
Abstract
Background:
The effect of interarm blood pressure difference on the development of diabetic retinopathy, proteinuria and chronic kidney disease remains unknown. We investigated to determine the impact of interarm blood pressure difference on the prevalence of diabetic retinopathy, proteinuria and chronic kidney disease in patients with type 2 diabetes.
Methods:
The study included 563 patients with diabetes, who were evaluated with a simultaneous bilateral blood pressure measurement. The cutoff values for interarm blood pressure difference were 5, 10 and 15 mmHg. Logistic regression analysis was used to explore the relation between interarm blood pressure difference and diabetic retinopathy, proteinuria and chronic kidney disease.
Results:
Diabetic patients with systolic interarm blood pressure difference ⩾5, ⩾10 and ⩾15 mmHg showed an increased risk of diabetic retinopathy [adjusted odds ratio = 1.48 (95% confidence interval = 1.01–2.18), odds ratio = 1.80 (95% confidence interval = 0.99–3.22), odds ratio = 2.29 (95% confidence interval = 1.00–5.23)] after adjustment. There were significant associations between interarm blood pressure difference ⩾5 and ⩾10 mmHg and proteinuria [odds ratio = 1.68 (95% confidence interval = 1.15–2.44), 1.89 (95% confidence interval = 1.05–3.37)].
Conclusion:
The association between interarm blood pressure difference and the presence of diabetic retinopathy emerged even for systolic interarm blood pressure difference ⩾5 mmHg without interaction of systolic blood pressure. Systolic interarm blood pressure difference should be considered a surrogate marker for vascular complication in patients with type 2 diabetes.
Keywords
Introduction
Diabetic retinopathy (DR), one of the microvascular complications of diabetes, is a significant cause of vision loss and legal blindness in working-age adults. 1 While controlling other risk factors such as glycaemic levels and duration of diabetes, the effect of blood pressure (BP) on the development of DR remains unknown. Authors of the UK Prospective Diabetes Study (UKPDS) 2 recommended BP control as a means of preventing visual loss due to DR in patients with type 2 diabetes. Nevertheless, other studies, including the Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR), found no beneficial effect of intensive BP control on the progression of DR, suggesting that the benefit of preventing the progression of DR may be limited to uncontrolled high BP.3–5
An increased interarm blood pressure difference (IABPD) ⩾10 mmHg has been linked to an increased risk of cardiovascular disease (CVD), peripheral arterial disease (PAD) and mortality.6–8 IABPD ⩾10 mmHg is presented in approximately 2%–2.9% of the general population7,9 and in 9%–10% of patients with type 2 diabetes. 10 As this difference in the prevalence of IABPD may be associated with vascular diseases, it is necessary to investigate the relationship between IABPD and diabetic vascular complications. Several studies have demonstrated that IABPD may be associated with an increased risk of mortality and vascular complications in patients with type 2 diabetes.11,12 A previous study by Clark et al. 11 suggested that IABPD ⩾15 mmHg was associated with DR in heterogeneous type diabetes (type 1 diabetes, type 2 diabetes, steroid-induced diabetes and gestational diabetes). However, another study on IABPD and cardiovascular risks in patients with type 2 diabetes showed that IABPD ⩾10 mmHg might predict vascular damage such as arterial plaque; however, damage to some target organs, including transient ischaemia, coronary artery disease, left ventricular hypertrophy and DR, was unpredictable. 12 Systolic BP is not a significant predictor for DR or other diabetic vascular complications in patients with type 2 diabetes, 3 and there have been controversial results regarding the effect of IABPD on the occurrence of target organ damage.11,12 Therefore, we aimed to determine the effect of systolic IABPD on diabetic vascular complications, including the prevalence of DR, proteinuria and chronic kidney disease (CKD) in patients with type 2 diabetes.
Materials and methods
Patients and study design
This study included patients with type 2 diabetes who visited the Veterans Health Service Medical Center (Seoul, Korea) for diabetes care from August 2011 to March 2019. The study design was approved by the institutional review board (IRB No. 2019-09-007) of VHS Medical Center, and as this was a retrospective study, the requirement for informed consent was waived.
Eligibility was based on data from the Veterans Hospital Medical Information System (ezCaretech, Korea), which included pharmacy records, laboratory data, outpatient data, data on hospitalization and diagnoses of diseases; the data had been collected using a clinical data warehouse (CDW). Patients with type 2 diabetes (defined using codes E11.0–11.9 from the 10th revision of the International Statistical Classification of Diseases and Related Health Problems) who had attended follow-up examinations in the Veterans Health Service Medical Center were eligible subjects. Of these, only patients who had undergone IABPD measurement were included. The exclusion criteria were as follows: (1) missing data; (2) malignancies affecting diabetes progression (stomach, pancreas or kidney); and (3) patients who did not receive diabetes medications; and (4) patients diagnosed with a subclavian artery stenosis or abnormalities of the upper limb vasculature. Finally, the data of 563 patients were included in this study.
Baseline covariates included demographics (age, sex), body mass index, presence of hypertension, presence of dyslipidaemia, systolic BP (mean, higher), diastolic BP (mean, higher), creatinine, serum creatinine, estimated glomerular filtration rate (eGFR), proteinuria and comorbidities used. Dyslipidaemia was defined as total cholesterol 200 mg/dL and/or by the use of lipid-lowering treatment. Since we considered glycated haemoglobin <7% to indicate well-controlled type 2 diabetes, diabetes control was defined as glycated haemoglobin <7%.
Interarm blood pressure measurement
The ankle-brachial index (ABI) is broadly accepted as a screening tool for identifying the presence of PAD. It is a non-invasive and cost-effective assessment for patients with intermittent claudication. An ABI < 0.9 has a sensitivity of 90% and a specificity of 98% for detecting a lower-extremity arterial stenosis of greater than 50%. 13 High-risk patients older than 70 years, or aged 50–69 years with diabetes, or with a smoking history were subsequently enrolled and screened for peripheral arterial occlusive disease using the ABI. 13 Brachial BP was obtained as part of an ABI measurement by trained technicians according to a standard protocol: simultaneously in each of the four limbs using a non-invasive vascular screening device (VP-1000 Plus, Omron Co. Ltd., Kyoto, Japan) after a 5-min resting period with the patient’s arm placed at heart level (supine position). Measurements were taken twice in the following sequence: right arm, left arm, right ankle and left ankle. If the initial and repeat BP differed by 10 mmHg at any site, a third measurement was taken. The interarm systolic blood pressure difference was defined as the absolute difference between the single or average BP measurement in each arm. The cutoff values for systolic and diastolic IABPD were 5, 10 and 15 mmHg. The first screening data was obtained in the patients with repeated ABI measurements.
DR and other vascular complications
The vascular complications assessed in this study were the presence and severity of DR, CKD, proteinuria, coronary artery disease and previous stroke. Baseline comorbidities and vascular complications were extracted from the electronic medical record by ICD-10 codes: DR associated with type 2 diabetes mellitus (E11.30-11.38), ischemic heart disease (I20.0-24.9) and cerebrovascular disease (I60.0-69.0). In our hospital, DR was diagnosed in an ophthalmology outpatient clinic as no DR or DR (non-proliferative and proliferative) after a retinal examination or fundus photography of the dilated pupil. In addition, fluorescein angiography was performed to evaluate the presence of new vessels. The severity of DR was classified as no DR, mild non-proliferative diabetic retinopathy (NPDR), moderate NPDR, severe NPDR and proliferative diabetic retinopathy (PDR) according to the Early Treatment Diabetic Retinopathy Study guideline:14,15 the presence and extent of the hard exudates, cotton wools spots microaneurysms or haemorrhages due to leakage of fluid and blood from the vessels. 16 For the statistical analysis, the severity of DR was grouped into three categories: no DR, NPDR and PDR. Screening of DR was conducted based on international classification of DR as follows: re-examination in 1 year for no DR, 6–12 months for mild NPDR, 3–6 months for moderate NPDR and 3 months for severe NPDR or PDR. 16 Retinal examinations or retinal images from within 1 year after the ABI test were investigated for the relationship between IABPD and the presence and severity of DR.
CKD was identified using the eGFR according to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines. 17 The renal function was classified according to eGFR level (mL/min/1.73 m2): ⩾90 is CKD stage 1; 60–89 is CKD stage 2; 45–59 is CKD stage 3; 15–44 is CKD stage 4; and <15 is CKD stage 5. CKD stages 1–2 were considered normal renal function. Proteinuria was classified into four categories based on the results of a strip examination of a random specimen: negative-to-trace for 0–30 mg/dL, 1+ for 30–100 mg/dL, 2+ for 100–300 mg/dL and 3+ for >300 mg/dL. A negative-to-trace level of proteinuria was considered normal; other levels were considered to indicate significant proteinuria. 16
Statistical analysis
All data analyses were performed using SPSS version 21.0 (SPSS Inc. Chicago, IL, USA) and the R Statistical Package, Version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at p < 0.05. The chi-square test or Fisher’s exact test was used for categorical variables. Differences between the groups were analysed using one-way analysis of variance or the Kruskal–Wallis test; in the case of significant differences, a post hoc test was performed. Multiple logistic regression models were used to evaluate the association of systolic IABPD with the prevalence of DR, proteinuria and CKD. We fitted four models: (model 1), adjusted age and sex; (model 2), further adjusted for height, weight, hypertension, dyslipidaemia and diabetes control in addition model 1; (model 3) further adjusted for mean systolic BP in model 2; (model 4) further adjusted for mean systolic BP ⩾140 mmHg in model 2. When an association between variables was observed, a subgroup analysis and interaction test for heterogeneity in IABPD ⩾5 mmHg was performed, with subgroups defined according to mean systolic BP. With DR severity levels as dependent variables, IABPD ⩾5, ⩾10 and ⩾15 mmHg were examined by ordered logit regression, in which the proportional odds assumptions were assessed with Brant test and met for all models of DR severity. 18
Results
We studied 563 patients with type 2 diabetes: 532 (94.49%) men and 31 (5.51%) women. The baseline characteristics of the enrolled subjects are shown in Table 1. The mean age was 70.25 ± 6.50 years old; comorbidities included hypertension (83.66%) and dyslipidaemia (73.36%). The prevalence of systolic IABPD ⩾5 mmHg was 34.64% (n = 195), that of systolic IABPD ⩾10 mmHg was 9.77% (n = 55) and that of systolic IABPD ⩾15 mmHg was 4.44% (n = 25). The prevalence of diastolic IABPD ⩾5 mmHg was 15.99% (n = 90), that of diastolic IABPD ⩾10 mmHg was 3.02% (n = 17) and that of diastolic IABPD ⩾15 mmHg was 1.24% (n = 7). Vascular complications included DR in 28.77% (n = 162), CKD in 52.93% (n = 298), coronary artery disease in 64.65% (n = 364) and stroke in 31.44% (n = 177). DR was classified into mild NPDR (n = 67, 11.90%), moderate NPDR (n = 33, 5.86%), severe NPDR (n = 4, 0.71%) and PDR (n = 57, 10.12%). We merged mild NPDR, moderate NPDR and severe NPDR into the NPDR group. Patients with PDR had a higher mean systolic BP (p = 0.018) and lower eGFR (p = 0.024) compared to no DR group. Proteinuria (p = 0.002) and CKD (p = 0.042) were more prevalent in PDR patients. There were no differences in coronary artery disease and stroke between the DR groups.
Clinical characteristics of the study subjects.
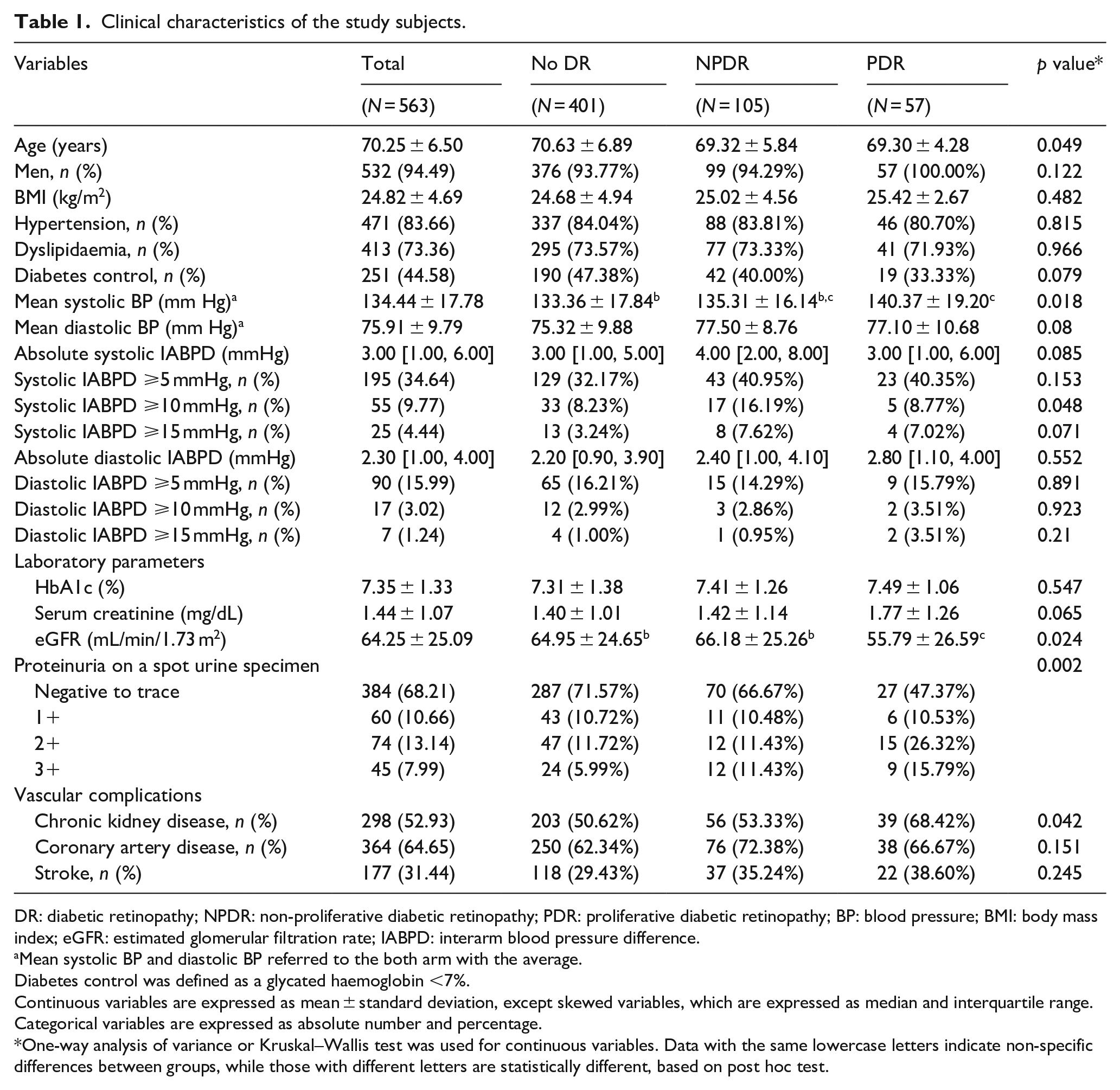
DR: diabetic retinopathy; NPDR: non-proliferative diabetic retinopathy; PDR: proliferative diabetic retinopathy; BP: blood pressure; BMI: body mass index; eGFR: estimated glomerular filtration rate; IABPD: interarm blood pressure difference.
Mean systolic BP and diastolic BP referred to the both arm with the average.
Diabetes control was defined as a glycated haemoglobin <7%.
Continuous variables are expressed as mean ± standard deviation, except skewed variables, which are expressed as median and interquartile range. Categorical variables are expressed as absolute number and percentage.
One-way analysis of variance or Kruskal–Wallis test was used for continuous variables. Data with the same lowercase letters indicate non-specific differences between groups, while those with different letters are statistically different, based on post hoc test.
Systolic IABPD and organ damage: DR, proteinuria and CKD
Diabetic patients with systolic IABPD ⩾5, ⩾10 and ⩾15 mmHg showed an increased risk of DR [odds ratio (OR) = 1.51, 95% confidence interval (CI) = 1.03–2.22; OR = 1.82, 95% CI = 1.00–3.25; and OR = 2.32, 95% CI = 1.01–5.31, respectively] in model 2 after adjusting for age, sex, height, weight, hypertension, dyslipidaemia and diabetes. However, the associations with systolic IABPD ⩾10 mmHg and the DR were not significant after adjusting for the mean systolic BP (model 3) (Table 2). Further analysis was performed after the mean systolic BP of both arms was set to 140 mmHg (model 4), since the effect of systolic BP is large and the effect of IABPD may be limited. Systolic IABPD ⩾5 and ⩾15 mmHg were associated with increased risk of DR severity (OR = 1.47, 95% CI = 1.01–2.15; OR = 2.22, 95% CI = 1.00–4.77, respectively) after adjusting for mean systolic BP (model 3).
Diabetic retinopathy, diabetic retinopathy severity, proteinuria, and CKD according to systolic IABPD.
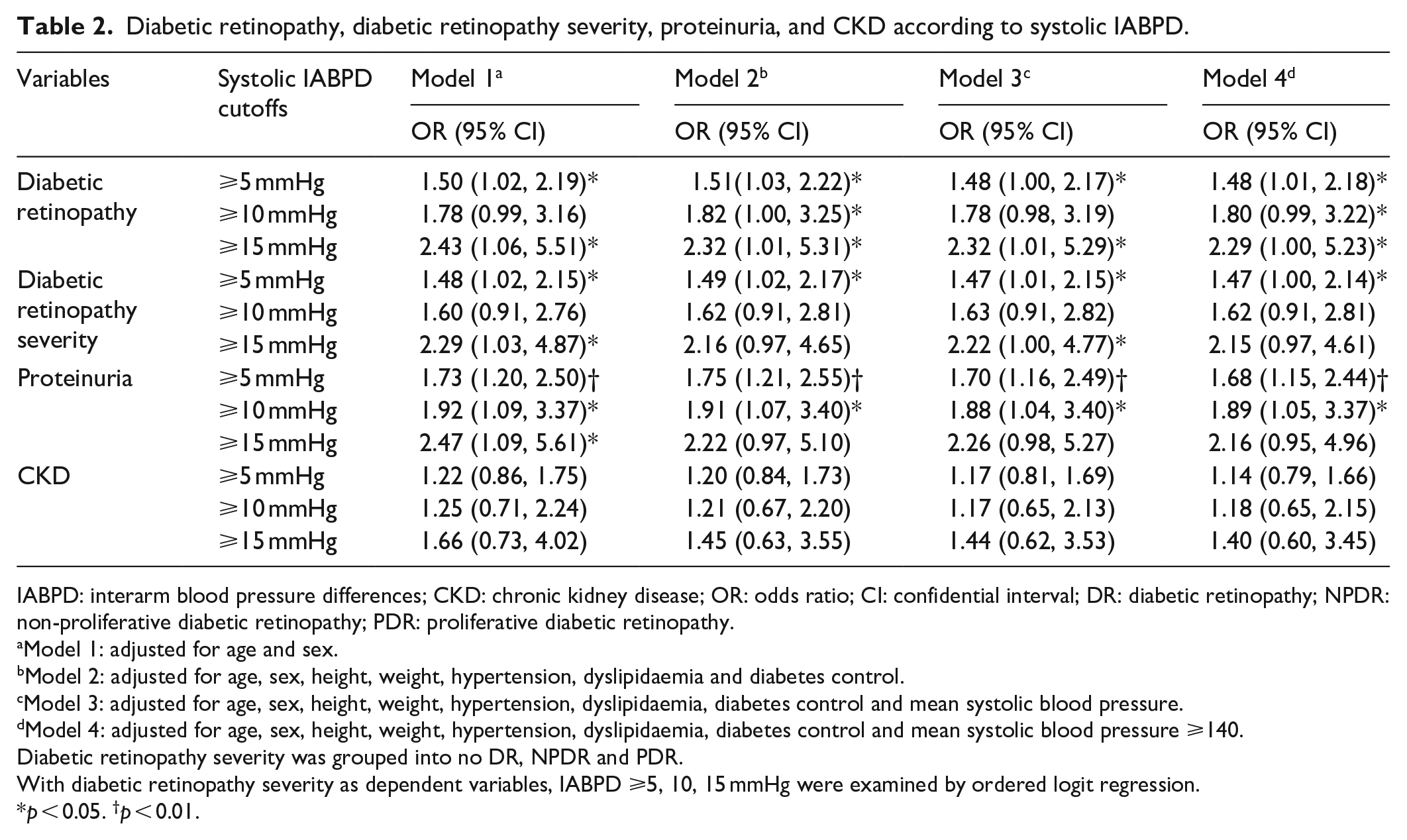
IABPD: interarm blood pressure differences; CKD: chronic kidney disease; OR: odds ratio; CI: confidential interval; DR: diabetic retinopathy; NPDR: non-proliferative diabetic retinopathy; PDR: proliferative diabetic retinopathy.
Model 1: adjusted for age and sex.
Model 2: adjusted for age, sex, height, weight, hypertension, dyslipidaemia and diabetes control.
Model 3: adjusted for age, sex, height, weight, hypertension, dyslipidaemia, diabetes control and mean systolic blood pressure.
Model 4: adjusted for age, sex, height, weight, hypertension, dyslipidaemia, diabetes control and mean systolic blood pressure ⩾140.
Diabetic retinopathy severity was grouped into no DR, NPDR and PDR.
With diabetic retinopathy severity as dependent variables, IABPD ⩾5, 10, 15 mmHg were examined by ordered logit regression.
p < 0.05. †p < 0.01.
Systolic IABPD ⩾5, ⩾10 and ⩾15 mmHg were associated with proteinuria (OR = 1.73, 95% CI = 1.20–2.50; OR = 1.92, 95% CI = 1.09–3.37; and OR = 2.47, 95% CI = 1.09–5.61, respectively) in model 1 after adjusting for age and sex (Table 2). In models 2, 3 and 4, systolic IABPD ⩾5 and ⩾10 mmHg were associated with proteinuria after adjustments. However, systolic IABPD was not associated with the presence of CKD.
Subgroup analysis and interaction test for systolic BP and systolic IABPD: DR, proteinuria and CKD
To determine if systolic BP and IABPD are related to the presence of DR, a distribution plot was drawn (Figure 1). Subgroup analysis and interaction test was performed to determine the effect of mean systolic BP and systolic IABPD independently on the presence of DR, DR severity, proteinuria and CKD (Figure 2). Study subjects were categorized by mean systolic BP at 140, 145 and 150 mmHg. Based on the interaction analysis for DR and DR severity, the p-values over 0.05 indicated that the systolic IABPD ⩾5 mmHg was associated with DR and DR severity independent of the mean systolic BP. However, for the presence of proteinuria and CKD, the systolic IABPD ⩾5 mmHg was significant in patients with a mean systolic BP ⩾140, ⩾145 and ⩾150 mmHg (p-value for the interaction < 0.05). These results suggested that there were differences in IABPD influence on proteinuria and CKD depending on the mean systolic BP.
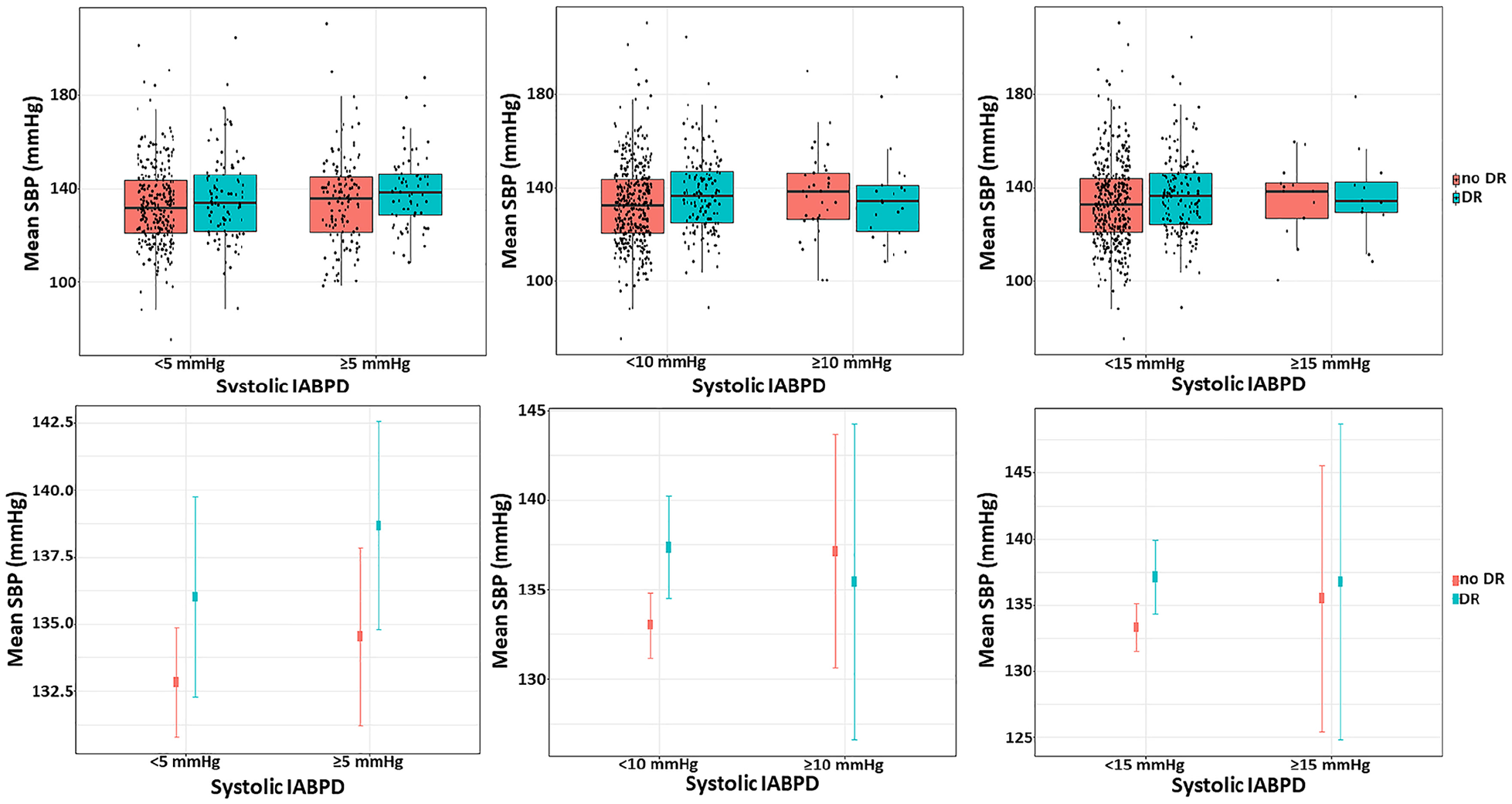
Distribution of mean systolic blood pressure in subjects with or without diabetic retinopathy when the cutoff values of the systolic IABPD are 5, 10 and 15 mmHg.
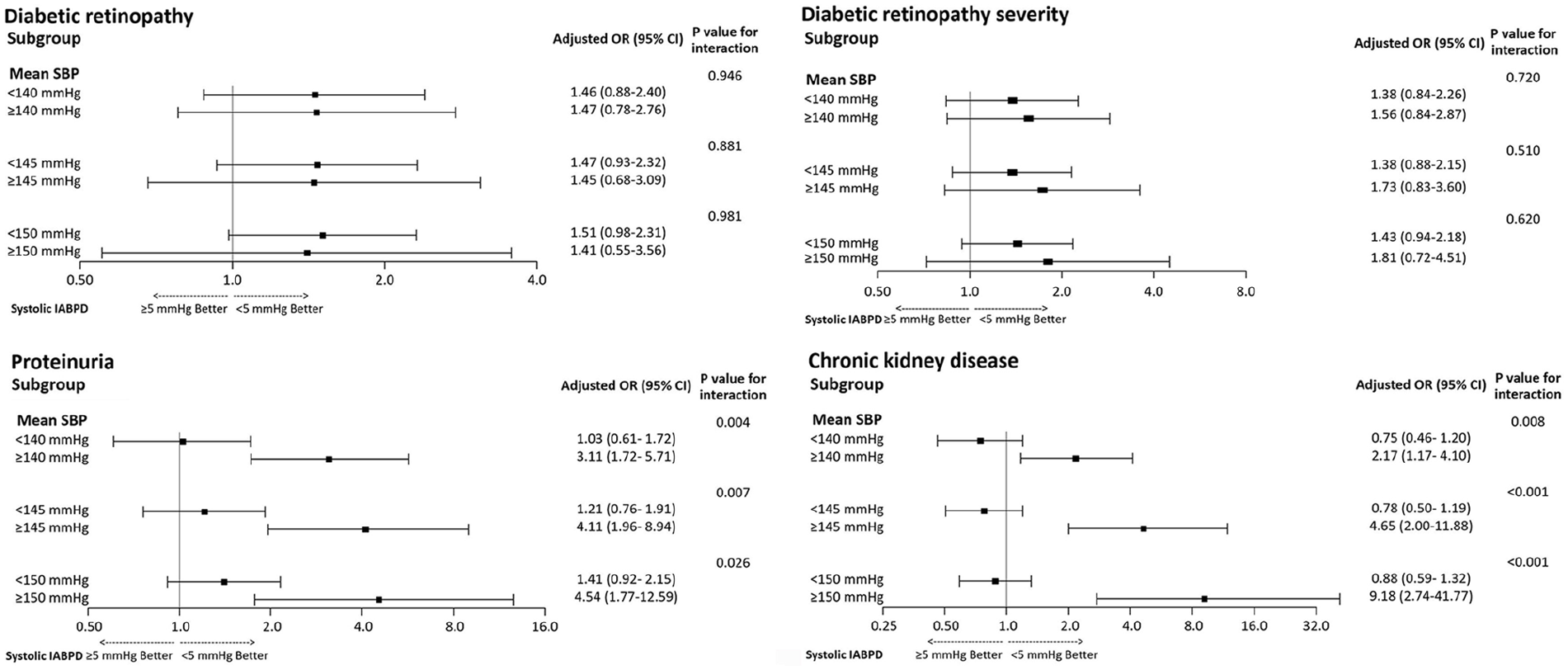
Interaction between mean systolic blood pressure and systolic interarm blood pressure difference: diabetic retinopathy, diabetic retinopathy severity, proteinuria and chronic kidney disease.
Discussion
Our results revealed a high prevalence of IABPD and a relationship between systolic IABPD and the presence of DR and proteinuria in patients with type 2 diabetes. The prevalence of systolic IABPD ⩾5 mmHg was 34.64%, that of IABPD ⩾10 mmHg was 9.77% and that of IABPD ⩾15 mmHg was 4.44%, which is consistent with the findings of previous studies on diabetes.10,12
Diabetes is a well-known risk factor of CVD; they share conditions such as subclinical atherosclerosis and dyslipidaemia, 19 for which IABPD may be a predictive factor. A previous study by Tanaka et al. 20 showed that IABPD might be a novel risk marker for subclinical atherosclerosis in patients with type 2 diabetes. Moreover, Clark 21 suggested that IABPD may be a marker for peripheral vascular disease. In our study, the patients with subclavian arterial stenosis or abnormality of the upper limb vasculature were excluded, which may affect the results of the study, since the previous study had shown that 6.7% of patients with subclavian stenosis showed a prevalence of IABPD ⩾25 mmHg. 8 Abnormal ABI below 0.9 is an independent marker for predicting PAD; in our study, two patients having IABPD greater than 30 mmHg had ABIs of 0.53 and 0.8, suggesting the possibility of PAD. Okada and colleagues 22 also suggested that a difference in systolic BP between arms and between lower limbs was correlated with albuminuria. Together, these findings indicate that IABPD may be correlated with micro- and macrovascular complications in patients with type 2 diabetes.
A previous study of IABPD in patients with type 2 diabetes 11 showed that IABPD ⩾15 mmHg was associated with the presence of DR [OR = 7.0 (1.4–35.0); p = 0.01] but not with the prevalence of CKD. These findings partially differed from our study in that the association of IABPD with DR was diluted with adjustment for covariates, including mean systolic BP. The reason for this is that our study was conducted using a veterans hospital cohort with mainly elderly male patients (mean age 70.25 years in our study vs 63 years in the previous study). 11 We also observed associations between systolic IABPD and systolic BP and relatively higher comorbidities [hypertension (83.7%) and dyslipidaemia (73.4%)]. Furthermore, Tanaka et al. 20 suggested in another study that IABPD was higher in patients with PDR than in those with no DR. However, these findings are of limited value, since the authors used only univariate analysis; they excluded retinopathy and nephropathy as potential confounding factors in multiple regression. On the other hand, Spannella et al. 12 suggested that systolic IABPD was associated with neither nephropathy nor retinopathy, which is differed with our results. In their study, they investigated vascular damages in a relatively large cohort of up to 800 subjects with type 2 diabetes. Although IABPD ⩾5 and ⩾10 mmHg were related to vascular damage (ORs 1.73 and 2.49, respectively), organ damage, including nephropathy, and retinopathy, was not fully explained by systolic IABPD alone. According to Quiroga et al., 23 increased systolic IABPD is an independent predictor of cardiovascular events in patients with CKD. Considering our finding that IABPD was correlated with proteinuria in addition to higher systolic/diastolic BP, it would be reasonable to infer that there are common underlying mechanisms, including age, dyslipidaemia, diabetes and hypertension. Hypertension increases the risk of vascular complications in patients with diabetes via several putative mechanisms, such as up-regulation of the renin–angiotensin–aldosterone system, endothelial dysfunction, oxidative stress, inflammation and advanced glycation end-products. 24 Clinically, it is difficult to separate systolic IABPD and systolic BP; in a systemic review and meta-analysis of the prevalence of IABPD, Clark et al. 9 reported that they vary depending on the characteristics of the study subjects.
As IABPD may reflect subclinical atherosclerosis, researchers may be interested in the association between DR and atherosclerosis. The early stage of DR is characterized by vessel hyperperfusion. 25 The elevated blood flow is likely to increase shear stress and cause vessel damage, which leads to endothelial dysfunction, disruption of the basement membrane and extracellular matrix remodelling.26,27 In a study by Liu et al., 28 the presence of DR was significantly associated with subclinical atherosclerosis (OR = 1.93, 95% CI = 1.03–3.60). This is consistent with the results of a study by Son et al., 29 which showed an association between subclinical atherosclerosis and DR in patients newly diagnosed with diabetes. The associations between DR and the carotid artery intima media thickness and arterial stiffness were independent of age, duration of diabetes and HbA1c. 30 DR alone or in combination with diabetic nephropathy was associated with carotid artery plaques in type 2 diabetic patients. 31 Although the mechanism of IABPD and micro-macrovascular complications remains unexplained, part of this correlation is mediated by arterial stiffness. 32 Significant IABPD was associated with carotid-femoral pulse wave velocity in the Baltimore Longitudinal Study of Aging. 32 Increased arterial stiffness and narrowing of the arterial lumen cause differences in waveform reflection. 33 Yun et al. 34 showed that DR was associated with the arterial stiffness as measured by the brachial ankle pulse wave velocity. In this study, however, the sample was too small to assess of involvement of DR and atherosclerosis; this could be solved with the analysis of a larger cohort. In this regard, the authors suggest that the results of this study could be supplemented.
A major strength of this study was the large cohort. Moreover, the available medical records included information on comorbidities. However, our study had several limitations. First, the patients in the veteran’s medical centre were predominantly male, and more than 80% of the veterans were older than 65 years of age. Older adults with multiple comorbidities are at substantial risk for diabetic vascular complications. The application of our findings to the general population must be done with caution. Second, given that our data are from a single centre, the results should be confirmed in community-based studies. Third, interaction analysis was performed to determine the independent effect of the mean systolic BP and systolic IABPD on the DR. This subgroup analysis decreased the sample size, which suggests a reason for the insignificant OR result. Fourth, the cross-sectional study design did not allow us to determine a cause–effect relationship. As this study was a retrospective review, it was difficult to determine atherosclerosis risk factors such as smoking habits. Further research including atherosclerosis risk factors has been prospectively designed to determine the relation of systolic IABPD to DR, proteinuria, and CKD prevalence and mortality.
Conclusion
Our findings suggest an association between systolic IABPD and the presence of DR and proteinuria. We observed a relationship between DR and systolic IABPD ⩾5, ⩾10 and ⩾15 mmHg, after adjusting for covariates. Further analysis showed that both of systolic mean BP and IABPD independently affected the prevalence of DR. A systolic IABPD ⩾5 and ⩾15 mmHg was associated with increased severity of DR. Proteinuria was associated with IABPD ⩾5 and ⩾10 mmHg after adjustments. Hence, systolic IABPD could be considered a surrogate marker for vascular complication in patients with type 2 diabetes.
Footnotes
Author contributions
J.H.L. contributed to study design and conception, and had full access to all data in the study and take responsibility for integrity of the data and writing the manuscript. Y.A.K. contributed to data acquisition, data analysis and interpretation, and manuscript revision. Y.L. contributed to data analysis and interpretation, had full access to all data in the study and take responsibility for integrity of the data and writing the manuscript. W.-D.B. contributed to data analysis and interpretation, and writing the manuscript. J.H.S. contributed to study design and conception, data analysis and interpretation, writing the manuscript and revision of the manuscript. All the authors approved the final version of the manuscript to be published. J.H.S. is the guarantor of this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval and consent to participate
The study design was approved by the Veterans Health Service Medical Center institutional review board (IRB No. 2019-09-007). As this was a retrospective study, the requirement for informed consent was waived and was conducted in accordance with Declaration of Helsinki.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by a VHS Medical Center Research Grant, Republic of Korea (grant number: VHSMC17036). The funding organization had no role in the design or conduct of the study; collection, management, analysis or interpretation of the data; preparation, review or approval of the manuscript; or decision to submit the manuscript for publication.