
Abstract
The aims of this study were to analyze the results of inframalleolar bypass for chronic limb-threatening ischemia (CLTI) and to identify outcome-predicting factors. All consecutive patients undergoing inframalleolar bypass for CLTI between 2015 and 2018 were included in this retrospective, single-center study. Outflow artery was the most proximal patent vessel segment in continuity with inframalleolar arteries. Bypasses originating from the popliteal artery were defined as ‘short bypasses’. Sixty patients underwent inframalleolar bypass, with four patients undergoing bilateral procedures, making a total of 64 limbs included. The mean age was 73 ± 14 and 52 (81%) were male. The great saphenous vein was the preferred conduit (n = 58, 91%), in a devalvulated fashion (n = 56, 88%). Superficial femoral artery was the most common inflow artery for ‘long’ grafts (n = 22, 34%), while popliteal artery was the inflow artery for all ‘short’ grafts (n = 25, 39%). Dorsalis pedis artery was chosen as an outflow artery in 41 patients (63%). Median follow-up was 21 months. Two-year primary and secondary patency, limb salvage, amputation-free survival, and overall survival rates were 67 ± 6%, 88 ± 4%, 84 ± 4%, 72 ± 6%, and 85 ± 4%, respectively. At multivariate analysis, dialysis was an independent predictor for poor primary patency (HR, 4.6; 95% CI, 1.62–13.05; p = 0.004), whereas a short bypass was independently associated with an increased primary patency (HR, 0.3; 95% CI, 0.10–0.89; p = 0.03). In conclusion, bypass grafting to the inframalleolar arteries resulted in good patency rates, limb salvage and overall survival. Dialysis patients had lower primary patency but still had good limb salvage and survival. Short bypass was a predictor of improved primary patency.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI) is characterized by rest pain and tissue loss (Rutherford category 4–6, stages 2–4, according to the Wound, Ischemia and foot Infection (WIfI) classification), such as ulcers and gangrene. CLTI leads to lower limb amputations in 40% of patients and an annual mortality rate of 20%, if not treated.1–3 The best treatment for patients with CLTI is revascularization.
Open surgical revascularization is advisable in patients with high anatomic complexity lesions and WIfI stages 3 or 4. 3 However, its feasibility is dependent on different factors, among which the most important are the availability of good quality autologous venous material, outflow artery patency and specific surgical expertise. 4 Moreover, open surgical revascularization is burdened by a non-neglectable perioperative complication rate. 5
In our retrospective study, we included patients with Rutherford category 4–6 who underwent dorsalis pedis or plantar vessels bypass. The aim of our study was to analyze the patency, limb salvage and survival rates of this class of patients and to investigate the predictive role of associated risk factors.
Materials and methods
Patient cohort
A retrospective single-center study was conducted including all consecutive patients who underwent inframalleolar lower limb bypass for CLTI between January 2015 and December 2018 at the Vascular Surgery Unit of the University Hospital Gaetano Martino, Messina, Italy. CLTI was defined as peripheral artery occlusive disease with rest pain (Rutherford category 4) and/or trophic disorder, ulcer or gangrene (minor tissue loss, nonhealing ulcer, or focal gangrene: Rutherford category 5; major tissue loss extending above the transmetatarsal level: Rutherford category 6). 1 Inframalleolar bypass was defined as infrainguinal bypass to arteries below the tibio-tarsal level (i.e. dorsalis pedis artery and common plantar artery). 4 Patients who had undergone previous endovascular revascularization were also included. Patients undergoing inframalleolar bypasses for indications other than CLTI (acute or subacute limb ischemia, Buerger’s disease or other vasculitis) were excluded from this study. Patients who had no venous material available and underwent distal bypass with polytetrafluoroethylene (PTFE) graft with arteriovenous fistula according to Ascer’s technique were also excluded. Composite bypasses were not excluded.
This study is in agreement with the principles outlined in the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board. All patients gave a written informed consent to participate in the study.
Preoperative protocol
All patients underwent a preoperative blood test, evaluation of cardiological status, and a physical examination evaluating the proximal and distal pulse and presence of trophic disorders. The planning of the procedure was based on thorough duplex ultrasound arterial mapping. Angiography was performed only in cases of technical difficulties that hindered adequate ultrasound imaging. 6 Target artery and vein diameters were measured in B-mode on a transverse plane by ultrasound scan, with the patient in a supine position. Vein-graft compressibility, thickness and continuity were assessed. The great saphenous vein was the preferred conduit when available, followed by the small saphenous vein. When lower limb venous material was not available or not long enough, composite bypass using a heparin-bonded PTFE graft were performed (Propaten; WL Gore & Associates, Inc., Flagstaff, AZ, USA). Venous material was considered of good quality when it was at least 3 mm in diameter, did not present ectasia or post-phlebitic alterations. Nonetheless, veins with smaller diameter or with minor alterations were also used in the absence of good quality material. Inflow and outflow vessels were selected based on vessel patency.
Inflow artery was the last patent vessel with regular morphological status, and triphasic waveform at Doppler examination. Outflow artery was the most proximal patent vessel segment in continuity with inframalleolar arteries. Inflow arteries used were: external iliac artery, common and superficial femoral artery and popliteal artery. Outflow vessels were arteries under the tibio-tarsal level (inframalleolar arteries).
Vein and artery characteristics were evaluated with duplex ultrasound imaging with a 7 MHz linear probe at a 60° insonation angle.
Patients were deemed unsuitable for inframalleolar bypass surgery if they were permanently bedridden or had one of the following anatomical criteria: simultaneous absence of a good quality great saphenous vein, and small saphenous vein; no inframalleolar patent vessel; ulcer/gangrene extended above the ankle; were under optimal medical treatment, which included acetylsalicylic acid statin. Dual antiplatelet therapy with clopidogrel 75 mg was generally limited to patients with concomitant coronary artery disease.
General anesthesia, epidural, nerve blockade, local anesthesia, or a combination thereof were used.
Surgical technique
Patients with occlusion or severe stenosis of all three leg vessels down to the intermalleolar plane and with adequate venous material available were proposed inframalleolar bypass targeted to the dorsalis pedis artery or the plantar arch (Figure 1).
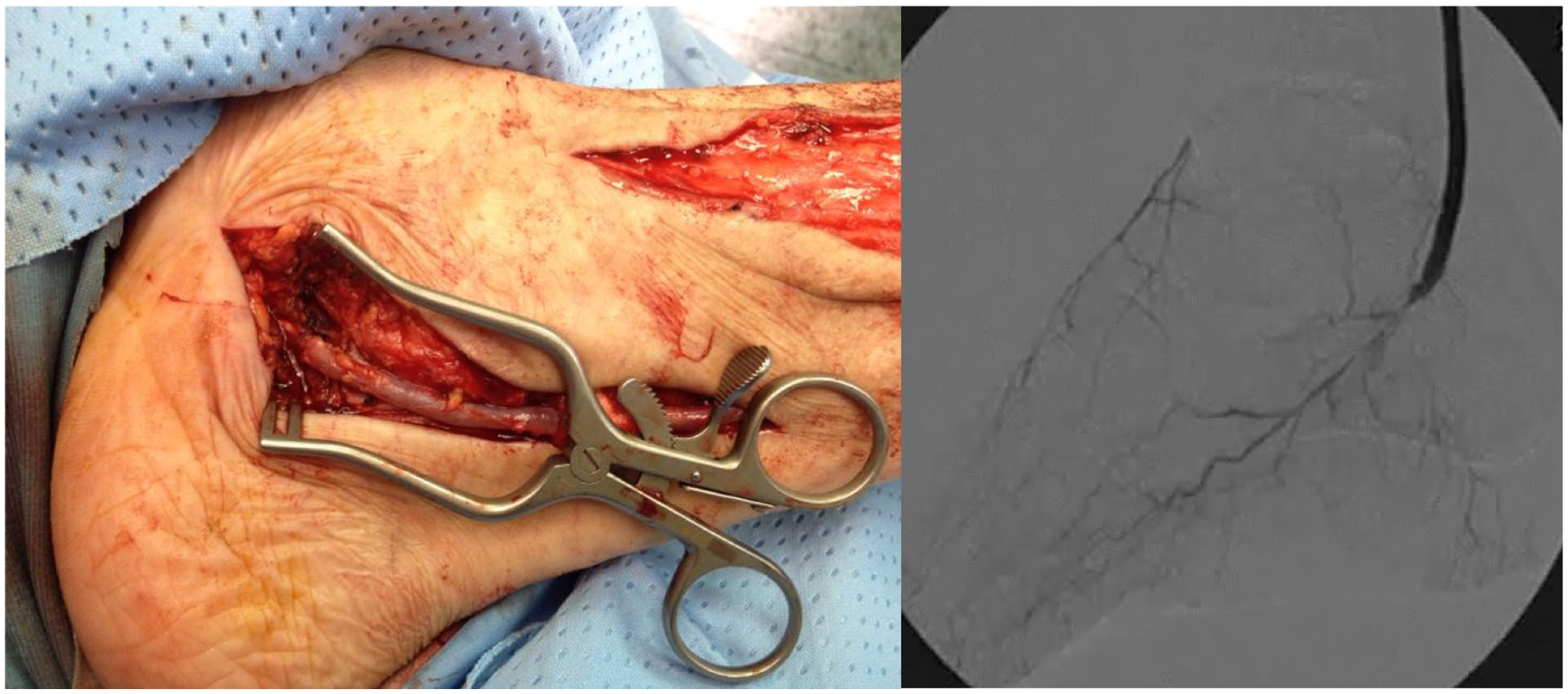
Detail of the distal anastomosis of a bypass to common plantar artery and angiogram showing the anastomosis and the distal runoff.
For bypasses targeting the dorsalis pedis, the vein was tunneled through the interosseous membrane. Patients received anticoagulation before arterial clamping (50 UI/kg). The valve lysis was carried out using the Chevalier Valvulotome (LeMaitre Vascular, Inc., Burlington, MA, USA). The distal anastomosis was usually performed without putting a clamp on the distal part of the artery in order to avoid trauma to the tiny heavily calcified vessel. The backbleeding was reduced by putting the patient in an extreme Trendelenburg position, with the head raised to avoid discomfort. Then, the distal occlusion was achieved by gentle external compression with a finger.7–9
All surgeons in our unit were trained to use binocular magnifier glasses, which were used for performing the distal anastomosis. When suturing the wound at the level of distal anastomosis, special care was taken not to put tension on the wound edges.
The adequacy of bypass was evaluated intraoperatively with duplex ultrasound.
Postoperative management
During the postoperative course, limb elevation was maintained in order to limit limb edema. All patients were discharged with single antiplatelet therapy, unless dual antiplatelet therapy was indicated for concomitant cardiovascular disease or prosthetic graft. Follow-up with duplex ultrasound at 1, 3, and 6 months and every 6 months thereafter was performed. Patients with necrotic lesions underwent surgical debridement or minor amputation as needed in the same operation or in the following days and were followed up with ambulatory wound care weekly.
Outcomes
Primary outcomes included 2-year primary patency and limb salvage. Secondary outcomes included 2-year overall survival, amputation-free survival, assisted primary patency, secondary patency, and functional status.10,11 Outcomes were defined according to Rutherford reporting standards. 1 Demographic variables and cardiovascular risk factors, such as smoking, hypertension, diabetes, and renal insufficiency were recorded. A long bypass was defined as any bypass originating proximal to the popliteal artery. A short bypass was defined as any bypass originating from the popliteal artery.
Statistical analysis
Patient demographics, comorbidities, clinical and anatomical characteristics (artery and vein diameters), procedure-related data, complications, and outcomes were collected in a dedicated Excel (Microsoft, Redmond, WA, USA) database.
Continuous variables were reported as mean ± SD or median with range as appropriate. Categorical variables were reported as counts (percentages). Statistical analysis was performed using R (The R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org/). Life table analysis was used to estimate time-to-event outcomes (cumulative bypass graft patency, limb salvage, and survival). Subgroups were compared with log-rank test. A Cox proportional hazard model was built to identify variables predictive of loss of patency, amputation, and death.
Multivariate models were built using a stepwise procedure to select predictive variables. Factors were identified at univariate analysis as being significantly associated with the survival endpoint. The significance levels for explanatory variables entry (SLE) and for stay (SLS) were set to 0.25. Hazard ratios are presented with 95% CIs. A significance level of 0.05 was used for all statistical tests.
Results
Patient cohort and risk factors
Between January 2015 and December 2018, 545 patients underwent lower limb revascularization procedures at our center. Out of 545, 253 (46.4%) were treated with infrainguinal bypass. Sixty patients matched the inclusion criteria for inframalleolar bypass, with four patients undergoing bilateral procedures, for a total of 64 limbs included. All limbs matched the criteria for CLTI. 3 Fifteen patients had undergone previous endovascular revascularization procedures. These involved treatment of the inflow artery in eight cases (six superficial femoral arteries proximal to a popliteo-distal bypass, two iliac arteries). Risk factors and comorbidities are reported in Table 1.
Patient demographics and risk factors (N = 64).
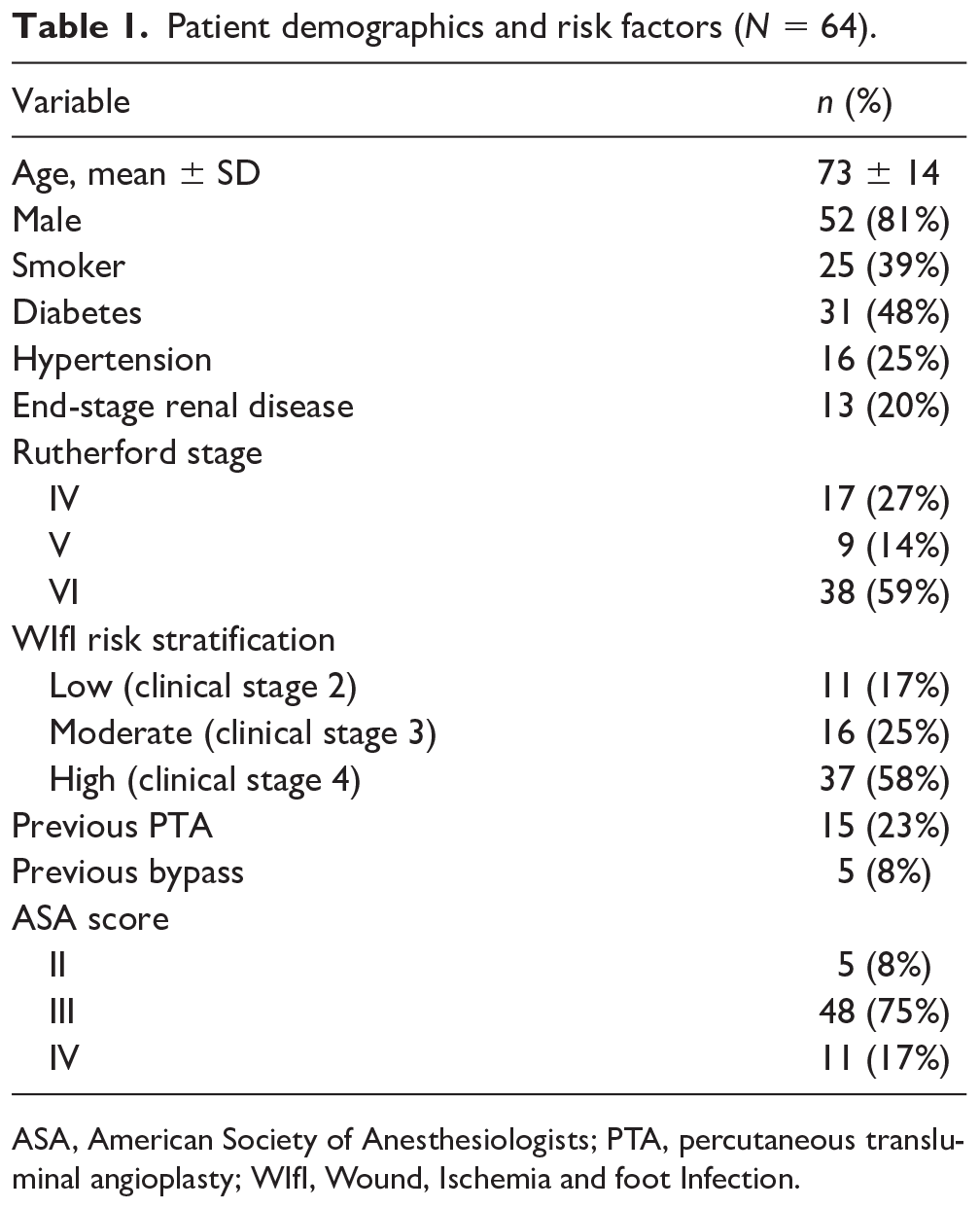
ASA, American Society of Anesthesiologists; PTA, percutaneous transluminal angioplasty; WIfI, Wound, Ischemia and foot Infection.
Operative details
Most of the bypasses (59) were performed using only autogenous vein graft. In five cases, in which autogenous vein material was insufficient, a composite prosthetic graft was performed using the vein (a segment of great saphenous vein in all five cases) for the distal part of the graft. Great saphenous vein was the preferred conduit (n = 63, 98%, including five composite), in a devalvulated fashion (n = 56, 88%), while the reversed vein was used in eight (12%) cases (Table 2). Vein graft diameter ranged from 2.3 mm to 3.5 mm. Thirty-nine (61%) bypasses were long and 25 (39%) were short. Superficial femoral artery was the most common inflow artery for long bypasses (n = 22, 34%), while popliteal artery was the inflow artery for all short grafts (n = 25, 39%). Short bypasses were performed significantly more frequently on diabetic patients (55% vs 24%, p = 0.012). Dorsalis pedis was chosen as an outflow artery in 41 patients (63%) (Table 2). Outflow artery diameter ranged between 1.5 mm and 2.2 mm. Three patients had surgical wound dehiscence at mid or proximal leg, which was treated with debridement and vacuum assisted closure (VAC) therapy. Two of these patients required a bypass revision at 3 months to maintain patency. Thirty-four patients underwent minor amputation: four limited to toes, 18 toes extended to transmetatarsal level, 12 complete transmetatarsal. Forty-seven (73%) patients were discharged with single antiplatelet therapy and 17 (27%) patients were discharged with dual antiplatelet therapy due to concomitant cardiovascular disease.
Operative details (N = 64).
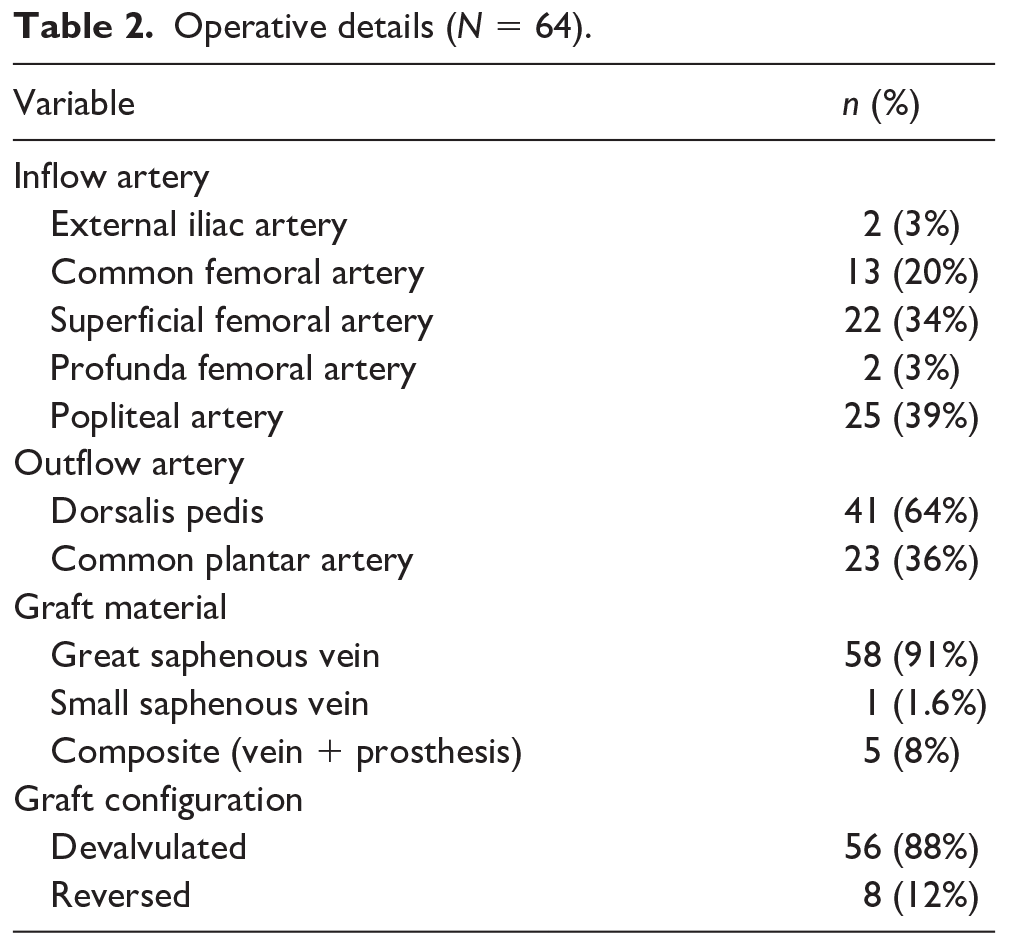
Data are presented as n (%).
Follow-up outcomes
The median follow-up was 21 months (range 0–48 months). Two-year primary, assisted primary, and secondary patency rates were 67 ± 6%, 86 ± 4%, and 88 ± 4%, respectively. Two-year limb salvage, amputation-free survival, and overall survival were 84 ± 4%, 72 ± 6%, and 85 ± 4%, respectively (Table 3). A statistically significant difference in primary patency was seen between patients on dialysis and patients not on dialysis (p < 0.02; Figure 2), although no difference was found in terms of secondary patency and limb salvage between these subgroups. The limb salvage rate was significantly better in men compared to women (p < 0.003) and in patients who were smokers before surgery compared to non-smokers (p = 0.05). No significant difference in terms of outcomes was observed for patients who had undergone previous endovascular or surgical treatment. The use of a composite graft was not associated with significantly different outcomes (data not shown). Amputation-free survival is reported in Figure 3. At multivariate analysis, dialysis remained a statistically significant independent predictor for poor primary patency (hazard ratio (HR), 4.6; 95% CI, 1.62–13.05; p = 0.004), whereas a short bypass (i.e. originating from popliteal artery) was independently associated with an increased primary patency (HR, 0.3; 95% CI, 0.10–0.89; p = 0.03) (Figure 4).
Follow-up outcomes.
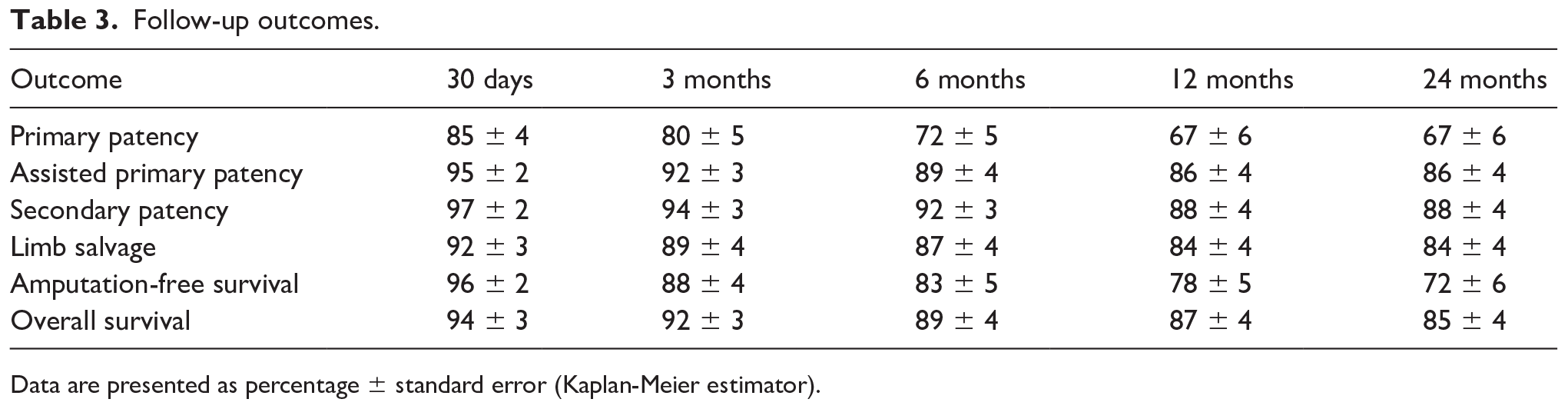
Data are presented as percentage ± standard error (Kaplan-Meier estimator).
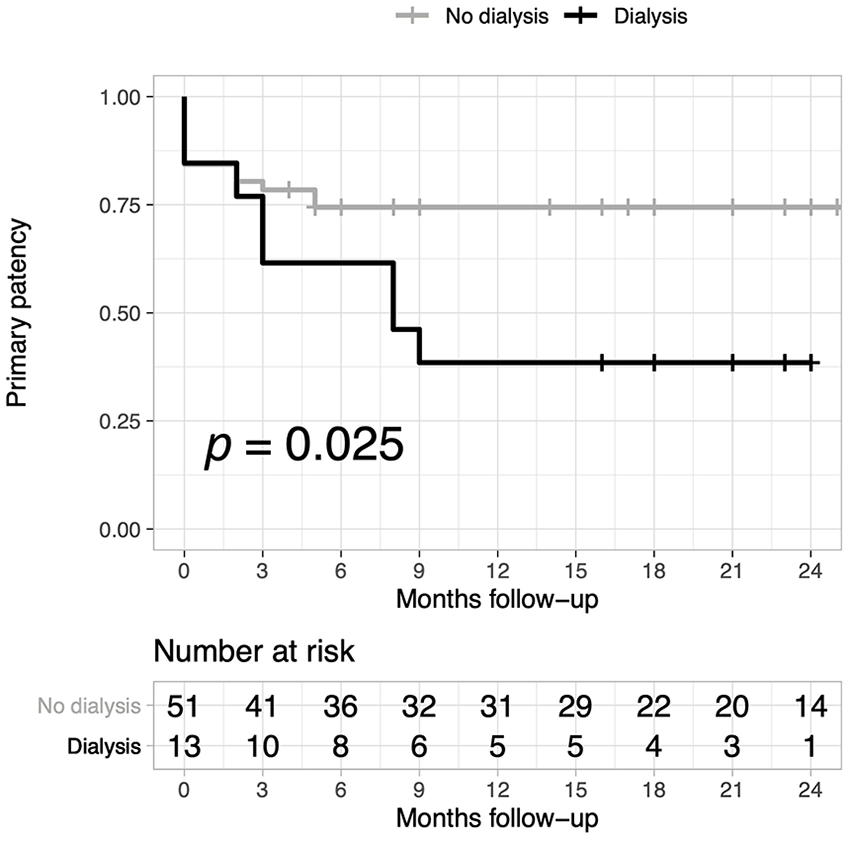
Primary patency by dialysis status. Primary patency rates ± standard error for the dialysis group were: 85 ± 10, 77 ± 12, 61 ± 14, 46 ± 14, 39 ± 14 at 1, 3, 6, 12, 24 months, respectively.
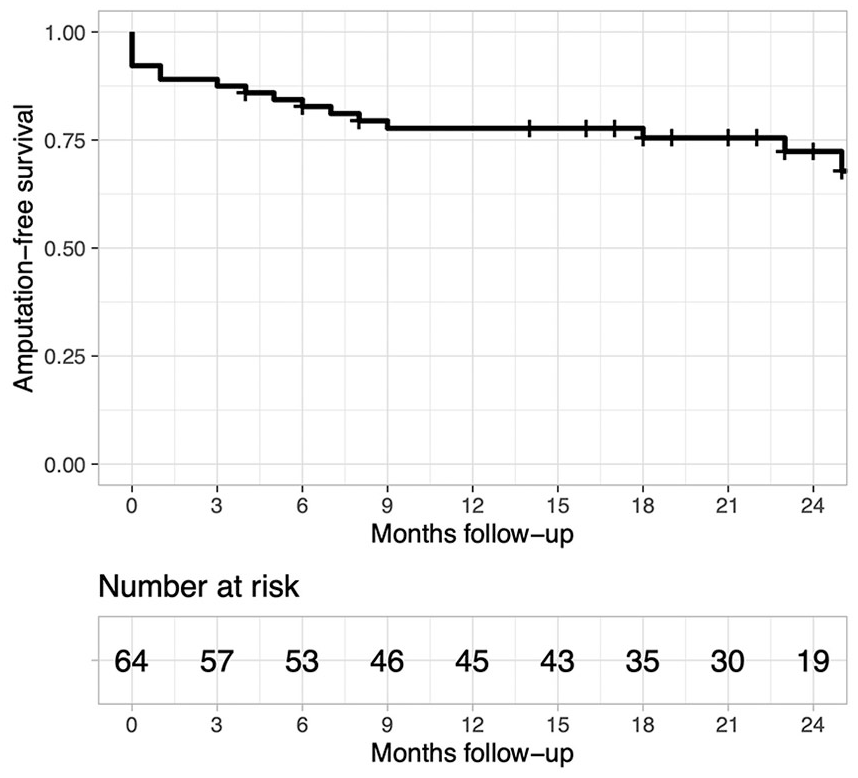
Amputation-free survival for the overall cohort.
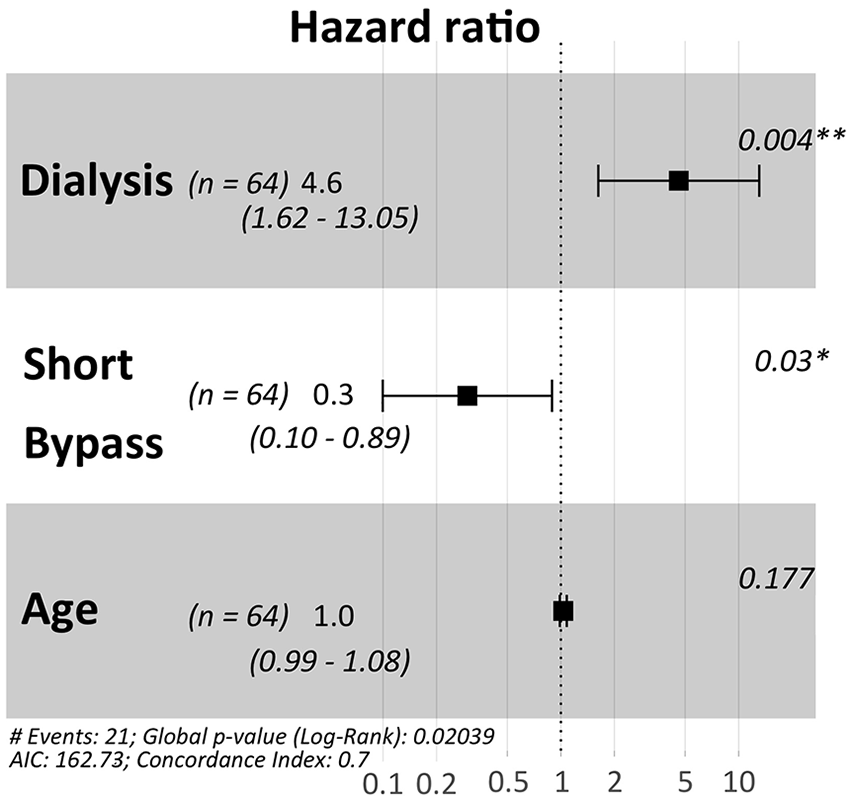
Forest plot for multivariate Cox regression analysis showing predictors of primary patency. AIC, Akaike information criterion.
On multivariate analysis, the association of limb salvage with sex (HR, 0.27; 95% CI, 0.07–1.07; p = 0.06) and smoking status (HR, 0.17; 95% CI, 0.02–1.37; p = 0.09) was not statistically significant. In total, 10 patients underwent major amputations: six below the knee and four above the knee.
Discussion
Besides relief of ischemic pain, ulcer healing, prevention of limb loss, and survival, functional recovery is a major objective of CLTI treatment, being strictly related to quality of life. 10 Infrainguinal bypasses are recommended for TASC D lesions. 12 The new Global Vascular Guidelines for treating CLTI, support surgical revascularization in those patients with extensive steno-occlusions of leg arteries and with WIfI stages 3 to 4.2,3 Infrainguinal bypass should originate from an uncompromised artery and, most importantly, should have a good quality outflow artery, whose flow is in continuity with distal arteries (good run-off). This is important to determine patency. 5
Numerous studies have already demonstrated that inframalleolar bypasses with vein graft are effective and durable. 13 However, the surgical approach to inframalleolar vessels is really challenging and is performed only in a few centers with high expertise in this field, contrarily to endovascular approach, which is more widely available.
Our experience was characterized by a very limited use of arteriography for diagnostic purposes, whereas the planning of bypass procedures was based on duplex ultrasound arterial mapping. Although heavily calcified arteries may be really challenging to study with only ultrasound imaging, artery patency can be evaluated with hemodynamic information given by a punctilious duplex imaging study. 6 In our experience, in the inframalleolar district, duplex ultrasonography can be more sensitive than arteriography in detecting a patent target vessel with a very slow flow. Moreover, it is harmless and costs less than arteriography. However, test quality depends on operator ability.
In our study, we wondered whether inframalleolar bypass patency, limb salvage, and survival rates were good overall in patients with extensive arterial leg occlusion. Moreover, we sought to identify any risk factors that could potentially affect outcomes.
Interestingly, regarding risk factors, our study population was characterized by a relatively low mean age and half of the patients did not have diabetes, which might appear counterintuitive for patients with such distal arterial disease. Nonetheless, almost all of the patients had at least one risk factor among heavy smoking, hemodialysis, diabetes, and old age. We can speculate that other factors might have played a role in the development of arterial disease in our study population, such as regional eating habits that included traditional handmade cured meat and preserves very rich in salt and fat. Unfortunately, detailed information about eating habits were usually lacking in the clinical records.
The results of our study are comparable with patency and limb salvage rates reported in the literature. 14 We reported a primary patency of 67%, a secondary patency of 88%, and limb salvage of 84% at 2 years. Such rates are remarkable, considering that, as a tertiary referral center, patients are routinely referred to our institution after failure of revascularization procedures performed at other centers.
The great saphenous vein was the material of choice when available, preferably devalvulated, either in situ or ex situ. A prosthetic graft was only used to create a composite graft when the vein material was not long enough for the whole bypass. As reported in the literature,15,16 autogenous vein graft material has better outcomes compared to prosthesis, with a prevalence of in situ great saphenous vein usage.16–18 In our study, a composite graft was not associated with worse outcomes. However, this was used in a few cases and therefore no conclusion can be drawn in this regard.
When ipsilateral great saphenous vein is not available or not adequate, small saphenous vein, cephalic vein and basilic vein are feasible alternatives, with acceptable patency rates. 19
Patients with end-stage renal disease (ESRD) are known to suffer from poor patency and limb salvage rates after open revascularization due to extensive calcifications of calf arteries and high susceptibility to infection.20,21 Berceli et al. reported, out of 384 inframalleolar bypass grafts, 21 (5%) were performed on patients undergoing renal replacement treatment, with overall patency and limb salvage rates of 68% and 87% at 5 years, respectively. Johnson et al.20–22 reported 13 inframalleolar bypasses in ESRD patients, with a graft patency rate of 62% at 2 years, and 50% limb salvage. In our series, patients on dialysis had significantly worse outcomes in terms of primary patency compared with patients not on dialysis. However, we also reported good secondary patency, limb salvage, and overall survival rates in patients on dialysis, with no significant difference compared to the subgroup not on dialysis.
Another risk factor apparently associated with worse outcomes was female sex. In fact, we observed a higher rate of limb salvage in men compared to women. This finding is consistent with the observation of smaller vessels in women compared to men. Nonetheless, the multivariate analysis did not show an association between sex and bypass failure.
As patients with CLTI often have moderate to high operative risk due to several comorbidities, the endovascular approach represents an increasingly appealing alternative to bypass surgery.
Moreover, in the last few decades, improvement of the endovascular technique, along with the use of pharmacological adjuncts, has led to good patency rates and decreased postoperative morbidity and mortality. 23 Endovascular tarsal and pedal intervention is a tempting alternative to inframalleolar bypass in view of the reduced invasivity.
Several studies reported the safety and feasibility of below-the-ankle angioplasty, using subintimal or intraluminal recanalization techniques of dorsalis pedis and plantar arteries. Balloon angioplasty is the standard endovascular technique for treating inframalleolar vessels.24,25 Manzi et al. 26 reported that, out of 25 patients treated with the pedal loop technique for CLTI, an acute success of 85% and an amputation-free survival of 71% was achieved at 6 months. Mohapatra et al. 27 reported similar limb salvage at 1 year between bypass and endovascular revascularization groups. Instead, primary patency and primary assisted patency were higher in the bypass group. In our experience, an endovascular-first approach is offered to patients with limited tissue loss or short arterial occlusion. Patients with extensive arterial disease and tissue loss are first considered for open surgical revascularization.
In previous reports from our group,7,8,28 lower patency and limb salvage rates were reported in patients with previous failed endovascular procedures, compared to patients treated with bypass surgery as the first option. In fact, prior failed endovascular intervention was associated with a 30% increased risk of limb loss and graft occlusion at 1 year. Similar results were found by other authors and confirmed in a recent meta-analysis. 29 Such evidence has led to a review of the ‘endovascular-first’ policy in favor of a ‘surgery first’ approach for patients with extensive vascular lesions associated with advanced clinical stage, as recommended in the latest guidelines. 3
This study, conversely, failed to identify the presence of previous endovascular intervention as a predictor of worse outcomes. This discrepancy might be explained in light of the attitude of our group to safeguard the most distal tibial artery segments and inframalleolar arteries during endovascular procedures and to limit the pedal loop technique to strictly selected cases. In other words, the distal anastomosis of inframalleolar bypasses at our center is usually carried out on an arterial segment that was not previously treated, even in patients who had undergone previous endovascular treatment on the same limb. Nonetheless, we recognize that a larger number of patients is necessary to confirm this finding.
A bypass originating from the popliteal artery was independently associated with better primary patency in our study. A similar finding was recently reported by Saarinen et al., who speculated on different possible explanations. These included a more severe disease profile in patients with multilevel occlusion, the opportunity to choose the best vein segment for short bypass procedures, and a lower rate of wound complications. 14 Indeed, in our study, a short bypass was significantly more commonly performed on diabetic patients, suggesting that the subgroup undergoing short bypasses had a different risk profile and disease pattern.
On the other hand, other authors did not find a better patency from short bypasses. 30
Our study showed a favorable patency and limb salvage rate for patients treated with lower limb bypass revascularization if compared to the endovascular results reported in the literature of patients treated for arterial disease extended below the ankle. 31
Our cohort of patients had extensive steno-occlusive disease with ulcer and gangrene, and numerous comorbidities. Probably, most of those patients, without a bypass procedure, would have undergone amputation. Our aggressive surgical first approach in Rutherford category 5 and 6 patients with extensive distal arterial disease appears justified in light of recent studies which have showed better results for bypass surgery compared to an endovascular approach. 10 We believe that revascularization is feasible in all patients with advanced CLTI, letting only permanently bedridden patients and patients with extensive gangrene or infection undergo primary amputation. Kalra et al. reported amputation as a significant independent risk factor for higher long-term mortality. 4 Panayiotopoulos et al. reported better survival in patients with successful surgical infrainguinal procedures compared with amputees.4,32 We reported limb salvage of 84% at 2 years, with only 10 major amputations, and 85% survival. Moreover, the majority of patients had good functional recovery within the first 6 months after surgery. These results encourage us to consider the inframalleolar bypass as a viable approach, even in patients with a moderate-to-high surgical risk profile. In lack of endovascular studies with long-term outcomes, we assume that bypass grafting to inframalleolar arteries should be preferred over endovascular treatment in all patients with severe foot ischemia and extensive distal disease of the tibial vessels.
Limitations
This study has some limitations. It is a retrospective study and as such it has an inherent risk of bias. The number of patients included is relatively small and therefore the sensitivity of subgroup and multivariate analyses was reduced. Moreover, as a referral center, some of the patients included had previous interventions at other centers and therefore technical details about previous interventions were not always available. Finally, electronic medical records were incomplete before 2015 and for this reason we decided not to collect data of patients treated before this date, thus limiting the maximum follow-up available at 48 months.
Conclusion
Bypass grafting to the inframalleolar arteries resulted in good long-term patency, limb salvage and overall survival. A short bypass was independently associated with improved primary patency. In patients with ESRD, inframalleolar revascularization is feasible and can be expected to result in success, although a closer follow-up is advisable. Secondary patency and limb salvage rates were comparable between patients with and without ESRD.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.