
Abstract
The rate of cardiovascular disease (CVD) mortality reduction in the United States has plateaued recently, despite the development of novel preventive pharmacotherapies, increased access to care, and healthcare spending. This is largely due to American’s poor dietary patterns and practices causing increasing trends in the prevalence of obesity and type 2 diabetes mellitus. For decades, dietary guidelines on ‘healthy diets’ to reduce CVD risk, grounded in epidemiological research, have been nationally distributed to Americans. In this review, we highlight landmark events in modern nutrition science and how these have framed past and current understandings of diet and health. We also follow the evolution of dietary recommendations for Americans throughout the years, with an emphasis on recommendations aimed to reduce risk for CVD and mortality. Secondly, we examine how the low-fat ideology came to dominate America in the last decades of the 20th century and subsequently contributed to an excess intake of refined carbohydrates which, in the context of an increasingly sedentary lifestyle, may have fueled the obesity epidemic. We then examine the current major evidence-based dietary patterns and specific dietary approaches to reduce CVD risk, reviewing the literature surrounding nutritional components of the heart-healthy diet and discussing the dietary patterns proven most effective for CVD prevention: the Dietary Approaches to Stop Hypertension (DASH) diet, the Mediterranean diet, and the healthy vegetarian diet. Finally, we discuss emerging dietary trends, considerations for nutrition counseling, and future directions within the important field of nutrition, with the ultimate goal of improving vascular health.
Introduction
Cardiovascular disease (CVD) is the leading cause of death in the United States (US) for both men and women. 1 For the first decade of the 21st century, age-adjusted mortality from coronary heart disease (CHD) declined by 30%. This can be attributed to reduced smoking rates, percutaneous intervention for acute thrombotic events, as well as the use of evidence-based medicine to improve therapies intended for controlling blood pressure and cholesterol. 2 However, after 2011, the rate of decline of CVD mortality decreased, and has plateaued in men, women, and all racial/ethnic groups, with poor diet and obesity believed to be a major contributor.2,3 Meta-analyses of prospective studies and clinical trials have associated poor diet with almost half of all deaths from CHD, stroke, cancer, and type 2 diabetes mellitus. 4 The US Burden of Disease Collaborators has cited poor diet as the leading cause of premature death and disability nationally. 5
In the mid-20th century, the US experienced a rise in chronic diseases such as CVD, obesity, and type 2 diabetes. As a result, nutrition science began to focus on dietary risk factors for the development of chronic conditions. This sparked decades of studies using observational cross-sectional and prospective cohort studies to draw associations between components of the human diet to CVD development. The purpose of which were to optimize diet to prevent CVD and its risk factors. However, much of the data from these early epidemiological studies were observational in nature and thus subject to the study design flaws that often plague these data. Common issues in these studies included information bias, reverse causation, erroneous causal inferences, and residual confounding from other social and behavioral factors.6–8 Nonetheless, the US government, the American Heart Association (AHA), the Surgeon General, and other public health agencies used the most up-to-date evidence at the time to inform national dietary recommendations for Americans to promote heart health.
Owing to constantly evolving evidence, the recommendations for heart-healthy diets have dramatically shifted throughout the last 50 years (Figure 1). In this review, we will take a walk through time and explore the dynamic landscape surrounding heart-healthy dietary guidelines and CVD prevention. We will first explore the evolution of evidence relating diet to CVD and how they informed recommendations for heart-healthy diets throughout the years. We will highlight how lessons learned from the past have impacted current research methods and national dietary guidelines. We will then review the evidence supporting the present US government and AHA dietary recommendations. We end by discussing the emerging dietary trends, considerations for patient counseling, and future directions in the field of nutritional epidemiology.
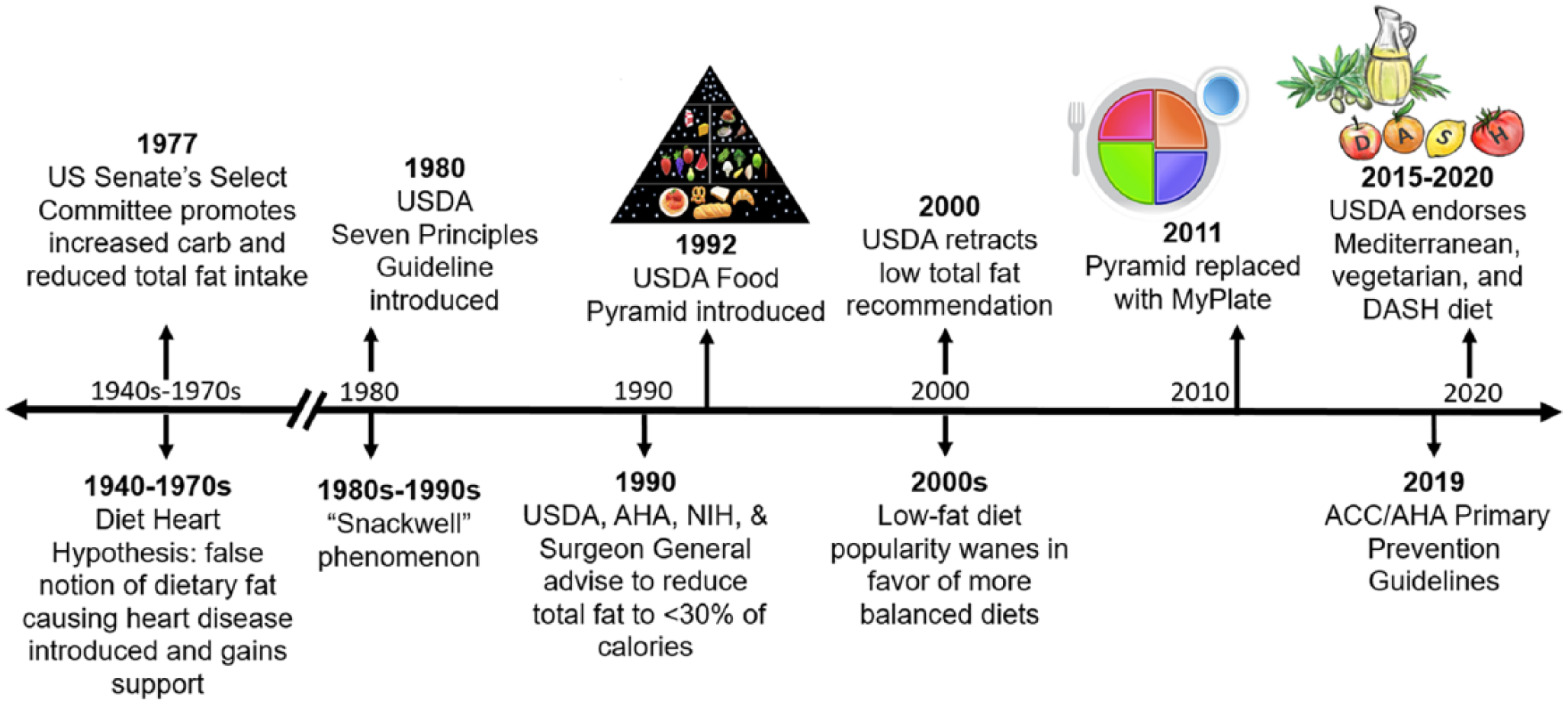
The evolution of the heart-healthy diet. This depicts the timeline of major dietary recommendations distributed by the USDA, DHHS, AHA, ACC, NIH, and other public health agencies throughout the years.
The past: Evolution of the heart-healthy diet and focus on fat reduction
1940s–1970s: The development of the diet-heart hypothesis
Starting in the 1940s, CHD was identified as the leading cause of death in the US. 9 The rise of chronic diseases during this time period galvanized nutrition scientists to shift their focus to potential dietary causes of CVD and other non-communicable diseases. 10 In 1948, the National Heart, Lung, and Blood Institute (NHLBI) initiated the Framingham Heart Study, the first cohort study to investigate hypertension, CVD, CHD, and stroke. 11 To date, it has prospectively followed participants for over 70 years and recruited three generations of participants. In 1957, the Seven Countries Study began to examine the relationship among diet, lifestyle, and rates of CHD and stroke in populations with differing dietary patterns. 12 The data from these studies were used to generate much of the knowledge we currently have regarding CVD risk factors, like smoking, obesity, and lack of exercise. 13
These studies were also used to draw a correlation between diets high in saturated fat and cholesterol with increased CVD incidence. 14 This inspired researchers and scientists to widely accept the ‘diet-heart hypothesis’, 15 which deduced that since dietary saturated fat raises serum cholesterol and high cholesterol contributes to CHD, then saturated fat intake must also cause CHD. This led to recommendations that Americans should reduce their intake of total fats. Although initially only a hypothesis, this ideology would be ultimately propagated within several federal government dietary recommendations, public health policies, and popular health media. (Of note, many scientists have since disagreed. Presently, the AHA recommends replacement of saturated fats with unsaturated fats. 16 )
In the 1970s, the US Senate’s committee on nutrition and human needs first convened. Although originally created to address malnutrition in America, they were the first to ‘put the diet-heart hypothesis on the national agenda’. 9 Its hallmark report, ‘Dietary Goals in the United States’, published in 1977,17,18 was the first statement from any government agency to address risk factors in the American diet and stated: ‘too much’ fat, sugar, and salt in the diet can lead to heart disease, cancer, obesity, and stroke. 18
1980s: The emergence of the dietary guidelines
The Dietary Goals report served as the impetus for the federal government to begin making formal dietary guidelines to Americans. In 1980, the Department of Health and Human Services (DHHS) and the US Department of Agriculture (USDA) first jointly issued the Dietary Guidelines for Americans and have continued to do so every 5 years. These provide recommendations for healthy dietary habits for people aged ⩾ 2 years. The 1980 version included a seven-principle guideline for a healthy diet. The first two guidelines formed the framework of a healthy diet, and the next five targeted single nutrients of the healthy diet. The first principle was to eat a variety of foods including fruits, vegetables, whole grains and enriched breads, milk, meats, and legumes. The second principle encouraged Americans to maintain desirable weight, which was influenced by the emerging evidence linking obesity to high blood pressure, hypertriglyceridemia, and hypercholesterolemia. The third principle, echoing the diet-heart hypothesis, encouraged Americans to avoid cholesterol and total fat, including saturated fat. The fourth recommendation was to eat foods with adequate starch and replace dietary fat with more carbohydrates, especially complex carbohydrate foods (beans, peas, nuts, seeds, fruits, vegetables, and whole grain breads) over simple carbohydrates, like table sugars. Lastly, the remaining guideline recommends limiting the intake of alcohol and especially sodium, which they linked to hypertension. These messages are generally reiterated in the 1985, 1990, and 1995 guidelines. In addition to the federal government, the food industry played a role in promulgating the diet-heart hypothesis.
1990s: The low-fat ideology and the ‘SnackWell’ phenomenon
Corporations capitalized on the widely accepted low-fat recommendation and initiated what would become known as the ‘SnackWell’ phenomenon. This is a term coined to describe how Americans, perceiving low-fat foods to be healthier, consumed these sugary foods in larger quantities than they would have for normal-fat snacks. 9 These snacks, however, were similar in caloric value to their normal-fat counterparts. This, in turn, may have encouraged overconsumption of calories from carbohydrates.
By 1990, the USDA, AHA, National Institutes of Health (NIH), and the Surgeon General independently advised Americans to reduce fat to < 30% of total calories.9,19,20 In 1992, the USDA released the food pyramid, which further reinforced the ideology of a low-fat diet. The pyramid was a diagram advising the optimal number of daily servings to be consumed from the basic food groups, 21 and is widely considered the most distributed and recognized nutritional education device ever created in the country. 9 The pyramid urged individuals to consume most of their daily intake from grains (6–11 servings, including bread, cereal, rice, and pasta), without distinguishing between whole grains and refined grains, vegetables (three to five servings), and fruits (two to four servings) (depicted in Figure 1).
During this 1980s to 2000s period, Americans were encouraged to receive most of their energy from grains and consume low-fat products containing high quantities of sugar. It is thus unsurprising that following these recommendations and in conjunction with the SnackWell phenomenon, there was an alarming increase in obesity and type 2 diabetes prevalence trends in the US (Figure 2). 22 This temporal relationship, however, does not imply causation. Multiple factors could have also contributed to this epidemic, including the increasingly sedentary lifestyle of the average American, the introduction of entertainment technologies, and the proliferation of fast foods. 9
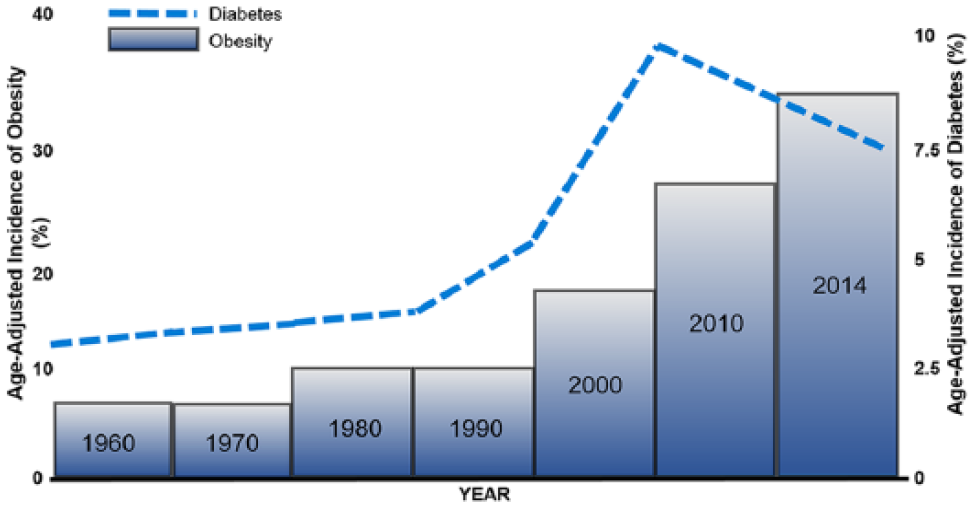
Timeline of age-adjusted incidence of obesity and type 2 diabetes in the US. Since the 1960s, the US has experienced an ongoing chronic disease epidemic in which the incidence of obesity and type 2 diabetes have both increased in parallel.
The push for low fat and acceptance of the diet-heart hypothesis was well intentioned, yet had lasting consequences. The campaign against dietary fat was grounded in reducing saturated fat intake, which was presumed to cause CVD. However, this aversion to saturated fat was ultimately generalized to include all dietary fat, including unsaturated fats, which are found in nuts, fish, and vegetable oils, and are considered healthful. 23 Furthermore, although the guidelines recommended the intake of complex carbohydrates and low fat, evidence suggests the absolute fat intake of Americans remained approximately the same during this time and actually led to an increase in total calories consumed from refined grains and simple sugars, including white bread, crackers, cereals, and other starchy foods. 24 This has had lasting impacts, as up to 70% of Americans continue to exceed the recommended amount of refined grain consumption.23,25 With the turn of the century, more robust nutrition science data emerged discrediting the diet-heart hypothesis.
2000s: Challenging the low-fat ideology with evidence
Eventually, the low-fat ideology was challenged by additional scientific evidence. In 2006, the Women’s Health Initiative Dietary Modification Trial, the largest study to compare the long-term effectiveness of an intervention targeting fat reduction with usual diet control, was published. 26 They found low-fat interventions did not reduce the risk of cancer and CVD, and only modestly improved cardiometabolic risk factors. 26 This was followed by a systematic review and meta-analysis of randomized clinical trials (RCTs), including 53 studies and over 68,000 participants that did not find that low-fat diets conferred improved weight loss over other types of dietary interventions. 27
Even before these publications, the Dietary Guideline Advisory Committee started to recognize a disconnect between restricted fat intake and the troubling obesity and CVD incidence trends. 24 In 2000, the Dietary Guideline Advisory Committee reversed its previous recommendation to lower total fat intake and cited that this may have inadvertently caused people to believe any diet low in fat was healthy and, thus, encouraged over-consumption of total calories from carbohydrate which led to the adverse metabolic effects of high carbohydrate diets. 24 Consequently, the 2005 Dietary Guidelines reversed decades of previous recommendations by revising the < 30% fat composition recommendation to 20–35% of calories. In these guidelines, they also emphasize lowering saturated fat consumption, rather than total fat. The 2005 Dietary Guidelines also unsubscribed to the ideology that complex carbohydrates are the base of healthful diets, as evidenced by the food pyramid, and called on the public to restrict added sugars and refined grains. In 2011, ‘My Plate’ was introduced to replace the prior food pyramid, with an icon that emphasizes fruit, vegetable, grains, protein, and dairy (depicted in Figure 1). 28 This plate endorses eating fewer calories overall, making half the plate fruits and vegetables, and drinking water instead of sugar-sweetened beverages.
In summation, there are three main lessons to gather from the past. First, make dietary recommendations as specific as possible (e.g. distinguish total fat from saturated fat). Second, avoid a reductionist approach to dietary research in which individual nutrients are isolated, such as fat, and linked to outcomes; rather, acknowledge the complexity of diet and consider dietary patterns over single nutrients. Third, use only robust scientific evidence to support national dietary guideline recommendations. With the turn of the century, nutritional science made great advances and additional research emerged regarding the impact of dietary patterns and macronutrient consumption on CVD risk. This all ultimately led to our modern understanding of the heart-healthy diet as we currently know it.
The present: Dietary components, dietary patterns, and their cardiovascular outcomes
Current dietary guideline recommendations for cardiovascular health
In contrast to the past, modern nutrition science uses data from mostly RCTs to inform the current dietary recommendations and guidelines. The modern 2015–2020 Dietary Guidelines for Americans endorses consumption of whole grains, legumes, non-starchy vegetables and fruits, with limited intake of lean meats, seafood, nuts, low-fat dairy, and vegetable oil. 29 Consumption of trans-fats, saturated fats, sodium, red meat, refined carbohydrates, and sugar-sweetened beverages should be minimized or eliminated altogether. In addition, the 2015–2020 guidelines recommend three main healthy eating patterns: (1) US Healthy Eating Diet, (2) Healthy Mediterranean Diet, and (3) Healthy Vegetarian Diet (Table 1).
The current nationally endorsed heart-healthy dietary patterns.
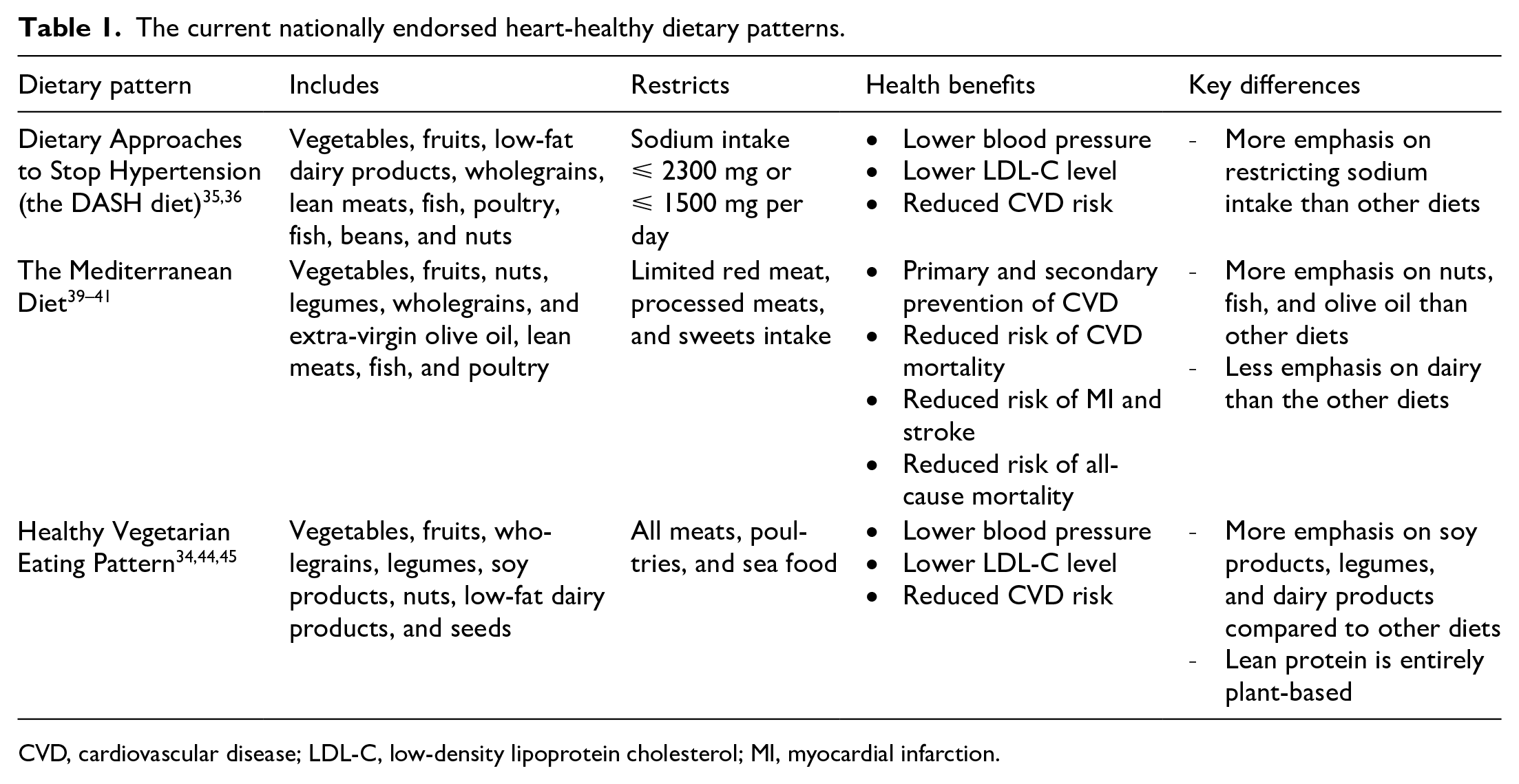
CVD, cardiovascular disease; LDL-C, low-density lipoprotein cholesterol; MI, myocardial infarction.
The 2019 American College of Cardiology (ACC)/AHA guidelines on the primary prevention of CVD warn Americans that diets associated with CVD mortality are more likely to contain high amounts of sugar, low-calorie sweeteners, refined carbohydrates, trans-fat, saturated fat, sodium, red meat, sugar-sweetened beverages, and processed meats like bacon, salami, ham, hot dogs, and sausage. 16 Instead, the guidelines recommend a plant-based or a Mediterranean diet that is high in vegetables, fruits, legumes, nuts, whole grains, and fish to decrease CVD risk factors. It is also advised to reduce cholesterol and sodium, and to replace saturated fat and trans-fats with monounsaturated and polyunsaturated fats to reduce CVD risk. 16
Dietary components: Macronutrient approaches to optimize health
Dietary fats
Dietary fat can be divided into three main categories: (1) unsaturated fat (mono- and polyunsaturated); (2) saturated fat; and (3) trans-fat. Saturated fat and trans-fats are commonly found in processed foods like milk, margarine, butter, and cheese. Unsaturated fats, or ‘healthy fats’, are mostly found in olives, nuts, seeds, oil, and fish. One proposed reason why attempts to reduce fat consumption did not meaningfully translate into cardiovascular health benefits in the past is that these dietary fats have differing associations with total and cause-specific mortality.
Combining data from two longitudinal cohort studies with 126,233 participants, monounsaturated and polyunsaturated fats were found to be inversely associated with CVD risk (hazard ratios (HR) 0.89; 95% CI 0.84–0.94 and 0.81; 95% CI 0.78–0.84, respectively). 30 Saturated fats were associated with increased CVD risk (HR 1.08; 95% CI 1.03–1.14), as well as trans-fats (HR 1.13; 95% CI 1.07–1.18). Interestingly, this study found replacing 5% of total energy consumed from saturated fats with equivalent energy from mono- or polyunsaturated fats was associated with a reduction in total mortality by 27% and 13%, respectively. These findings support the 2019 ACC/AHA dietary recommendations to replace saturated fats with unsaturated fats. 16 Lastly, multiple studies have shown trans-fat intake to be particularly harmful and associated with higher mortality, and should be avoided.16,30,31
Carbohydrates
Like fat, differing carbohydrate types have disparate effects on CVD risk and mortality. Kwok et al. performed a meta-analysis linking dietary components with their individual risk of CVD and all-cause mortality. The consumption of whole grain carbohydrates, including whole grain bread, pasta, oatmeal, and breakfast cereal, was independently associated with a reduced risk of all-cause mortality, in a dose–response relationship. 32 In contrast, refined grains, which include white bread, spaghetti, and crackers, demonstrated a lesser benefit to CVD risk reduction and all-cause mortality. 32 These findings align with the current USDA and AHA endorsement of wholegrain over refined carbohydrate consumption.
Sugar
Added sugars are sugars or syrups used to package or prepare foods and beverages. This excludes natural sugars found in fruits and milks. In a prospective cohort study with 31,147 participants, researchers examined the US trends over time of added sugar consumption (percentage of daily calorie intake) and its association with CVD mortality. The researchers observed a dose–response relationship between the percentage of daily calorie consumption from added sugar and CVD mortality. 33 Consequently, both the 2015–2020 Dietary Guidelines for Americans and the 2019 ACC/AHA guideline urge Americans to minimize or entirely eliminate refined carbohydrate or sugar-sweetened beverage consumption.
Protein
Similar to fats, protein varieties also have divergent associations with cardiovascular outcomes. In longitudinal cohort studies, the association of animal and plant protein consumption with all-cause and cause-specific mortality was examined in 131,342 participants. 34 Animal protein intake was associated with higher cardiovascular mortality (HR 1.08 per 10% energy increment; 95% CI 1.01–1.16), while plant protein was inversely related to both cardiovascular mortality (HR 0.88 per 3% energy increment; 95% CI 0.80–0.97) and all-cause mortality (HR 0.90 per 3% energy increment; 95% CI 0.86–0.95). These data support the current recommendation to replace animal sources of protein with plant sources.
Diet and cardiovascular health – Understanding modern heart-healthy dietary patterns
In addition to studies analyzing individual dietary components and CVD outcomes, a number of dietary patterns have also been examined. Three particular diets have been linked to decreased risk of CVD, CHD, and mortality: the Dietary Approaches to Stop Hypertension (DASH) diet, the Mediterranean diet, and the healthy vegetarian diet. Although introduced decades ago, these dietary practices have soared in popularity more recently after the discovery of their cardiovascular benefits.
The DASH diet
The NHLBI first proposed the DASH diet in 1977 as a novel strategy to control hypertension. It consists of a diet rich in fruits, vegetables, lean protein, and low-fat dairy, and limits intake of sodium and saturated fats. The diet has been shown to reduce blood pressure among individuals with and without hypertension. 35 In 2003, the OmniHeart RCT demonstrated that the DASH diet lowers systolic blood pressure by 5–6 mmHg, diastolic blood pressure by 3 mmHg, reduces low-density lipoprotein (LDL) cholesterol levels by 11 mg/dL, and decreases the overall cardiovascular risk compared to diets that more closely resemble a typical American diet. 36 The DASH-Sodium trial also further confirmed these results and demonstrated a step-wise lowering of blood pressure as sodium intake was reduced. 37 The DASH dietary pattern has also been associated with decreased incidence of CVD and diabetes. 38 The AHA and USDA recognize the DASH diet as an ideal eating plan for Americans.
The Mediterranean diet
The Mediterranean diet is inspired by the eating habits of the countries bordering the Mediterranean Sea, such as Spain, Italy, and Southern Greece. It emphasizes: (1) high consumption of leafy green vegetables, fruits, nuts, legumes, wholegrains, and extra-virgin olive oil; (2) moderate consumption of lean meat, fish, poultry, and low-fat dairy; and (3) limited consumption of red meat and sweets. The major difference between this and the DASH diet is that the Mediterranean diet places less emphasis on dairy consumption and more emphasis on fruits, vegetables, whole grains, and seafood.
This diet has been shown to be beneficial for both primary and secondary CVD prevention and to reduce the risk of CVD mortality and all-cause mortality.39–42 The PREDIMED (Prevención con Dieta Mediterránea) study was the first large RCT to show that the Mediterranean diet reduces the risk of myocardial infarction, stroke, and death from cardiovascular causes when compared to a low-fat diet. 40 It is important to note there were methodological concerns with the original publication; however, the retracted and revised analyses came to similar conclusions. 40
The Mediterranean diet has also been proven to be beneficial for secondary prevention. In one trial, adherence to the Mediterranean diet was associated with reduced risk of major adverse cardiovascular events in patients with high-risk stable coronary artery disease. 42 Furthermore, patients post-myocardial infarction randomized to the Mediterranean diet experienced a 72% reduction in recurrent non-fatal myocardial infarction, and a 56% decline in mortality risk at 4 years of follow-up, compared to the cohort randomized to the AHA Step I diet (total fat < 30%). 41
Adhering to the Mediterranean diet is currently highly recommended due to its proven benefit for weight loss and protection against CHD and all-cause mortality.
The vegetarian diet
The vegetarian diet substitutes meat, seafood, and poultry with the consumption of soy products, whole grains, nuts, and legumes. Overall, the vegetarian diet is associated with a lower risk of CVD, a reduction in LDL cholesterol levels, and improvement of systolic blood pressure.34,43,44 However, there is a wide variety of vegetarian diet practices, and thus also a large range of reported impacts on CVD risks. The differences in outcomes come down to what foods people choose to replace traditional protein sources (meat, poultry, and seafood) with in their diet.
Satija et al. conducted a meta-analysis of 210,298 people eating vegetarian diets, and split the participants into 10 groups based on what proportion of their diets were made up of healthful foods (whole grains, fruits/vegetables, nuts/legumes, and oils) versus less healthful foods (juices/sugar-sweetened beverages, refined grains, potatoes, and sweets). 45 They found those with increased adherence to a more healthful vegetarian diet were 25% less likely to develop CHD. Contrastingly, those with diets consisting more of the unhealthful vegetarian foods were also 32% more likely to develop CHD. 45 The vegetarian diet is associated with many health benefits including reducing body mass index (BMI), improving cholesterol levels, and reducing systolic blood pressure. This leads many people to adopt it in an attempt to reduce their risk of CVD. However, it is important to note the above findings and appreciate that not all vegetarian diets are created equally.
Dietary patterns and cardiovascular health – Meal frequency and timing
While individual foods and nutrients are important, eating behaviors can also impact an individual’s heart health. A 2017 AHA statement addressed the impact of breakfast eating, meal frequency, and meal timing on cardiometabolic health. 46 Based on combined epidemiological and clinical intervention data, daily breakfast consumption can improve insulin and glucose metabolism and may slightly improve cardiometabolic risk profiles. Some epidemiological studies suggest a potentially harmful effect of nighttime meals on cardiovascular health, 47 but more clinical interventional trials are needed. Lastly, altering meal frequency, or the number of daily eating occurrences, under isocaloric conditions has not been proven to improve cardiometabolic risk factors. However, more regular energy intake throughout the day, with a greater proportion of calories earlier in the day, does have positive effects on CVD risk factors. Taken together, current AHA recommendations encourage intentional eating with mindful attention to timing and frequency of eating occasions (i.e. eating at planned intervals to evenly distribute energy consumption throughout the day). This may lead to heathier lifestyles and reduce cardiovascular risk.
Comparison of healthy diets for CVD prevention
In sum, the most evidence-based diets proven to lead to CVD prevention and weight loss include the DASH diet, Mediterranean diet, and vegetarian diet. The major national guidelines endorse diets with: (1) high consumption of non-starchy vegetables, fruits, wholegrains, and legumes; (2) moderate consumption of nuts, seafood, lean meats, low-fat dairy products, and vegetable oil; and (3) limited to no intake of trans-fats, saturated fats, red meats, sodium, refined carbohydrates, and sugar-sweetened beverages. It is important to understand that the proposed dietary models are more similar than they are different. They all encourage the consumption of non-processed fruits and vegetables, wholegrains, and lean protein while limiting intake of processed and sugar-sweetened products. This can be summed up nicely by Michael Pollan’s famous quote: ‘Eat food. Not too much. Mostly plants’.
Future diets: Emerging dietary trends and the need for more research
As mentioned, public interest in associating diet with cardiovascular health outcomes has shifted from a nutrient-specific approach of the past to dietary patterns of the present. Continuing this trend, a number of dietary fads have emerged and attracted considerable attention in popular culture, nutrition science, and clinical research. These include the intermittent fasting diet and low-carbohydrate, high-fat diets such as the ketogenic diet and Paleolithic diet. Below, we briefly discuss these emerging diets, but it is important to note they have not yet been endorsed by any major national guidelines. 48
The ketogenic diet, Paleolithic diet, and the intermittent fasting diet
The ketogenic diet involves a high intake of fats and proteins, while restricting carbohydrate consumption to as low as 20–50 g of carbohydrates daily. 49 Three meta-analyses investigating this diet have produced contrasting results of cardiovascular health benefits, weight loss, and long-term mortality.50–52 However, studying ketogenic diets is challenging, as the total fat and protein composition between studies differ and there is difficulty discerning if low-carb diets were legitimately ketogenic. 53 The Paleolithic (or ‘Paleo’) diet has also recently gained a following. This diet consists of foods assumed to have been available prior to human agricultural practices: lean meat, fish, vegetables, fruits, roots, eggs, and nuts, 54 and excludes grains, legumes, dairy products, salt, refined sugars, and processed oils. Only a handful of small studies have been performed studying the diet’s effect on cardiovascular health.54–57 Another diet pattern receiving significant attention is intermittent fasting. Fasting has been practiced by several populations including Muslims, Christians, Jews, Buddhists, and Hindus for millennia. Several studies have highlighted the weight loss benefit of this practice in obese and overweight patients.58–60 It is likely, however, that the mechanism of weight loss with intermittent fasting is in part due to reduction in overall total calorie intake.
Although increasing in popularity, the evidence for these proposed diets are currently limited. For this reason, no major societal guidelines have endorsed these diets to date. 48 Studies with more participants and longer study durations are warranted to reveal the health implications of these diets before they can be safely recommended to patients.
Current challenges in nutritional studies and nutritional counseling
Nutritional epidemiology – Considerations and future directions
For decades, societal dietary guidelines are published based on the most current observational studies relating diet to health outcomes. As mentioned, common issues in these observational studies include information bias, erroneous causal inferences, and confounding from social and behavioral factors.6–8 These issues can plague the dietary guidelines from which they are based. This lesson from the past has guided us to accept the current notion that RCTs provide the best evidence to shape guidelines. However, RCTs are difficult to conduct for dietary interventions as participants are not blinded, may not adhere to assigned dietary treatment, and long-term follow-up is required to evaluate for hard clinical outcomes. Thus, observational data will continue to play an important role in informing health promotion research and public health policy.
In light of this, it is critical to optimize observational study design and methods to provide the best quality evidence. Several research groups have proposed techniques to improve studies by reducing potential biases, which is an especially important consideration in nutritional epidemiology.7,8 Not only is diet a continuous set of multiple exposures over time, but it is also heavily connected to potential confounding variables like behavioral and social factors. These issues make it difficult to define causal relationships between diet exposure and disease. To address this, one team proposed a checklist to identify adequate source populations, test for validity of exposure measurement, assess for reverse causation, and adjust for confounders including socioeconomic status. 7 This checklist could ideally be used when reviewing and validating the data from any nutritional epidemiology study.
Additionally, methods to collect data, analyze them, and report findings lack transparency in the nutrition science literature. For example, food frequency questionnaires are commonly used to collect data on diet but have important limitations, including the inability to collect complex information or to capture variability in the consumption of foods. 6 Similarly, statistical methodologies employed by these studies are not always apparent in the analysis. To address this, some have proposed using a universal, standardized methodological approach to data collection, analysis, and reporting for each study. 6
Nutritional epidemiologic studies will continue to guide future policies and guidelines. Important future directions include reducing sources of bias and standardizing data collection, analysis, and reporting. Although there are inherent challenges to RCTs, they should be the preferred source to inform future guidelines and policy, as their limitations do not negate their importance in providing the best quality evidence.
The importance of nutrition counseling to patients
Nutrition counseling to patients during clinical visits is crucial to improving the population’s health for several reasons. First, the public is justifiably bewildered by the rapidly evolving dietary recommendations throughout the years. This is only further exacerbated by conflicting messages from the media, food industries, and commercial outlets pushing certain messages to meet their own agendas. Individual counseling allows practitioners to address false beliefs, caution patients about the limited scientific evidence for novel diets, and assure their familiarity with the current evidence-based dietary recommendations. Second, nutrition counseling plays a critical role in the primary and secondary prevention of CVD and its risk factors. 61 Third, obesity and poor diet substantially contribute to the slowed rate of improvement in CVD morbidity and mortality. Thus, weight-loss counseling and subsequent progress visits have never been so important.
In a recent review, Pallazola et al. provide guidance for clinicians regarding how to best advise patients on evidence-based heart-healthy diets during clinic visits. 62 Emphasis is placed on conducting a brief patient assessment to evaluate the patient’s lifestyle, goals, and barriers to interventions before effective counseling can occur. The authors also recommend asking patients what lifestyle modifications are both affordable and reasonable for them. These strategies allow the practitioner to then create a tailored lifestyle intervention plan for each patient. An initial recommendation, such as replacing sugar-sweetened beverages with water, can have a significant impact on CVD risk factors. For patients concerned with cost, providers can also suggest the consumption of low-cost, high-nutrient foods such as milk, yogurt, legumes, carrots, oatmeal, as well as low-sodium canned and frozen fruits, vegetables, and legumes. Going forward, it is imperative that clinicians become familiar with the evidence surrounding healthy dietary recommendations, and practice personalized counseling based on a patient’s medical history, health literacy, financial constraints, and cultural background.
Conclusions
The effective marketing of low-fat foods and guidelines emphasizing reduced fat intake may have synergistically contributed to increased refined carbohydrate intake, further propagating the obesity epidemic in the US. In the 21st century, nutrition research shifted focus from avoiding fat to an appreciation for balanced diets with an intake of healthier unsaturated fats. A wave of studies followed assessing the impact of specific macronutrients, foods, and diets on cardiometabolic health, informing our modern day understanding of dietary science. Presently, for improvement in CVD risk factors, the ACC/AHA guidelines recommend increased consumption of vegetables, fruits, legumes, nuts, whole grains, and fish, replacement of saturated fats with unsaturated fats, reduced consumption of sodium, cholesterol, refined carbohydrates, and sugar-sweetened beverages, and avoidance of trans-fats. The DASH, Mediterranean, and healthy vegetarian diets have the strongest evidence to-date for the reduction of CVD risk. With regards to nutritional epidemiology, key lessons from the past are to exercise caution when making causal inferences from observational data. Future directions will include appreciating the importance of food type and quality and continuing to investigate the clinical implications of emerging dietary trends. To facilitate these further investigations, methodologies in the field of nutritional epidemiology should be improved to address the challenges specific to these nutritional science studies. Furthermore, we should prioritize the inclusion of RCTs, which can better inform future public health practice and policymaking.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Michos is funded by the unrestricted Blumenthal Scholars fund for Preventive Cardiology at Johns Hopkins University.