
Abstract
Antiplatelet therapy is commonly prescribed following endovascular interventions. However, there is limited data regarding the regimen and duration of antiplatelet therapy following lower extremity endovascular interventions. The aim of this study was to investigate the practice patterns of dual antiplatelet therapy (DAPT) after lower extremity endovascular interventions. We identified all patients who received an endovascular intervention in the Vascular Study Group of New England (VSGNE) registry from 2010 through 2018. The antiplatelet regimen was examined at the time of discharge and follow-up. Variables predicting discharge antiplatelet therapy and duration of antiplatelet therapy were investigated. There were 13,510 (57.69%) patients discharged on DAPT, 8618 (36.80%) patients discharged on single antiplatelet therapy, and 1292 (5.51%) patients discharged without antiplatelet therapy. Patients with coronary artery disease (CAD), prior vascular bypass and endovascular intervention, preoperative statin use, stent placement compared with angioplasty, and femoropopliteal and tibial treatment were associated with higher odds of being discharged with DAPT compared with no antiplatelet therapy and single antiplatelet therapy. Of the patients discharged on DAPT who were followed up at 9–12 months and 21–24 months, 56.49% and 49.63% remained on DAPT, respectively. Only a narrow margin of the patient majority undergoing endovascular interventions was discharged with DAPT, suggesting that only a small proportion of patients undergoing endovascular intervention remain on DAPT long-term. As the number of peripheral vascular interventions continues to grow, further studies are crucial to identify the optimal duration of DAPT.
Introduction
Peripheral artery disease (PAD) is a common disorder, affecting up to 15–20% of people over the age of 70 years. 1 Endovascular interventions are among the most commonly performed procedures for lower extremity revascularization in the setting of PAD, and continue to increase each year.2,3 Antiplatelet therapy is often prescribed following endovascular interventions to prevent thrombosis by inhibiting platelet aggregation. 4 This regimen typically consists of single or dual antiplatelet therapy (DAPT) including aspirin or a P2Y12 receptor blocker, and is associated with a decrease in lower extremity ischemic events.5,6 Furthermore, several studies have suggested an additional cardiovascular benefit to DAPT in patients with PAD.7–9
Although there are established guidelines within the cardiac literature regarding the recommended length of DAPT following percutaneous coronary intervention based on multiple large, randomized controlled trials, no such data exist in the peripheral vascular literature. 10 Data regarding antiplatelet therapy is sparse, and limited by small sample sizes and short-term outcomes.11,12 It is unclear how long patients remain on antiplatelet therapy following endovascular intervention in a real-world setting, and what factors influence initiation of an antiplatelet regimen. Thus, we sought to use the Vascular Study Group of New England (VSGNE) registry to identify the practice patterns of DAPT following endovascular intervention.
Methods
Database
A retrospective analysis was performed on patients within the VSGNE registry, which is a prospectively collected regional database including more than 35 academic and community hospitals. Details regarding the VSGNE registry have been previously published, and additional information can be located at https://www.vqi.org/regional-groups/current-regional-quality-groups/vascular-study-group-of-new-england/. 13 As the registry consisted of deidentified data, no individual patient consent was required. Institutional review board approval was provided through the Yale University Institutional Review Board.
Variables
From January 2010 to July 2018, there were 24,368 endovascular procedures performed, with follow-up data on 16,125 patients. Follow-up data consisted of a single postoperative visit after the time of intervention. Patients missing data on antiplatelet therapy or those who were noncompliant were excluded from analysis.
Patients were categorized based on discharge antiplatelet regimen. Medication information is reviewed from the electronic medical record by an abstraction team dedicated to the registry. Medications are reviewed on the day of discharge from the day of procedure, and reviewed again during follow-up to determine current anticoagulation and antiplatelet medications. Patients discharged without an aspirin or P2Y12 antagonist were classified as discharged with no antiplatelet therapy. Single antiplatelet therapy consisted of either aspirin 81 mg or 325 mg, or P2Y12 antagonist. DAPT consisted of aspirin plus a P2Y12 antagonist. P2Y12 antagonists included clopidogrel, prasugrel, ticlopidine, and ticagrelor. There were 6863 patients discharged on aspirin alone and 1755 patients discharged on a single P2Y12 antagonist. Comparison between the two groups revealed few significant differences, and thus the two groups were combined into a single monotherapy group to simplify comparison with the other antiplatelet groups.
Prior lower extremity intervention was defined as either a bypass or endovascular intervention. Arterial segments treated included aortoiliac, femoropopliteal, tibial, and pedal arterial vessels. Interventions included angioplasty, stent, atherectomy, and special balloon. Stent included self-expandable, balloon-expandable, stent grafts, and drug-coated stents. Special balloon angioplasty included cutting balloons and drug-coated balloons. There were many patients who received multiple forms of intervention within one procedure. For comparison within this study, this was classified as a single primary procedure. If a patient received a stent, regardless of the other interventions, this was classified as a stent. If a patient received special balloon angioplasty or atherectomy without stent placement, this was classified as such. If a patient received only balloon angioplasty and no other types of intervention, this was classified as angioplasty.
Given that the majority of patients within the database were white, the categorical variable ethnicity was condensed to include non-white and white race. Anticoagulation included vitamin K antagonists, thrombin inhibitors, and factor Xa inhibitors. Systemic complications included perioperative respiratory, cardiac, renal, or other systemic complications. Procedural complications included perioperative thrombosis, embolus, dissection, perforation, hematoma, or infection. The Charlson Comorbidity Index was calculated based on available variables within the database, including age, myocardial infarction (MI), congestive heart failure, peripheral vascular disease, stroke or transient ischemic attack, chronic obstructive pulmonary disease, diabetes mellitus, and moderate to severe chronic kidney disease.
Statistical analysis
Analysis of variance (ANOVA) was used to compare continuous variables in Table 1, while chi-squared and Fisher’s exact test were used when appropriate to compare categorical variables. A Tukey post-hoc test was used to make multiple comparisons between the groups. Binary logistic regression was used to compare discharge antiplatelet therapy regimens in Table 2. DAPT was chosen as the comparison group against no antiplatelet and single antiplatelet therapy. Variables including age, sex, ethnicity and those with a p-value of less than 0.2 were included in the final regression model.
Patient demographics and characteristics.
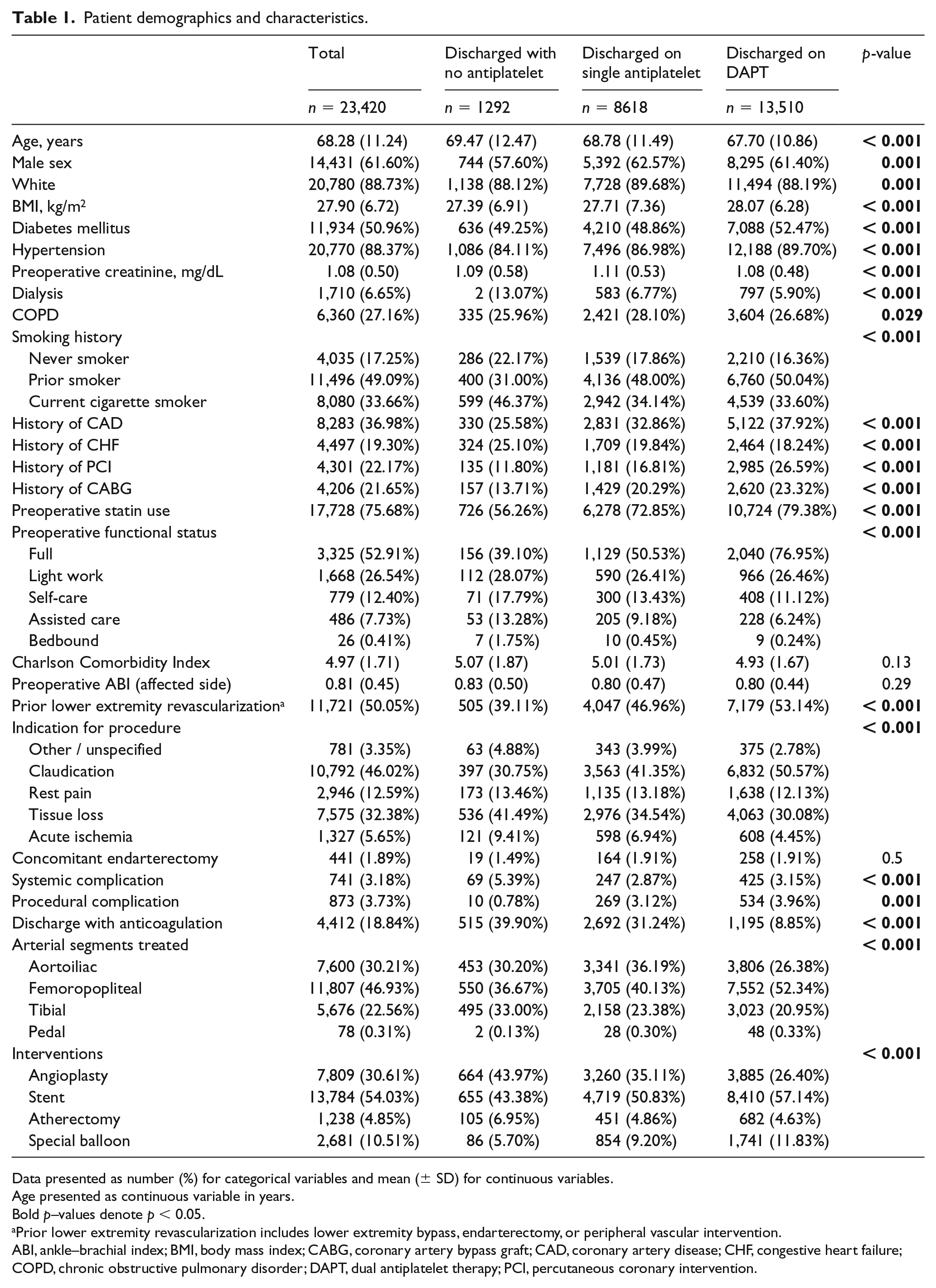
Data presented as number (%) for categorical variables and mean (± SD) for continuous variables.
Age presented as continuous variable in years.
Bold p–values denote p < 0.05.
Prior lower extremity revascularization includes lower extremity bypass, endarterectomy, or peripheral vascular intervention.
ABI, ankle–brachial index; BMI, body mass index; CABG, coronary artery bypass graft; CAD, coronary artery disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disorder; DAPT, dual antiplatelet therapy; PCI, percutaneous coronary intervention.
Logistic regression of odds of being discharged with DAPT compared with no antiplatelet therapy and single antiplatelet therapy.
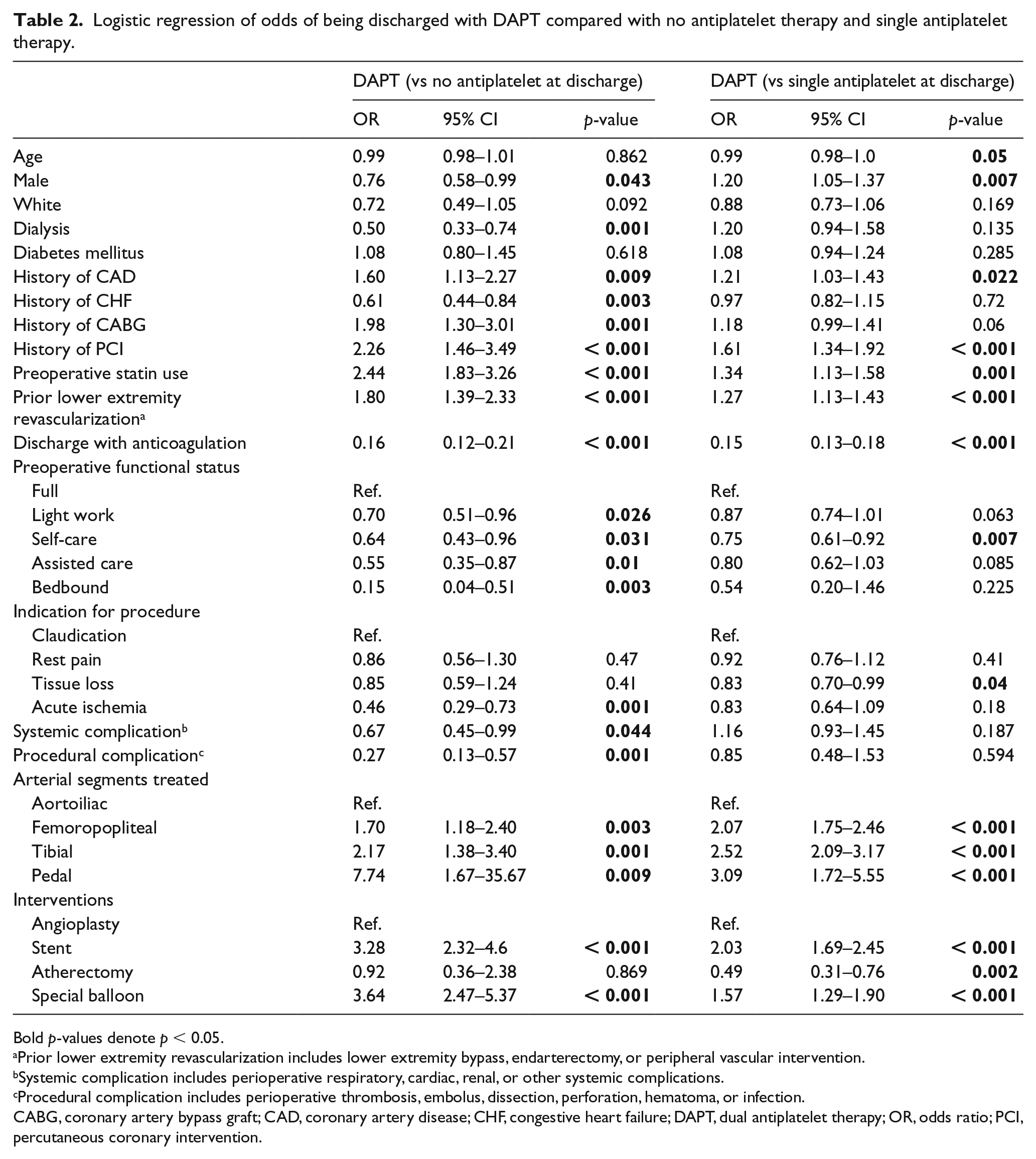
Bold p-values denote p < 0.05.
Prior lower extremity revascularization includes lower extremity bypass, endarterectomy, or peripheral vascular intervention.
Systemic complication includes perioperative respiratory, cardiac, renal, or other systemic complications.
Procedural complication includes perioperative thrombosis, embolus, dissection, perforation, hematoma, or infection.
CABG, coronary artery bypass graft; CAD, coronary artery disease; CHF, congestive heart failure; DAPT, dual antiplatelet therapy; OR, odds ratio; PCI, percutaneous coronary intervention.
Missing data were encountered for patients lost to follow-up and follow-up antiplatelet therapy medication regimen. There were 16,124 follow-up visits recorded of the 26,163 procedures performed. Multiple imputation via chained equations from sequential multivariable models with fully conditional specifications was performed with 25 iterations. All variables involved in previous analytic models including the outcome variables were included. The mi estimate function in Stata 15 was used to derive the imputed proportion of follow-up antiplatelet regimens by time to follow-up and intervention performed.
A sensitivity analysis was performed to assess the effect of discharge with anticoagulation in our model. Multivariable logistic regression was performed using the variables included in the prior model with the exception of discharge anticoagulation.
Statistical analysis was performed using Stata 15 (StataCorp LLC, College Station, TX, USA).
Results
There was a total of 23,420 interventions performed. There were 1,292 patients (5.52%) discharged with no antiplatelet therapy, 8,618 patients (36.80%) discharged with single antiplatelet therapy, and 13,510 patients (57.68%) discharged with DAPT (Table 1). Based on univariate analysis, patients discharged with DAPT were younger, had a higher body mass index (BMI), and were more likely to have diabetes mellitus and better functional status compared with patients discharged on no antiplatelet or single antiplatelet therapy. They also had higher rates of coronary artery disease (CAD), prior percutaneous coronary intervention (PCI), prior coronary artery bypass graft (CABG), and prior lower extremity intervention. Patients discharged with no antiplatelet therapy were more likely to be discharged with anticoagulation, be dialysis dependent, and have a systemic complication compared with single antiplatelet therapy and DAPT.
Logistic regression demonstrated that patients discharged on DAPT were more likely to have CAD, prior PCI or CABG, prior lower extremity revascularization, and be on a statin (Table 2). Patients discharged on DAPT were also less likely to be on anticoagulation. Patients who received femoropopliteal, tibial, or pedal interventions were more likely to be discharged on DAPT compared with aortoiliac treatment. Patients who underwent stenting or special balloon angioplasty were also more likely to be discharged on DAPT compared with those who received only balloon angioplasty.
Sensitivity analysis using logistic regression without discharge anticoagulation demonstrated that a history of CAD, preoperative statin use, and prior lower extremity revascularization remained significantly predictive of discharge with DAPT as compared to single or no antiplatelet therapy (online Supplemental Table 1). Patients who received interventions in the femoropopliteal, tibial, and pedal segments as compared with aortoiliac, and patients who underwent stent and special balloon angioplasty as compared with balloon angioplasty alone also remained significantly predictive of discharge with DAPT as compared with single or no antiplatelet therapy.
There were follow-up data for 9041 (66.9%) of the 13,510 patients discharged on DAPT. Multiple imputation was used to account for the missing follow-up data. Of the patients with follow-up between 0–3 months, 70.47% remained on DAPT (Figure 1). Of the patients who were followed up at 9–12 months, 56.49% remained on DAPT. At 21–24 months, this decreased to 49.63% of patients who remained on DAPT. Analysis of patients newly discharged on DAPT and preoperatively demonstrated a similar rate to patients on DAPT (online Supplemental Figures 1 and 2). At 9–12 months, 56.42% and 66.96% of patients newly discharged on DAPT and on preoperative DAPT, respectively, remained on DAPT. At 21–24 months, the number of patients remaining on DAPT who were newly discharged on DAPT or on preoperative DAPT decreased to 49.44% and 62.88%, respectively.
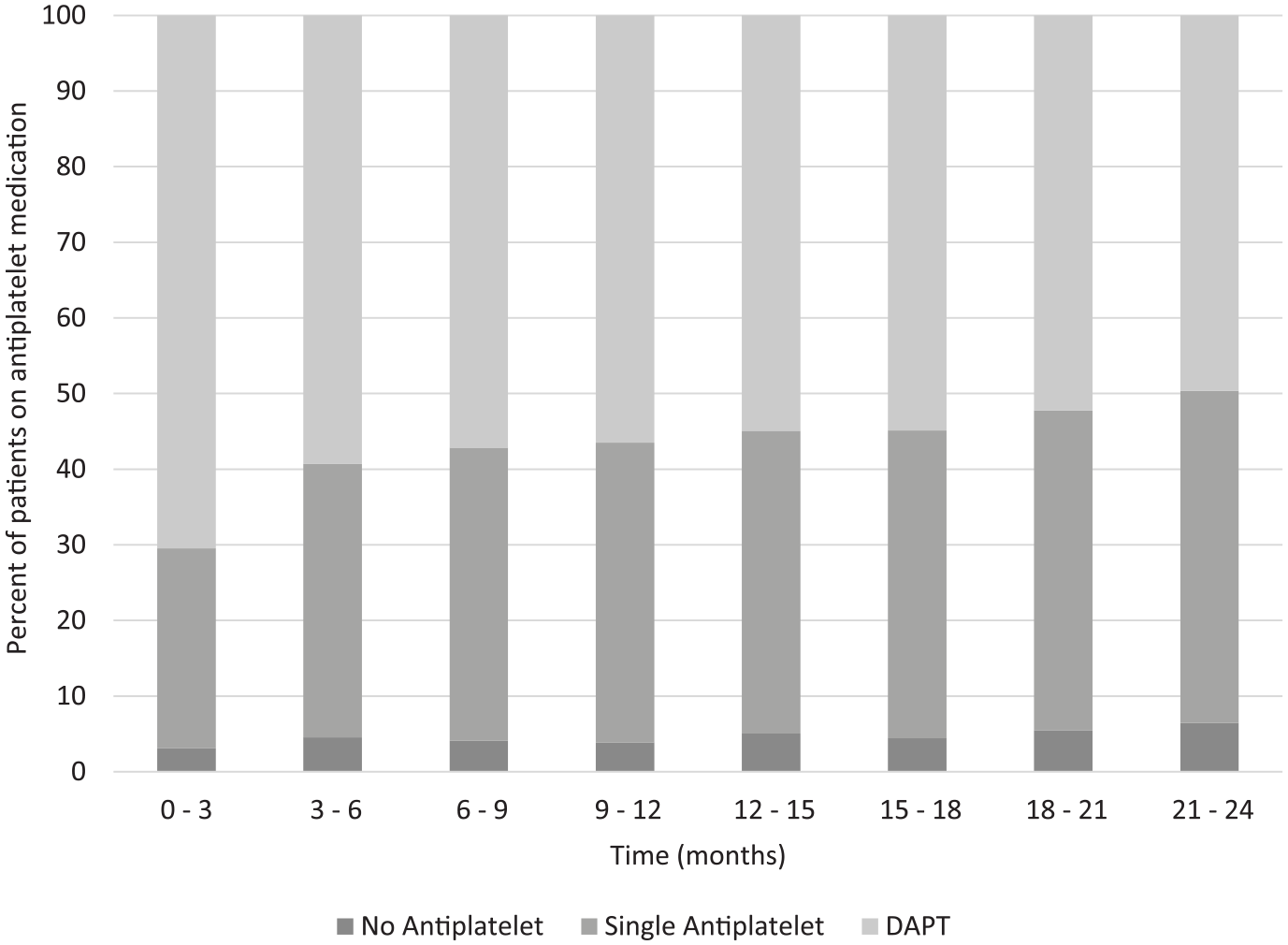
Follow-up antiplatelet regimen of patients discharged on DAPT.
Patients discharged on DAPT were stratified by intervention to investigate whether this had any effect on duration of antiplatelet therapy (Figure 2). At 0–3 months, 59.12% of patients who received angioplasty remained on DAPT, as did 61.26% who received a stent, 54.75% who received a special balloon, and 52.08% who received atherectomy. This steadily decreased over the subsequent 2 years, and at 21–24 months, 27.32% of patients who received angioplasty, 23.39% who received a stent, 23.68% who received a special balloon, and 27.50% of patients who received atherectomy remained on DAPT. Analysis of patients newly discharged on DAPT demonstrated similar ratios of patients who remained on DAPT. The rate of discharge on DAPT following lower extremity intervention remained steady throughout the study period, ranging from 53.96% to 58.88% during the study period.
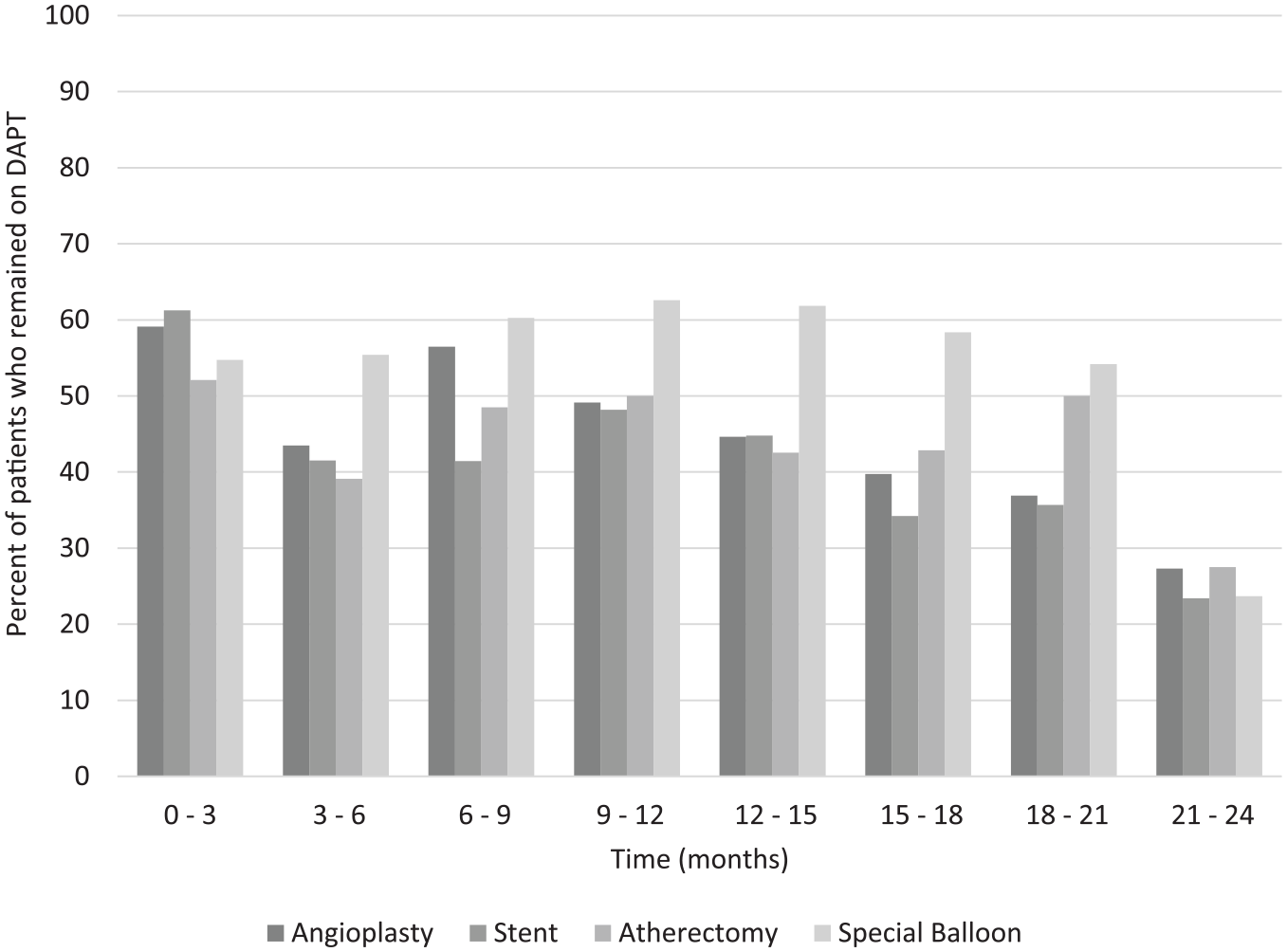
Proportion of patients who remained on DAPT at follow-up by intervention.
Discussion
Unfortunately, current guidelines for DAPT use in the lower extremities remain unclear. The only randomized trial comparing DAPT and single antiplatelet therapy is the MIRROR (Management of peripheral arterial interventions with mono or dual antiplatelet therapy) trial, which randomized 80 patients to aspirin alone or aspirin plus clopidogrel following femoropopliteal balloon angioplasty with provisional stenting. 12 There was a high rate of stenting, with 62.5% in the DAPT group and 47.5% in the aspirin alone group. At 6 months, target lesion revascularization (TLR) was significantly lower in the DAPT group with no difference in bleeding complications or mortality. A subsequent 12-month study demonstrated no difference in TLR or mortality between the groups, although DAPT was stopped at 6 months and patients were continued on aspirin alone. 11
Our short-term findings are similar to that of Sarode et al. who investigated DAPT use after 3 months following infrainguinal endovascular intervention in 368 patients. 14 After 3 months, 43.2% of patients remained on DAPT. Although limited by the short duration of the study, bleeding complications were no different between DAPT use for greater and less than 3 months.
Current American College of Cardiology/American Heart Association (ACC/AHA) guidelines state that DAPT is reasonable to reduce the risk of limb-related events following lower extremity revascularization, although based on class 2B evidence. 15 Within the cardiac literature, the ACC/AHA have established guidelines stating that patients with stable ischemic heart disease with a bare metal stent or drug-coated stent should receive DAPT for at least 6 months, and at least 12 months for those with a MI. 16 Furthermore, patients without a bleeding complication may be continued on an extended regimen of DAPT indefinitely.
Only a narrow margin of the patient majority undergoing lower extremity endovascular intervention (57.69%) were discharged with DAPT. Of those who were followed up at 1 year, 56.49% remained DAPT, with 49.63% at 2 years. Among those newly started on DAPT following endovascular intervention, rates were comparable, with 56.42% at 1 year and 49.44% at 2 years. It can be argued that the long-term rates of DAPT use reflected in this real-world study are too low. As there is no class I evidence, we believe that critical limb ischemia (CLI), defined as ischemic rest pain or tissue loss, can be viewed as the lower extremity counterparts of angina and MI.
DAPT use following an MI has been shown to decrease rates of stroke, MI, and cardiovascular death.8,17 The use of DAPT in patients with PAD compared with aspirin was associated with a lower combined endpoint of cardiovascular death, MI, or stroke in the subgroup analysis of the CHARISMA and PEGASUS-TIMI 54 trials.7,18,19 Beiswenger et al. conducted a systematic review of aspirin monotherapy compared with DAPT, showing reduced rates of major adverse cardiac event, major adverse limb events, and TLR with DAPT. 20 Major bleeding events were no different, although there was a modest increase in moderate bleeding events. Soden et al. used the VSGNE database to show that DAPT compared with aspirin monotherapy following lower extremity revascularization lowered mortality in patients with CLI, but not in patients with claudication. 9 Similar results were published by Thott et al., who demonstrated that diabetic patients with CLI who underwent femoropopliteal stenting and received DAPT had decreased rates of amputation compared with aspirin alone, although there was no difference in bleeding or mortality. 21
There are no specific recommendations regarding duration of DAPT use within the instructions for use (IFU) of the devices. The initial trials of the drug-coated balloons used DAPT for 1–3 months, while the Zilver PTX randomized trial used DAPT for 60 days.22–24 In this study, although patients who received stents and special balloons were more likely to be discharged with DAPT compared with angioplasty, there did not appear to be any major differences in duration of DAPT length. There was even a slightly higher proportion of patients who received angioplasty who remained on DAPT at 2 years compared with stenting. The reasons for this are unclear, although it is possible that many patients were indiscriminately kept on DAPT.
Distal interventions within the femoropopliteal, tibial, and pedal vessels were associated with higher rates of DAPT use compared with aortoiliac interventions. This may be due to the smaller caliber of the vessels, placing them at higher risk of thrombosis. Stent placement and special balloon angioplasty were also associated with increased DAPT use, likely partially driven by the IFU of drug-coated stents and balloons, which recommend DAPT use.22–24
Patients with a history of CAD and prior PCI or CABG were more likely to be discharged with DAPT, following from guidelines for DAPT use in PCI. 16 The association of statin therapy with higher rates of DAPT use is likely also related to the higher rates of CAD. Statin use in combination with aspirin or DAPT has been associated with increased survival in patients with PAD, and is generally recommended in this patient population per United States Preventive Services Task Force (USPSTF) guidelines.25,26
Oral anticoagulant therapy was a predictive factor for decreased DAPT use, likely due to the increased risk of bleeding. Within this study, there was a small minority of patients on triple therapy, although the duration was highly variable. Data from the cardiac literature demonstrated a 4.7% bleeding rate for patients on triple therapy, mostly within the first several months of triple therapy initiation, with 50% of these events leading to mortality. 27 A subsequent meta-analysis demonstrated a 2.2% monthly rate of bleeding in patients on triple therapy. 28
The subgroup analysis of patients with PAD in the Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS) trial found that rivaroxaban 2.5 mg plus aspirin had a significant reduction in the composite endpoint of cardiovascular death, MI, or stroke, as well as reduced rates of amputation compared with rivaroxaban 5 mg or aspirin alone.29,30 The rate of major bleeding was relatively low at 3%, although significantly higher than aspirin alone. It will be interesting to see how these results, in addition to the ongoing Vascular Outcomes study of ASA along with Rivaroxaban in Endovascular or Surgical Limb Revascularization for Peripheral Artery Disease (VOYAGER PAD) trial, will influence prescribing patterns of low dose rivaroxaban as well as DAPT. 31
Patients with decreased functional status trended toward less DAPT use. It is possible that this may be due to an increased risk of falls in those with impaired ambulation, although advanced age, an established risk factor, was not associated with decreased DAPT use in this cohort. 32
Although patients with allergies to antiplatelet medications were excluded from this study, it is possible that a number of patients who were prescribed clopidogrel were resistant, with estimates that 4–30% of patients are resistant.33,34
Limitations
An important limitation of the study is the availability of follow-up data within the registry. Only a single follow-up visit at a variable time was included in the registry. Furthermore, although bleeding complications were recorded during the initial visit, it was not recorded in subsequent follow-up data. Additional complications including cardiac events were also not included. Thus, it is likely that a bleeding event is the reason for a proportion of patients taken off DAPT. Long-term mortality rates of patients on DAPT following endovascular intervention within this database have been previously published by Soden et al., although cause of death was not recorded. 9 Additional limitations include the categorization of intervention variables. Drug-coated balloons and stents were classified within the database as special balloons and stents, respectively. It would have been useful to see the trends in drug-coated device use, as it also likely had an effect on DAPT administration. Although this study has a relatively large sample size, caution must be exercised when extrapolating to the broader population, as the majority of the patients in this database were older white males. Further studies including randomized trials are needed to determine the optimal length of DAPT therapy after endovascular intervention, and to determine which patients are at an elevated risk of bleeding complications.
Conclusion
Although patients undergoing percutaneous coronary interventions are recommended to have DAPT, only a narrow majority of patients who received lower extremity endovascular interventions were discharged with DAPT in this study. Comorbid conditions and prior coronary and infrainguinal interventions drove higher use of DAPT. Of those discharged with DAPT at 1 year, 56% remained on it, with 49% at 2 years. This suggests that most patients discharged with DAPT after undergoing endovascular intervention remain on DAPT long-term. As the number of lower extremity endovascular interventions grow exponentially every year, further studies are crucial to identify the optimal duration of DAPT.
Supplemental Material
10.1177_1358863X19880602_Supplemental_figures_and_tables – Supplemental material for Practice patterns of dual antiplatelet therapy after lower extremity endovascular interventions
Supplemental material, 10.1177_1358863X19880602_Supplemental_figures_and_tables for Practice patterns of dual antiplatelet therapy after lower extremity endovascular interventions by Tanner I Kim, Julia F Chen and Kristine C Orion in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.