
Abstract
The neutrophil–lymphocyte ratio (NLR), as a marker of inflammation, is associated with the severity of peripheral artery disease (PAD). The role of the NLR on predicting future complications after elective revascularization for patients with PAD remains unknown. We aimed to examine the role of the NLR in the development of major adverse limb events (MALE) and the long-term mortality of these patients. We evaluated 1708 revascularization procedures from May 2001 to December 2015 at the Veterans Affairs Western New York Healthcare System from a prospectively maintained vascular database that included demographics, comorbidities and pre-procedural medications. Peri-procedural laboratory findings including complete blood cell count and metabolic panel were further retrieved from the electronic health record. The NLR was calculated, and the patients were categorized into tertiles according to NLR cut-off points. Multivariate Cox regression analysis was performed to determine MALE and 10-year mortality. The primary endpoint of the study was MALE, and the secondary endpoint included 10-year mortality. A total of 1228 patients were included for final analyses. Patients in the third NLR tertile were more likely to experience MALE during the follow-up period (p<0.001). In addition, fewer patients in tertile 3 survived over the follow-up period compared to tertiles 1 and 2 (p<0.0001). Patients in tertile 3 tended to be older with a higher frequency of hypertension, diabetes, chronic kidney disease, coronary artery disease and congestive heart failure. Our multivariate analysis demonstrated that the NLR was independently associated with higher rates of MALE in the affected vessels following revascularization procedures. Similarly, the NLR was revealed to be an independent predictor of higher long-term mortality in these patients.
Keywords
Introduction
Peripheral artery disease (PAD) of the lower extremities is a manifestation of a systemic atherosclerotic disease, 1 affecting approximately 8.5 million Americans aged 40 years or more and 202 million people globally.2,3 In addition to the increased risk of cardiovascular and limb events,4,5 PAD leads to impaired daily function and decreased quality of life. 6 While lifestyle modifications and medical treatment is the main therapy for patients with PAD,7,8 in a subset of patients, including those with persistent lifestyle-limiting claudication, endovascular or surgical revascularization is inevitable.7,9 However, restenosis after stenting is a major concern10,11 that mandates identifying determinants of long-term success.12–14
The ratio of the number of neutrophils to the number of lymphocytes (NLR) in peripheral blood as a marker of inflammation is suggested to be associated with the complexity of PAD. 15 It has recently shown that the NLR is an independent predictor of death or major amputation among PAD patients with advanced chronic kidney disease following percutaneous transluminal angioplasty. 16 In addition, in patients with critical limb ischemia, an elevated NLR was independently associated with higher mortality. 17 Another study in patients with critical limb ischemia or intermittent claudication has demonstrated an association between increased NLRs and higher cardiovascular mortality.18,19 In 126 patients, the postoperative but not preoperative NLR was predictive of infra-inguinal bypass graft patency at 1 year. 20 Furthermore, a higher white blood cell count (WBC) and neutrophil count but not lymphocyte count was shown to predict a worse outcome in patients undergoing percutaneous transluminal angioplasty for advanced PAD. 21 However, the predictive role of pre-procedural NLR in the development of major adverse limb events (MALE) after elective revascularization for PAD is unknown.
To further examine the validity of this inflammatory marker in a large retrospective cohort study, we aimed to evaluate the predictive value of pre-procedural NLR for MALE, including limb amputations, open revision and bypass procedures on the same leg, or thrombolysis procedures at follow up as the primary endpoint and 10-year mortality as the secondary endpoint in patients who had undergone an elective revascularization procedure for PAD. We hypothesized that patients with higher NLR values are more likely to develop MALE and they carry a higher risk of dying within 10 years of revascularization.
Methods and patients
This is a retrospective cohort study including all patients with a diagnosis of lower-limb PAD who had undergone revascularization (stenting/bypass graft) from May 2001 to December 2015 at the Veterans Affairs Western New York Healthcare System. The study protocol and methods of data collection were reviewed by the institutional review board (IRB) at this facility and were approved by both the IRB and research and development committee. Owing to its chart review nature and the minimal risk involved, the study was waived from obtaining informed consent from the participating patients. Patients with acute limb ischemia upon presentation and also those who had undergone an amputation for a non-salvageable limb were excluded from the study.
Demographics information, comorbidities including ischemic heart disease, chronic kidney diseases, diabetes mellitus, hypertension, pre-procedural medications, laboratory findings (including neutrophil, lymphocyte and platelet count) before the procedure and status of the limb at last follow up were retrieved from patients’ medical records. The NLR was calculated by dividing the neutrophil count by the lymphocyte count in the peripheral blood sample. The follow-up data for defined clinical outcomes and long-term all-cause mortality were obtained from the VA system. In the VA system, the death of a patient is reported through Veterans Benefits Administration regardless of the location of death, and all deaths are registered within 24 hours even if they have occurred outside of the VA. After discharge of patients, the in state and out of state patient records are scanned to the computerized patient records program.
All patients were followed postoperatively, and at 3 and 6 months, and every 6 months thereafter for ankle–brachial index (ABI) measurements, graft or stent velocities, and duplex imaging. The minimum period of follow up was 1 year after the primary procedure. The status of the limb at last follow-up was categorized into two groups based on the primary stent/graft patency as well as the occurrence of MALE. The loss of patency was defined as occlusion, >70% restenosis, an elevated ratio of velocity to the proximal segment being >300% by duplex examination, loss of a previously palpable pulse, dampened pulse volume recordings (PVR) or a decrease in ABI of >0.2. Repeated interventions were performed for maintaining patency, or when clinically indicated.
Primary patency was defined as patency of the endovascular treated segment or bypass without the need for additional or secondary surgical or endovascular procedures, or the interval from the time of the original intervention until any intervention designed to maintain or re-establish patency is performed. Assisted primary patency was defined as patency of the endovascular intervention achieved with the use of an additional or secondary surgical or endovascular procedure, as long as occlusion of the primary treated site has not occurred. Secondary patency is patency obtained with the use of an additional or secondary surgical or endovascular procedure after occlusion occurs.
Primary and secondary endpoints
MALE was defined as the primary endpoint of the study. All-cause mortality for 10 years and major adverse cardiac event (MACE) were defined as our secondary endpoints. MALE included occurrence of one or more of the following events: limb amputations, open revision and bypass procedures on the same leg, or thrombolysis procedures. 22 MACE included occurrence of one or more of the following events: cardiac arrest, death, postoperative myocardial infarction, cardiogenic shock and hemodynamically significant dysrhythmias, within 30 days of surgery.
Statistical analysis
Data analysis was performed using IBM SPSS 24.0 (IBM Corp., Armonk, NY, YSA). Descriptive statistics were stated as mean ± standard deviation for continuous variables and frequency (%) for categorical variables. The chi-squared test or Fisher’s exact test were used for comparing categorical variables as appropriate. Bonferroni adjustment was used for all multiple comparisons. For comparing the numerical data, the independent t-test or Mann–Whitney U-test (in non-normally distributed variables) were used. Patients were categorized into three groups based on NLR tertile cut-off points and compared regarding study variables. For determining the independent predictors of MALE and 10-year mortality, multivariate Cox regression analysis was performed. We used receiver operating characteristic (ROC) curves to determine the sensitivity and specificity of the NLR in predicting study endpoints. Since the SPSS program does not automatically provide C statistics for multivariable regressions, separate binary logistic regression analyses were performed for the Cox models built for MALE and 10-year mortality and the predicted probabilities were saved for each occurrence. Subsequently, the area under the curve (AUC ± SE) was provided for each model as a part of the corresponding tables. A two-sided p-value less than 0.05 was considered as statistically significant.
Results
From May 2001 through December 2015, a total of 1708 lower extremities were revascularized. Following exclusion of the repeat procedures and those with missing data, 1228 patients were analyzed (Figure 1). The study cohort comprised mainly elderly men (median age of 67 (61–75) years), with only 14 female patients. The NLR values were significantly lower among the survivors compared to those who died within 5 and 10 years of their revascularization date (p<0.0001) (Figure 2).
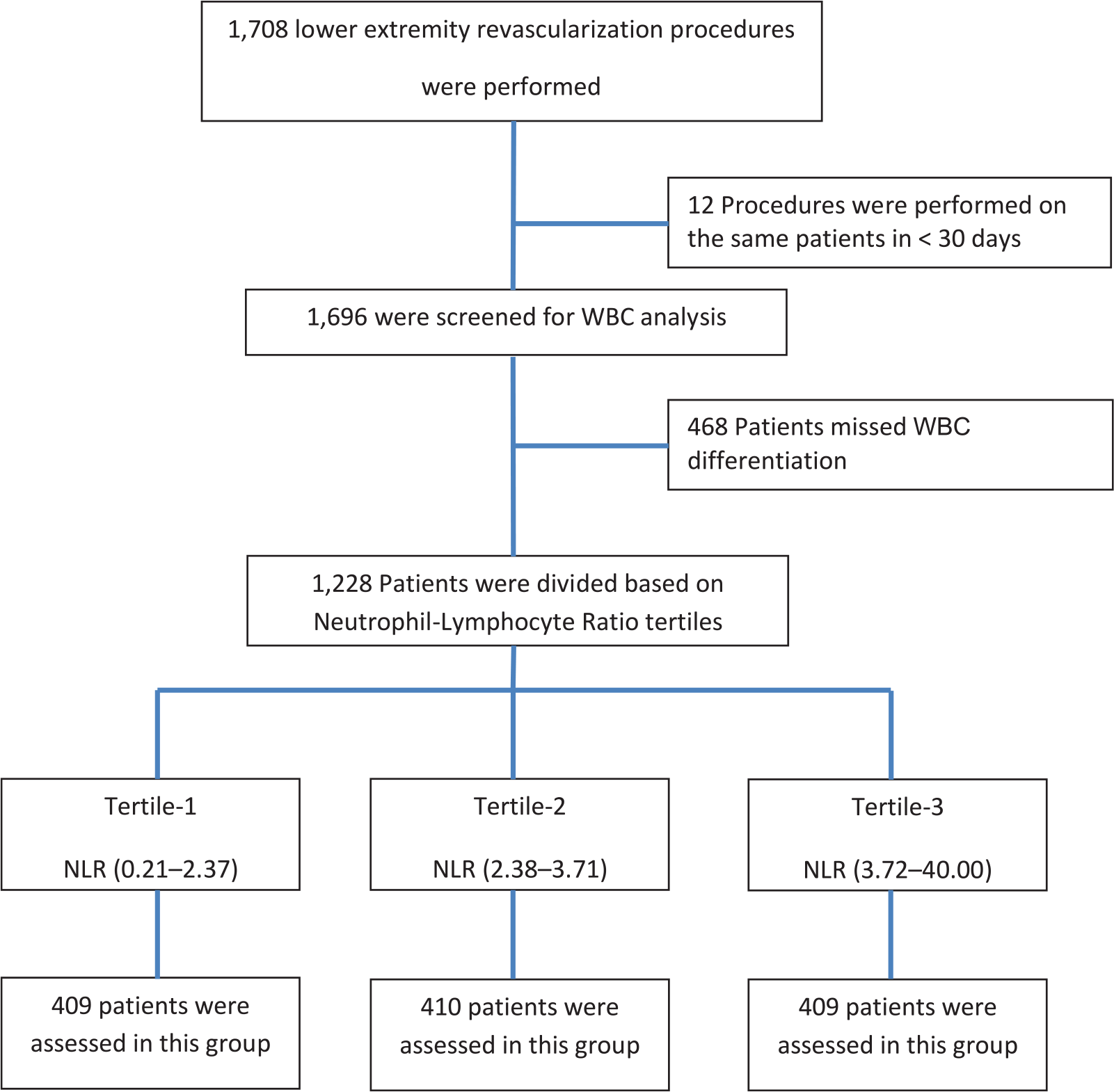
Flow diagram of the study design.
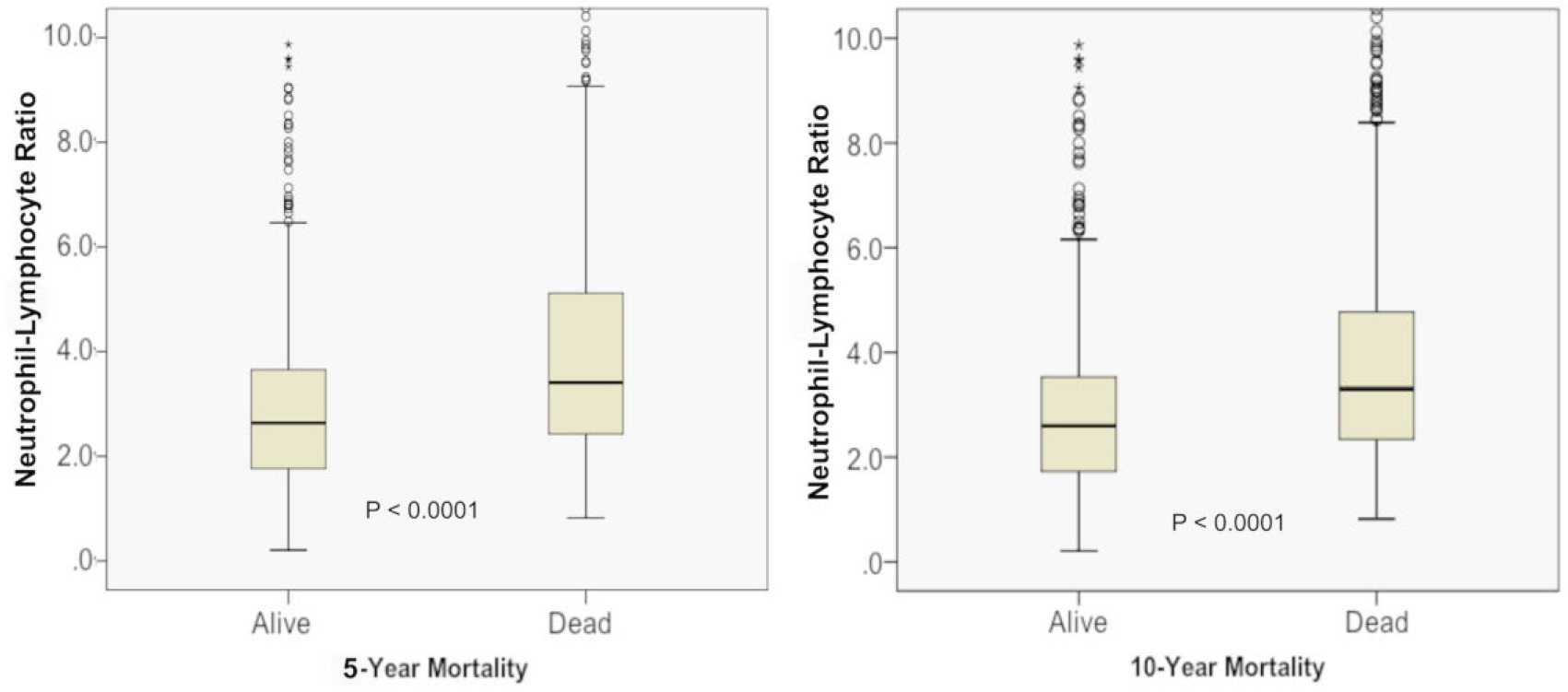
The NLR in between the survivors and no survivors after 5 years (left panel) and 10 years (right panel). The p-values for the comparison are shown in each graph (* indicates statistical significance)..
The frequency of hypertension, diabetes, coronary artery disease, history of prior coronary revascularization, congestive heart failure, cerebrovascular diseases and chronic kidney diseases were higher among both the MALE and the MACE groups. In patients who were presented with critical limb ischemia as opposed to those presented with intermittent claudication, MACE and MALE were significantly higher (p < 0.001 for all three events). Critical limb ischemia was also associated with lower patency rates and limb salvage compared to the claudication group (p < 0.001). The frequency of hypertension, chronic obstructive pulmonary diseases and chronic kidney diseases were significantly higher in the primary patency group. The use of statins and clopidogrel were significantly associated with lower MACE and MALE. The use of acetylsalicylic acid was significantly associated with lower MACE and MALE as well as a higher primary patency rate (Table 1).
Cross-tabulation of the patient demographic, comorbidities, and relevant clinical information to observed adverse outcome.
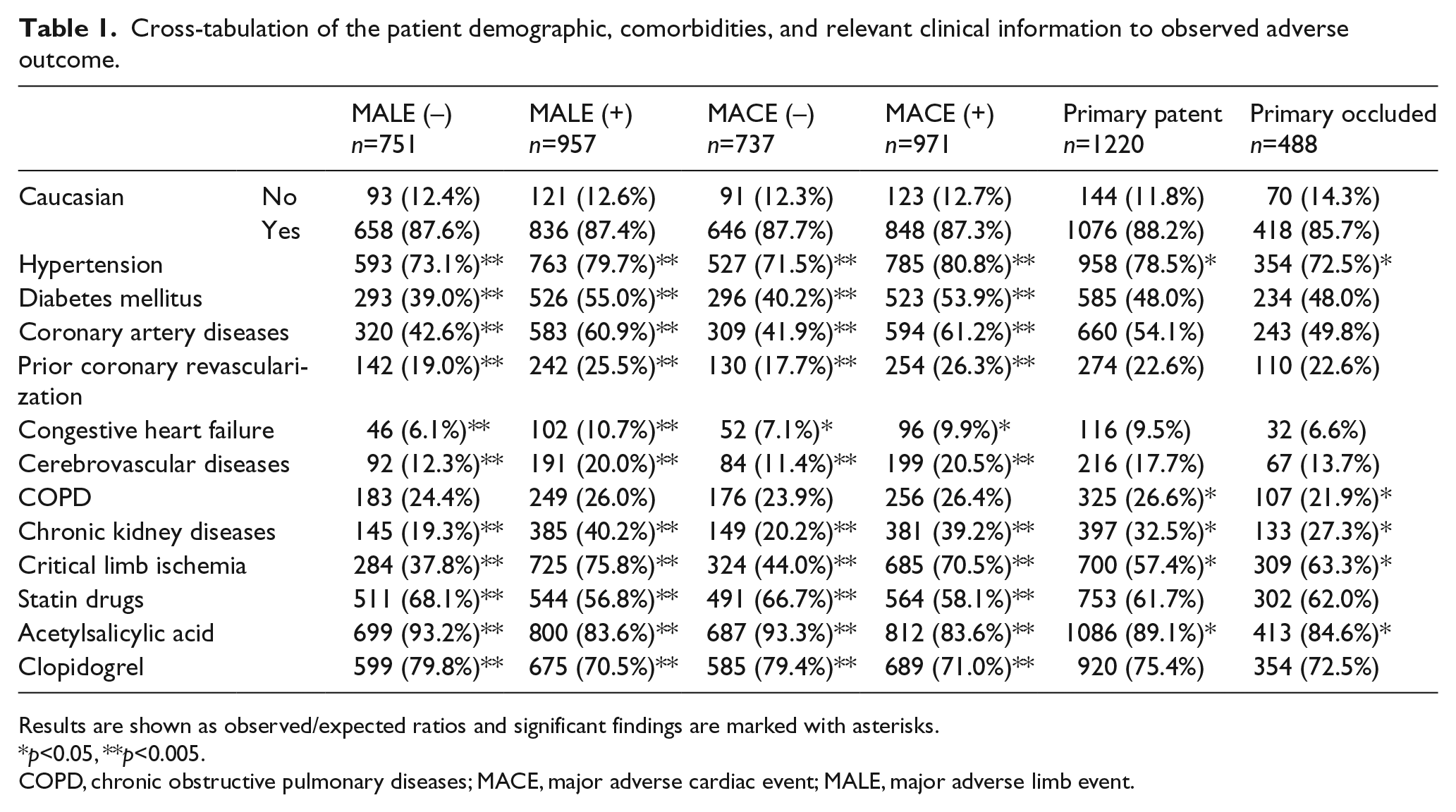
Results are shown as observed/expected ratios and significant findings are marked with asterisks.
p<0.05, **p<0.005.
COPD, chronic obstructive pulmonary diseases; MACE, major adverse cardiac event; MALE, major adverse limb event.
Patients were grouped into three according to their NLR tertile rank, with 409, 410 and 409 patients in tertiles 1 through 3. There was a significant racial distribution of Caucasians between tertiles 1 and 2. Patients in the third NLR tertile tended to be older with a higher frequency of hypertension, diabetes mellitus, coronary artery disease, prior coronary revascularization, chronic kidney disease, congestive heart failure and cerebrovascular disease. In addition, they were more likely to be classified as American Society of Anesthesiologists (ASA) class IV or V compared to patients in tertiles 1 and 2 (Table 2). Patient characteristics and comorbidities in the non-included patient group are presented in Supplementary Table 1.
Patient characteristics and preoperative comorbid diseases based on tertile assignment of the NLR.
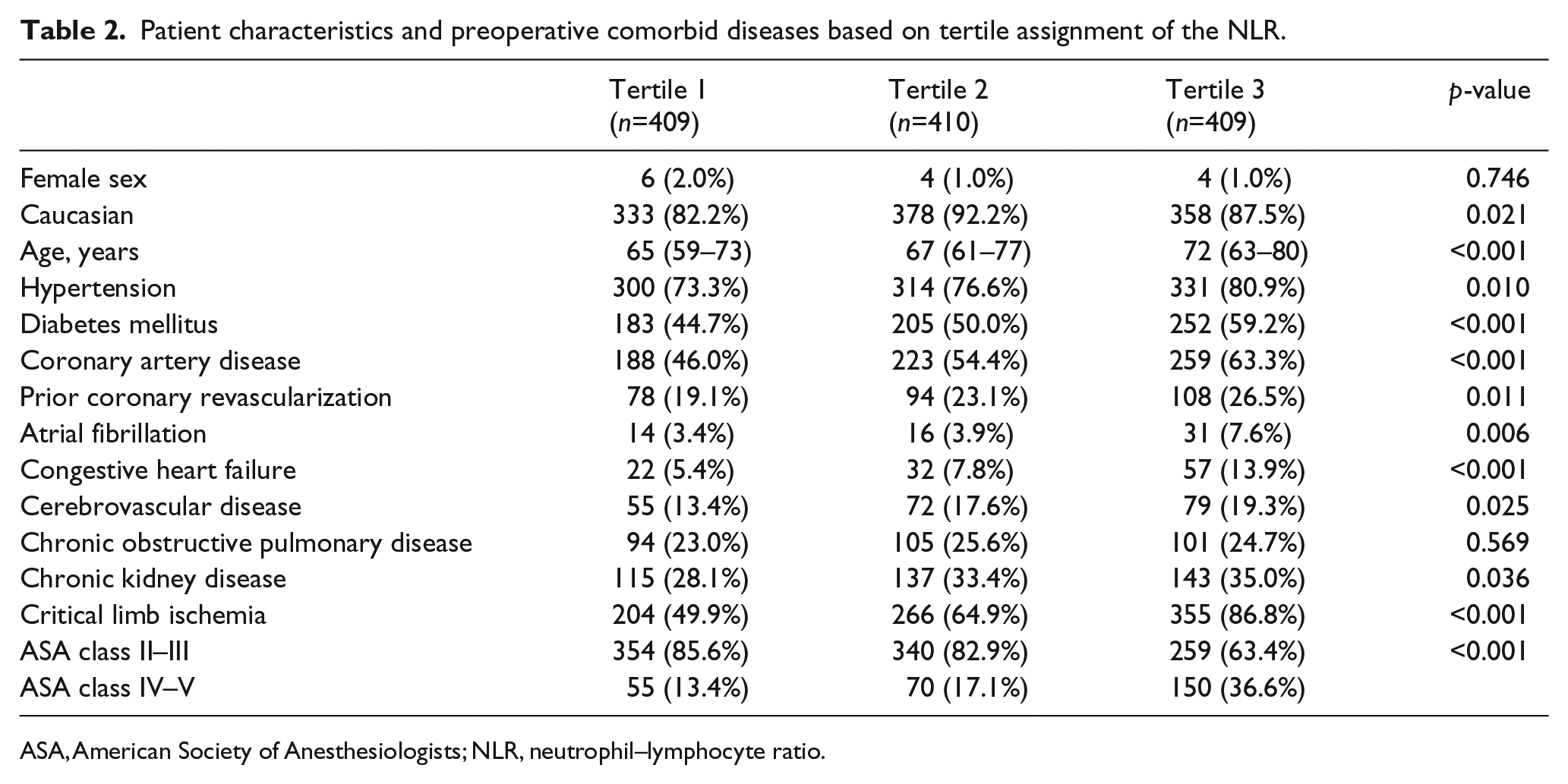
ASA, American Society of Anesthesiologists; NLR, neutrophil–lymphocyte ratio.
Fewer patients in the third NLR tertile survived over the follow-up period compared to those in tertiles 1 and 2 (p<0.0001). The hazard risk of 10-year mortality was 1.30 with a 95% CI of 1.23–1.39, meaning that for every tertile increase in NLR value the risk of dying increases by 30% per year (Figure 3, left panel). Similarly, the hazard risk of MALE was 1.34 with a 95% CI of 1.26–1.43, meaning that the risk of MALE is increased by 34% per year from one tertile to the next (Figure 3, right panel).
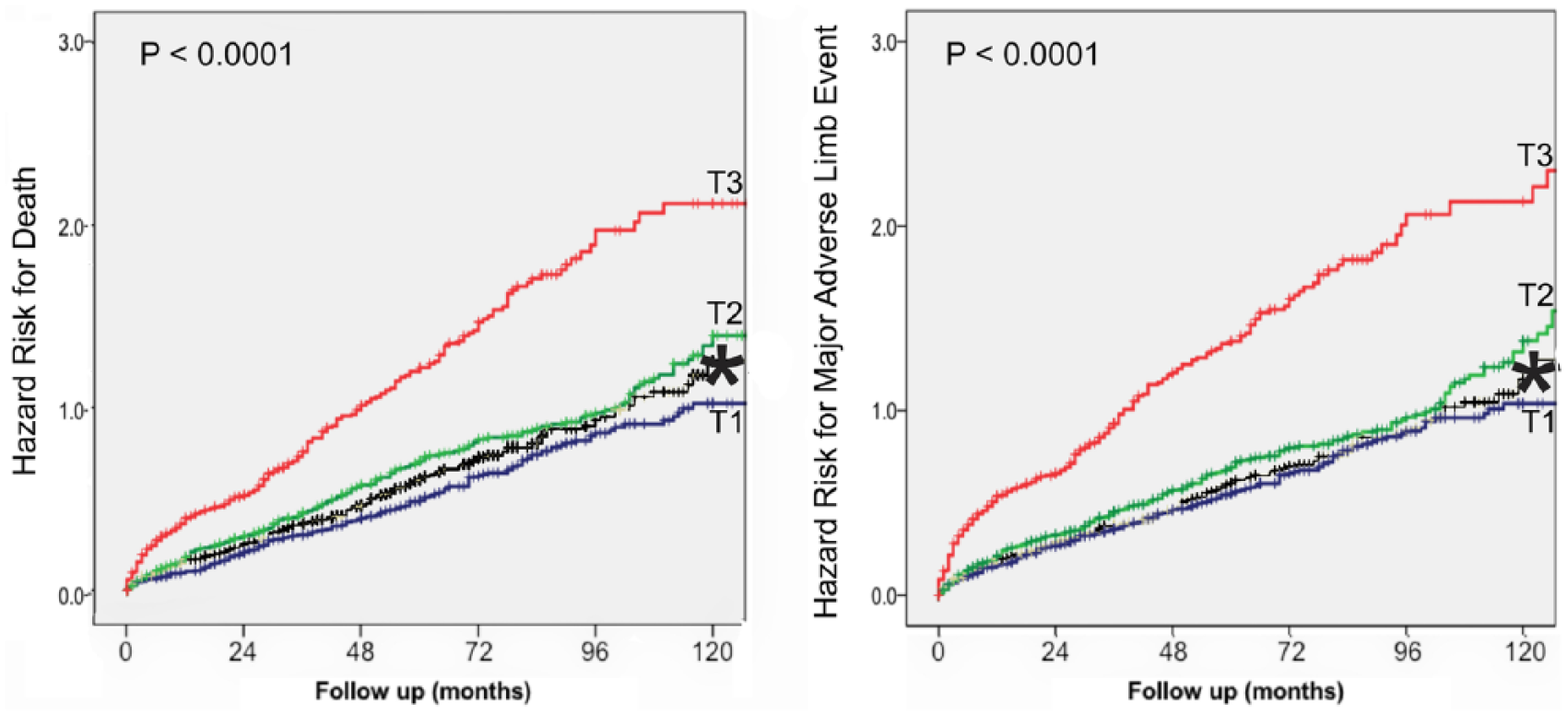
Hazard ratio for 10-year mortality (left panel) and for major adverse limb events (right panel) are shown using the Cox multivariate regression model for the three tertiles of the NLR and non-included cases.
In multivariate Cox regression analysis for prediction of MALE, the NLR was independently associated with MALE (hazard ratio (HR): 1.094, 95% CI: 1.071–1.118, p<0.001) (Table 3). The AUC for this model for prediction of MALE was 0.785 ± 0.014. Similarly, by including all influential variables (from Table 2) in the multivariate Cox regression model, the NLR was still an independent predictor of 10-year mortality (HR: 1.096, 95% CI: 1.072–1.120, p<0.001) (Table 4). Again, the AUC for this multivariable model in predicting 10-year mortality was 0.791 ± 0.014.
Multivariate Cox regression model for MALE.
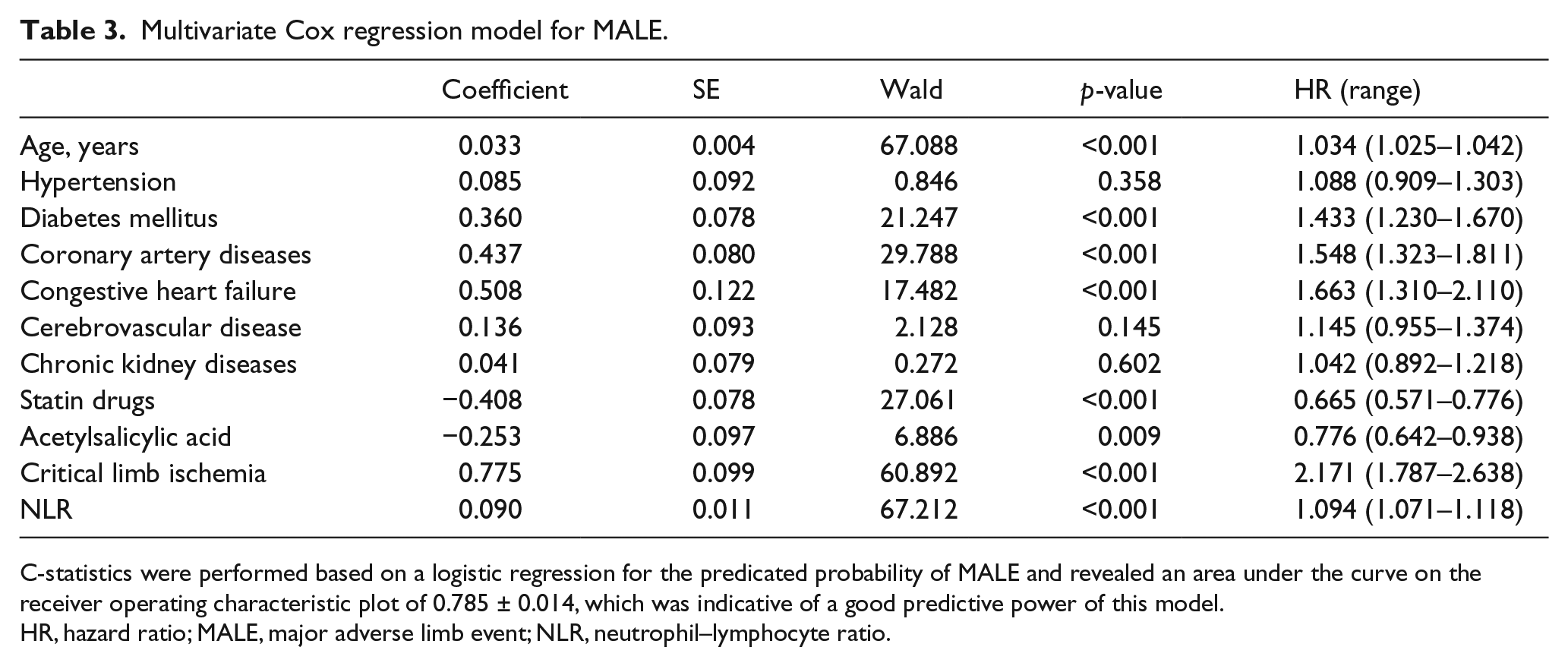
C-statistics were performed based on a logistic regression for the predicated probability of MALE and revealed an area under the curve on the receiver operating characteristic plot of 0.785 ± 0.014, which was indicative of a good predictive power of this model.
HR, hazard ratio; MALE, major adverse limb event; NLR, neutrophil–lymphocyte ratio.
Multivariate Cox regression model for overall all-cause 10-year mortality.
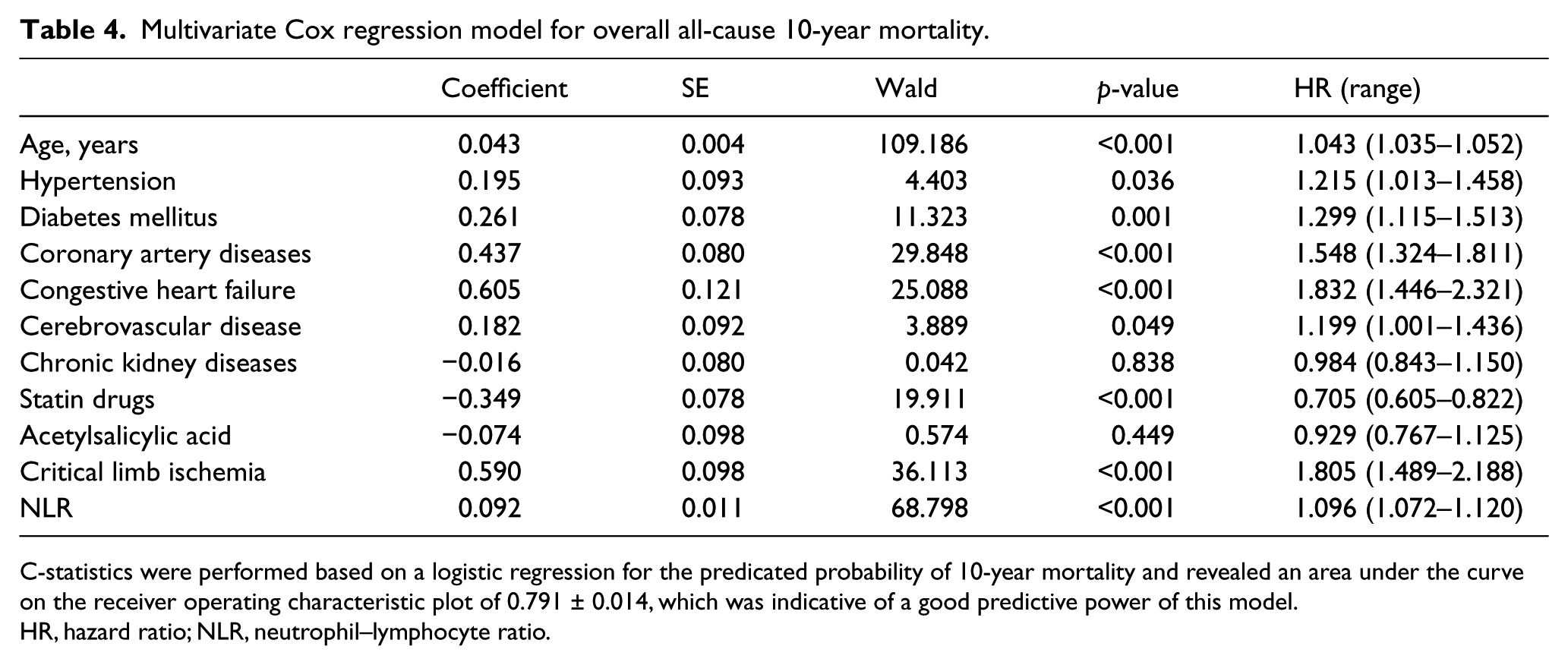
C-statistics were performed based on a logistic regression for the predicated probability of 10-year mortality and revealed an area under the curve on the receiver operating characteristic plot of 0.791 ± 0.014, which was indicative of a good predictive power of this model.
HR, hazard ratio; NLR, neutrophil–lymphocyte ratio.
The cut-off value for the NLR for prediction of MALE was 2.91 using ROC with an AUC of 0.634 ± 0.012, which indicated a moderate predictive value of the NLR for MALE. This cut-off had a sensitivity of 82% and only 60% specificity, with a higher probability for false positive reports. Similarly, the cut-off value for the NLR, which was predictive of 10-year mortality, was 2.82 using ROC. The AUC of 0.644 ± 0.017 indicated a moderate predictive value for this marker (Figure 4). This cut-off had 81% sensitivity and 61% specificity, with a higher probability for false negative and positive reports.
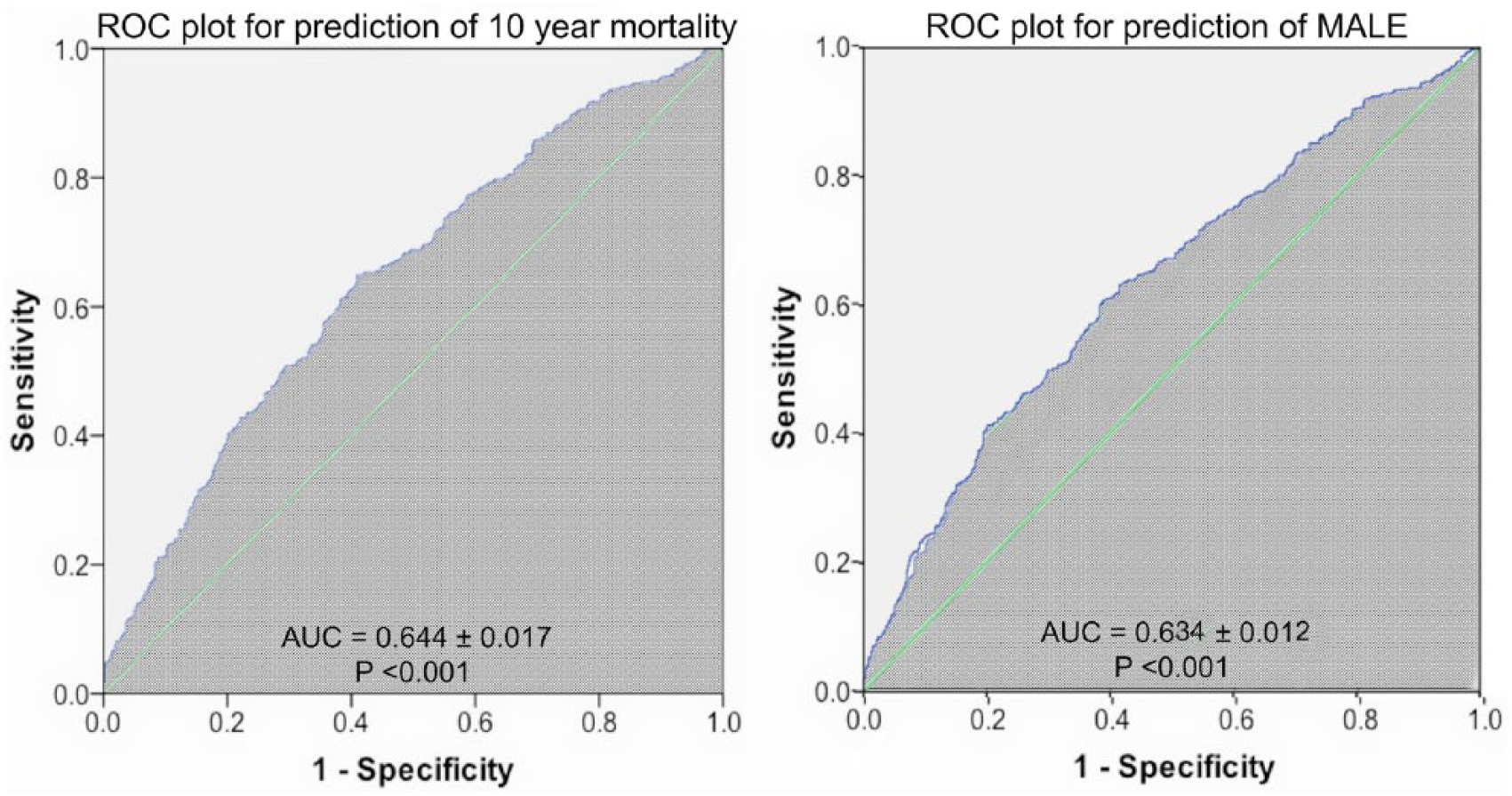
ROC plot for the NLR. The AUC is shaded and its numeric value is depicted.
Discussion
According to these results, increased levels of the NLR during the peri-operative period translated to a higher rate of MALE occurrence in affected limbs following revascularization. In addition, having a higher NLR before a procedure was indicative of higher 5-year and 10-year mortality rates in patients who underwent revascularization of the lower extremities.
Increasing clinical evidence indicates that inflammatory burden correlates with coronary risk factors and vascular diseases.23–25 Inflammation plays a major role in initiation and progression of PAD disease processes.26,27 Despite the fact that revascularization procedures are increasingly being used for the treatment of patients with critical limb ischemia and intermittent claudication,7,9,28 not many studies have been performed to investigate the role of peri-procedural inflammatory status in the long-term patency rate and future complications. The severity of artery stenosis, type of lesion, site of stenosis, type of graft, and location of distal anastomosis in operative procedures are among the predictors of patency rate after peripheral revascularization.7,14,29 While C-reactive protein (CRP), an acute phase reactant of inflammation, is shown to predict restenosis after percutaneous transluminal angioplasty of the femoropopliteal artery, 30 in another study, elevated baseline levels of CRP and fibrinogen were associated with graft patency only in women but not in men. 31 In our study, we sought to determine the possible role of the NLR in the occurrence of MALE after revascularization in a large cohort of patients with PAD and found an increased NLR is an independent predictor of MALE. In a study by Kullar et al., in which they have included 126 consecutive patients undergoing infra-inguinal bypass grafting, there was no significant association between the preoperative NLR and graft patency at 1 year. However, the postoperative NLR was an independent predictor of graft patency in their study. 20 Similarly, in a paper published by Chan et al., the NLR was not a predictor of 1-year patency in 83 patients who had undergone infra-popliteal percutaneous interventions for critical limb ischemia. 32 Although patients with critical limb ischemia on presentation were more likely to develop MALE in our study sample, the NLR remained a significant predictor of MALE with adjustment for this factor in multivariate analysis.
According to our findings, an increased peri-procedural NLR is an independent but modest predictor of 10-year all-cause mortality in patients with PAD who undergo revascularization procedures. This finding confirms the results of the recent study published by Amrock et al., in which they analyzed data from 556 individuals with PAD and found the NLR to be an independent predictor of all-cause mortality. 33 In addition, Chen et al. evaluated 148 PAD patients with concomitant advanced chronic kidney disease who received percutaneous transluminal angioplasty, and described the elevated NLR as a predictor of intermediate-term all-cause mortality. 16 Similarly, Chan et al. identified the NLR as a predictor of all-cause mortality in 83 PAD patients who received infra-popliteal percutaneous interventions for critical limb ischemia. 32 Likewise, Erturk et al., in a study of 593 patients with a diagnosis of symptomatic PAD and a median follow-up period of 20 months, found the NLR to be an independent predictor of long-term cardiovascular mortality. 18 Our results are consistent with the findings of the previous reports regarding the role of the NLR in the long-term mortality of PAD; however, the previous reports included smaller numbers of patients and we confirmed these results in a larger sample of PAD patients.
The increased long-term mortality of PAD patients in a higher NLR group may partly be related to the complexity of atherosclerotic plaque in this group of patients. 34 Furthermore, in patients with PAD, CAD is common and is one of the major causes of death. 7 Herein, we also describe that patients in a higher NLR tertile group are older and have a higher prevalence of hypertension, diabetes mellitus, coronary artery disease and congestive heart failure. On the other hand, the NLR is also reported as an independent predictor of mortality in patients with CAD. 35 However, the association of NLR with long-term mortality remained significant even after adjustment for all these factors in multivariate analysis.
The exact underlying causes of imbalance between the number of neutrophils and lymphocytes in the peripheral blood of PAD patients are not known. However, a higher ratio is clearly an indicator of acute inflammatory response that causes a myeloproliferative response by acute changes in the number of circulating neutrophils. Higher levels of NLR also may be produced by reduced levels of circulating lymphocytes rather than increased levels of neutrophils. Decreases in peripheral lymphocytes are believed to be a consequence of generalized stress response and the resultant increase is systemic cortisol levels. In addition to the NLR, different inflammatory markers are also described as risk factors of higher mortality in PAD. 33
Limitations
One of the limitations of our study was that we measured the NLR only once and did not have the information about the temporal changes of this index. Since the nature of our study is descriptive, it is not feasible to determine the underlying pathogenesis by which the imbalance of neutrophils and lymphocytes occur. Basic science studies are warranted to better understand the mechanism by which neutrophils and lymphocytes affect the prognosis of patients with PAD. Of note, there were very few female patients in our study sample. As a result, the findings of this study may not be applicable to the female patient population.
Conclusions
Our results demonstrated that a higher NLR in patients with PAD who undergo revascularization procedures was associated with a higher rate of MALE as well as 10-year mortality. Although patients in the higher NLR group were older with a higher burden of comorbidities, this association remained significant in multivariate analysis. Inclusion of the NLR in multivariable predictive models of both MALE and 10-year mortality improves its predictive power significantly as it is only a modest predictor of these events by itself. The NLR as an inexpensive, overly simple and widely available index may be useful for predicting a future MALE and the long-term mortality of these patients.
Supplemental Material
10.1177_1358863X18774623_supplemental_material – Supplemental material for Neutrophil–lymphocyte ratio is a marker of survival and cardiac complications rather than patency following revascularization of lower extremities
Supplemental material, 10.1177_1358863X18774623_supplemental_material for Neutrophil–lymphocyte ratio is a marker of survival and cardiac complications rather than patency following revascularization of lower extremities by Leili Pourafkari, Catherine Choi, Reza Garajehdaghi, Arezou Tajlil, Hasan H Dosluoglu and Nader D Nader in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Veterans Affairs Western New York Healthcare System in Buffalo, New York (VHA 1020889). The opinions expressed herein do not necessarily represent those of the Veterans Administration or the US Government.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.