
Abstract
Giant cell arteritis (GCA) is the most common vasculitis in adults. However, comprehensive analyses of the healthcare burden are still scarce. The aim of the study is to report the healthcare burden and cost of illness of GCA in the Friuli Venezia Giulia (FVG) region of Italy, based on a data linkage analysis. To this end, a retrospective study was conducted through the integration of many administrative health databases of the FVG region as the source of information. Cases were identified from two verified, partially overlapping sources (the rare disease registry and medical exemption database). From 2001 to 2017, 208 patients with GCA were registered. The prevalence of GCA in the population aged ⩾ 45 years as of December 31, 2017 was 27.2/100,000 inhabitants (95% CI 23.5–31.4). The mean time of observation was 4.5 ± 3.6 years. A total of 3182 visits (338 per 100 patient-years) was recorded. The most frequent specialty visits were rheumatology (n = 610, 19.2%), followed by internal medicine (n = 564, 17.7%). A total of 287 hospitalizations (30 per 100 patient-years) were reported. A total of 13,043 prescriptions (1386 per 100 patient-years) were registered. More than half of the patients were prescribed an immunosuppressive agent. The overall estimated direct healthcare cost was €2,234,070, corresponding to €2374 per patient-year. Overall, GCA is a rare disease which implies a high healthcare cost.
Introduction
Giant cell arteritis (GCA) is the most common systemic vasculitis in persons aged 50 and above. 1 The most important feature that can greatly affect the quality of life is eye involvement, that can lead to visual loss in 20–30% of patients, due to an ischemic optic neuropathy. This justifies a prompt therapeutic intervention with glucocorticoids once the diagnosis has been suspected. Emergency departments, neurology units, vascular surgeon units beside rheumatology or internal medicine units are often involved in the diagnostic work-up of GCA, which comprises laboratory testing, imaging studies, and temporal artery biopsy (TAB). The standard treatment is with glucocorticoids for long-term use, but they can lead to many dangerous adverse effects. Immunosuppressive agents, such as methotrexate or more recently tocilizumab, the monoclonal anti-interleukin (IL)-6 receptor antibody, appear to be useful to lower the recurrence rate and save steroids.1,2
Since GCA is a rare disease, accurate estimates of incidence and prevalence are difficult to obtain and there are limited data on healthcare burden and resource consumption. Fast and easy access to epidemiological information, though, would be crucial, not only to plan diagnostic and therapeutic approaches but also to monitor outcomes and change the management of the disease, accordingly. The integration of administrative databases by a clinical and epidemiologic task can be the way to reach this end. Herein, we report the healthcare burden and cost of illness of GCA in the Friuli Venezia Giulia (FVG) region of Italy, based on a 17-year integrated analysis of several health databases, the result of the local network of rheumatologists and epidemiologists.
Patients and methods
Data source
This retrospective cohort study was based on the administrative data of the regional health information system of FVG, a 1,200,000-inhabitant region located in the northeast of Italy. The System covers the entire regional population and includes several health-related databases, which are completely anonymous and with no possibility of identifying subjects; nonetheless, databases can be linked with each other at the individual subject level through a univocal encrypted stochastic key.
For this research, we analyzed and matched the following databases: the database of regional potential healthcare beneficiaries, the hospital discharge database, the ambulatory care database, the pharmaceutical prescription database, the emergency department (ED) database, the mortality database, the anatomic pathology database, the database of exemptions from medical charges, and the regional rare disease registry. Of those databases, two were used to identify GCA cases living in FVG: the exemption database – where patients with GCA may be found if the disease entitles them to receive free medical care, and the rare disease registry – where patients with GCA may be found since 2009 if they were visited and recorded by a specialist doctor in a center included in the Regional Rare Disease Network. Since none of the two databases is complete, due to competing causes of exemption from medical charges and incomplete/ongoing case registration in the rare disease registry, we ensured the maximum case ascertainment by considering both data sources (see online supplemental material).
All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Since this analysis was based on anonymous administrative data, patient-informed consent and Ethical Committee approval were not required in Italy.
Measures
We assessed the overall case identification rate of GCA in FVG by sex and age group, from the 5-year age category including the youngest incidence case to the category ⩾ 90 years of age. The annual regional populations of FVG were used as the denominator for the rates. We also calculated the annual case identification rates, sex and age-standardized on the Italian population of the median year of observation (2009), according to the Italian National Institute of Statistics, namely ISTAT (http://demo.istat.it/), to evaluate any trends in registration regardless of changes in the regional population structure during the study period. We expected that case identification rates were low before the rare disease establishment, and progressively approached the true incidence rate after the registry run in phase. Thus, we considered the 2017 case identification rate as our best estimate of the true GCA incidence rate. For that year, we estimated the crude GCA incidence rate. We also estimated the prevalence of GCA in FVG as of December 31, 2017, using the 2017 regional population as the denominator. Confidence intervals for rates and prevalence were estimated based on the mid-p exact method.
We also described the demographic characteristics of subjects registered as patients with GCA in terms of the frequency of their ED visits for the most common symptoms associated with the disease, the frequency of ambulatory specialist visits, the prescription of medications, the frequency and cause of hospitalization, the causes of death, the average direct healthcare costs per patient-year – calculated as the sum of the costs for outpatient visits, hospitalizations, and medications divided by the total person-years of observation. The estimated cost of drug prescriptions is different depending on the type of medicine and mode of distribution. For drugs retrieved by patients at community pharmacies, the cost is the drug public price with the application of discounts set by the law,3,4 whereas for drugs bought directly by the regional health system and either distributed by hospitals upon a patient’s discharge or by community pharmacies on behalf of the regional health system, the cost is based on negotiations between pharmaceutical manufacturers and the regional health system, and also, when community pharmacies are involved, on agreements stipulated with wholesalers and pharmacy associations. 5 On the other hand, tariffs were used to estimate the costs of hospitalizations and ambulatory care. In particular, we used diagnosis-related group (DRG) tariffs as proxies of the hospitalization costs, although they may not correspond to the real production costs. 6 For ambulatory care, we used regional tariffs (per unit of service), which are adopted in FVG to fund healthcare providers. 7 All the analyses were conducted using SAS software, Version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Epidemiology
From 2001 to 2017, 208 patients with GCA were registered in FVG. Seventy percent of patients were female (n = 146). Age at registration ranged from 48 to 91 years, with a mean of 71 ± 9 years. The prevalence of GCA in the regional population aged ⩾ 45 years as of December 31, 2017 was 27.2/100,000 inhabitants (95% CI 23.5–31.4). Before the establishment of the rare disease registry in 2013, the case identification rate in the population aged ⩾ 45 years was very low; the large majority of patients were registered in the last 5 years, with a spike in registration in 2013 corresponding to an intense promotional activity by the Regional Rare Disease Coordinating Center (Figure 1). The crude identification rate in 2017 (i.e. our best estimate of the incidence rate) in the population aged ⩾ 45 years was 3.8/100,000 person-years (95% CI 2.5–5.5). The maximum rate was observed in the age group 70–74 years (see online supplemental material).
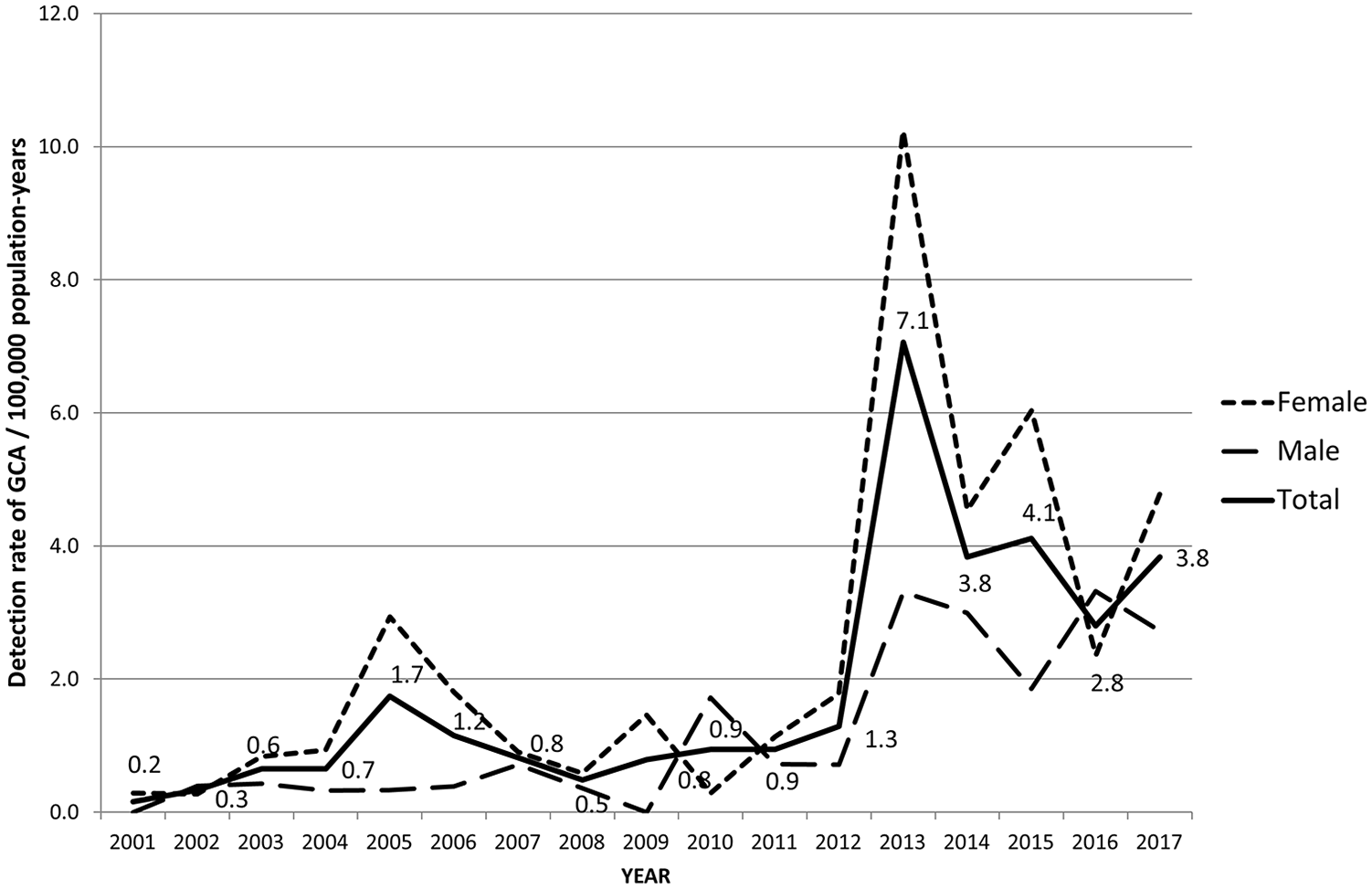
Annual detection rate of GCA per 100,000 person-years in the population aged ⩾ 45 years from the Italian region of Friuli Venezia Giulia (2001–2017) standardized on the 2009 national population.
Of all 208 cases, 109 (52.4%) underwent TAB in one of the regional pathology laboratories: in 69/109 (63.3%), the biopsy was compatible with the suspicion of GCA, showing inflammation in the vessel wall (41/69, 59%) or in the presence of giant cells (28/69, 41%). In 11/109 (10%) cases, there was arterial fibrosis, or arteriosclerosis, or other findings (atheroma, congestion, calcium deposit). Finally, in 29/109 (26.7%) cases, no alterations were detected.
Healthcare burden
In our cohort, patients contributed to an average of 4.5 ± 3.6 years of observation (median 3.9), totaling 940.8 years of observation. During the observation time, 44 patients were visited at the ED because of headache, visual loss or pain, for a total of 59 visits (6.3 per 100 patient-years). Of all ED visits, nine (15%) were due to headache, 17 (29%) to abdominal pain, 15 (25%) to thoracic pain, 17 (29%) to other pain, and one to GCA with no symptom specification.
A total of 192 patients had at least one ambulatory specialist visit, from a total of 3182 visits (338 per 100 patient-years). The most frequent specialties where visits were needed were rheumatology (n = 610, 19.2%), internal medicine (n = 564, 17.7%), ophthalmology (n = 292, 9.2%), orthopedics (n = 191, 6%), ENT (n = 163, 5.1%), cardiology (n = 126, 3.9%), neurology (n = 72, 2.2%), dermatology (n = 71, 2.2%), oncology and hematology (n = 53, 1.7% and 85, 2.7%, respectively), and pulmonology (n = 40, 1.3%).
A total of 108 (52%) patients had at least one hospitalization, from a total of 287 hospitalizations (30 per 100 patient-years). The categories of main discharge diagnoses are illustrated in Figure 2. Circulatory diseases were the most common, followed by musculoskeletal conditions.
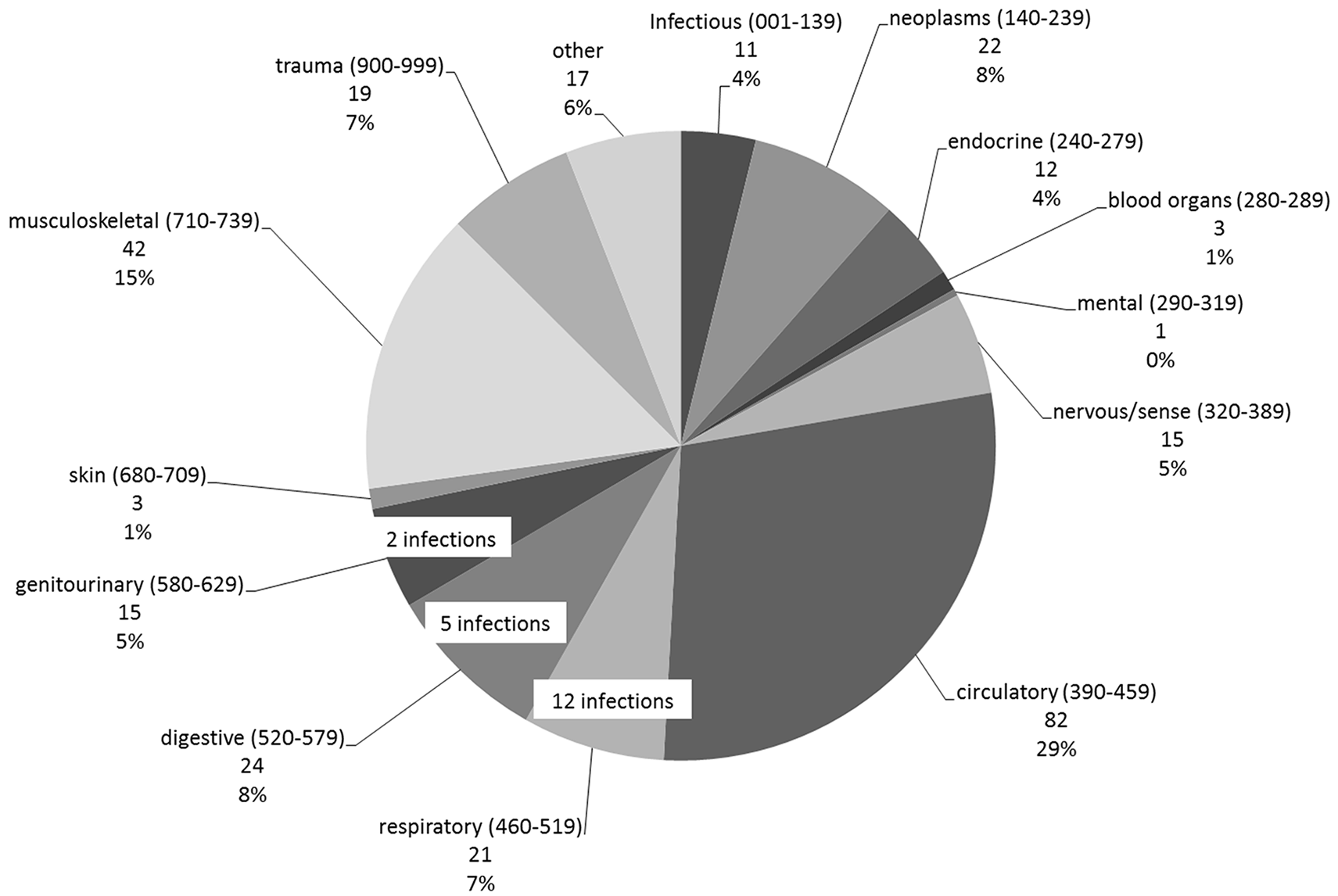
Distribution of the categories of main discharge diagnoses as ICD-9-CM codes for 287 hospitalizations of patients with GCA in the Italian region of Friuli Venezia Giulia (2001–2017).
Twenty-one subjects died during the observation period. Mean age at death was 83 ± 7.6 years (median 86, range 66–93), slightly higher than the regional mean age at death in FVG (81.9 years). 8 Causes of death are shown in Table 1. As reported, the main causes of death were cardiovascular or cerebrovascular diseases (10/21, 47.6%), cancer (6/21, 28.6%), or respiratory tract diseases (4/21, 19.0%).
Causes of death, as ICD-9-CM codes, among the cohort of patients with GCA in the Italian region of Friuli Venezia Giulia (2001–2017).
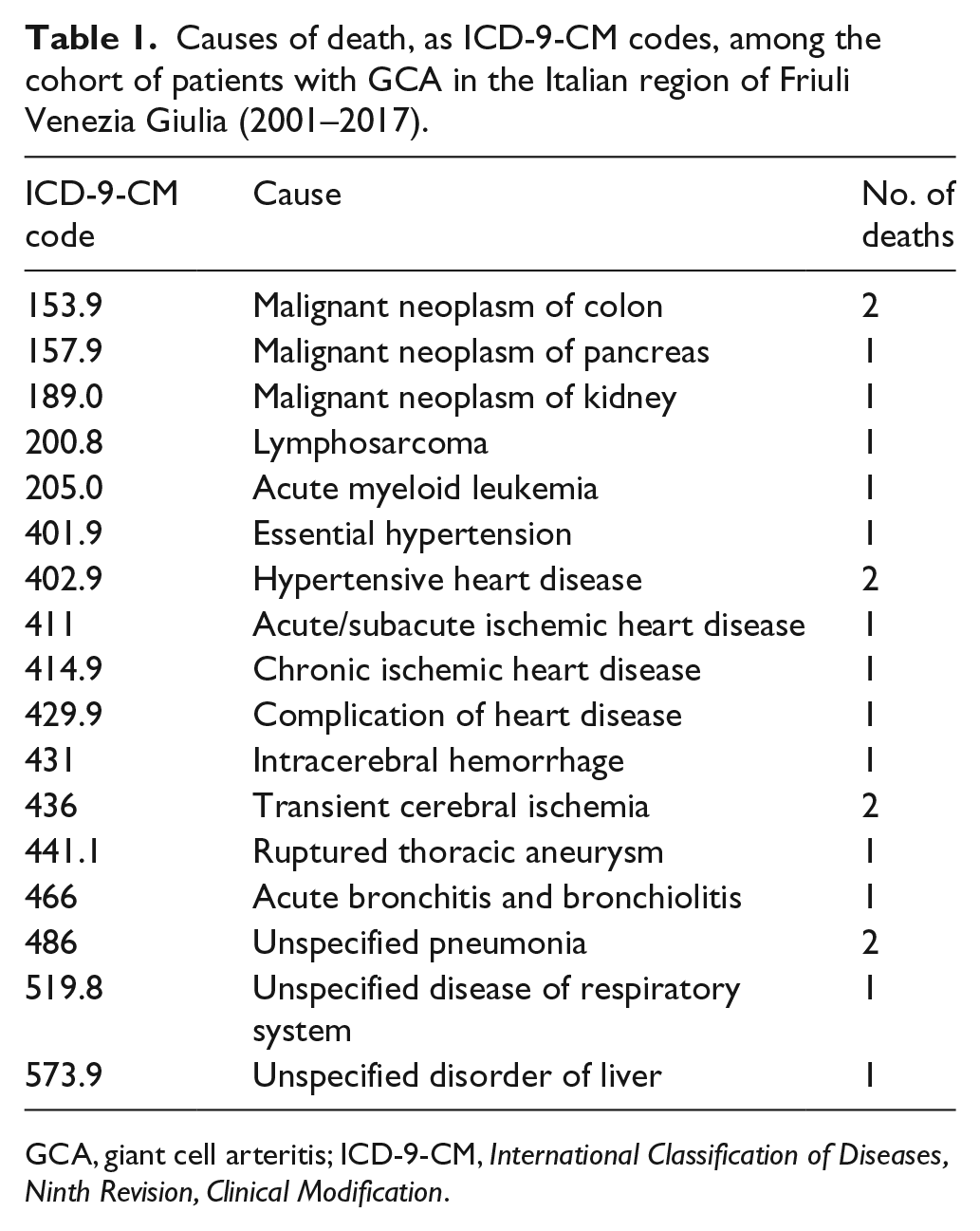
GCA, giant cell arteritis; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification.
Medications
After being officially registered either in the exemption database or in the rare disease registry, 199 individuals were prescribed medications among those of interest, for a total of 13,043 prescriptions (1386 per 100 patient-years). Overall, 186 (89.4%) patients were reported to be treated with glucocorticoids and/or immunosuppressive agents after they were registered for the exemption and/or enclosed in the registry (but if we also consider medications prescribed before being registered as GCA patients, we observe that all patients but one had used glucocorticoids). Of patients using glucocorticoids after registration, 82 (44%) only used glucocorticoids, whereas 98 (53%) were also prescribed an immunosuppressive agent. Six patients (3%) took only immunosuppressive agents. Cardiovascular medications were prescribed to 154 (74%) patients: 144/154 (93.5%) used low-dose aspirin, and 99 of them did not use any anticoagulant drug; there were 18 ever-users of traditional anticoagulants and nine of new oral anticoagulants. The statin users were 89/199 (44.7%), atorvastatin being the most prescribed drug, followed by simvastatin, rosuvastatin, and pravastatin. In 116 patients (56%), bisphosphonates were prescribed to ensure bone protection; three patients needed teriparatide and four denosumab.
The frequency of prescriptions for each of the drugs of interest and the number of patients with prescriptions for each medication are shown in the online supplemental material. Glucocorticoids accounted for 42% of all prescriptions: over 60% of patients received at least one prescription of prednisone and over 40% received methylprednisolone. Immunosuppressive agents accounted for 8%. Low-dose aspirin represented more than one-fourth of prescriptions and it was prescribed to two-thirds of patients, whereas the new oral anticoagulants were less than 1%.
Costs
The overall estimated direct healthcare cost for 940.8 patient-years was €2,234,070, corresponding to €2374 per patient-year (61 for outpatient visits, 1661 for hospitalizations, 312 for prescribed medications, and 340 for medications directly dispensed by the hospital pharmacies).
For comparison, in 2017 the estimated healthcare cost for the general population of Udine Province (about 500,000 inhabitants, the area of FVG with the highest population density) and the estimated healthcare cost for patients suffering from diabetes (i.e. a chronic disease often complicated by ocular involvement and cardiovascular disease), applying the same methods, were €1163 and €2674, respectively (unpublished data).
Discussion
The present study reported a 17-year observation in a cohort of patients with GCA, through the integrated analysis of multiple healthcare system databases. Validation of this epidemiologic approach has been previously provided. 9 Importantly, a high level of integration was carried out among many healthcare databases, which included the hospital discharge database, the ambulatory care database, and the ED database (including records from all the regional hospitals – either public or private accredited to the public health system), the pharmaceutical prescription database (which contains information on all the prescriptions made by physicians working in the public health system – except prescriptions paid out-of-pocket), the mortality database (which includes data on all deaths of the individuals living in the region), the database of exemptions from medical charges (which includes records on all the potential healthcare beneficiaries who are entitled, because of low income, age, or chronic diseases, to receive free medications and outpatient specialist care), and finally even the anatomic pathology database (which includes information on all the cytological and histological examinations performed in the region to inpatients and outpatients). Interpretation of the results was performed by a team of rheumatologists and epidemiologists.
Overall, even if GCA does not affect mortality, the health system resource consumption seems very high for a rare disease, and it reflects the high level of morbidity of the disease in these first two decades of the third millennium.
Epidemiology
The prevalence of GCA in our regional population aged ⩾ 45 years as of December 31, 2017 was 0.027% (95% CI 0.023–0.031). Overall, the prevalence of GCA is still poorly reported, and the available data gave contrasting results, probably due to the different methods applied.10,11
In our study, the incidence, based on the crude identification rate in 2017 (i.e. our best estimate of the incidence rate) was 3.8/100,000 person-years (95% CI 2.5–5.5), with a trend towards an increase of incidence with age. This incidence is lower than that reported by Salvarani et al. in Reggio Emilia, Italy 12 (6.9/100,000, in a population aged ⩾ 50 years, over a 9-year period (1980–1988)), but closer to the incidence of GCA in Germany (3.5 per 100,000 inhabitants per year in the over-50 age group). 13 Nevertheless, the prevalence and the incidence estimates are lower than expected, depending on the methods, which focused on a 1-year observation (i.e. 2017) with a small sample.
About one-half of the patients did not undergo TAB for diagnosis in our cohort. This is not surprising since in the tocilizumab trial (GiACTA), where the diagnosis of GCA was based on the results of TAB or on evidence of large-vessel vasculitis on imaging study, the proportion of patients with GCA diagnosed by positive imaging was 46%. 2 Positive biopsy for the presence of granulomatous inflammation was observed in a total of 26% of the patients, consistent with other works which focused on this issue.14,15 These results further support the actual international guidelines for the diagnostic work-up of GCA. 16
Healthcare burden
The healthcare burden of the disease is concentrated in three specialties, such as rheumatology, internal medicine, and ophthalmology. This distribution clearly reflects the role of the rheumatologist in the primary care of the disease, both in the context of rheumatology clinics or in the internal medicine unit. Moreover, the placement of ophthalmology indicates the importance of eye involvement, since it is known that any loss of vision is irreversible. 17
Hospitalization and comorbidity
Interestingly, while mortality is not affected by GCA, 18 morbidity is very increased. A half of the patients showed at least one hospitalization, and the main discharge diagnoses concerned cardiovascular disease, including aortic aneurysms or dissections, followed by musculoskeletal conditions. Cardiovascular disease was also the main cause of death in this population, consistent with the higher cardiovascular risk observed in other chronic inflammatory rheumatic diseases. Thus, it is not surprising that three-quarters of our patients took cardiovascular drugs – low-dose aspirin being the most prescribed drug of this class. Notably, statins were also prescribed to almost half of the patients, thus reinforcing the idea that patients with GCA are a high-risk group of patients for cardiovascular disease.
A recent comprehensive analyses of cause-specific death patterns in GCA in France, using a large death certificate database, revealed that GCA is associated with increased risk of dying from large-vessel disease (aortic aneurysm and dissection), other cardiovascular diseases, and potentially treatment-related comorbidities, including diabetes and opportunistic infections. 19 Low-dose aspirin, owing to its antiplatelet effect, has been shown to prevent ischemic events such as strokes and myocardial infarctions in patients with atherosclerotic cardiovascular disease. There is currently no evidence from RCTs to determine the safety and efficacy of low-dose aspirin as an adjunctive treatment in GCA. 20 In GCA, low-dose aspirin may decrease the incidence of cranial ischemic complications.21,22 Since there have been reports of ischemic complications developing in a substantial number of patients soon after GCA was diagnosed and treatment was started, or later during tapering of the dosage of steroids, 23 patients with GCA may benefit from the addition of low-dose aspirin to the steroid treatment. Also, aspirin was reported to have action complementary to steroids in suppressing inflammation in GCA, predominantly by suppressing interferon-γ.24,25
Moreover, clinicians must also recognize the established hemorrhagic risks associated with aspirin, especially in the context of concurrent treatment with glucocorticoids.
Treatment
High doses of glucocorticoids are the cornerstone of the treatment for GCA. 1 Many of the patients start an immunosuppressive drug in order to spare glucocorticoids, since the risk of developing serious adverse events, such as diabetes, glaucoma, osteoporosis, fractures, serious infection requiring hospitalization, and death, is strictly related to the high and prolonged doses of glucocorticoids. 26 Based on three meta-analyses, methotrexate may decrease the risk of recurrences, and then the cumulative glucocorticoid exposure in GCA,27–29 while one recent international trial led to the licence of TCZ in the treatment of GCA. 2 In our cohort, less than 50% of the patients were treated with glucocorticoids alone, while the majority received immunosuppressive agents. This therapeutic approach could explain the low incidence of hospitalized infections in our patients. Nevertheless, one of the important complications among patients with GCA who received glucocorticoids in the long term (> 3 months) is the steroid-induced osteoporosis that leads to an increased risk of fracture. 30 Generally, risk of fracture in patients who received long-term glucocorticoids is doubled and it depends on the daily and cumulative dose. 31 Consistent with that, the other specialism frequently involved in the management of GCA is orthopedics, as emerged in our cohort. In addition, more than 50% of the patients took bisphosphonates as a prophylactic osteoporosis medication or treatment for osteoporosis. In a recent work evaluating the adherence to prophylactic osteoporosis medication, 117/118 patients (99.2%) were prescribed calcium and vitamin D, while only 61/118 (51%) patients were prescribed bisphosphonates for polymyalgia rheumatica/GCA. 32 As patients may be on steroids for many months or even years, it is appropriate to consider for all patients a concomitant prescription of bisphosphonates and calcium/vitamin D therapy when steroid treatment begins. This is particularly important because GCA may occur in older people who are already at greater risk of osteoporosis.
Medical costs
It is known that direct medical outpatient costs in GCA were increased in the month preceding and in the first 4–5 years following GCA diagnosis. Higher use of outpatient physician, laboratory, and radiology visits, and ophthalmologic procedures were responsible for the increased cost of care, accounting for a median incremental cost attributed to GCA over a 5-year period of $4662, if compared to a matched referent cohort in the USA, and amounting to €1342 for the first 6 months, €1498 between 6 and 12 months, and €1165 between 12 and 18 months in France.33,34 In our cohort, the overall estimated direct healthcare cost was €2374 per patient-year, and it was largely determined by the costs for hospitalizations (70%) and medications (27.5%), clearly highlighting the most important outcome for new treatments (i.e. the lowering of the hospitalization rate for GCA).
Interestingly, as a chronic disease, the healthcare cost of GCA was very similar to that estimated for diabetes (i.e. a chronic disease with possible ocular involvement and carrying a high cardiovascular risk), and it was two times higher than that calculated for the general population. Thus, GCA is a chronic rare vasculitis that absorbs many resources, like more frequent and popular chronic diseases, with similar outcomes in terms of complications.
Strengths and limitations
The main strength of this study is the complete regional coverage of all the health administrative databases used in the analyses, which ensures that the estimates of the case registration rate and of the prevalence of GCA are population-based. The use of full-coverage administrative databases for the assessment of the healthcare burden, in terms of medication use, ambulatory care, hospitalizations, and mortality, also minimized the risk of information bias. Another advantage of analyzing data from the regional health information system is the information was available on a very long time span, allowing us to set up and study a relatively large cohort of GCA patients, despite the rarity of the disease. Notably, this integrative analysis included the anatomic pathology database of the region. In addition, the interpretation of the results was made on a clinical and epidemiologic ground. A primary limitation is the racial composition of the population of the FVG region, which is mostly Caucasian. Thus, this does not allow to extrapolate results to non-Caucasian populations. However, herein the study clearly confirmed that GCA is a costly disease, and this can be applied to any country. The second important limitation of this study is the suspected incompleteness of case ascertainment in the first years of operation of the rare disease registry, as suggested by the GCA detection rates before 2013. The detection rate in the last available year (i.e. 2017) is our best estimate of the true incidence rate in the FVG; however, the rate estimate for a single year is imprecise since it is based on a limited number of cases and it does not take into account the variation of incidence over the years. Maintaining accuracy of case registration in the next years will permit the gaps to be filled and allow more precise estimates of the incidence rate.
Conclusion
This 17-year analysis of regional databases focusing on a rare disease such as GCA allows us to perform a snapshot of the healthcare burden of the disease and plan future approaches to improve its management and cost. Morbidity, especially adverse events secondary to long-term exposure to glucocorticoids, is the main issue that affects patients with GCA. Clinicians and healthcare system decision-makers must be aware that eye involvement, cardiovascular disease, and bone preservation are the main clinical domains where the management of GCA should be focused in the long term. Importantly, the healthcare costs of GCA seem to be very close to those observed in another disease which can affect the eyes and cardiovascular system – diabetes. New treatments should aim to prevent hospitalizations for GCA and to eventually save on the costs of the illness.
Supplemental Material
10.1177_1358863X19886074_Supplemental_files – Supplemental material for Data linkage analysis of giant cell arteritis in Italy: Healthcare burden and cost of illness in the Italian region of Friuli Venezia Giulia (2001–2017)
Supplemental material, 10.1177_1358863X19886074_Supplemental_files for Data linkage analysis of giant cell arteritis in Italy: Healthcare burden and cost of illness in the Italian region of Friuli Venezia Giulia (2001–2017) by Francesca Valent, Milena Bond, Elena Cavallaro, Elena Treppo, Da Riol Rosalia Maria, Annarita Tullio, Christian Dejaco, Salvatore De Vita and Luca Quartuccio in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.