
Abstract
The aim of this study was to assess postoperative opioid prescribing patterns, usage, and pain control after common vascular surgery procedures in order to develop patient centered best-practice guidelines. We performed a prospective review of opioid prescribing after seven common vascular surgeries at a rural, academic medical center from December 2016 to July 2017. A standardized telephone questionnaire was prospectively administered to patients (n = 110) about opioid use and pain management perceptions. For comparison we retrospectively assessed opioid prescribing patterns (n = 939) from July 2014 to June 2016 normalized into morphine milligram equivalents (MME). Prescribers were surveyed regarding opioid prescription attitudes, perceptions, and practices. Opioids were prescribed for 78% of procedures, and 70% of patients reported using opioid analgesia. In the prospective group, the median MMEs prescribed were: VEIN (31, n = 16), CEA (40, n = 14), DIAL (60, n = 17), EVAR (108, n = 8), INFRA (160, n = 16), FEM TEA (200, n = 11), and OA (273, n = 4). The median proportion of opioids used by patients across all procedures was only 30% of the amount prescribed across all procedures (range 14–64%). Patients rated the opioid prescribed as appropriate (59%), insufficient (16%), and overprescribed (25%), and pain as very well controlled (47%), well controlled (47%), poorly controlled (4%), and very poorly controlled (2%). In conclusion, we observed significant variability in opioid prescribing after vascular procedures. The overall opioid use was substantially lower than the amount prescribed. These data enabled us to develop guidelines for opioid prescribing practice for our patients.
Introduction
Over the past decade there has been a dramatic increase in prescription opioid use for pain control, with a concomitant rise in opioid abuse. 1 The Centers for Disease Control and Prevention reported that 259 million prescriptions were written for opioids in 2012. 2 According to the National Survey on Drug Use and Health, 4.3 million Americans used prescription pain relievers for non-medical purposes in 2014. 3 Beginning in 2011, non-heroin opiates were the leading cause of substance abuse treatment admissions and drug-related fatalities in Vermont. 4 As a result of this public health crisis, medical professionals are examining their role in the opioid epidemic by analyzing prescribing practices and characterizing the pain management needs of their patients.
Despite growing concern surrounding opioid prescription and the potential for subsequent abuse, little has been published on opioid prescribing practices after vascular surgery. There is no consensus regarding prescribing practices, especially with regard to standards for the duration and quantity of opioids prescribed after specific procedures.
The goal of this study was to assess postoperative opioid prescribing patterns, usage, and pain control after common vascular surgeries. First, we aimed to describe health care professionals’ practice patterns and perceptions toward opioid prescribing at discharge through a retrospective analysis and prescriber survey. Second, we aimed to assess the patient experience with postoperative pain management, including actual medication usage and satisfaction with pain control through a prospective survey. Our final objective was to develop evidence-based guidelines to standardize opioid prescribing after vascular surgery.
Methods
We performed a retrospective and prospective review of opioid prescribing practice after seven common elective vascular surgery procedures at the University of Vermont Medical Center from July 2014 to June 2017. During the study period no institutional or departmental protocols or quality improvement initiatives were in place regarding opioid prescribing, and the state-wide prescription database was not in use.
Vascular procedures
The procedures included radiofrequency ablation of the greater saphenous vein with or without varicose vein ligation (VEIN), carotid endarterectomy (CEA), dialysis access procedures (DIAL) including arteriovenous fistula (AVF) and prosthetic grafts (15 AVFs, two transposition AVFs, and two arteriovenous grafts), infrainguinal bypasses (INFRA), femoral endarterectomy (FEM TEA) with or without concomitant peripheral vascular intervention, endovascular abdominal aortic aneurysm repairs (EVAR), and open aortic procedures (OA), which included both open abdominal aortic aneurysm repair and aortobifemoral bypass. Prior opioid use was defined on the date of surgery as any opioid use within the past month.
Retrospective review of opioid prescribing
A retrospective review of opioid prescribing patterns from July 2014 to June 2016 was conducted to establish baseline prescribing practices. This historical cohort included 939 patients who underwent one of the vascular procedures of interest: VEIN (n = 418), CEA (n = 170), DIAL (n = 161), INFRA (n = 76), FEM TEA (n = 38), EVAR (n = 27), and OA (n = 49). Procedure and prescribing data were extracted from the clinical data warehouse with support from the UVMMC Jeffords Institute for Quality and Operational Effectiveness. The data warehouse includes electronic medical record data from an Epic-based system in place since 2009. Opioid prescriptions at discharge were converted into morphine milligram equivalents (MME) as recommended by the Centers for Disease Control and Prevention. 5 Five vascular surgery attending physicians and three mid-level providers were asked to categorize the seven procedures into one of four pain control categories based on daily opioid dosing according to their experience: none, low (30 MME), moderate (60 MME), and high (90 MME).
Prospective review of opioid prescribing
We administered a standardized telephone questionnaire to 110 patients between December 2016 and July 2017 (supplementary online Appendix A). This prospective cohort included: VEIN (n = 20), CEA (n = 21), DIAL (n = 19), INFRA (n = 19), FEM TEA (n = 13), EVAR (n = 13), and OA (n = 5). VEIN procedures included phlebectomy of varicose veins with radiofrequency ablations in 13 and high ligations of the saphenous vein in three cases.
Eligible patients were identified through UVMMC’s electronic operating room scheduler (Picis Clinical Solutions, Inc., Wakefield, MA, USA) and entered into Research Electronic Data Capture (REDCap, Nashville, TN, USA) a secure, HIPAA-compliant web-based software application designed for electronic collection and management of research and clinical study data.
Patients undergoing one of the above elective procedures with discharge to home were offered enrollment if they were ⩾ 18 years old and able to provide informed consent. Patients were excluded if the operation was urgent or emergent, involved multiple procedures, or if they had another procedure within the previous 30 days. Patients were also excluded if they required reoperation during the index hospitalization, discharge to a location other than home, or if they required readmission during the 30-day postoperative period.
Patients were contacted 5–7 days after discharge and administered a standardized telephone questionnaire including questions regarding discharge instructions on pain control, opioid prescription (dose, quantity, and duration), the amount of opioid used, and their perceptions on the adequacy of pain management. If a patient was still taking an opioid medication at the time of the first contact, the patient was re-contacted 7–10 days later to ascertain how much total opioid they used and if any medication refills were required. The electronic medical record (EMR) was cross-referenced for details regarding the initial opioid prescription at discharge. After enrollment, subjects were excluded if they were unable to be reached, declined to participate, or were unable to understand the questionnaire due to barriers such as hearing impairment, mental status, or language. Of 154 eligible patients, 73% (112/154) were contacted and 98% (110/112) completed the telephone questionnaire.
Prescriber survey
Prescribers (n = 4), including a vascular service physician assistant, two nurse practitioners, and a 5+2-year vascular fellow, were anonymously surveyed regarding their opioid prescription attitudes, perceptions, and practices (supplementary online Appendix B). In brief, the survey included questions regarding an individual’s background, training, and areas of concern regarding postoperative opioid prescribing and current understanding of opioid monitoring in the state of Vermont.
Outcomes
Our primary measure was the proportion of opioid medication used by the patient compared to the amount prescribed at discharge. Secondary measures included the type and amount of medication prescribed (including as-needed prescriptions), patients’ satisfaction with their pain management, education regarding alternative pain management instructions, and instructions regarding proper disposal of leftover opioids.
Statistical analysis
Univariate statistics were used to characterize the MMEs prescribed for specific surgical procedures in the retrospective and prospective periods. The types and amounts of opioid prescribed between periods were compared using Kruskal–Wallis rank tests. Analyses were carried out with Stata, version 14.2 (StataCorp, College Station, TX, USA).
The study followed the principles of the Declaration of Helsinki and the University of Vermont Institutional Review Board approved the study protocol, including the informed consent document (CHRMS #16-443).
Results
Retrospective prescribing survey
The average patient age in the retrospective cohort was 63 years old, 52% were male, and 18% were current smokers. Preoperative opioid use was recorded in 11% (12/110) of patients and distributed across seven procedures. In the retrospective cohort, 85% (799/939) were prescribed an opioid medication upon discharge to home. The median MME per procedure was: VEIN 96, CEA 80, DIAL 100, EVAR 96, INFRA 300, FEM TEA 200, and OA 240 (Table 1). The opioids prescribed included hydrocodone (28%), oxycodone (27%), hydromorphone (25%), and tramadol (4%). Morphine and codeine were each prescribed for less than 1% of procedures. The five vascular surgeons and three mid-levels categorized the expected daily dosing as ‘none’ to ‘low’ for VEIN, CEA, AV access, and EVAR, ‘moderate’ for FEM TEA and INFRA, and ‘high’ for OA surgery, with no significant variability amongst respondents.
Retrospective analysis of opioid prescriptions at discharge, July 2014 – June 2016.
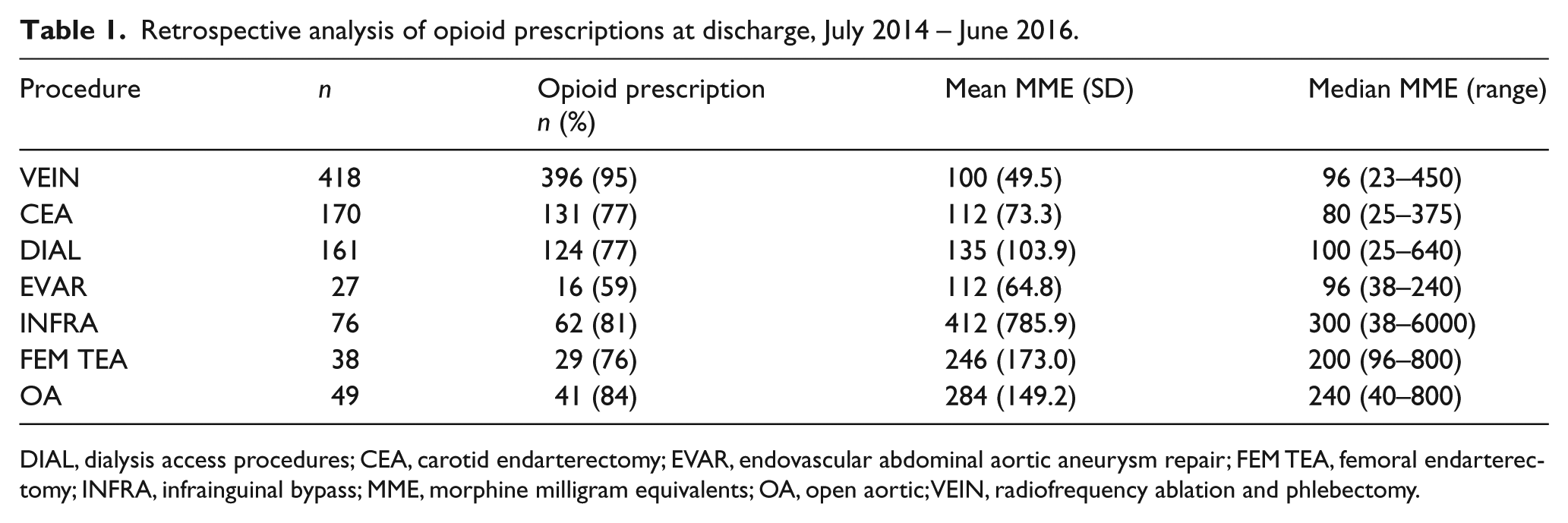
DIAL, dialysis access procedures; CEA, carotid endarterectomy; EVAR, endovascular abdominal aortic aneurysm repair; FEM TEA, femoral endarterectomy; INFRA, infrainguinal bypass; MME, morphine milligram equivalents; OA, open aortic; VEIN, radiofrequency ablation and phlebectomy.
Prospective group
In the prospective cohort, 110 patients completed the survey; the average age was 63 years (SD 13.2), 55.7% were males, and 12% had been on opioids prior to surgery. A total of 78% (n = 86) patients were prescribed an opioid medication at discharge, with the median MMEs prescribed ranging from 31 to 273 across all procedures: VEIN (31, n = 16), CEA (40, n = 14), EVAR (108, n = 8), DIAL (60, n = 17), INFRA (160, n = 16), FEM TEA (200, n = 11), and OA (273, n = 4) (Table 2).
Prospective analysis of opioids prescribed for seven vascular procedures.
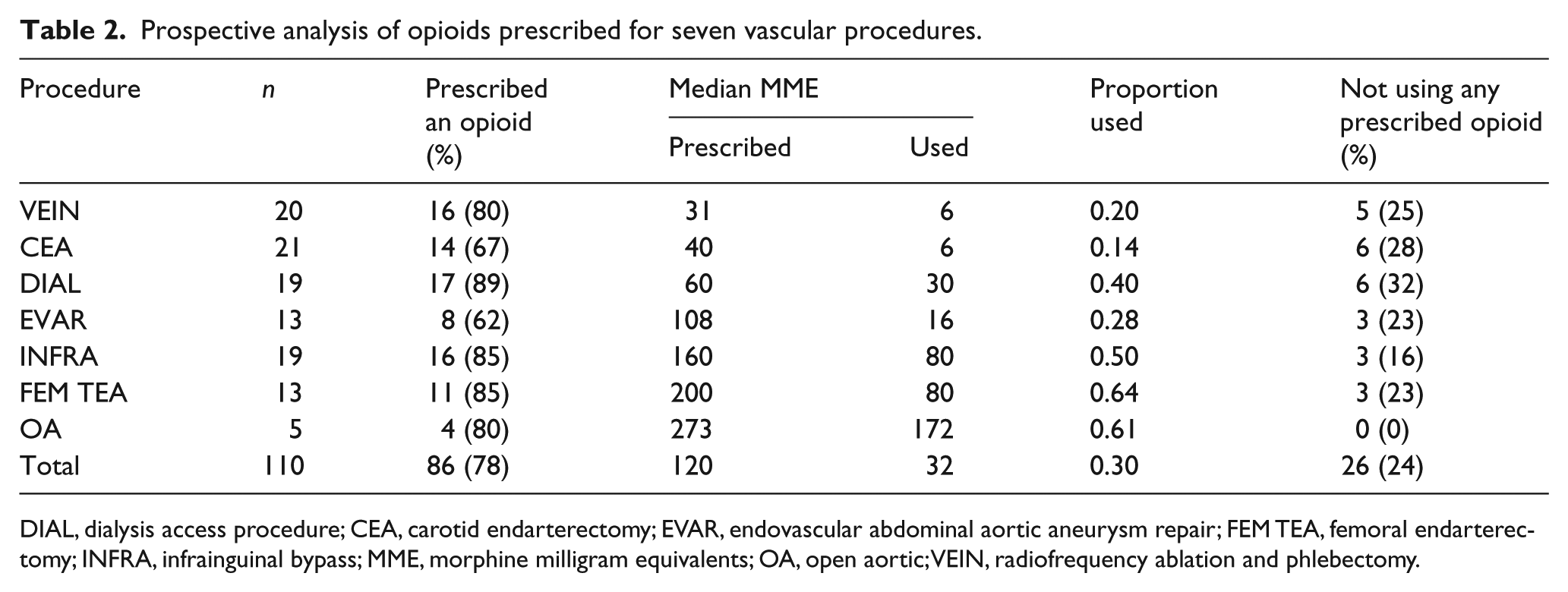
DIAL, dialysis access procedure; CEA, carotid endarterectomy; EVAR, endovascular abdominal aortic aneurysm repair; FEM TEA, femoral endarterectomy; INFRA, infrainguinal bypass; MME, morphine milligram equivalents; OA, open aortic; VEIN, radiofrequency ablation and phlebectomy.
Hydromorphone (60%) was the most commonly prescribed opioid at discharge followed by oxycodone (22%), tramadol (13%), and hydrocodone (6%) (Figure 1). When comparing the median MMEs prescribed in the retrospective versus prospective group data, there was a significant reduction in MMEs prescribed for several procedures in the prospective group: VEIN –49 MME, p < 0.0001; CEA –40 MME, p = 0.0002; DIAL –60 MME, p = 0.0001; INFRA –160 MME, p = 0.0015 (Figure 2). Three procedures had no significant change in MMEs prescribed (EVAR, p = 0.90; FEM TEA, p = 0.62; OA, p = 0.94).
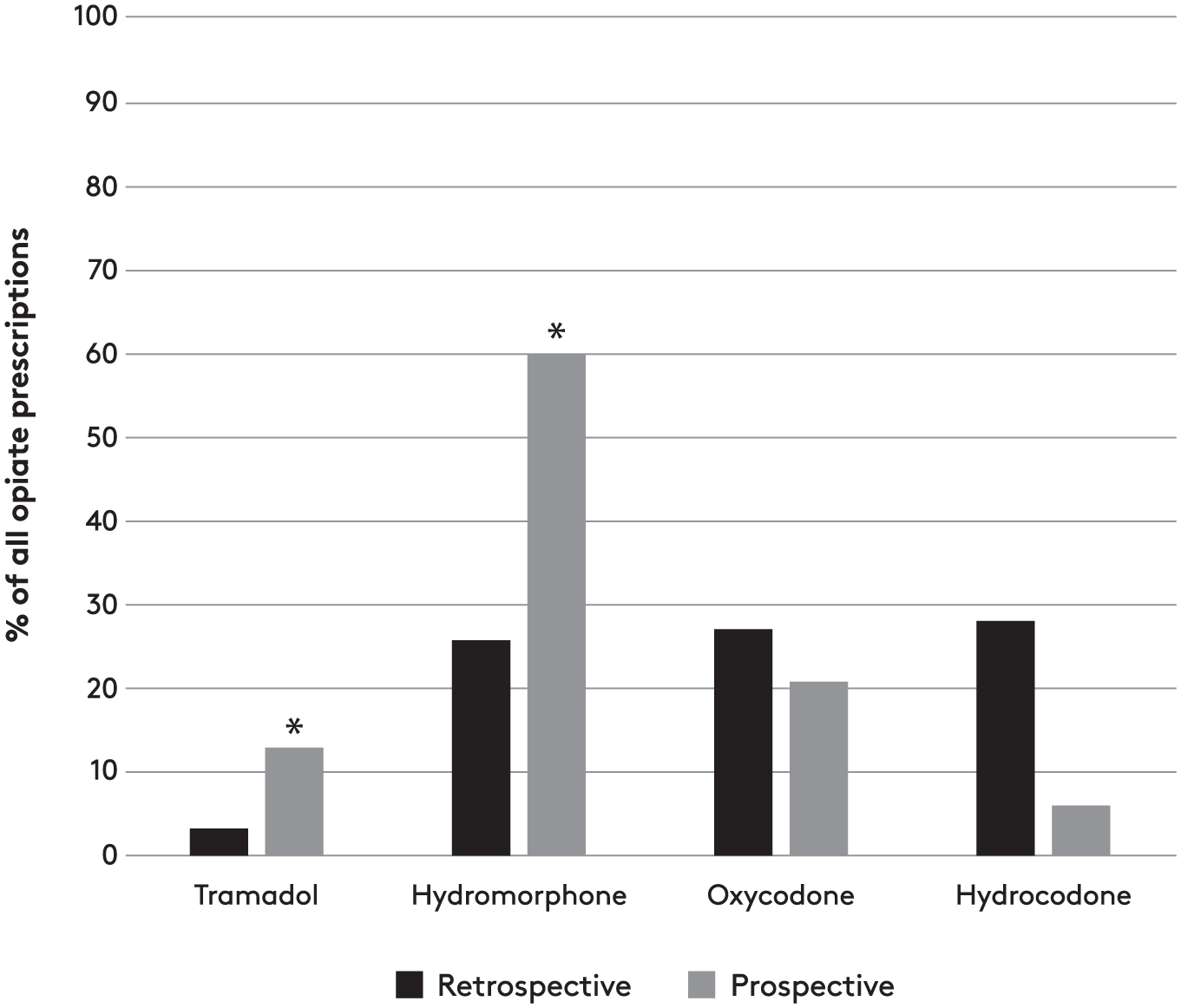
Types of opioids prescribed at discharge in the retrospective and prospective groups.
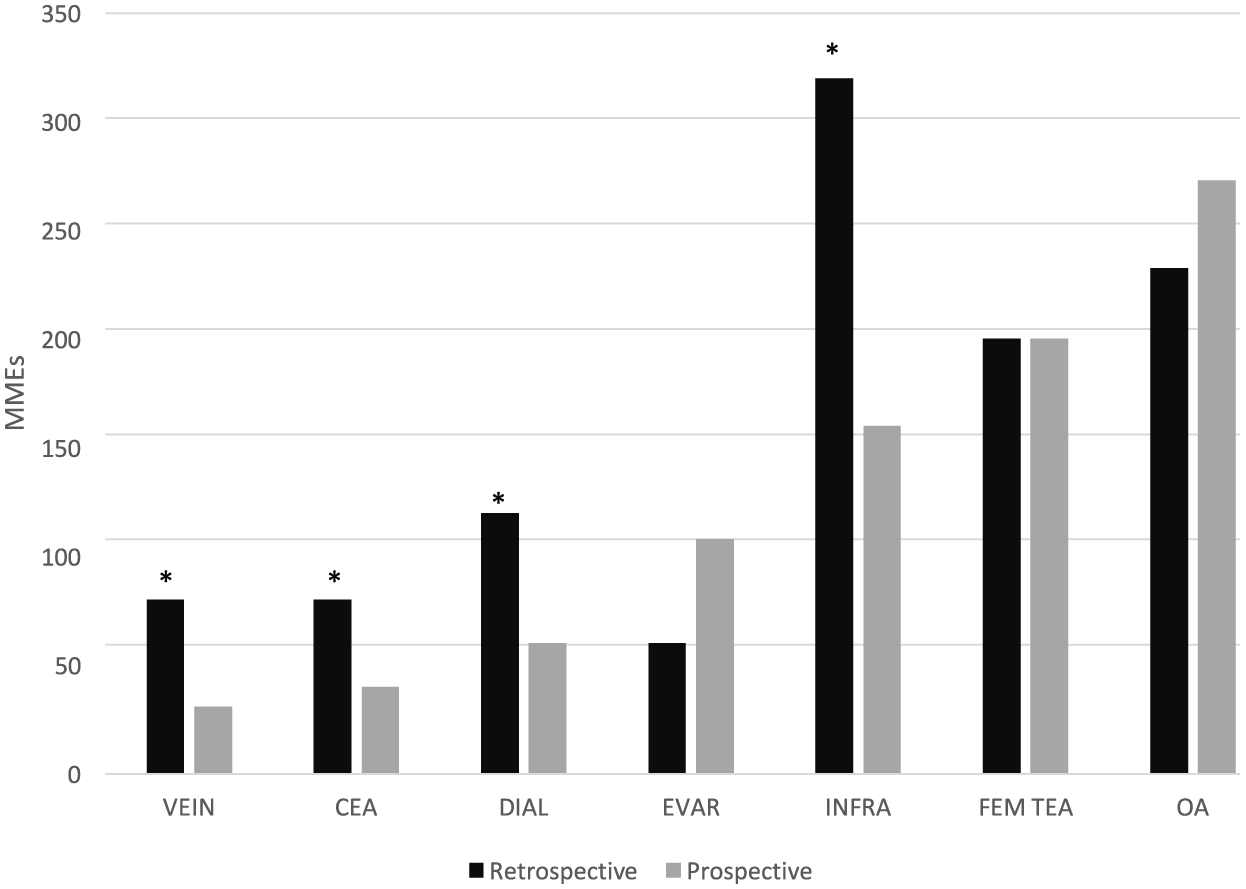
Median MMEs per procedure in the retrospective versus prospective groups.
After a vascular procedure, 78% of patients were prescribed an opioid medication at discharge. Of these patients prescribed an opioid, 70% reported using at least some of the medication. The median proportion of dispensed opioid used was 30% for all procedures and ranged from 14% to 64% across procedures. One-quarter of all patients receiving an opioid at discharge reported not using any of the medication (range of 0–43% across procedures) (Figure 3). For each procedure variability was noted in the proportion of opioid used across individual patients.
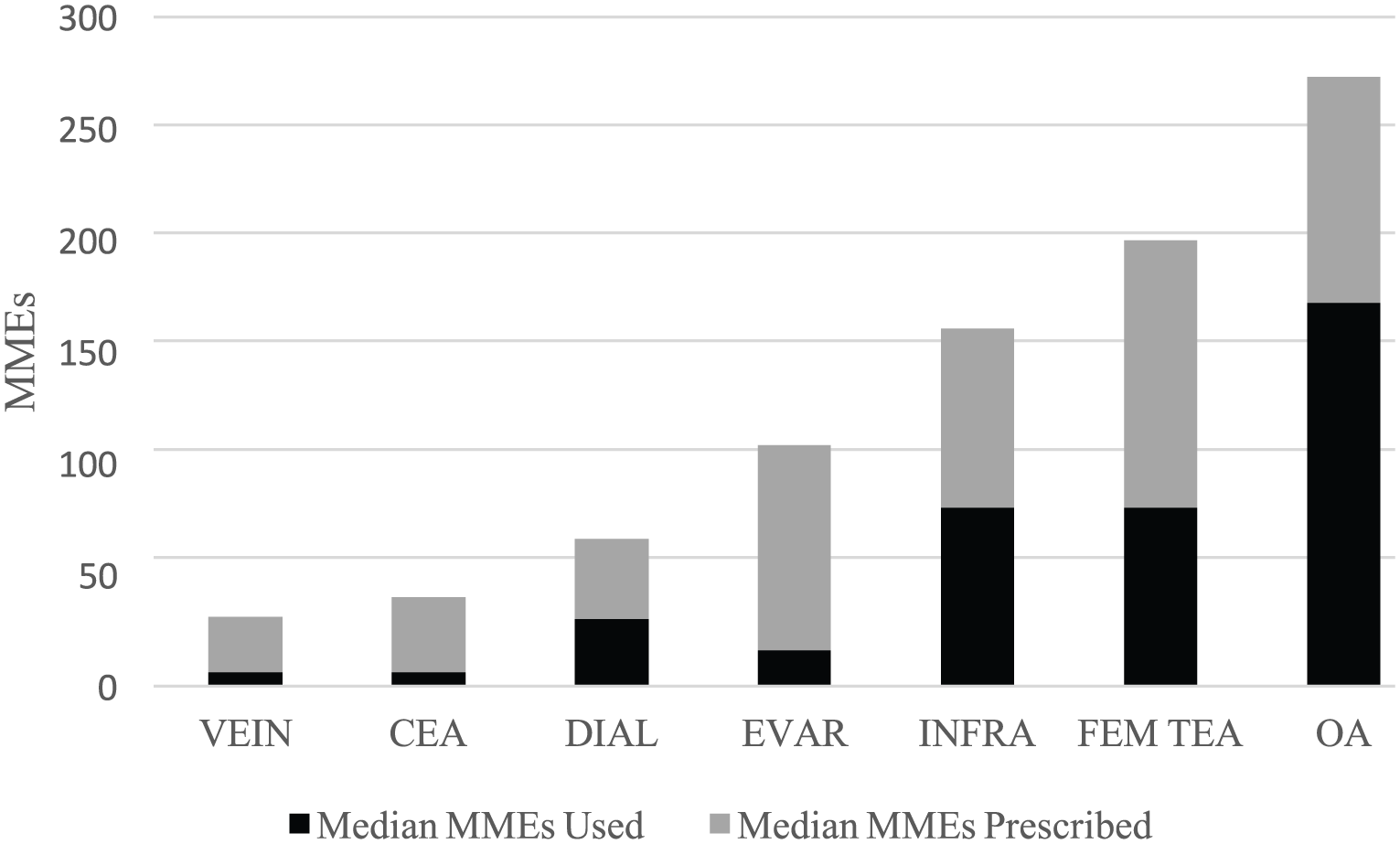
Proportion of median MMEs used per procedure compared to prescribed.
At the time of the first telephone call, 5–7 days after discharge, 36% were still taking medication, most commonly post FEM TEA (75%) and INFRA (62%) procedures. Only 8% of patients required a refill of their medication, most commonly after INFRA procedures (14%). Only 29% of patients reported receiving instructions on how to dispose of unused pain medication. A total of 73% of patients received instructions regarding non-opioid pain management strategies, of which 96% included the use of acetaminophen or non-steroidal anti-inflammatory drugs in place of or to supplement opioid analgesia (Figure 4).
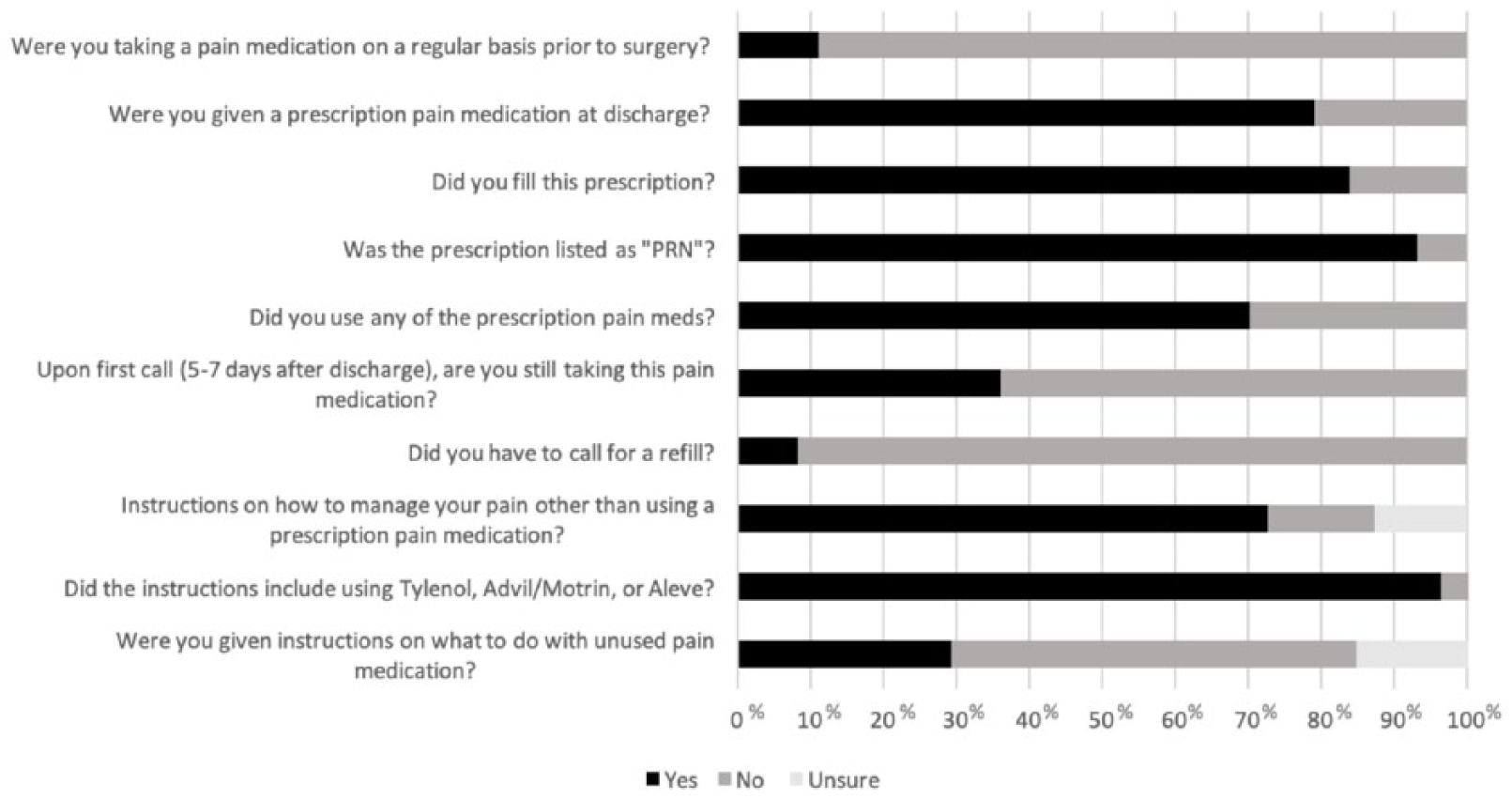
Responses to patient survey.
Patient satisfaction
Patients rated their pain control as very well controlled (47%), well controlled (47%), poorly controlled (4%), and very poorly controlled (2%). Patients rated the amount of opioid prescribed as just the right amount (59%), less than needed (16%), and more than needed (25%) to manage their pain needs. The subset of patients (n = 23) that did not receive an opioid prescription reported satisfaction as very well (52%), well (39%), poorly (9%), and very poorly controlled (0%). Overall satisfaction was 92% versus 94% in patients with preoperative opioid use versus opioid-naïve groups.
Prescriber survey
All prescribers responded that prescription misuse ‘is an important issue for providers’, and that the medical community needs to do a ‘better job addressing the issue of prescription misuse’. All were either ‘somewhat satisfied’ or ‘somewhat dissatisfied’ with the education and training they had received regarding prescribing opiates, though they felt that formal lectures were very influential in their training around opioid prescribing. All would like to know how their prescription patterns compare to those of their peers. Respondents cited opioid misuse as an important issue for surgeons and indicated a need for peer comparison, continuing education, and protocols for opioid prescription.
Discussion
In this study, we found clinically significant overprescribing of postoperative opioids based on the fact that, on average, patients only used one-third of the amount prescribed. Opioid use and abuse in America has become a public health crisis likened to an ‘epidemic’. The opioid epidemic has forced us to examine our role in solving the problem of misuse and non-medical use of opioids. Misuse of prescription drugs is defined as taking a medication in a way or dose other than prescribed, using another person’s prescription (even if for a legitimate medical complaint), or to feel euphoria. 6 Non-medical use of prescription drugs is included in these categories of misuse. 6 Several studies have reported that both minor and major surgery are risk factors for chronic opioid use.7,8 The incidence of chronic opioid use in opioid-naïve patients undergoing surgery ranges from 3% to 13%.7–10 In a study of long-term analgesia after four low-risk surgeries in Canada, Alam et al. reported that 51% of patients were prescribed opioids after varicose vein surgery, and that patients receiving an opioid prescription were 44% more likely to use opioids long term. 9 The rate of continued opioid use after surgery is substantially higher in patients with chronic opioid use, reaching as high as 77% after bariatric surgery. 11
The reasons for the opioid problem are multifactorial but include American cultural norms regarding pain and the proliferation of opioids for relief, as evidenced by the fact that the United States consumes 99% of the world’s supply of hydrocodone and 83% of the world’s oxycodone. 12 The attention to perioperative pain is underscored by the highly publicized effort by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) to label pain as the ‘fifth vital sign’, which prompted hospitals to develop policies aimed at treating pain.13,14 Overprescribing coupled with a poorly developed system for disposal can result in diversion of medication.15,16 Finally, the lack of data and surgeon driven evidence-based guidelines have contributed.
Sun et al. reported that risk factors for chronic opioid use in surgical patients include male sex, age > 50 years, and a preoperative history of drug abuse, alcohol abuse, depression, and benzodiazepine or antidepressant use. 7 This large study, and others, have identified different risks based on the type of operation.7,10 Unfortunately, representation of vascular surgery is very limited in all these studies, making our study one of the few to examine opioid prescribing practice and patient response after vascular procedures.
As expected, we found a wide variation in the amount of opioids prescribed between procedures at discharge. Comparing the MMEs prescribed in the retrospective versus prospective group data, we noted an approximately 50% or greater reduction in median MMEs prescribed for several procedures in the prospective group (VEIN, CEA, DIAL, INFRA). Three procedures had no statistical change in MMEs prescribed (EVAR, FEM TEA, and OA). The reason for this decrease is not apparent but may be secondary to the increased awareness of the opioid problem. There was no systemic effort to change prescribing practice. Based on our survey data, prescribers’ preconceived estimates of low/moderate/high MME requirements were broadly in line with patients’ actual usage. However, this did not translate into effective prescribing. The most striking and unexpected finding was that the vast majority of opioids prescribed at discharge went unused, as shown by the median usage of dispensed opioids of only 30%. Across all vascular procedures, only 20% of patients reported using all of their pain medication and only 8% of patients asked for a refill of their opioid, with infrainguinal bypass accounting for 67% of the requested refills. Hill et al. reported similar findings after five outpatient general and breast surgeries. 17
Satisfaction with analgesia was high, with 94% of all surveyed patients reporting that their pain was either ‘very well controlled’ (47%) or ‘well controlled’ (47%). A total of 59% of patients prescribed an opioid stated that they were prescribed ‘just the right amount of medication’, and only 25% responded that they were prescribed more medication than needed. The discordance between this survey response and the amount of unused opioids highlights the need for patient education. The majority (73%) of patients were given instruction on alternatives to prescription pain medication. Only 29% of patients were given instructions on what to do with unused pain medications. The above findings indicate there is a prime opportunity for quality improvement to decrease the amount of opioids prescribed without reducing patient pain control. Fortunately even simple measures, such as a reminder card for surgeons listing best practices for non-opioid analgesia and opioid guidelines, have been shown to be effective. 18
Based on this study, the vascular surgery division implemented new guidelines for postoperative opioid prescribing as part of a departmental wide initiative (see supplemental online Appendix C). Consensus was reached on the amount of opioids that should be prescribed for each procedure, factoring in the anticipated day of discharge. Specific procedures, such as CEA and vein ablations, were targets for not needing postoperative opioids – with the alternative of using non-opioid medications. VHD rules for opioid prescribing for acute pain include: (1) written informed consent for first-time prescriptions; (2) use of non-opioid analgesics; (3) limiting opioids to 350 MME, or 50 MME/day; (4) database monitoring for prescriptions over 10 pills and for refills; and (5) patient education about methods of storage and disposal.
Study limitations
There are several limitations to this study, including the lack of randomization, which would be difficult and ethically problematic. We included a small number of open aortic procedures and did not include subsets of patients, such as major amputees, and excluded patients discharged to a rehabilitation facility. The usage of MMEs postoperatively is a complex process that can be affected by numerous variables. We did try to control for some variables via our inclusion/exclusion criteria; however, we do acknowledge that we cannot control for all confounders. There is a larger, department-wide study ongoing at our institution that will include multiple surgical specialties and control for patient and surgical factors such as complications and redo surgery. Our findings may not be applicable to all vascular practices since we focused on a group of surgeons with fairly established practices at a single hospital. The main strength of the study is direct surveying of patients, including actual opioid usage. This powerful tool gives a unique and insightful understanding into how patients manage their postoperative pain. We expect this data will allow us to study the impact of the changes mandated by the VDH that are being implemented at our institution. In particular, we must remain aware of unintended consequences, such as increased pain, or the potential for increases in emergency room visits or hospital readmission, which have been linked to high postoperative pain. 19
Conclusion
Historically, opioid prescribing after vascular surgery has been anecdotal and based on opinion rather than evidence-based guidelines. Our data showed significant variability exists in opioid prescribing patterns across vascular procedures but, overall, opioid use was substantially lower than prescribed. Using this information we developed vascular surgery specific guidelines for postoperative prescribing that can serve as a reference for others. Vascular surgeons should examine their practice in an effort to reduce opioid prescribing while maintaining patient analgesia.
Supplemental Material
10.1177_1358863X18807540_Supplementary_material_AppendixA – Supplemental material for Postoperative opioid prescribing patterns and use after vascular surgery
Supplemental material, 10.1177_1358863X18807540_Supplementary_material_AppendixA for Postoperative opioid prescribing patterns and use after vascular surgery by Ilsley B Colton, Mayo H Fujii, Thomas P Ahern, Charles D MacLean, Julie E Lahiri, Matthew Alef, Andrew C Stanley, Georg Steinthorsson and Daniel J Bertges in Vascular Medicine
Supplemental Material
10.1177_1358863X18807540_Supplementary_material_AppendixB – Supplemental material for Postoperative opioid prescribing patterns and use after vascular surgery
Supplemental material, 10.1177_1358863X18807540_Supplementary_material_AppendixB for Postoperative opioid prescribing patterns and use after vascular surgery by Ilsley B Colton, Mayo H Fujii, Thomas P Ahern, Charles D MacLean, Julie E Lahiri, Matthew Alef, Andrew C Stanley, Georg Steinthorsson and Daniel J Bertges in Vascular Medicine
Supplemental Material
10.1177_1358863X18807540_Supplementary_material_AppendixC – Supplemental material for Postoperative opioid prescribing patterns and use after vascular surgery
Supplemental material, 10.1177_1358863X18807540_Supplementary_material_AppendixC for Postoperative opioid prescribing patterns and use after vascular surgery by Ilsley B Colton, Mayo H Fujii, Thomas P Ahern, Charles D MacLean, Julie E Lahiri, Matthew Alef, Andrew C Stanley, Georg Steinthorsson and Daniel J Bertges in Vascular Medicine
Footnotes
Acknowledgements
Presented at the 44th Annual Meeting of the New England Society for Vascular Surgery, Boston, MA, USA; Oral plenary presentation, September 8, 2017.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.