 and overweight/obesity (n = 10).34–36,40,41,43,45,46,48–50,52
Intervention
All but one of the included studies examined the acute effects (4–10 hours) of breaking up SB in laboratory-based crossover RCTs. The remaining study was a 19-week community-based cluster RCT. 47 Methods of breaking up SB were variable and included standing, light intensity walking, moderate intensity walking, vigorous intensity walking, high intensity interval training, under-desk pedaling, stationary cycling, and resistance training. Studies included at least one and up to three36,52 methods of breaking up SB, most commonly light intensity walking (n = 10 studies)33,37–39,41–43,46,48,51,52 and standing (n = 6).33–35,43,45,51,52 SB break frequency varied substantially between studies, ranging from breaks every 20 minutes33,36,41–43,46 to every 120 minutes.37,38 Similarly, the length of each break was also variable, ranging from approximately 1.3 minutes 44 to 30 minutes.34,35,52 In addition to examining the effects of breaking up prolonged SB, a few studies (n = 3)36,42,49,50 also sought to compare the differential effects of one continuous bout of PA to multiple breaks in SB over the course of the intervention period. In every study, SB breaks were compared to a prolonged sitting condition or lack of intervention in the case of the community-based study. 47
Outcome measures
BP (SBP and DBP) was the most commonly reported vascular outcome, assessed in 16 of the included studies.33,34,36,39–49,51,52 Notably, few studies (n = 3) were specifically powered for any of the included vascular outcomes.36,38,42 Two studies were powered to evaluate the effects of the intervention on BP36,42 and one study was powered to detect changes in superficial femoral artery (SFA) FMD. 38 Although all studies included at least one vascular outcome, most also included glycemic control (e.g. postprandial glucose) as a primary (n = 10)33,36,39,41–44,46,51,52 or secondary (n = 1) 48 outcome. Popliteal and brachial artery FMD, calf circumference, cerebrovascular conductance, cerebrovascular carbon dioxide (CO2) reactivity, epinephrine, nitrates/nitrites, endothelin-1, intracellular adhesion molecule-1, and vascular cell adhesion molecule-1 were each only included in a single study and are therefore not reported on further.
The frequency of measurement of each outcome varied substantially. The most frequent assessment occurred in studies using ambulatory BP monitoring, where BP was recorded every 15 minutes (n = 2).33,36 Most commonly (n = 10), BP was measured hourly and immediately prior to a SB break.33–35,39,41,42,44–46,48,49 Three studies (assessing FMD37,43 and calf circumference 45 ) included pre- and post-measurements only.
Effect of break type on vascular outcomes
The effects of various break types on systemic vascular outcomes (i.e. SBP, DBP, MAP, heart rate), sorted by break intensity and observed response, are reported in Table 1. A total of six studies evaluated the impact of breaking up prolonged SB with standing on SBP,33,34,43,45,51,52 only one of which found a significant decrease in SBP in response to the intervention. 52 Similarly, there was no consistent effect of standing breaks on DBP.33,34,43,45,52
Acute effects of different break types on systemic vascular outcomes (e.g., SBP, DBP, MAP, HR).
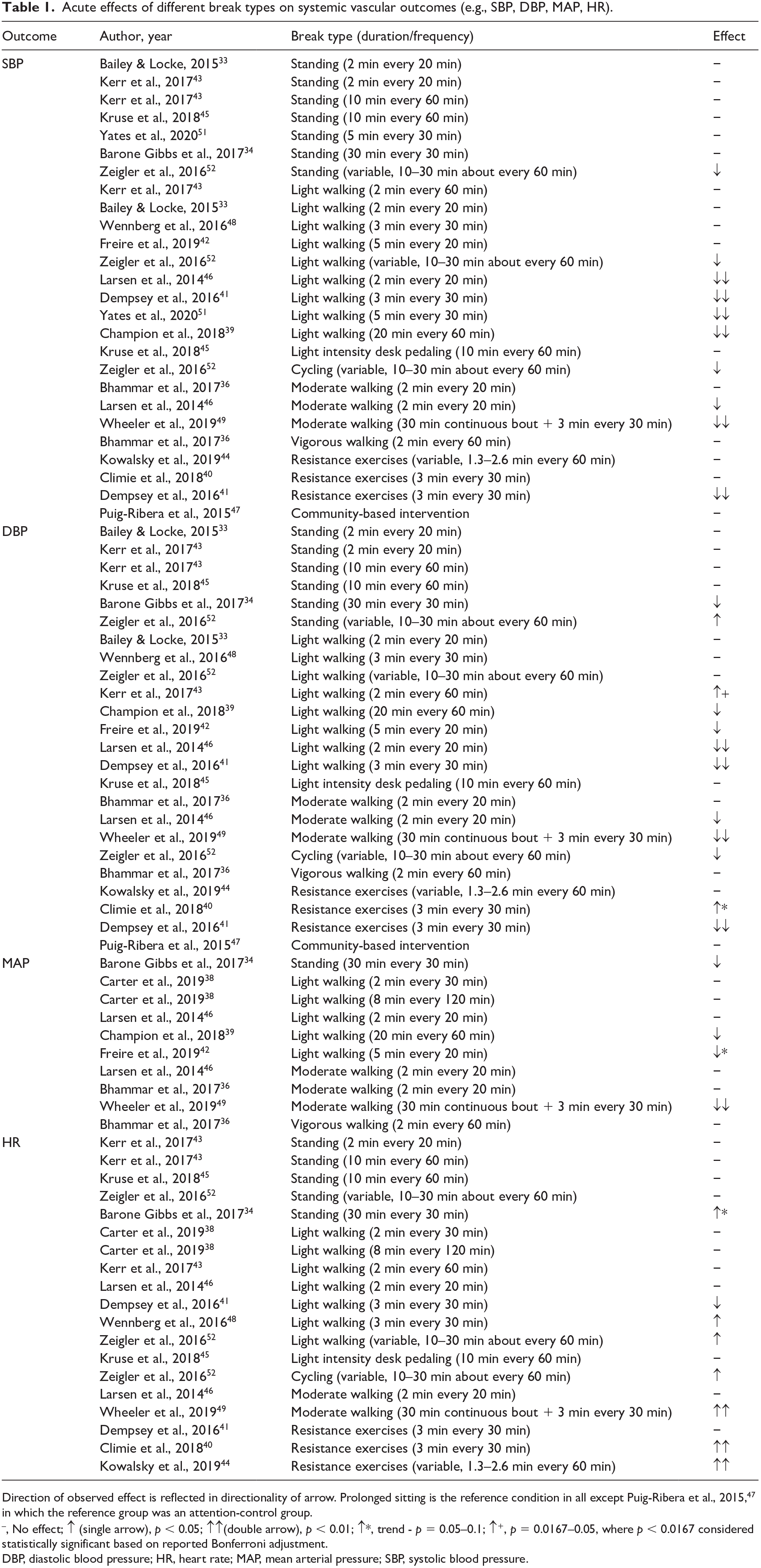
Direction of observed effect is reflected in directionality of arrow. Prolonged sitting is the reference condition in all except Puig-Ribera et al., 2015, 47 in which the reference group was an attention-control group.
−, No effect; ↑ (single arrow), p < 0.05; ↑↑(double arrow), p < 0.01; ↑*, trend - p = 0.05–0.1; ↑+, p = 0.0167–0.05, where p < 0.0167 considered statistically significant based on reported Bonferroni adjustment.
DBP, diastolic blood pressure; HR, heart rate; MAP, mean arterial pressure; SBP, systolic blood pressure.
Conversely, light and moderate intensity walking resulted in significant reductions in SBP in n = 5/939,41,46,51,52 and n = 2/336,46,49 of the included studies, respectively. Significant reductions in DBP were observed in n = 4/839,41,42,46 studies that evaluated light intensity walking and n = 2/346,49 of those that examined moderate intensity walking. There were no clear patterns with respect to the effect of SB break type on MAP or HR, with the exception that moderate walking and resistance training significantly increased average HR over the measurement period.40,44,49
The effect of different types of breaks on regional vascular outcomes (e.g. FMD, PWV, cerebral blood flow) are reported in Table 2. The most commonly assessed regional vascular outcome was SFA FMD (n = 3).38,40,43 There was no clear evidence of the effects of different types of breaks on SFA FMD, with significant improvement observed in only one 43 of the two studies38,43 that examined the effects of light intensity walking on SFA FMD. There was no evidence of an effect of SB breaks on PWV or middle cerebral artery blood flow velocity.
Acute effects of different break types on regional vascular outcomes (e.g. PWV, SFA FMD, cerebral blood flow).
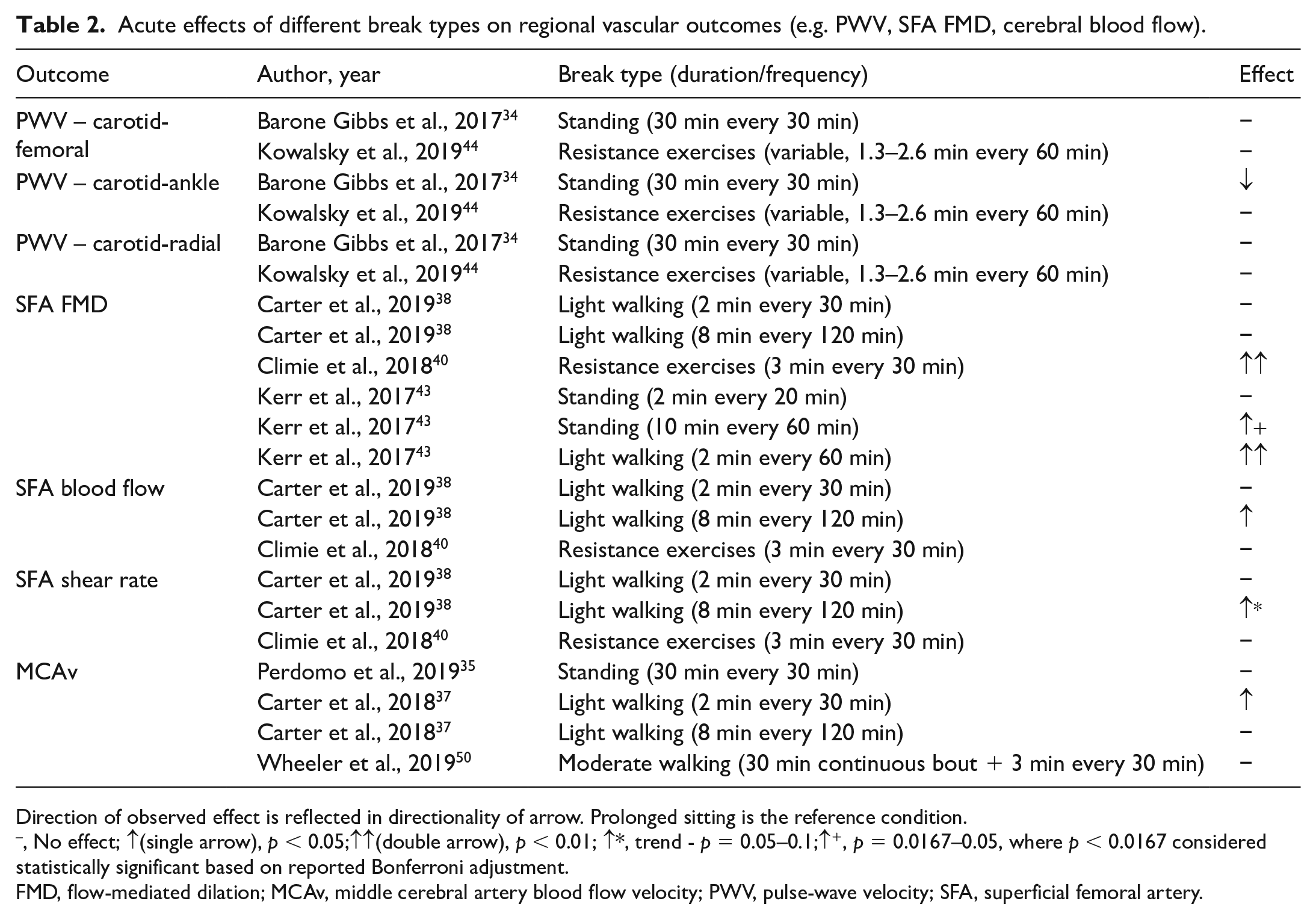
Direction of observed effect is reflected in directionality of arrow. Prolonged sitting is the reference condition.
−, No effect; ↑(single arrow), p < 0.05;↑↑(double arrow), p < 0.01; ↑*, trend - p = 0.05–0.1;↑+, p = 0.0167–0.05, where p < 0.0167 considered statistically significant based on reported Bonferroni adjustment.
FMD, flow-mediated dilation; MCAv, middle cerebral artery blood flow velocity; PWV, pulse-wave velocity; SFA, superficial femoral artery.
The impact of break type on norepinephrine, the only blood biomarker of vascular function included in two or more studies, is reported in online Supplemental Table 3. Although light walking and resistance training resulted in decreased norepinephrine in one study, 41 a second study found no effect of moderate intensity walking breaks on this biomarker. 49
Rigor of research
Key methodological considerations related to eligibility criteria and study conditions, and if they were adequately addressed, are reported in Supplemental Table 4. Some of the common issues identified were that few studies included objective measurement of PA and SB when evaluating whether a potential participant met eligibility criteria for sedentariness and physical inactivity (n = 4)42,48,51,52 and methods of assessment varied substantially (e.g., pedometer, wrist or hip-worn accelerometers). Additionally, menopausal status was not assessed objectively (via follicle stimulating hormone (FSH)) in any of the included studies and was reported in only five of the included studies.36,40,42,43,49,50 Regarding the intervention, less than half of the included studies obtained objective SB/MVPA data during each condition (n = 8)34–36,39,41,47,48,51,52 and timing of testing in relationship to female hormonal cycle was only documented in five of the included studies.36–39,44,45 Additionally, washout periods between conditions varied substantially (e.g., no reported washout period (i.e., all visits completed in a single 7-day period),37,38 visits separated by up to 14 days,34,35,41,44 and no reported upper limit on time between visits33,36,39,40,45,49,50) and guidelines regarding abstention from caffeine, alcohol, and smoking were inconsistent.
Risk of bias and quality of the evidence
Ratings of risk of bias for the included studies are reported in online Supplemental Table 5. Most of the included studies had potential bias related to lack of blinding of participants, personnel, and outcome assessors to experimental condition. Additionally, the presence of bias related to allocation concealment was unclear in most articles. Overall, the strength of the evidence is moderate to suggest a positive effect of light intensity walking and moderate intensity walking on BP, and insufficient for other SB break types and vascular outcomes.
Discussion
Our primary finding is that whereas standing alone was insufficient to acutely influence BP, breaking up prolonged SB with light and moderate intensity PA did result in lower SBP and DBP in adults with overweight/obesity. The data are insufficient to conclude whether other break types (e.g., high intensity aerobic activity or resistance training) have similar effects, the long-term effects of SB breaks, or the impact of the specific duration and frequency of the break. We did not find evidence of an effect of SB breaks on PWV and SFA FMD, likely in part due to the small number of studies that included these outcomes. Importantly, few of the included studies were adequately powered to evaluate the effects of SB breaks on the reported vascular outcomes, which limits our ability to draw clear conclusions.
Our results are consistent with those reported in a pooled analysis of four trials by Dempsey et al., which suggests that light walking breaks effectively lower BP acutely when compared to prolonged sitting. 53 The most substantial reductions in BP were observed in individuals with hypertension or prehypertension. 53 Limitations in the available data preclude a conclusion about the impact of SB breaks on FMD and PWV in adults at risk for T2D; however, the work of Paterson et al. 28 suggests that SB breaks may counteract the negative effects of prolonged sitting on lower extremity vascular dysfunction among healthy adults. As norepinephrine was the only blood biomarker of vascular health assessed in two or more studies,41,49 the effect of SB breaks on these outcomes is unknown.
Although exercise training is known to have a positive effect on vascular outcomes in individuals with overweight/obesity 54 and T2D, 55 the potential unique effects of intermittent breaks in SB versus one continuous bout of PA on BP, FMD, and other vascular outcomes remain unclear. Only three studies (four articles) directly compared the effects of SB breaks to a single continuous bout of activity (Supplemental Table 2).36,42,49,50 The available data support the conclusion that light and moderate intensity activity breaks have acute, positive effects on BP, similar to those observed with continuous bouts of PA in these studies. This is comparable to what has been observed in studies comparing multiple SB breaks to a single, continuous bout of PA with respect to glycemic outcomes. 56 A recent systematic review and meta-analysis of 26 studies comparing SB breaks to one bout of PA found that SB breaks moderately attenuated postprandial glucose, insulin, and triacylglycerol levels, with a small but signifcant advantage for SB breaks compared to continuous PA when energy expenditure was matched between conditions. 56 Additional studies are needed to evaluate if the effects of SB breaks are aligned with or different from improvements in vascular outcomes observed with exercise.
An important consideration in the interpretation of these studies is the relative homogeneity of the individuals in which SB breaks have been evaluated. There is a critical gap in understanding the vascular effects of breaking up SB in individuals other than healthy adults. Only one of the included studies specifically enrolled participants with T2D, 41 yet individuals with T2D are at highly elevated risk for significant CVD complications. Additionally, few studies enrolled individuals with elevated BP or hypertension. Given that the most robust intervention effects could be expected among individuals who have vascular dysfunction, evaluating methods of breaking up SB in this population is essential.
Study limitations
We identified some limitations with respect to the scientific rigor of the available studies. Importantly, whether some of the included vascular outcomes, such as PWV, are amenable to acute changes in SB is unclear. A wide variety of vascular outcomes have been reported in the literature, and, while we limited our analysis to outcomes assessed in two or more studies, future studies must carefully consider and justify which vascular measures should be included. Additionally, methods to assess key outcomes, including BP and FMD, were quite varied, making comparisons of the magnitude of change across studies difficult. Frequently, studies did not address female hormonal cycle and menopausal status, yet female sex hormones are known to influence cardiovascular outcomes 57 and responses to PA. 58 Additionally, few studies included an objective measurement of habitual PA and SB, yet being ‘sedentary’ was frequently included in the list of study eligibility criteria. Blinding of study participants and personnel was also a common issue. Though challenging, blinding of personnel and outcome assessors would ultimately increase confidence in the observed differences between interventions. Finally, the small number of studies, diversity of outcome measures, and variability in the study samples prohibit the examination of dose–response relationships or response in subpopulations of individuals such as older adults or women.
Recommendations and future directions: Call to action
The studies identified in this review were instrumental in laying the foundation regarding the effect of different types of breaks in prolonged SB on vascular outcomes in individuals with overweight/obesity or otherwise at an elevated risk for T2D, but extensive further research needs to be conducted in this area. First, it is critical that well-powered, rigorous studies are conducted to clearly examine the acute effects of breaking up SB on vascular outcomes, especially in populations at risk for vascular disease. Additionally, the relationship between the timing of testing and female hormonal cycle, use of caffeine/alcohol, and smoking must be considered. Researchers should also consider using objective measures such as accelerometry and posture monitors to assess SB and PA pre-intervention to quantify participants’ habitual physical behavior. For metabolic studies in humans, including standardized study design components, such as a ⩾ 7-day washout period between a control and intervention period, dietary controls, and matching energy expenditure could help eliminate some of these challenges and facilitate future meta-analyses. It would also be beneficial for the field to standardize the frequency/duration of breaks in SB, but this will require further study to come to consensus. To facilitate this standardization, we have developed a theoretical study design (Figure 2), based on our review and suggestions by Dunstan and colleagues, 59 with key issues that researchers conducting this work should consider.
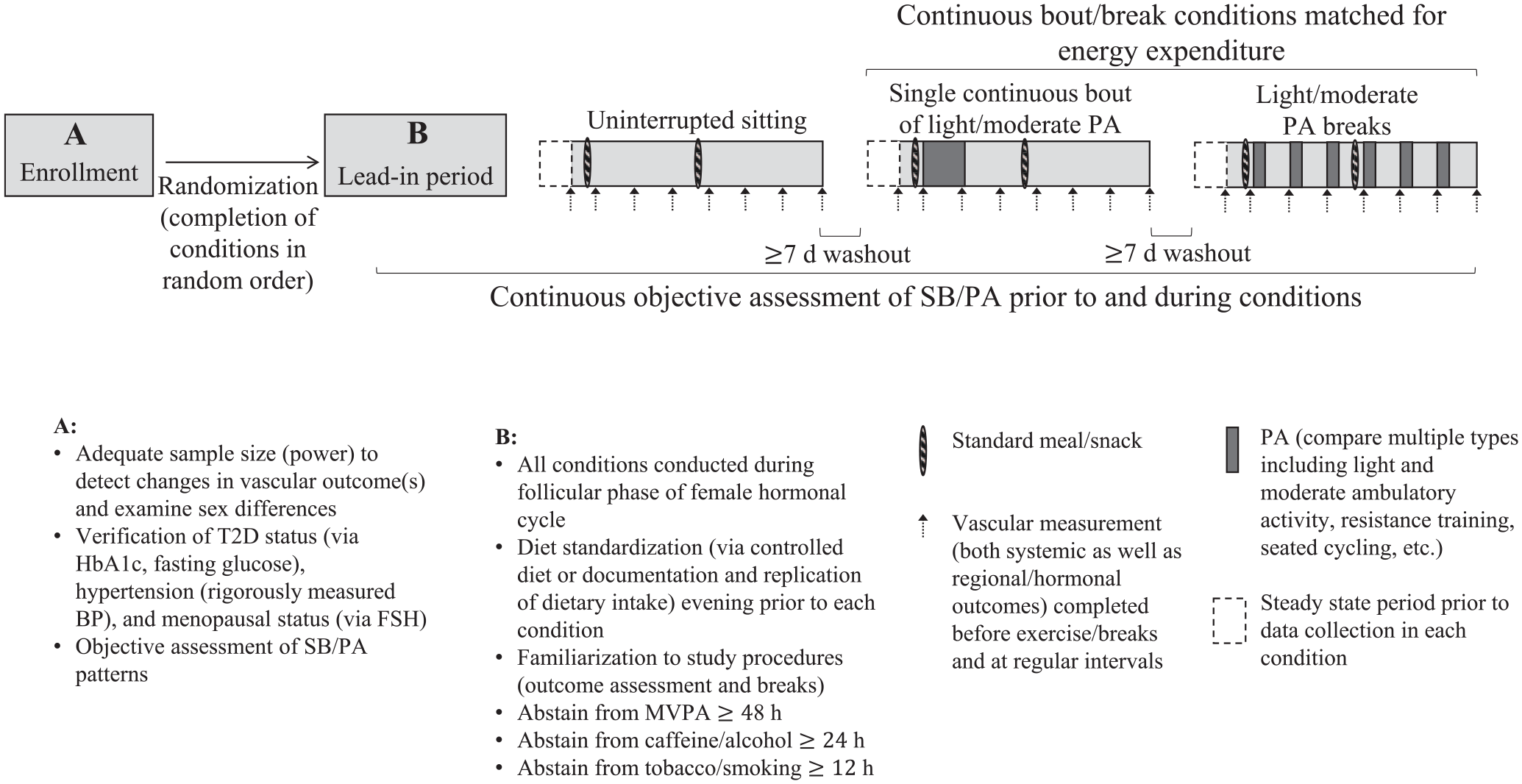
Schematic of theoretical study design to examine the effects of sedentary breaks on vascular outcomes in humans with key design characteristics we recommend researchers consider.
It is also unclear if the positive effects of SB breaks are sustained or diluted over time. Though acute, highly controlled, laboratory-based studies are important to evaluate the physiological impacts of different types of interventions, translation of these efforts into community-based interventions is needed to understand the real-world health effects as well as long-term effects of SB breaks on health. Additionally, it is essential to understand if the effects of SB breaks are population-dependent, including if there are sex-related differences in response. 60 Understanding the effects of SB breaks in older adults with hypertension and T2D is also of importance, as most studies have focused on young, healthy individuals.
Finally, it is important to understand whether the observed effects are due to multiple interruptions in SB or simply the result of an increase in total volume of PA/energy expenditure. Studies should compare light and moderate intensity breaks with matched energy expenditure between intervention groups, as well as investigate if there are differential effects of multiple breaks in SB when compared to a single continuous bout of exercise with the same duration of sedentary and active time. If similar outcomes are observed in light and moderate breaks (i.e. light activity is enough to induce favorable health effects), it could provide an approachable target for increasing PA, particularly among older adults and populations with chronic conditions, where a focus on MVPA may initially seem overwhelming or unattainable.
Conclusion
In summary, although there is some evidence to suggest that breaking up SB with light and moderate intensity walking has beneficial effects on BP for adults with overweight/obesity, the existing data are based on very few studies. The effects of other types of SB breaks (e.g. walking, cycling, resistance training) or impact of light/moderate intensity activity on other vascular outcomes is unclear. Our conclusions are tempered by the caveat that few studies have been adequately powered to examine vascular outcomes, individuals with risk factors for T2D other than elevated BMI have rarely been studied, and variability in the type, frequency, and duration of the breaks makes direct comparisons of the effectiveness of different break modalities challenging. Future rigorously designed studies should focus on individuals who are most vulnerable to the effects of SB, including diverse groups of older adults, office workers, and those with T2D and other risk factors for CVD, as these individuals tend to be highly sedentary and at greatest risk of poor health outcomes.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X211009307 – Supplemental material for Acute effects of sedentary breaks on vascular health in adults at risk for type 2 diabetes: A systematic review
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X211009307 for Acute effects of sedentary breaks on vascular health in adults at risk for type 2 diabetes: A systematic review by Mary O Whipple, Kevin S Masters, Amy G Huebschmann, Rebecca L Scalzo, Jane EB Reusch, Audrey Bergouignan and Judith G Regensteiner in Vascular Medicine
Footnotes
Acknowledgements
The authors would like to thank Ms Kristen Desanto, MSLS, MS, RD, AHIP, Clinical Librarian and Assistant Professor, University of Colorado Strauss Health Sciences Library for her valuable assistance in refining the database searches.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This publication was made possible by funding to Dr Whipple from the National Institute of Aging (NIA), NIH (T32AG000279, PI Schwartz), and the Center for Women’s Health Research; to Dr Masters from the Colorado National Obesity Research Center (P30DK048520); to Dr Huebschmann from the National Cancer Institute (NCI), NIH (P50CA244688, PI Glasgow); to Dr Scalzo from a Veterans Administration (VA) Career Development Award (BX004533); to Dr Reusch from VA BX002046, VA CX001532, NIH P30DK116073 (PI Reusch), NIH UL1TR000154 (PI Sokol), and the Center for Women’s Health Research; to Dr Bergouignan from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), NIH (R00DK100465, PI Bergouignan), and the Colorado National Obesity Research Center (P30DK048520); and to Dr Regensteiner from the Center for Women’s Health Research. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.