
Abstract
Our aim is to examine the effects of climatic conditions on the incidence of ruptured abdominal aortic aneurysms (rAAA) in Catalonia, Spain. We combined clinical data from the Public Health official registries in Catalonia, Spain (HD-MBDS) of all rAAA with local climatic data obtained from the closest meteorological station (69 stations, National Meteorological Service: MeteoCat) from 2008 to 2017. We analyzed the median, maximum, minimum, and variability of atmospheric pressure (hPa) and air temperature (°C), solar irradiation (MJ/m2), humidity (%), accumulated precipitation (mm), median wind, and maximum flaw direction and velocity (°, m/s), recorded on the days of events, the previous day, and mean results for 3, 7, and 30 days before, as well as seasonality. Seventy-five control days were randomly selected in a 1-year period around every rAAA day at the same meteorological station, and compared. A total of 717 days and locations with rAAA were identified, and 53,775 controls were randomly selected. For the rAAA days, there were significantly lower temperatures, lower solar global irradiation, and higher mean humidity levels in all time periods (p < 0.001, p < 0.001, p < 0.05); higher atmospheric pressure variability during 1 week and 1 month before (p = 0.011, p = 0.007); and they often occurred during autumn/winter (57.6%, p < 0.001). Logistic regression identified low mean temperatures on the days of ruptures and high mean humidity the week before as independent rupture predictors. In conclusion, low median temperatures the same day and high humidity during 1 week before were identified as independent predictors of rAAA occurrence. The role of climate on pathophysiologic mechanisms may require further investigation.
Keywords
Introduction
Ruptured abdominal aortic aneurysms (rAAA) still carry important morbidity and mortality rates,1–3 even though these rates have diminished with the introduction of centralization 4 in some areas, augmentations in prophylactic repairs, and advances in endovascular surgery. The roles of predisposing factors, such as smoking, sex, age, family history, arterial hypertension, aortic diameter, and wall stress, on the development of rAAA have been widely investigated.1,5,6
The effects of meteorological factors have also been analyzed; however, evidence is confounding and inconclusive. Several studies have been published, buttressing an association between weather conditions and higher rates of rAAA – primarily low atmospheric pressure and low temperatures.7–12 Nonetheless, other publications demonstrate no relation between the incidence of rAAA and these conditions.10–16 Some authors have shown a seasonal peak in the occurrence of rAAA, mostly in autumn and winter,6,7,11,12,15–17 but others have failed to prove this association.8,9,14,15,18–21
As noted above, the results of these investigations show a marked disparity, mainly because of biased publications, since most of these studies were performed in countries with severe winter conditions or with few meteorological variations between seasons. Also, most of the investigations were based on single-center experiences, with imprecise crude meteorological data and methodological biases.
The purpose of this study is to examine the effects of climatic conditions on the incidence of rAAA in public health centers in Catalonia, Spain over a 10-year period, employing precise national climatic registries.
Methods
A retrospective observational study was designed to identify climatic factors related to rAAA, analyzing up to 1 month before every episode of rupture. Data of rAAA occurrence was provided by the official database of the Catalan National Health System (CatSalut) – Public Data Analysis for Health Research and Innovation Program (Project PADRIS), whose mission it is to make available to the scientific community health information to promote research, innovation, and health assessment through using public healthcare resources and thereby accomplishing ethical principles. PADRIS is a public program led and managed by the Catalan Health Quality Assessment Agency (AQuAS) of the Health Department. Data were obtained from the Catalonian hospital discharge Minimum Basic Data Set (MBDS; http://catsalut.gencat.cat/ca/proveidors-professionals/registres-catalegs/registres/cmbd/), a valid, comprehensive, and mandatory registry for all public hospital discharges. It is based in Catalonia, a Spanish region with a population of 7,543,825 inhabitants and a density of 234 inhabitants/km2 (Institute of Statistics of Catalonia, https://www.idescat.cat/; January 2018). MBDS collects dates of admission and discharge, age, sex, primary and secondary diagnoses, surgical procedures according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM; the database moved to ICD-10 in 2018), vital status at discharge (alive or deceased), and the hospital that provides the assistance. We focused on rAAA (ICD-9-M 441.3) and the dates and hospitals of the initial admissions of each episode.
To gather meteorological data of each episode, we contacted the National Meteorological Service of Catalonia, Spain (MeteoCat), which records precise daily climatic variables among meteorological stations. We identified the closest station to every rAAA initial hospital admission (the first center where the patient consulted or was admitted, not the final treating hospital), dismissing stations with discontinuous information among the study periods. Sixty-nine stations were finally utilized. The following parameters were analyzed: median, maximum, minimum, and variability (maximum – minimum) of atmospheric pressure (hPa: hectopascal) and air temperature (°C), as well as solar irradiation (MJ/m2: megajoules per square meter), humidity (%), accumulated precipitation (mm), median daily wind velocity (m/s) and direction (u-module: °), and maximum wind flaw (m/s) and direction (°), at 10, 6, and 2 meters high.
Readings from these meteorological conditions were obtained for the days of the events, the previous days, and the mean results for 3 days, 1 week, and 1 month prior to the events, following previous studies that suggest meteorological conditions can impact aneurysmal rupture several days or weeks before the event occurs. For seasonality, we used the astronomic seasons (spring: March 21 – June 20; summer: June 21 – September 22; autumn: September 23 – December 20; and winter: December 21 – March 20).
To compare meteorological conditions in the rupture days, we randomly selected 75 control days for every rupture. They were randomly chosen in a 1-year period (from 6 months before to 6 months after) for every rupture day, in the same meteorological area (station) where the rupture occurred; thus, control days are a representation of usual meteorological conditions in the same area during the whole year, not exclusively of non-rupture days. It produced 53,775 control days, which compared meteorological conditions to rupture days. The analyzed unit was the meteorological daily conditions (rupture vs control days), not the case itself; thereafter, matched case–control was not possible.
Inclusion criteria were all diagnosed cases of rAAA admitted to any public healthcare center in Catalonia from January, 2008 to December, 2017 (initial admission excluding transfers between hospitals in the same episode), and the randomly selected cases, as previously described. Exclusion criteria were rAAA cases without treatment (ICD-9-CM procedure codes 38.44, 39.25 for open repairs and 39.71 for endovascular repairs) and discharged alive (not transferred to another hospital), and cases with both open and endovascular repairs in the same admission episodes. These cases were excluded because of probable misdiagnoses (possible non-ruptured AAA and complicated elective surgeries with secondary rupture, respectively).
Owing to the use of aggregated data in public databases, informed consent was not obtained. The study was approved by the Hospital Clinic Aortic Committee Board, following the principles of the Declaration of Helsinki.
Statistical analysis
Descriptive parameters (described as mean ± SD) and frequencies (number and %) from all obtained data were extracted using SPSS, Version 23 (IBM Corp, Armonk, NY, USA). Univariate analysis (comparisons of all weather and season variables between groups: rupture and control days) was performed using parametrical tests: Pearson’s chi-squared, t-test for independent samples, and ANOVA analysis. After identification of significant differences in univariate analysis, forward conditional logistic regression was performed with all analyzed weather and variables to identify independent prognostic factors of days of rAAA. A p-value less than 0.05 was deemed to be statistically significant.
Results
After application of inclusion and exclusion criteria, 717 rAAA were identified, and respective locations and rupture days were included; 53,775 control days were randomly selected. The mean age of the patients was 75.9 (SD 9.59) years, mostly male (660, 92.1%).
After comparing all analyzed climatic variables (median, maximum, minimum, and variability of atmospheric pressure and air temperature, solar irradiation, humidity, precipitation, and wind and flaw velocity and direction), no significant median atmospheric pressure differences were observed on days with rAAA (999.76 hPa (19.92)) compared to control days (999.34 hPa (20.13)), p = 0.619 (Table 1), although mean atmospheric pressure variability for 7 days and 1 month prior to the events showed an increment in rAAA risk occurrence (p = 0.011 and p = 0.007, respectively). In regard to temperature, there were significantly low temperatures for all the time periods evaluated, but temperature variability did not reveal any differences. There was low solar global irradiation in all analyzed time periods (from the same day to 1 month prior) when rAAA occurred (p < 0.001). Mean humidity levels did not show differences on the days of the ruptures, despite higher values in all the other analyzed periods.Table 1.
Climatic variables among control and rupture aneurysm days, in the different analyzed periods.
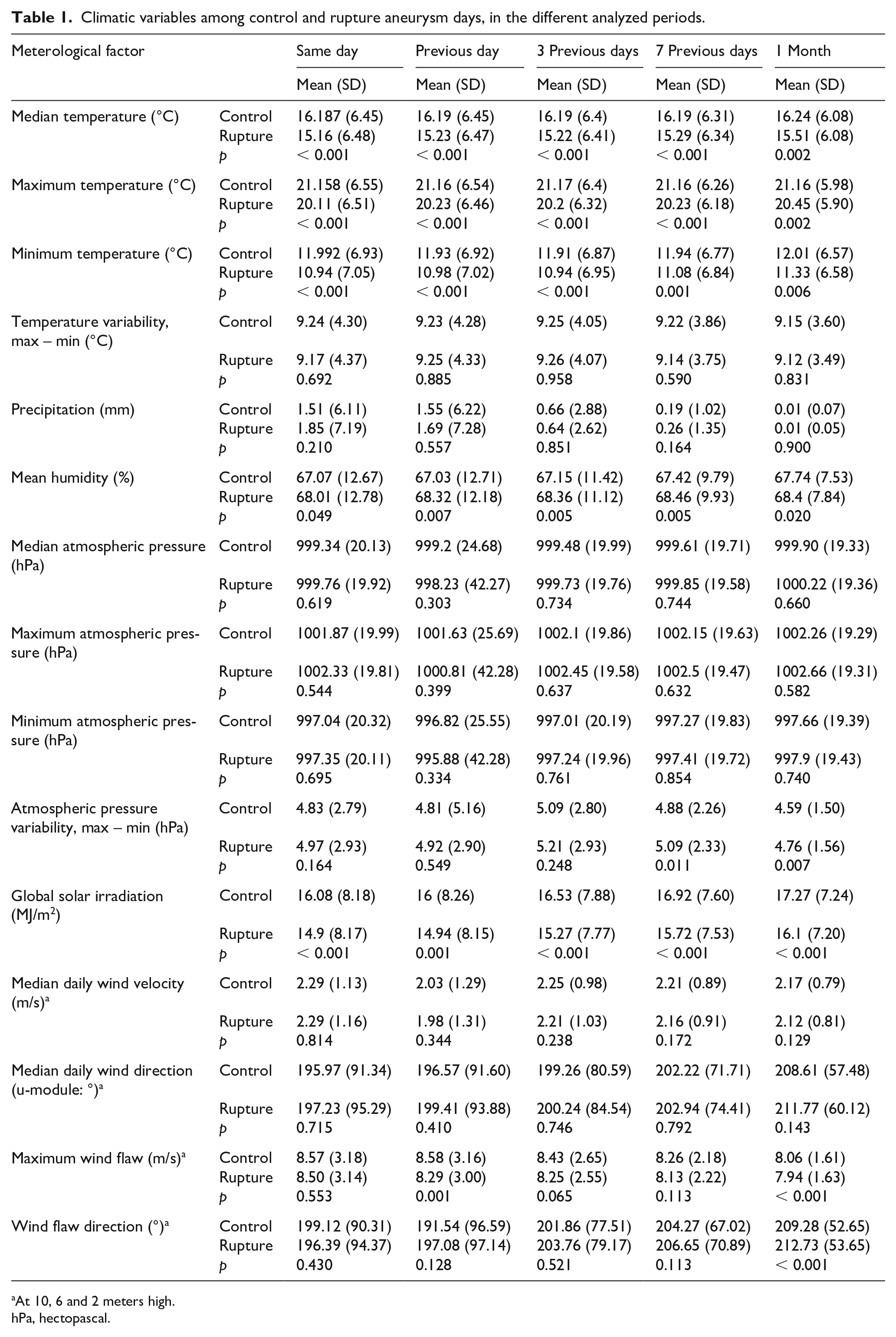
At 10, 6 and 2 meters high.
hPa, hectopascal.
The rAAA occurred more frequently in cold weather (57.6% during autumn and winter), mainly in autumn (p < 0.001, Figure 1). After identification of significant differences in univariate analysis, forward conditional logistic regression was performed with all weather and season variables in order to identify independent prognostic factors of rAAA. We identified low median temperature on the day of rupture and high mean humidity the week before rupture, as independent predictors of rupture days (OR 0.980, 95% CI: 0.966–0.994, p = 0.004 and OR 1.011, 95% CI: 1.002–1.020, p = 0.016, respectively; Table 2).
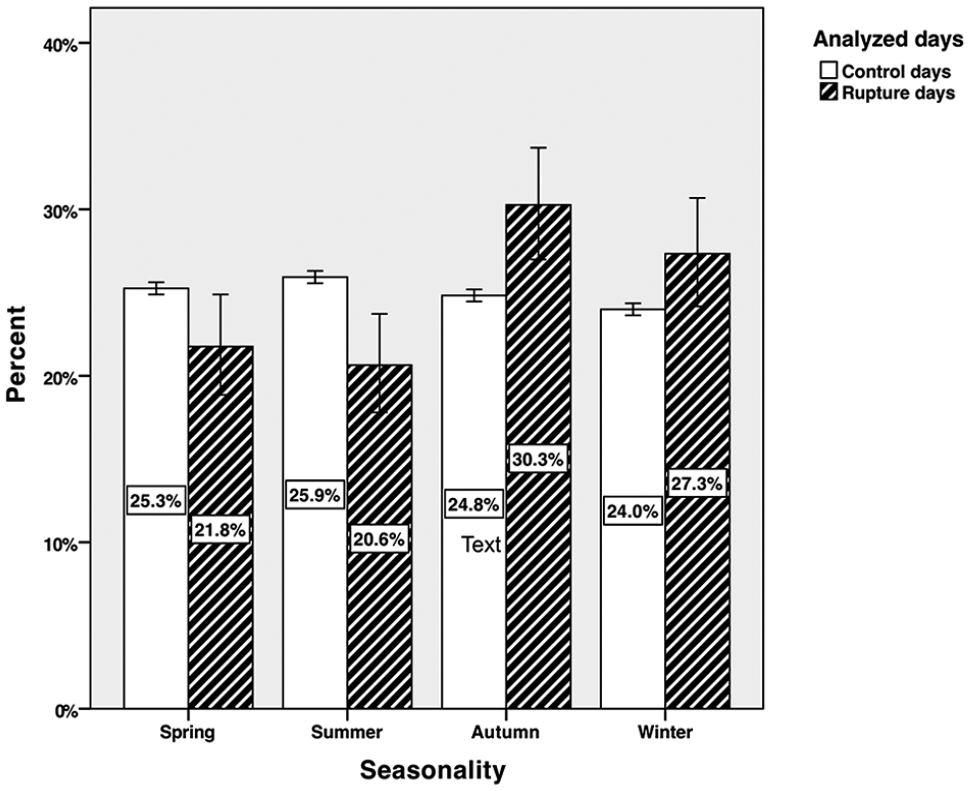
Occurrence of rAAA according to seasonality.
Forward conditional logistic regression of ruptured aneurysm days predictor factors.
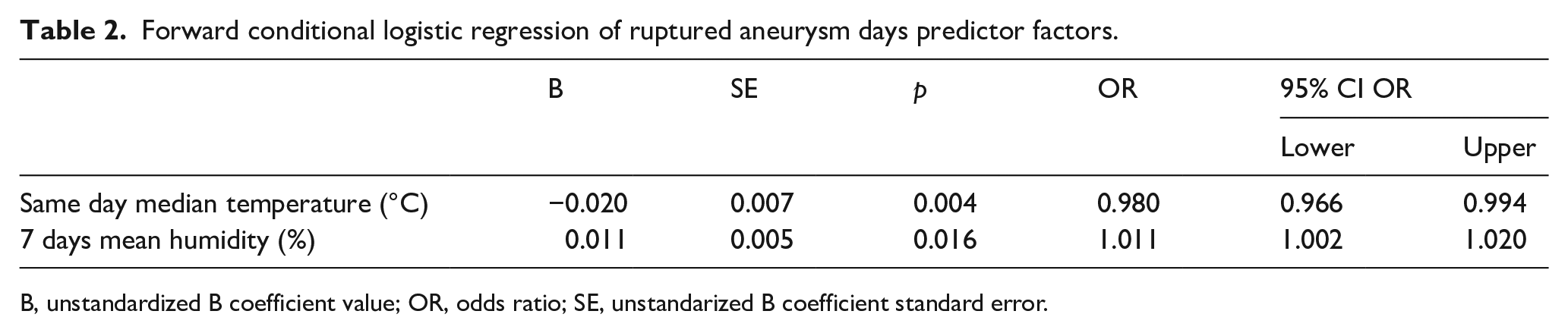
B, unstandardized B coefficient value; OR, odds ratio; SE, unstandarized B coefficient standard error.
Discussion
In our study, we observed that the incidence of rAAA is higher during autumn and winter. Furthermore, meteorological factors, such as temperature, global solar irradiation, humidity, and variability of atmospheric pressure on previous days (up to 1 month before rupture), increased the risk of AAA rupture. When analyzing these factors with a multivariate logistic regression, we identified same day temperature and mean humidity during 7 days before as independent prognostic factors of rAAA occurrence.
Previous publications have analyzed the effect of weather on rAAA occurrence. Most of them only examine seasonality, temperature or atmospheric pressure variability, but rarely does any study perform a thorough investigation of multiple meteorological variables.1–7 Actually, in a recently published systematic review of seasonal and atmospheric associations of rAAA, analyzing 51,589 patients, the only association found was a seasonality peak in autumn, followed by winter, but the limitations in the study did not permit finding any other associations. 18 In our work, we performed a deep variable analysis and a subsequent multivariate regression, endeavoring to include all possible variables and finding the independent prognostic factors. We included all registered meteorological items in the stations analyzed in order not to lose information.
Referring to controls, most published studies, to-date, do not specify their sources,13,14 or use days of non-ruptured cases.7–9,15,16 In our opinion, selecting controls from non-ruptured days (or from non ruptured periods) only, instead of a random selection of controls from days in the study period (including ruptures and non-ruptured days) introduces potential for selection bias error. In this study, we tried to identify whether rAAA occur randomly throughout the year, which is why our controls were randomly selected throughout the year.
In addition, most studies use generic meteorological country data,1–7 instead of what we did: search for the closest meteorological station for every rAAA, every single case and day. Using generic data, instead of precise local information, can again misinform, and in big countries it can be very unrealistic. In spite of the fact that our country is small (32,108 km2), we generally have a Mediterranean climate, but due to the big differences in topography, there is a significant contrast in local weather between the hot southern coast and the cold northern Pyrenees. Thus, altitude and eventually atmospheric pressure, solar irradiation or humidity can vary between regions in our country and invalidate generic national data for our purpose. In particular, humidity is generally higher and more constant on the coast than inland (where higher yearly variations occur), reaching the lower values in July to August and higher grades in September to October.
We analyzed 717 rAAA in a multicenter study. Most previously published studies analyze single-center data7–9,13–16 or, at maximum, data from two different hospitals that include a lower number of cases, except three previous meta-analyses published in recent years.8,18,19 Again, this reinforces the statistical power of our work, since we used a national database gathering information from all public hospitals in our region with admissions of rAAA (49 centers). Using multicenter studies in national registries can avoid selection bias, such as those patients not registered because they were transferred to other centers.
Despite previous severe bias, we can compare our results with previous publications. Most studies report a seasonal variation of rAAA, with autumn and winter (mostly autumn) being the seasons with the highest incidence of rupture.7–11,13,16,17,20–26 Our results are in line with these findings. Climatic conditions such as low mean atmospheric pressure,3,9,10–12 4-day variances in atmospheric pressure as independent factors, 8 low temperatures,8,27,28 high atmospheric pressure, 29 low humidity, 29 and low global solar irradiation30,31 have been related to rAAA occurrences. These studies analyze same day weather measurements up to 1 month before rupture. In our study, some analyzed variables showed a relation to rAAA occurrences in univariate analysis with significant differences. We also found significantly lower temperatures, lower solar global irradiation, but higher mean humidity levels in all analyzed time periods (from the same day to 1 month before) when rAAA occurred (p < 0.001, p < 0.001, and p < 0.05, respectively). Contrary to some previous publications,11,12,19 we found no differences in median atmospheric pressures, but the variability of atmospheric pressure during 7 days and 1 month before the events showed an increment in AAA rupture risks (p = 0.011 and p = 0.007). Logistic regression identified low median temperatures on the day of rupture and high mean humidity the week before rupture, as independent predictors of rupture.
The salient point of our study is that most rAAA occur during cold periods, where there is less global solar irradiation and higher humidity. Most of the published evidence agrees on a higher incidence of rAAA during cold seasons. Possibly, this relationship is based on pathophysiologic evidence, since there is a considerable amount of data that show blood pressure elevation during periods of cold temperature32–34 because of augmented sympathetic stimulus and, therefore, more secretion of catecholamines. Another interesting hypothesis considers less solar irradiation in cold climatic conditions, and, therefore, less exposure to UV radiation that triggers vitamin D synthesis – consequently yielding lower levels of this vitamin. It has been reported that 1,25(OH)2D can down regulate renin in the kidneys, suggesting that vitamin D deficiency is associated with arterial hypertension and cardiovascular disease. Additional studies showed a potential relation between sun exposure and its protective effect in preventing hypertension with a clear increase in vitamin D levels with reduction in systolic and diastolic pressures. 35 Other published investigations have proposed a relationship between vitamin D deficiency and aortic dilatation.36,37 Presumed pathogenesis includes endothelial dysfunction, inflammation, and reduced vessel compliance. Despite clinical and experimental research, the mechanisms that may explain the association among hypertension, rAAA, and low vitamin D levels remain unclear. In regard to atmospheric pressure, it has been observed that low levels of atmospheric pressure reduce arterial blood oxygenation, and this activates endocrine and autonomic responses that lead to an increment in blood pressure values.38,39 Taking all of the above into consideration, it seems as though poorer control of high blood pressure influenced by cold weather, can somehow increase the risk of rAAA. Once more, the question arises: do we need a stricter control or surveillance of patients with arterial hypertension in areas of extreme cold weather? Future investigations must be held to prove that these conditions trigger the onset of rAAA.
Catalonia’s climate is diverse. Areas by the coast have more stable, hot, Mediterranean weather, whereas inland areas tend to have more continental cold temperatures during winter and higher temperatures during summer. There is also higher humidity during cooler seasons. justifying that all the prognostic variables were more frequent in autumn/winter.
Short-term and long-term air pollution exposure has been related to myocardial infarction, 40 and the suggested mechanisms (mainly for short-term exposure, like non-obstructive coronary infarcts) could not only affect general health, but also AAA rupture. Unfortunately, we were not able to obtain accurate air pollution data for all the meteorological stations used during the whole study period, and this analysis was not possible. Future analysis of dedicated air pollution stations could help in this investigation.
Limitations
In this study, we tried to avoid the maximum number of biases. However, some limitations could occur. We used national databases, which offer a wide range of cases throughout our country, but they are based on old ICD-9 classification, and coding errors can arise (misdiagnoses of rAAA) and could affect our results. However, the Spanish systematic MBDS registry has shown a high correlation with independent databases in coronary disease validation studies (high sensitivity (85.1%) and very high specificity (98.31%) 41 in both diagnoses and treatments); thereafter, we can assume a similar behavior for rAAA registry, accepting it as a highly reliable national registry. Meteorological data are registered in days, instead of hours; a more precise measure of these variables, or measure of other variables, could improve the quality of the study. We used the closest station to every rupture, and the hospitals where the rAAA were diagnosed, but probably, in some cases, patients lived far from the hospitals, so weather measures could not be totally precise. We used 75 controls per patient, randomly distributed throughout all days of the year, trying to avoid selection bias, but more controls or case-paired analyses could improve this control data. Other interesting clinical data (aortic aneurysm diameter or aneurysm anatomy, peak wall stress) were not available in the national databases, and age or other clinical data-matched controls were not possible because of study design (controls were randomly selected days, not cases).
Conclusions
In summary, our study shows that the incidence of rAAA is higher during autumn and winter, and affected by lower temperatures, lower solar global irradiation, and higher mean humidity levels up to 1 month before, and variability of atmospheric pressure during 7 days and 1 month before rAAA occurrence. Furthermore, low median temperatures the same day and high mean humidity during 1 week before rupture were identified as independent predictors of rAAA occurrence.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.