
Abstract
Evidence suggests that statin therapy in patients with peripheral artery disease (PAD) is beneficial yet use remains suboptimal. We examined trends in statin use, intensity, and discontinuation among adults aged ⩾ 40 years with incident severe PAD and a subset with critical limb ischemia (CLI) between 2002 and 2015 within an integrated healthcare delivery system. Discontinuation of statin therapy was defined as the first 90-day gap in treatment within 1 year following PAD diagnosis. We identified 11,059 patients with incident severe PAD: 31.1% (n = 3442) with CLI and 68.9% (n = 7617) without CLI. Mean (SD) age was 68.6 (11.3) years, 60.5% were male, 54.2% white, 23.2% Hispanic, and 16.2% black. Statin use in the year before diagnosis increased from 50.4% in 2002 to 66.0% in 2015 (CLI: 43.7% to 68.0%; without CLI: 53.1% to 64.2%, respectively). The proportion of patients on high-intensity statins increased from 7.3% in 2002 to 41.9% in 2015 (CLI: 7.2% to 39.4%; without CLI: 7.4% to 44.2%, respectively). Of the 40.5% (n = 4481) who were not on a statin in the year before diagnosis, 13.5% (n = 607) newly initiated therapy within 1 month (CLI: 10.1% (n = 150); without CLI: 15.3% (n = 457)). Following diagnosis, 12.5% (n = 660) discontinued statin therapy within 1 year (CLI: 15.5% (n = 202); without CLI: 11.5% (n = 458)). Although use of statins increased from 2002 to 2015, a substantial proportion of the overall PAD and CLI subpopulation remained untreated with statins, representing a significant treatment gap in a population at high risk for cardiovascular events and adverse limb outcomes.
Keywords
Introduction
Lower extremity peripheral artery disease (PAD) is a common vascular morbidity affecting an estimated 200 million adults worldwide and 8–10 million Americans aged 40 years and older.1–3 The prevalence of PAD rises with age and affects 12–20% of adults aged 65 and older.1,2,4 PAD can progress to critical limb ischemia (CLI), a severe clinical manifestation of PAD characterized by ischemic rest pain, tissue gangrene or ulcers of the extremities.5–7 Individuals with PAD are at significantly increased risk for myocardial infarction, stroke, and death, 2 and those with CLI have both increased risk for cardiovascular events and major adverse limb events (including lower limb amputation or surgical bypass/revascularization).8,9 Individuals with CLI also have impaired function, poor quality of life and high healthcare costs.1,2,10 The burden from PAD and CLI is predicted to increase given the aging of the population in the United States as well as the increase in diabetes mellitus and the lasting effect of smoking.1,11
Despite the significant morbidity, quality of life impairment, and mortality seen in patients with PAD, including those with CLI, several studies have shown that those with PAD have poorer risk factor management relative to other atherosclerotic diseases.12–16 This is likely multifactorial and may include a lack of awareness by providers and patients and/or a lesser perceived risk.13,15,17 Furthermore, although the benefits of statin treatment in PAD have been demonstrated and current guidelines recommend statin therapy for all individuals with PAD,18–21 the use of statins has been found to be underutilized in those with PAD.12,22–24
We sought to examine temporal trends in statin use and statin intensity, as well as rates of statin discontinuation between 2002 and 2015 among a high-risk cohort of adults aged 40 and older with incident severe PAD, including CLI, within an integrated healthcare delivery system.
Methods
This retrospective study was conducted among members of Kaiser Permanente Southern California (KPSC), an integrated healthcare delivery system. KPSC currently provides healthcare for more than 4.5 million members in the Southern California region. The KPSC population is diverse and representative of the region except for slightly lower representation at the extremes of income and education. 25 Data on medical care are captured through an electronic health record (EHR). The majority of members (> 95% in recent years) have a drug benefit and fill their prescriptions at KPSC pharmacies.
Patients aged ⩾ 40 years with incident severe PAD, including a subset with CLI, diagnosed between October 1, 2002 and September 30, 2015 were identified by outpatient and inpatient International Classification of Diseases, Ninth Revision (ICD-9) diagnosis and procedure codes and Current Procedural Terminology (CPT) codes and assigned an index date based on the algorithm listed in online Supplemental Table 1. CLI was defined as the presence of one inpatient or one outpatient diagnosis code for atherosclerosis of the native arteries of the extremities with rest pain, ulceration, or gangrene. Severe PAD was defined as the presence of one inpatient or one outpatient diagnosis code for atherosclerosis of the native arteries of the extremities with or without intermittent claudication, atherosclerosis of a bypass graft of the extremities, chronic total occlusion of the artery of the extremities, or peripheral vascular disease plus a procedure code for a peripheral revascularization or an amputation within 90 days of the diagnosis code. To be included in the cohort, patients had to have 12 months of continuous membership and a pharmacy benefit (allowing gaps in coverage of up to 45 days) prior to the index date and 1 month after the index date to capture a change in therapy after a PAD/CLI diagnosis (Figure 1).
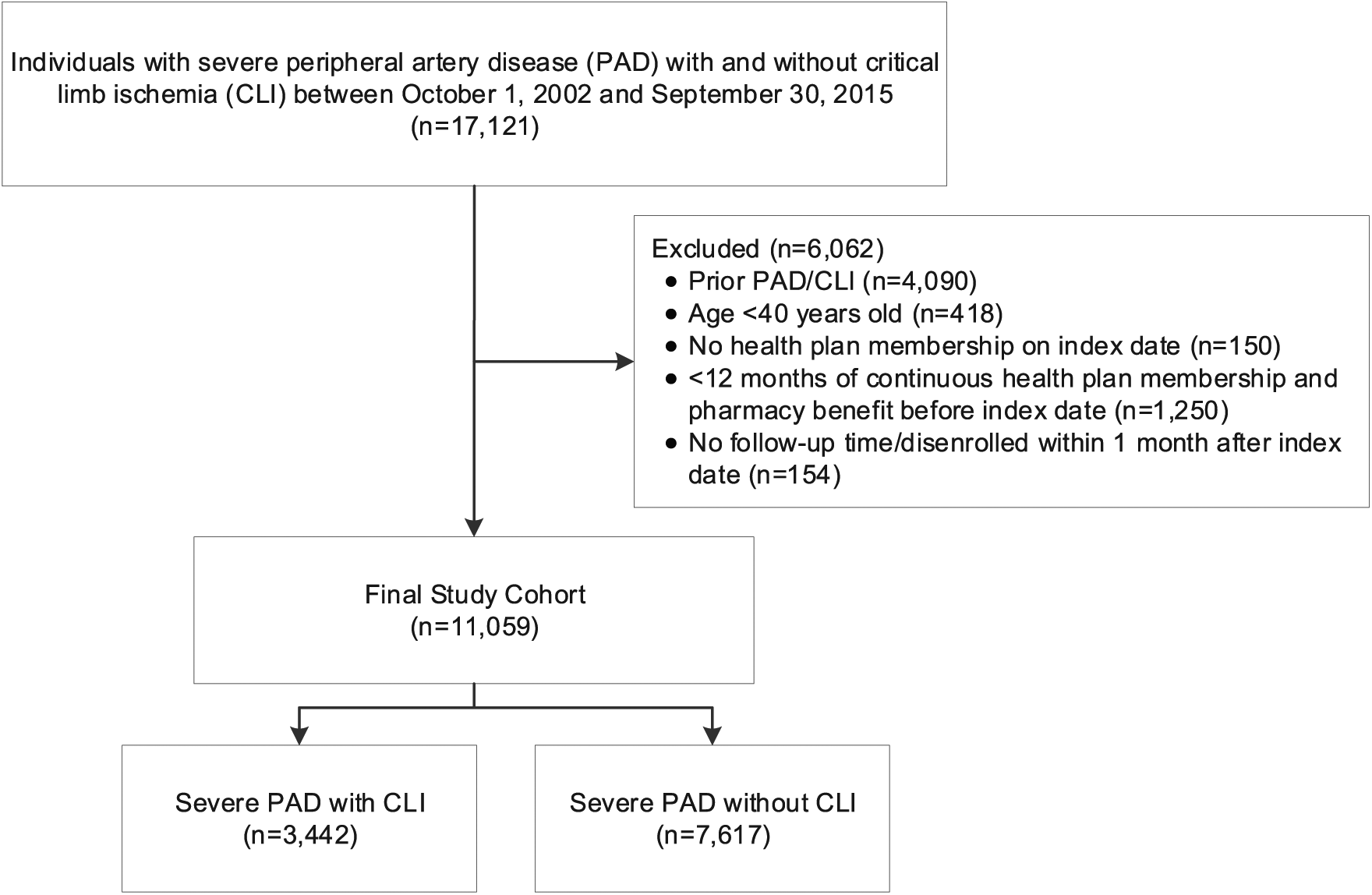
Cohort assembly of patients with incident severe PAD with and without CLI between October 1, 2002 and September 30, 2015.
Baseline information was extracted from the EHR and administrative sources in the 12 months before cohort entry, including: patient demographics (age, sex, and race/ethnicity), body mass index, smoking status (never, former, current), healthcare utilization (outpatient visits, hospitalizations, emergency department (ED) visits), laboratory results (high-density lipoprotein-cholesterol (HDL-C), low-density lipoprotein-cholesterol (LDL-C), total cholesterol, triglycerides, and hemoglobin A1c), comorbidities (hypertension, diabetes mellitus, history of atrial fibrillation, ischemic stroke, coronary heart disease, acute myocardial infarction, coronary revascularization, heart failure, chronic obstructive pulmonary disease, and chronic kidney disease), use of cardiovascular medications (antihypertensives, anticoagulants, antiarrhythmics, antiplatelets, insulin, and oral hypoglycemic agents). Comorbidities including the Charlson Comorbidity Index 26 were identified using ICD-9 diagnosis codes from inpatient, ED, and outpatient encounters. Statin use was extracted for the year before and the year after the index date. Statin intensity was defined as low-, moderate-, or high-intensity based on cholesterol treatment guidelines. 27 LDL-C results were extracted from the 12 months before the index date through 1 month after and including the index date. The LDL-C result most proximal to the index date was used in analyses. Data on all-cause mortality was obtained by using KPSC administrative data sources, state death certificates, and Social Security Administration files. To assess mortality risk, patients were followed from the index date through September 30, 2016.
The study protocol was reviewed and approved by the KPSC institutional review board, and a waiver for written informed consent was obtained due to the retrospective nature of the study. Compliance with Health Insurance Portability and Accountability Act regulations was ensured.
Statistical analysis
Baseline patient characteristics were assessed for the overall population and separately for those with and without CLI and described as means (SD) or medians (IQR) for continuous variables and proportions for categorical variables. We compared the baseline characteristics using t-tests for continuous variables and the χ2 test for categorical variables. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Statin use and intensity were examined at baseline (the 12 months before the index date) in the overall population and by racial/ethnic groups. The percentage of overall statin users and the percentage of those prescribed a low-, moderate- or high-intensity statin were calculated for each calendar year (defined as October 1 to September 30). The secular trend of statin use was tested using Poisson regression. Statin use and intensity in the 1 month and 12 months following and including the index date were examined to determine if a PAD diagnosis would result in the initiation of a statin or a statin dose escalation. Statin use at diagnosis was defined as having a statin dispensed in the 12 months before and within 1 month after the diagnosis.
Adherence to statin medication was calculated as the proportion of days covered (PDC) during the 12 months before the index date divided by the number of days covered (based on prescription dispense dates and days of supply). Adherence was defined as a PDC ⩾ 80%. 28 The percentage of patients who discontinued statin therapy was examined during the 1-year period following the index date. Discontinuation was calculated among patients with at least 1 year of continuous health plan enrollment following the index date and who were on a statin at least 1 day within the month following and including the index date. Discontinuation was defined as the first 90-day gap in statin therapy after the estimated end date of statin prescription. We examined statin use separately in those with and without CLI by baseline levels of LDL-C and the mean percentage change in LDL-C from baseline to 1 year after the index date. This analysis was restricted to patients who had an LDL-C value at baseline and 1 year after the index date (n = 5648). The LDL-C percentage change was examined for patients who downtitrated, uptitrated, discontinued or initiated statin therapy (i.e. no statin therapy within 1 year prior to the index date), or did not change statin therapy in the 1 year after the index date. To provide the most proximal LDL-C result for patients who downtitrated, uptitrated, discontinued or initiated statin therapy, we used the first LDL-C result between 90 days after the change in statin therapy and up to 1 year after the index date. The first LDL-C result in this period was used for patients with multiple LDL-C results. For patients who did not switch therapy, we used the last LDL-C result between 90 days and 1 year after the index date. Temporal trends in statin use and intensity were also examined in the subgroup of patients with a history of acute myocardial infarction and ischemic stroke using all available look-back in the EHR to identify both conditions.
We used Cox proportional hazards regression to calculate multivariable adjusted hazard ratios (HRs) of all-cause mortality by statin use adjusting for age, sex, race/ethnicity, baseline LDL-C, and Charlson comorbidity index score. Data were censored on September 30, 2016 or when a patient died or left the health plan.
Results
Study population
We identified a cohort of 11,059 patients with severe PAD, including 31.1% with CLI (n = 3442) and 68.9% without CLI (n = 7617) (Table 1). In the overall cohort, mean age (SD) was 68.6 (11.3) years, 60.5% were male, 54.2% were white, 23.2% Hispanic, 16.2% black, 4.1% Asian, and 2.3% were of unknown/other/multiple race/ethnicity. Over 80% of the cohort had at least one comorbidity: 75.7% had hypertension, 51.9% had diabetes, 29.8% had coronary heart disease, 11.3% had heart failure, 11.9% had chronic obstructive pulmonary disease, and 22.9% had chronic kidney disease.
Baseline characteristics of patients in the overall study population and in patients with severe PAD with incident CLI and without CLI from 2002 to 2015.
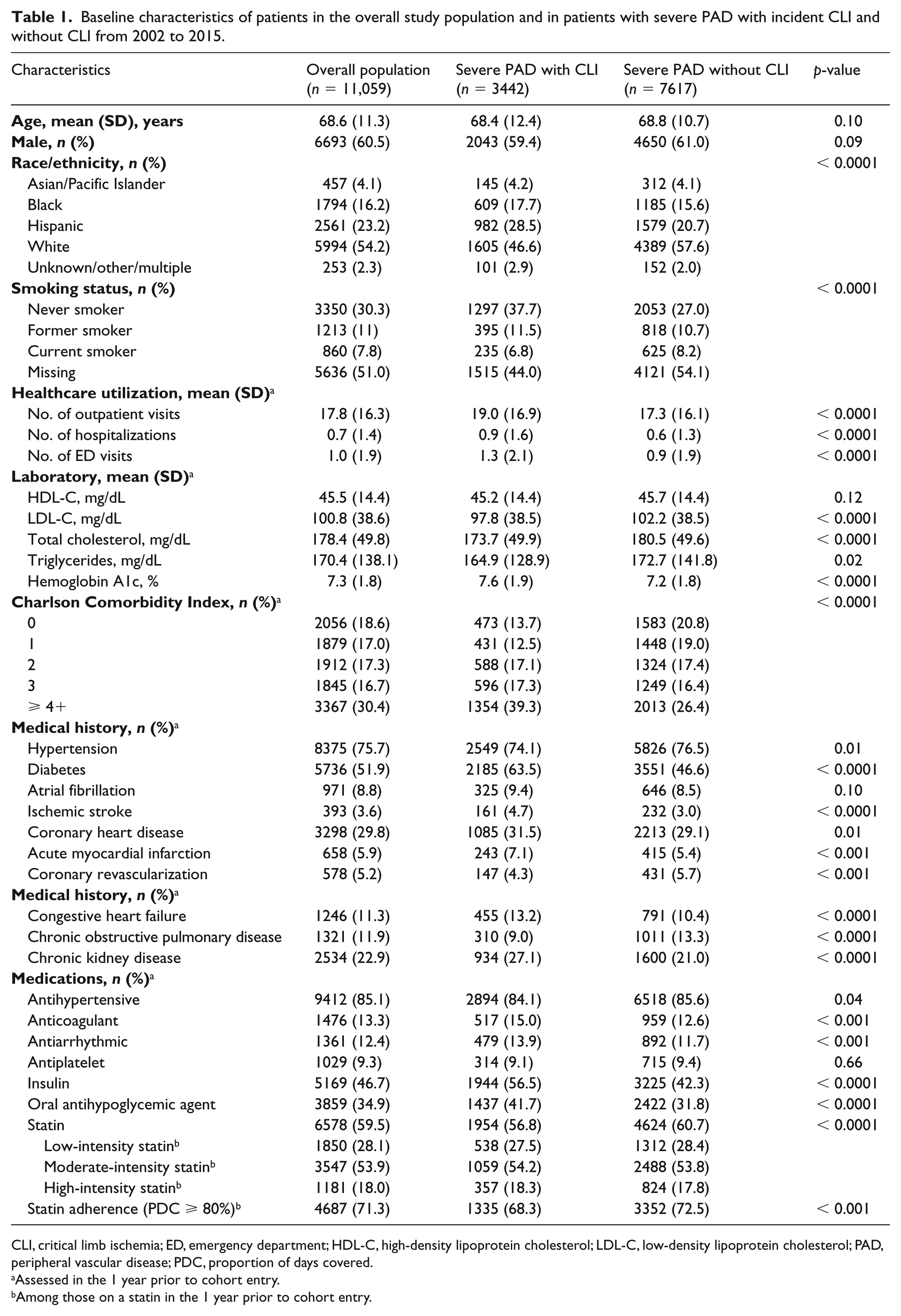
CLI, critical limb ischemia; ED, emergency department; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; PAD, peripheral vascular disease; PDC, proportion of days covered.
Assessed in the 1 year prior to cohort entry.
Among those on a statin in the 1 year prior to cohort entry.
Patients with CLI were more likely to be Hispanic or black and have higher healthcare utilization in the year before their CLI diagnosis than patients with severe PAD without CLI. Patients with CLI were also more likely to have a higher number of comorbidities compared with patients without CLI. Patients with CLI were more likely to have diabetes, ischemic stroke, coronary heart disease, acute myocardial infarction, congestive heart failure and chronic kidney disease but less likely to have hypertension, coronary revascularization, and chronic obstructive pulmonary disease. Consistent with a higher prevalence of diabetes, patients with CLI were more likely to be prescribed insulin and/or oral antihypoglycemic agents compared with patients without CLI. The use of anticoagulants was slightly higher in patients with CLI compared with those without CLI (15.0% vs 12.6%), while the use of statins was slightly lower (56.8% vs 60.7%). Adherence (PDC ⩾ 80%) to statins in the 12 months before the index date was slightly higher in patients without CLI compared with those with CLI (72.5% vs 68.3%).
Trends in statin use
Overall, 59.5% (n = 6578) of patients were prescribed a statin in the year before their diagnosis (56.8% in those with CLI and 60.7% in those without CLI). Among these 6578 patients, 28.1%, 53.9%, and 18.0% were prescribed a low-, moderate-, and high-intensity statin, respectively (Table 1). Statin use increased over the study period (p < 0.0001) (Figure 2). In 2002, 50.4% of patients were using a statin and this increased to 66.0% in 2015. The proportion on a high-intensity statin increased from 7.3% in 2002 to 41.9% in 2015. Conversely, the proportion using a low-intensity statin decreased from 46.7% to 10.0% between 2002 and 2015, while the use of a moderate-intensity statin increased slightly from 2002 to 2009 and then decreased to the level of use in 2002 from 2011 to 2015 as the use of high-intensity statins increased. Similar trends were found for patients with CLI (online Supplemental Figure 1A) and those with severe PAD without CLI (online Supplemental Figure 1B).
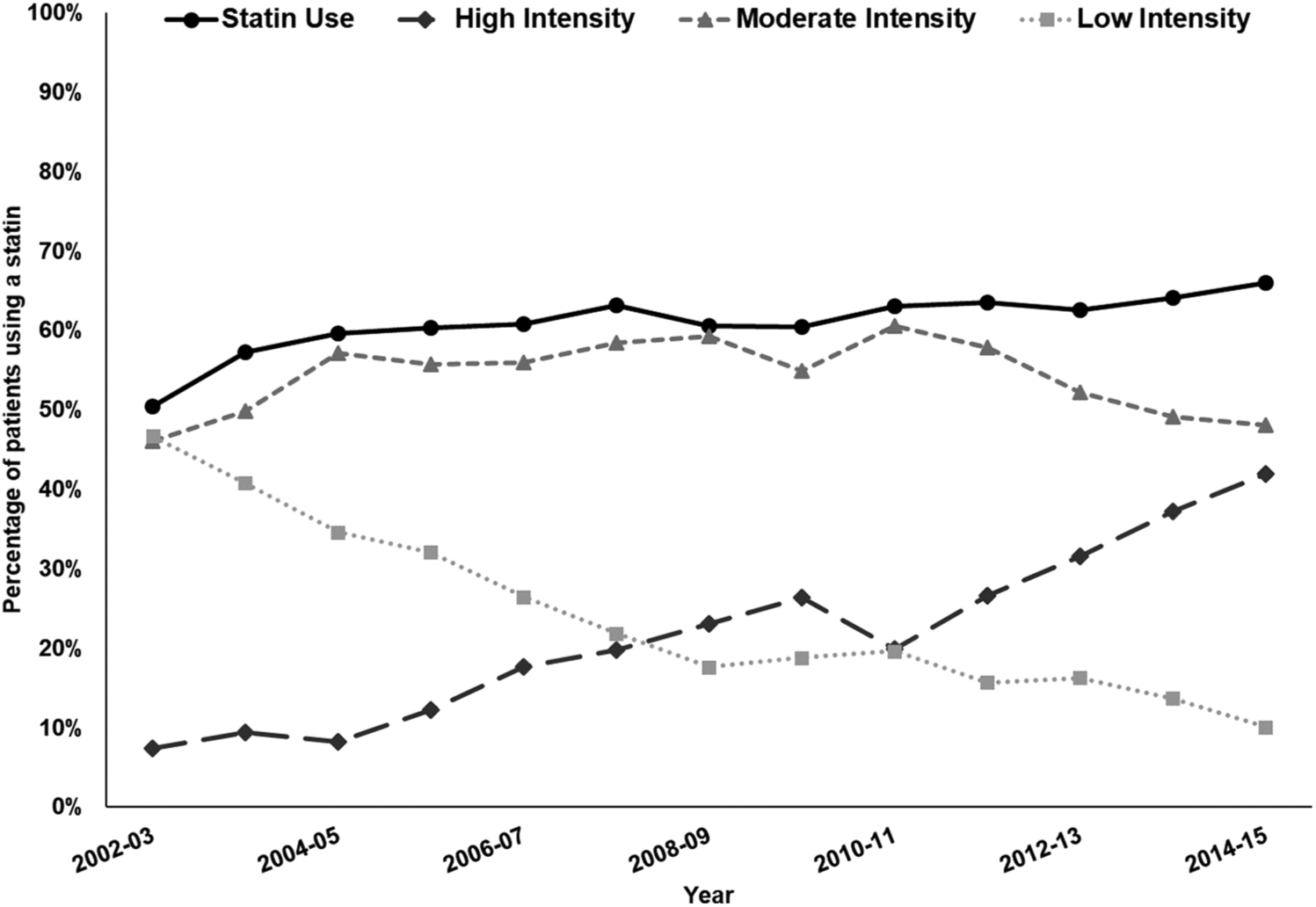
Temporal trends in statin use in the overall population (n = 11,059) and use of high-, moderate-, and low-intensity statins among those using statins in the 1 year prior to diagnosis of severe PAD.
Patients with a history of myocardial infarction or ischemic stroke were more likely to be prescribed a statin in the 12 months before their diagnosis and more likely to be prescribed a high-intensity statin (Figure 3). Among patients with a prior myocardial infarction, 76.9% were prescribed a statin in the year before their diagnosis compared to 55.7% of patients without a prior myocardial infarction. Similarly, 69.6% of patients with a history of ischemic stroke were prescribed a statin in the year before their diagnosis compared to 58.5% of patients without a history of ischemic stroke.
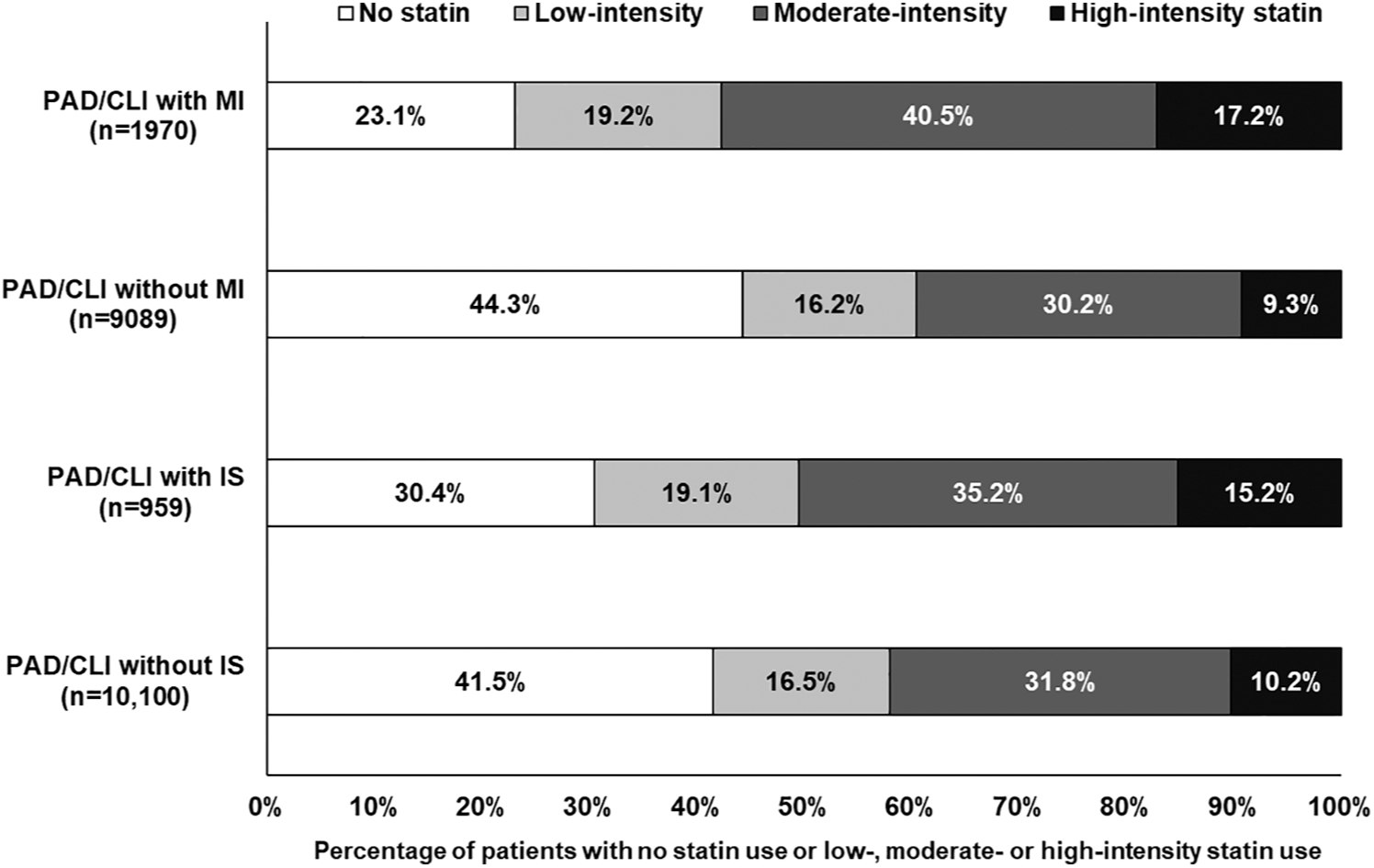
No statin use and use of high-, moderate-, and low-intensity statins in the 1 year prior to diagnosis of severe PAD stratified by presence of MI or IS.
Statin use was similar among black (56.5% for those with CLI and 58.7% for those with PAD without CLI) and white (55.8% for those with CLI and 59.9% for those with PAD without CLI) individuals (online Supplemental Figure 3). Statin use was highest among Asian/Pacific Islanders (64.8% for those with CLI and 67.3% for those with PAD without CLI) followed by Hispanic individuals (58.8% among those with CLI and 64.6% for those with PAD without CLI). The use of high-intensity statins was also highest among Asian/Pacific Islanders with CLI (15.2%) followed by black (13.1%), Hispanic (10.5%), and white (9.2%) individuals. Among patients with PAD without CLI, black individuals had slightly higher use of high-intensity statins (13.3%) followed by Hispanics (12.6%), Asian/Pacific Islanders (11.2%), and white individuals (9.7%).
Statin initiation, dose intensification, and discontinuation of statins
Among the 40.5% (n = 4481) of patients who did not have a statin fill in the year before their diagnosis, 35.7% (n = 1601) initiated therapy within 1 year after their diagnosis (Table 2) and 13.5% (n = 607) newly initiated therapy within 1 month (10.1% of those with CLI and 15.3% of those without CLI newly initiated therapy within 1 month) (data not shown). Among the 16.7% (n = 1850) who were taking a low-intensity statin in the year before their diagnosis, 10.5% (n = 194) intensified therapy to a high- or moderate-intensity statin. Among the 32.1% (n = 3547) on a moderate-intensity statin in the year before their diagnosis, 3.3% (n = 118) intensified therapy to a high-intensity statin (Table 2).
Concordance of statin therapy in the year before and the year after diagnosis of severe PAD.
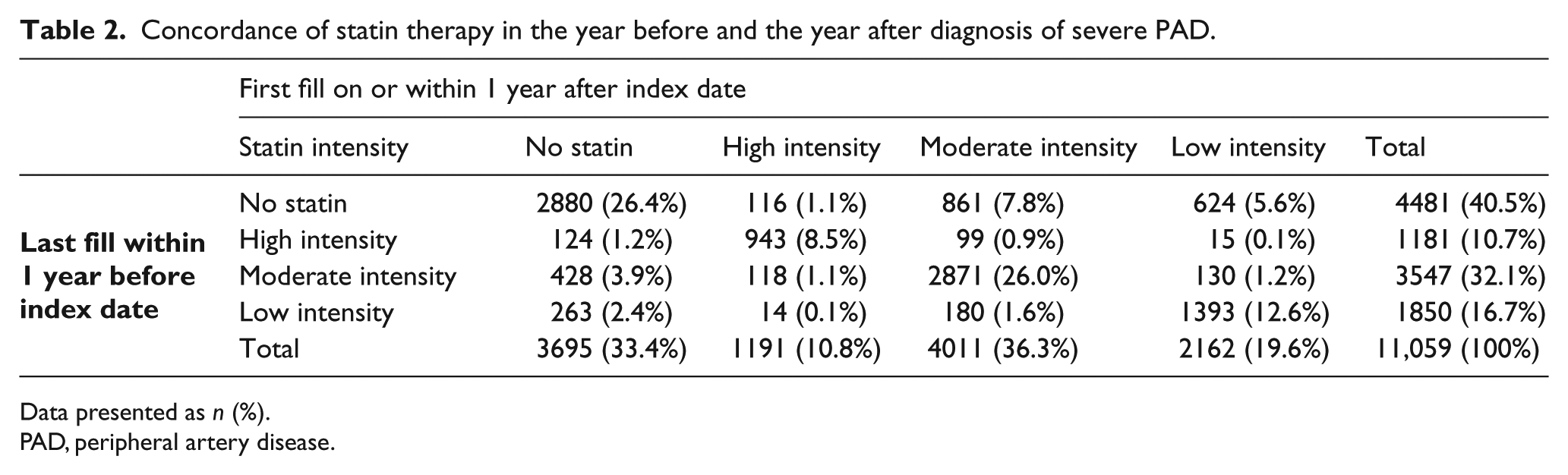
Data presented as n (%).
PAD, peripheral artery disease.
Following the severe PAD diagnosis, 12.5% (n = 660) of patients with 1 year of continuous enrollment (n = 5285) discontinued statin therapy within the year. The proportion who discontinued statin therapy within 1 year was higher in those with CLI compared to those without CLI: 15.5% vs 11.5%, respectively (data not shown).
Lipid profiles by statin use
The percentage of patients who were not on a statin in the 12 months prior to or 1 month following diagnosis increased with increasing LDL-C levels (Figure 4). Among the 8882 patients with LDL-C results in the year before or 1 month following their diagnosis, 44.4% (n = 3948) had LDL-C ⩾ 100 mg/dL (CLI: 40.0% had LDL-C ⩾ 100 mg/dL (online Supplemental Figure 2A); without CLI: 46.4% (online Supplemental Figure 2B)). Among the 5648 patients with LDL-C results at baseline and in the 1 year following the index date, patients who initiated statin therapy following their diagnosis had the largest mean percentage reduction in LDL-C (13.6%) followed by patients who uptitrated therapy (6.3%) (online Supplemental Figure 4).
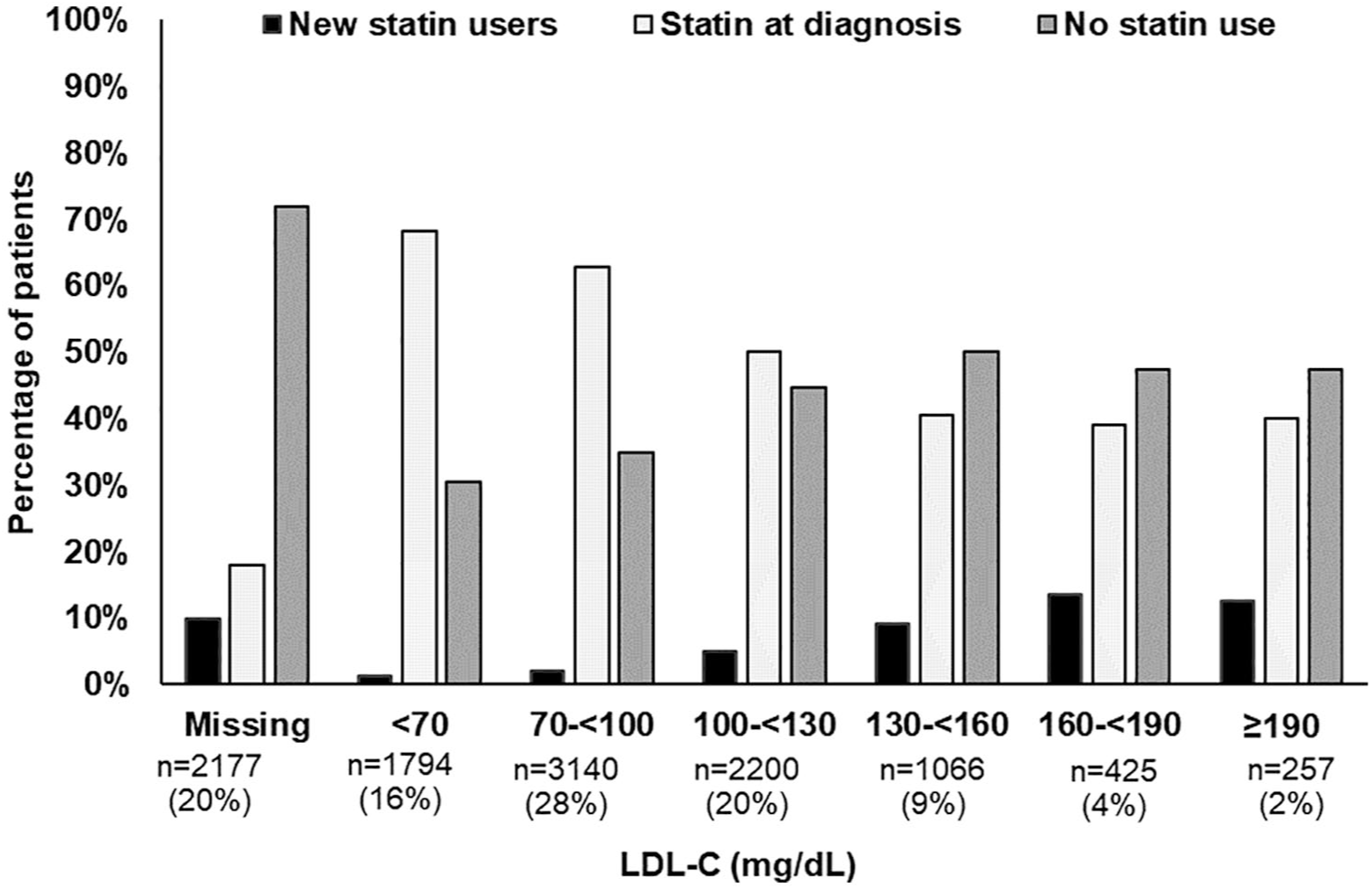
LDL-C levela by statin use in the overall population of patients with severe PAD.
All-cause mortality
In the year following the severe PAD diagnosis, 12.2% (n = 1346) of patients died (20.9% with CLI and 8.2% without CLI) and 3.5% (n = 385) disenrolled from the health plan (5.1% with CLI and 2.8% without CLI) (data not shown). Over a median 4.2 years of follow-up, 6410 (58.0%) of patients died. Patients using statins at baseline experienced lower mortality compared with their counterparts who were not using statins in the 1 year prior to their PAD diagnosis. The multivariable adjusted hazard ratios (95% CIs) for mortality associated with statin use were 0.81 (0.73 to 0.89) for patients with CLI and 0.80 (0.74 to 0.86) for patients with PAD without CLI (online Supplemental Table 3).
Discussion
In this insured population of high-risk patients with incident severe PAD, including a subset with CLI, the use of statins increased between 2002 and 2015; however, 40.5% were not using statin therapy at the time of their diagnosis and only 35.7% of these patients initiated a statin in the 1 year after diagnosis. Among patients already on a statin, there was little intensification following the severe PAD/CLI diagnosis. Over 20% of patients in our population did not have a baseline LDL-C result in their EHR, which could have contributed to statin treatment decisions by their healthcare provider. We observed an increase in the use of high-intensity statins over the study period while the use of low-intensity statins decreased. Temporal trends were consistent among patients diagnosed with CLI and those diagnosed with severe PAD without CLI. Further, among 5285 patients with 1 year of continuous membership following their diagnosis, 12.5% (n = 660) discontinued statin therapy. Finally, mortality was high, with 20.9% of the population with CLI and 8.2% of those with severe PAD without CLI dying within 1 year following their diagnosis and 58% dying over a median 4.2 years of follow-up. The risk of death was approximately 20% less among patients using statins in the year prior to their PAD compared with patients not taking a statin.
Despite the 2013 American College of Cardiology/American Heart Association (ACC/AHA) Cholesterol Treatment Guideline recommending statin therapy for all individuals with PAD, 20 recent studies have shown that the use of statins in these individuals is suboptimal,12,22,23,29 although use of statins has been increasing over time.12,16,30 Data from the National Ambulatory Medical Care and National Hospital Ambulatory Medical Care Surveys found that only 35% of patients with PAD were on a statin and use did not change significantly between 2006 and 2013 (30.5% vs 38.8%, respectively; p = 0.057). 29 The lower use of statins compared with our study likely reflects the lower risk population included in the surveys; only 32% had diabetes, 8% had chronic kidney disease, 65% had hypertension, and 24% had coronary artery diseases compared with 52%, 23%, 76%, and 30%, respectively, in our study. In a small study of 909 patients with PAD who underwent peripheral angiography and/or endovascular intervention between 2006 and 2013, 68.9% were prescribed a statin; however, only 13.6% were treated with high-intensity statins and the proportion did not differ by year. 22 A larger study of 155,657 Veterans Affairs (VA) patients with incident PAD found that 70–75% were on a statin at the time of the PAD diagnosis and this number remained stable between 2003 and 2014. 23 As in our study, use of high-intensity statins increased over the study period. The increase in statin use and a shift from low- to high-intensity statins in our population may be due to several factors including initiatives implemented within the healthcare system, guidelines from professional medical societies for the management of blood cholesterol and management of patients with PAD, 31 and a shift to generic statins after the patent for atorvastatin expired in 2011 potentially resulting in more widespread use of less costly generic formulations. 32
We observed that use of statins in patients with severe PAD was higher in those with concomitant cardiovascular disease (PAD and myocardial infarction: 77%; PAD and ischemic stroke: 70%). Similar to our findings, in the 155,657 VA patients with incident PAD, statin use and use of high-intensity statins was higher in patients with PAD and a concomitant diagnosis of coronary artery disease (82%), carotid artery stenosis (65%), or both (84%) versus patients with only PAD (68%). 23 The greater use of statins in patients with PAD and cardiovascular disease may indicate barriers to adoption of use of statins in patients with PAD alone. This suggests opportunities to improve provider knowledge regarding the benefits of statins in patients with PAD not just in reducing cardiovascular events but also in reducing major adverse limb events.23,33 Previous studies have shown that non-Hispanic black individuals are less likely than non-Hispanic white individuals to be taking statins when indicated.31,34–36 However, these previous studies were not specific to patients with PAD. We found that among a patient population with PAD, statin use was similar among non-Hispanic black and white individuals. We also found that the use of high-intensity statins was slightly higher in non-Hispanic black compared with non-Hispanic white individuals. In an analysis of Medicare beneficiaries, black patients were more likely than white patients to initiate high-intensity statins following a myocardial infarction. 32 Additional studies that examine statin use by race and explore reasons for disparities in statin use in patients with PAD are warranted. Our study findings also documented that statin intensification following a PAD diagnosis was infrequent, highlighting another important opportunity to optimizing statin therapy for patients with PAD. Among the 6331 patients who were not taking a statin at the time of their PAD diagnosis or were on a low-intensity statin, only 26.8% initiated a statin therapy in the year following their diagnosis. Other studies have reported similar results among patients following a myocardial infarction.37,38 Among 4340 patients with acute myocardial infarction in the TRIUMPH registry, 87% of statin-naïve patients initiated a statin during their hospitalization stay while only 26% had their statin therapy intensified. 37 In a cohort of 158,795 Medicare beneficiaries discharged for myocardial infarction, 53.7% discontinued statin therapy and then reinitiated therapy within 365 days, and 66.0% these individuals reinitiated the same statin and intensity. 38 A recent study from the international, prospective Patient-Centered Outcomes Related to Treatment Practices in Peripheral Arterial Disease: Investigating Trajectories (PORTRAIT) registry examined patterns of statin therapy before and after an evaluation for new or worsening claudication symptoms. Among 1144 patients assessed at 16 PAD specialty clinics between June 2011 and December 2015, 70.8% were taking a statin. Among the 29.2% who were not taking a statin, 30.8% initiated statin therapy following the evaluation and 31.0% who were not receiving a moderate or high-intensity statin underwent statin intensification. 39 There are likely many reasons for the low rates of statin intensification, including patient contraindications to statin therapy 40 or provider disagreement or lack of familiarity with treatment guidelines.12,41,42 Future studies should identify effective strategies to overcome barriers to statin intensification.
Limitations and strengths
This study has several limitations. We relied on diagnosis and procedure codes from the EHR to identify patients with severe PAD and CLI rather than objective measurements of ankle or toe pressures. We were not able to capture clinical information regarding ankle–brachial index testing or clinical presentations or symptoms of PAD as this information is in free-text clinical notes which would require chart review or natural language processing to extract the information. However, we used diagnosis and procedure codes reflecting severe PAD and CLI. The study was limited to a single healthcare system with an integrated model in southern California; as such, the findings may not be generalizable to other populations with severe PAD. We did not make direct contact with patients or their healthcare providers; therefore, we were not able to determine reasons patients were not prescribed a statin. It is possible that some patients were statin intolerant or were otherwise not eligible for a statin. We also cannot determine whether the healthcare provider or the patient chose to discontinue the statin in the year following the diagnosis. Further, our cohort concluded in 2015 and, thus, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors were not included in this analysis. However, PCSK9 inhibitors are not widely prescribed in our healthcare system. Data from 18 health systems participating in the National Patient-Centered Clinical Research Network (PCORNet) demonstrated that < 1% of the eligible 3.6 million patients aged 18 years and older were prescribed a PCSK9 inhibitor. 43 Lastly, it is possible that some patients we identified as incident severe PAD had pre-existing PAD, as the diagnosis codes are contingent upon documentation of PAD or CLI during a patient encounter. The strengths of the study include the large and diverse population with complete capture of point-of-care information including LDL-C levels and sold/dispensed statins.
Conclusion
In conclusion, the findings from our study show an encouraging trend toward greater use of high-intensity statins in this high-risk population. However, a substantial proportion of patients with severe PAD including CLI remained untreated or discontinued therapy within 1 year of their diagnosis. Further, the majority of patients on a statin did not have an intensification of therapy in the 1 year following their PAD diagnosis. These findings add to the growing body of literature demonstrating that many high-risk patients with PAD do not receive or stay on statin therapy. Given the burden of severe PAD, efforts aimed at identifying strategies to increase use of statin therapy are warranted.
Supplemental Material
10.1177_1358863X19871100_Supplemental_tables_and_figures – Supplemental material for Trends in statin utilization among adults with severe peripheral artery disease including critical limb ischemia in an integrated healthcare delivery system
Supplemental material, 10.1177_1358863X19871100_Supplemental_tables_and_figures for Trends in statin utilization among adults with severe peripheral artery disease including critical limb ischemia in an integrated healthcare delivery system by Kristi Reynolds, Katherine E Mues, Teresa N Harrison, Lei Qian, Songyue Chen, Jin-Wen Y Hsu, Kiran J Philip, Keri L Monda, Stephanie R Reading and Somjot S Brar in Vascular Medicine
Footnotes
Acknowledgements
The authors thank the patients of Kaiser Permanente for helping us improve care from the use of information collected through our electronic health record systems.
We would like to thank Mercedes A Munis (Department of Research & Evaluation, Kaiser Permanente Southern California) for assistance with the preparation of the tables and figures.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Reynolds reports institutional research grants from Regeneron, Sanofi, and Amgen, Inc. Drs Mues, Philip, Monda, and Reading are employed by Amgen, Inc.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a contractual agreement between the Southern California Permanente Medical Group and Amgen, Inc. The design and conduct of the study, interpretation of the results, and preparation of the manuscript was supported through a research grant from Amgen, Inc. (Thousand Oaks, CA). The authors from Kaiser Permanente conducted all analyses. Representatives of the funding agency were involved in the study design, manuscript writing, and decision regarding journal submission. Said representatives were not directly involved in the collection, management, or analysis of the data.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.