
Abstract

Keywords
What are DOACs?
The term DOAC (pronounced ‘DOH-ack’) stands for ‘
Current FDA-approved DOAC medications.
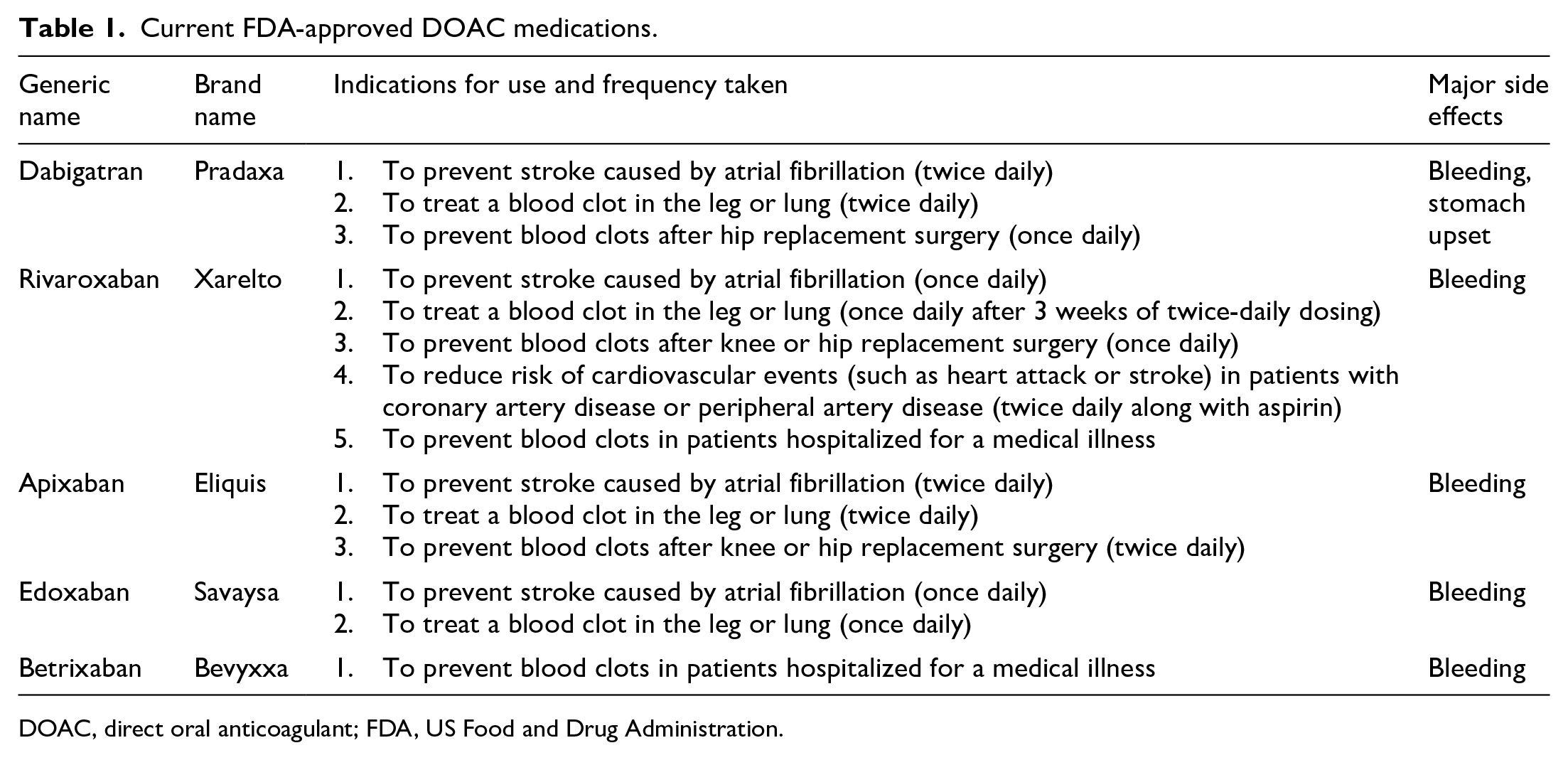
DOAC, direct oral anticoagulant; FDA, US Food and Drug Administration.
How do I know if I can take a DOAC?
A health care provider will consider several things to help decide if a DOAC is a good medication for each patient.
Am I taking the DOAC for the right reason?
DOAC medications should be used only for certain health conditions, such as atrial fibrillation (in the absence of heart valve disease), for the treatment or prevention of blood clots in the leg and/or lung (known as deep vein thrombosis and pulmonary embolism), or to prevent heart attacks and strokes caused by heart or blood vessel disease. Each patient should discuss with a health care provider whether a DOAC can be used for his or her condition.5–7
Are my liver and kidneys working well?
DOAC medications do not harm the liver or kidneys. Instead, these organs filter the medication out of the body. If the liver and kidneys are not able to filter out the medication, too much DOAC medication builds up in the blood and can increase the risk for bleeding. If a patient’s kidneys are not filtering well, his or her health care provider may prescribe a lower dose of a DOAC, or may prescribe warfarin instead, because warfarin does not require the kidneys to filter it from the body. Patients taking a DOAC should have a blood test to check kidney and liver function at least once every year.5,7
Will I need to monitor my INR while I am on a DOAC?
Warfarin is an unpredictable medication, and many factors influence the dose of warfarin needed for each patient. For that reason, health care providers use the international normalized ratio (INR) blood test to decide the right dose of warfarin. If a patient regularly takes his or her warfarin and gets INR blood tests but still the INR does not stay within the goal range, a DOAC may be a good choice to provide better and more consistent protection from forming blood clots. Because the DOACs are very predictable medications, patients taking a DOAC do not usually need regular blood testing to adjust the medication dose. Some patients who are familiar with taking warfarin may ask: ‘If I take a DOAC and am not getting my INR checked, how do I know if I am OK?’. The INR is specific to warfarin and will not provide helpful information for patients taking a DOAC. Also, many studies have shown that the DOAC dose is safe, effective, and predictable for most patients without the need for regular blood testing. 7
Some patients who take warfarin may have a hard time coming to a clinic or lab to get the INR blood test needed to adjust the dose of warfarin. In this case, a DOAC medication may be a good choice since no INR blood testing is needed. 7
What if I have trouble remembering to take medications?
DOACs begin working faster than warfarin. They also leave the body faster than warfarin. For example, a DOAC thins the blood and gives full blood clot protection within a few hours after the first dose, and then it leaves the body in about a day. With warfarin both processes can take several days. This difference is important to remember. Because DOACs leave the body so quickly, it is essential to take the DOAC every single day (or twice a day) as prescribed and it should not be stopped unless advised by a health care provider.5,7
Will I have to keep a consistent amount of vitamin K-containing foods in my diet?
For patients taking warfarin, eating a consistent weekly amount of vitamin K foods (like broccoli, spinach, or kale) can help keep the INR in range. If a patient changes his or her diet frequently, the INR can fluctuate. In contrast, the DOACs are not affected by foods containing vitamin K. 5 The DOACs work differently from warfarin, so patients taking a DOAC can eat as many or as few vitamin K foods as they choose without affecting the blood-thinner medication.
Can I afford to pay for the DOAC?
Before deciding to take a DOAC, the patient should find out the monthly cost of the DOAC medication and decide if he or she can afford that cost every month. When necessary, health care providers may help a patient find this information. Certain health insurance prescription plans may cover one DOAC but not another. 7
How do I change from warfarin to a DOAC?
If you and your health care provider decide to switch from warfarin to a DOAC, you will first need to have your INR tested. Based on your INR, your provider will give you specific instructions for when to stop warfarin and when to start the DOAC. 6
Are there medication interactions with DOACs?
Some medications may interact with the DOACs and cause the blood to be thicker or thinner.5,6 This interaction, in turn, may increase the risk of blood clots or bleeding, depending on the medication. It is important that patients taking any type of blood thinner let all their health care providers know they are taking the blood-thinner medication and ask the provider or pharmacist to check for interactions any time a new medication is prescribed. 7
Do I need to stop my DOAC before a surgery or procedure?
For some types of surgeries and procedures, patients taking DOACs will need to stop taking the DOAC before the procedure to prevent a bleeding problem during or soon after the procedure. 8 The plan for stopping a DOAC before surgery and restarting a DOAC after surgery is different for everyone. The plan will depend on the type of procedure, specific DOAC, and the patient’s kidney function. For example, procedures unlikely to cause bleeding, such as cataract surgery or dental extractions, may not require stopping the DOAC at all. In contrast, when patients have procedures that have a higher chance of bleeding in a critical area of the body (e.g. spinal surgery or colonoscopy with colon polyp removal), it is important to stop the DOAC for at least 2 days before the procedure. The DOAC may be restarted 1 or 2 days after the procedure, depending on the concern for bleeding. Patients taking a DOAC should talk with the provider performing the procedure and the provider who prescribed the DOAC to decide on the best individual plan.
What if I have a bleeding problem while taking a DOAC?
Bleeding is a common side effect of all blood thinners, including the DOACs. Several things can be done to lower the risk of bleeding while taking a DOAC (Table 2). Some bleeding problems are minor, while others are more serious and require medical attention. Patients who have a serious bleeding problem while taking a DOAC should either call 911 or go to the emergency room of the nearest hospital. Patients taking a DOAC should consider a medical alert bracelet or wallet card that lets emergency medical staff know about the DOAC. Medical staff at the hospital will perform an examination and do some blood tests. It is important to tell the medical staff what time the most recent dose of DOAC medication was taken. DOACs begin to leave the body within a few hours. In a serious bleeding situation, the medical staff may give intravenous fluids and possibly a blood transfusion.
Practical approach to decreasing bleeding risks with DOACs.
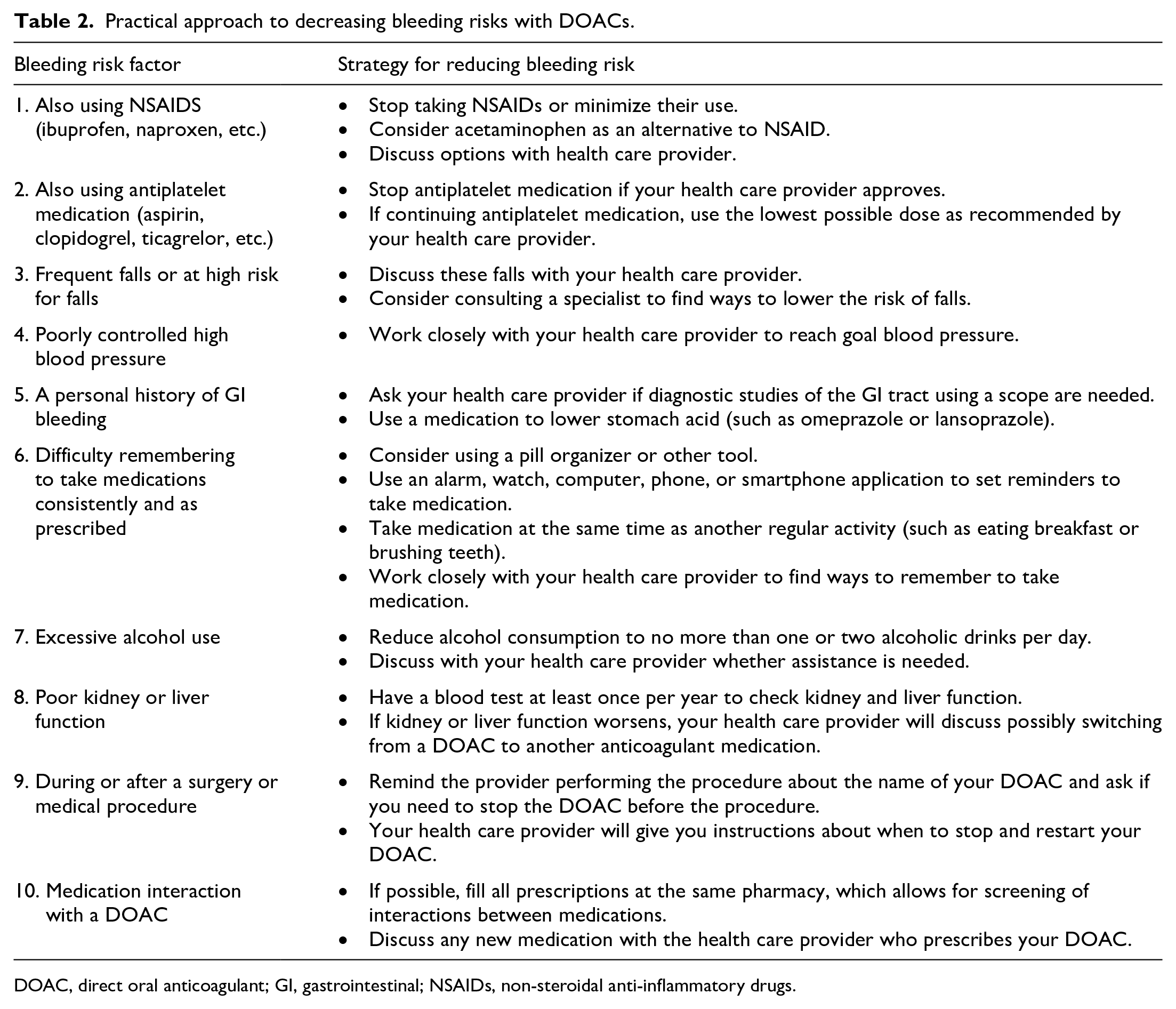
DOAC, direct oral anticoagulant; GI, gastrointestinal; NSAIDs, non-steroidal anti-inflammatory drugs.
Are DOACs reversible?
In a life-threatening bleeding situation or when a patient requires urgent surgery, medical staff may also give an antidote, which is a drug that is given to rapidly reverse the effects of the DOAC. For example, idarucizumab reverses dabigatran, and andexanet alfa reverses rivaroxaban and apixaban. These antidotes are very effective at reversing DOAC effects and helping to stop bleeding but may increase the risk of blood clots. Medical staff will use these costly antidotes carefully to ensure patient safety. 9
Do I still need to follow-up with an anticoagulation provider if I take a DOAC?
Even though patients taking DOAC medications do not need regular INR blood testing, it is still important to have regular contact with a health care provider.5–7 This provider can make sure that patients have on-time medication refills, answer questions about how to take DOAC medications before and after surgeries or procedures, help check for medication interactions, check kidney and liver blood tests, and answer any questions about bleeding or other side effects from DOACs.
How do I choose which DOAC to take?
Patients should work closely with their health care provider to determine which DOAC is best. They should talk about the differences, including once- versus twice-daily dosing, needing to take the DOAC dose with food versus at any time, the approved indications for use, and side effects (Table 1). In addition, there may be other factors the health care provider will discuss.5,7 These could include any problems with kidney or liver function, weight, and personal preferences.
Summary
DOACs are a group of oral blood-thinner medications that may have some advantages over warfarin. A health care provider will look at several different factors to help patients decide if a DOAC is a good choice. Patients taking DOACs should discuss medication changes, a plan for taking the DOAC before and after surgery, and any bleeding side effects with their health care provider.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage.
The Vascular Disease Patient Information page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Acknowledgements
This article is an update to the original version written by Sara Vazquez and Matthew Rondina in 2015.7
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sara R Vazquez is an editorial consultant for UpToDate® and a member of the Anticoagulation Forum Board of Directors.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.