
Abstract
Variation in the use of inferior vena cava filters (IVCFs) across hospitals has been observed, suggesting differences in quality of care. Hospitalization metrics associated with venous thromboembolism (VTE) patients have not been compared based on IVCF utilization rates using a national sample. We conducted a descriptive retrospective study using the Nationwide Readmissions Database (NRD) to delineate the variability of hospitalization metrics across the hospital quartiles of IVCF utilization for VTE patients. The NRD included all-payer administrative inpatient records drawn from 22 states. Adult (≥ 18 years) patients with VTE hospitalizations with or without IVCF were identified from January 1, 2013 through December 31, 2014 and hospitals were divided into quartiles based on the IVCF utilization rate as a proportion of VTE patients. Primary outcome measures were observed rates of in-hospital mortality, 30-day all-cause readmissions and VTE-related readmissions, cost, and length of stay. Patient case-mix characteristics and hospital-level factors by hospital quartiles of IVCF utilization rates, were compared. Overall, 12.29% of VTE patients had IVCF placement, with IVCF utilization ranging from 0% to 46.84%. The highest quartile had fewer pulmonary embolism patients relative to deep vein thrombosis patients, and older patient ages were present in higher quartiles. The highest quartile of hospitals placing IVCFs were more often private, for-profit, and non-teaching. Patient and hospital characteristics and hospitalization metrics varied by IVCF utilization rates, but hospitalization outcomes for non-IVCF patients varied most between quartiles. Future work investigating the implications of IVCF utilization rates as a measure of quality of care for VTE patients is needed.
Introduction
The clinical use of inferior vena cava filters (IVCFs) is supported by several societal guidelines for patients contraindicated to anticoagulation for the prevention of pulmonary embolism (PE) or for patients at high risk of venous thromboembolism (VTE). These guidelines are issued from multiple societies including interventional radiology, cardiology, and trauma.1–4 IVCF use has increased to roughly 10% of all VTE patients, 5 with the most recent estimates ranging from 12% to 17% of VTE patients. 6 Variation in utilization of IVCFs between institutions has been observed and is subject to some controversy regarding the appropriateness of implantation.7–10
Explanations for the observed variation in IVCF utilization rates between institutions have been previously evaluated. A study using the Nationwide Inpatient Sample Database between 2006 and 2008 explored patient-level characteristics such as comorbidities as well as hospital-level characteristics such as teaching status and hospital size. This study found no statistically significant relationships between IVCF placements in VTE patients and patient-level characteristics (e.g. cancer diagnoses), nor with hospital characteristics. 11 However, a more recent study of VTE patients found substantial variation in IVCF utilization among California hospitals in 2013. Much of the observed variation in IVCF utilization in this study was attributed to hospital characteristics such as hospital bed size, urban or rural location, hospital profit or non-profit status, and several patient-level characteristics such as acute bleeding at admission and metastatic cancer. 9
A 2016 study of VTE patients in Kentucky hospitals found that patient case-mix was a strong predictor of variation in IVCF utilization. 8 A follow-up study employing regression analysis to control for both patient and hospital-level characteristics among the population of Kentucky VTE patients found that patients with higher risk (e.g. older patients, having multiple comorbidities, metastatic tumors) were more likely to receive IVCFs. 7 In that analysis, between-hospital variation in IVCF utilization was approximately 7% after controlling for patient and hospital-level characteristics.
These prior studies were restricted to populations within single states. This study fills a gap in the literature by examining observed hospital-level variation in IVCF utilization from a nationally representative database and compares hospitals on patient factors, hospital characteristics, and hospitalization metrics. The primary aim was to assess if quality of care (i.e. hospitalization metrics) differed for VTE patients with or without IVCFs based on the hospitals’ overall IVCF utilization rate.
Methods
Data source
This retrospective cohort study used the Nationwide Readmission Database (NRD) (January 2013 through December 2014) from the Agency for Healthcare Research and Quality (AHRQ). The NRD is an all-payer administrative inpatient database in the United States, with records drawn from 21 State Inpatient Databases (SIDs) in 2013 and 22 states in 2014. 12 All patient discharge records from participating states are included in the NRD. Unique patient linkage numbers enable follow-up within each calendar year. This study was waived from formal review and informed consent by the institutional review board of University of Florida because NRD data are publicly available and de-identified. Use of the NRD follows regulations within the data use agreement as defined by the AHRQ.
Study population
VTE patients were identified by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnoses codes, with a primary diagnosis of PE (ICD-9, 415.1x) or deep vein thrombosis (DVT) (ICD-9, 451.xx and 453.xx).9,13,14 Patients aged 18 years or older at the time of index hospitalization were included, where the index hospitalization was defined as the first hospitalization of VTE as the primary diagnosis during the study period. Elective or planned hospitalizations were excluded. IVCFs were identified by ICD-9-CM procedure code 38.7.9,13
Patient case-mix and hospital-level characteristics
Patient characteristics included sex, age, race, anatomical location of DVT, insurance status, median income of zip code, urban/rural residence, weekend admission, and number of chronic conditions. Case-mix comorbidities included 28 AHRQ comorbidities, and hyperlipidemia, chronic obstructive pulmonary disease (COPD), sepsis, infection, trauma, bleeding, stroke, thrombolysis, embolectomy, and ventilator use. 15 Hospital characteristics included teaching status, urban/rural location, number of beds, and ownership.
Measures
Hospitals were stratified into quartiles of IVCF utilization rates, calculated as the percentage of VTE patients receiving a IVCF within each calendar year. Primary outcome measures were rates of in-hospital mortality, rates of 30-day all-cause, and 30-day VTE-specific unplanned readmissions by IVCF utilization quartile. Secondary measures were in-hospital cost and length of stay. In-hospital costs were calculated by multiplying the total charges with the cost-to-charge ratio and adjustment for the annual inflation rates from the US Consumer Price Index to 2016 dollars. 16
Statistical analysis
The distribution of VTE patients, IVCF placement, and hospital-specific IVCF rates by quartile were described. The percentage of VTE patients with PE, patient case-mix, and hospital-level factors were reported as percentages within each quartile. Cochran–Armitage trend tests were used to analyze the rates of IVCF utilization, in-hospital mortality, and 30-day readmission across the quartiles. ANOVA tests were used to assess the mean difference of the continuous variables (e.g. cost and length of stay). Hospitalization metrics were divided overall and by patients with and without IVCFs. All analyses were performed using SAS version 9.4 and JMP 13 Pro (SAS Institute, Cary, NC, USA). All tests were two-tailed. Statistical significance was assessed at p-value < 0.05.
Results
Overall, 207,246 VTE patients were identified, with 25,470 (12.29%) undergoing IVCF placement across 1614 hospitals (Table 1). Table 1 provides detail on the frequency of IVCF utilization, which ranged from 0–7.28% (median: 4.95%, interquartile range (IQR): 3.33–6.19%) in the lowest hospital quartile (Q1), 7.29–10.97% (median: 9.14%, IQR: 8.14–10.09%) in the second quartile (Q2), 10.98–15.83% (median: 13.04%, IQR: 12.05–14.19%) in the third quartile (Q3), and 15.84–46.84% (median: 19.35%, IQR: 17.48–22.22%) in the highest quartile (Q4) of hospital-specific IVCF rates. PE represented a greater proportion, relative to DVT, of VTE patients among the lowest IVCF utilization quartile (Table 1).
IVCF utilization stratified by quartiles of utilization rates among patients with VTE.
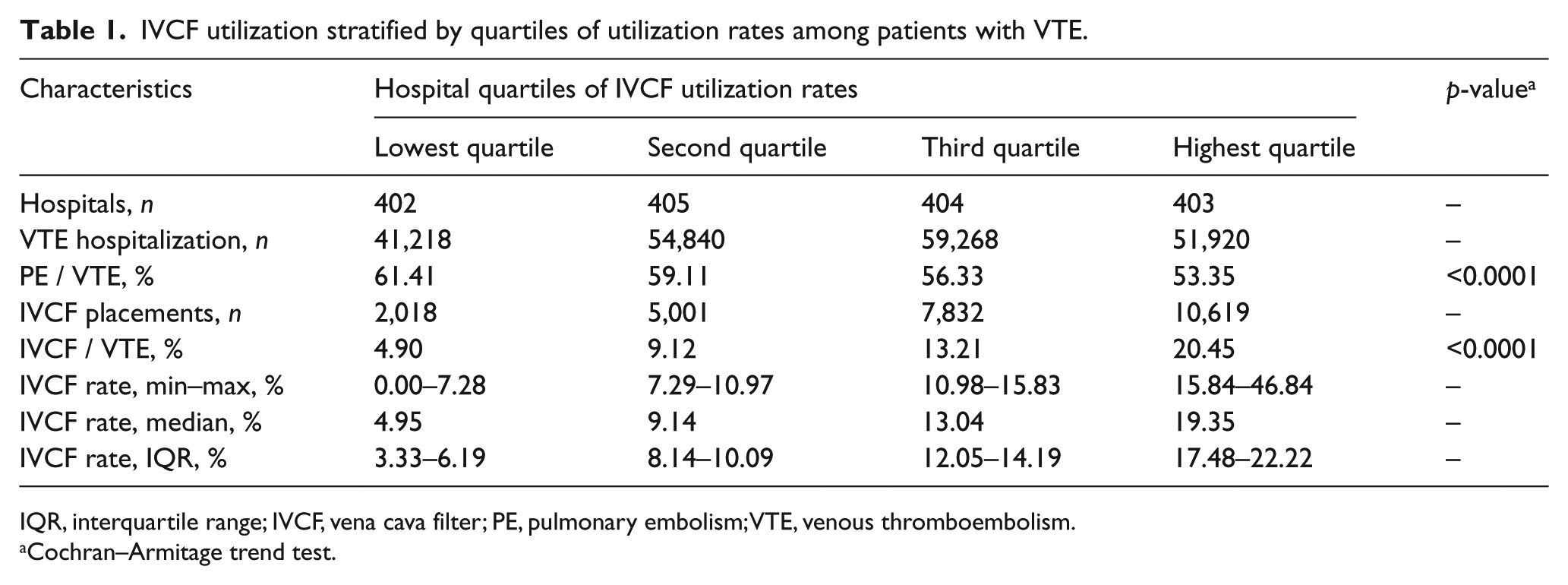
IQR, interquartile range; IVCF, vena cava filter; PE, pulmonary embolism; VTE, venous thromboembolism.
Cochran–Armitage trend test.
Utilization quartiles differed on all measured hospital characteristics though not all associations were consistent (e.g. teaching status was highest with Q2/Q3 and similar between Q1/Q4) (Table 2). Hospitals with larger numbers of beds were generally associated with higher quartiles, with Q3 having the highest proportion and Q1 the lowest of large hospital (by bed size) classifications. Q4 had the highest number of private and/or for-profit institutions. A greater proportion of IVCF placements occurred in hospitals with a lower proportion of PE patients, with Q4 having 53.35% of PE cases relative to 61.41% in Q1. Higher utilization rates were also associated with large metropolitan hospitals (i.e. hospitals in cities with > 1 million residents).
Comparison of hospital characteristics by IVCF utilization quartile in hospitalized patients with VTE.
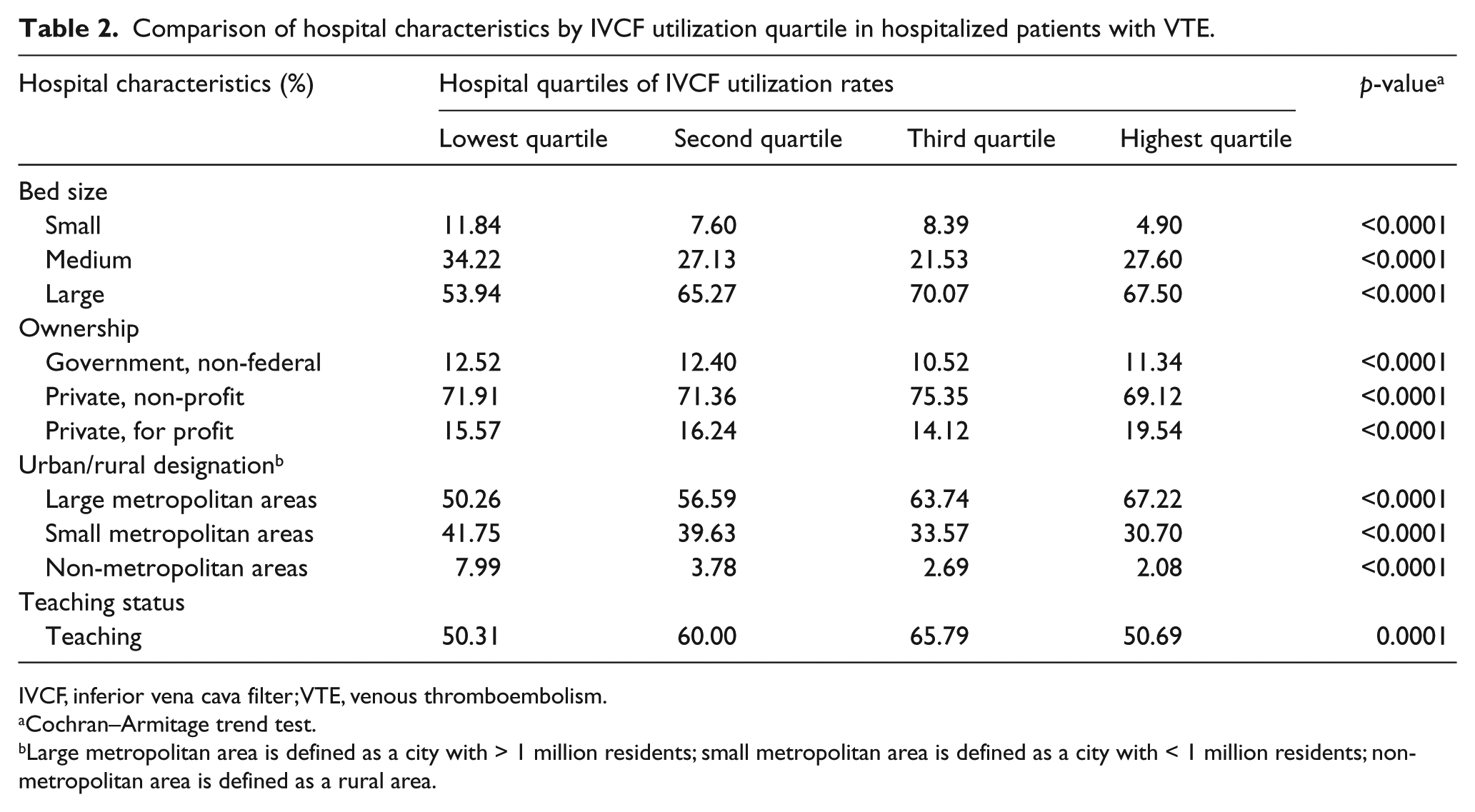
IVCF, inferior vena cava filter; VTE, venous thromboembolism.
Cochran–Armitage trend test.
Large metropolitan area is defined as a city with > 1 million residents; small metropolitan area is defined as a city with < 1 million residents; non-metropolitan area is defined as a rural area.
Among VTE patients with IVCFs placed, lengths of stay and costs generally decreased by increasing quartile (Table 3). Among the same group, mortality was inversely associated with increasing utilization quartile. The 30-day all-cause and VTE readmissions and their associated lengths of stay and costs were not significantly different within the IVCF group. Nearly all measures were significantly different between quartiles for VTE patients without IVCFs. Compared to patients with IVCFs, VTE patients without IVCFs had lower in-hospital mortality, shorter lengths of stay, and lower costs. Risks of readmissions were similar between these groups.
Comparison of hospitalization metrics by IVCF utilization quartile in hospitalized patients with VTE.
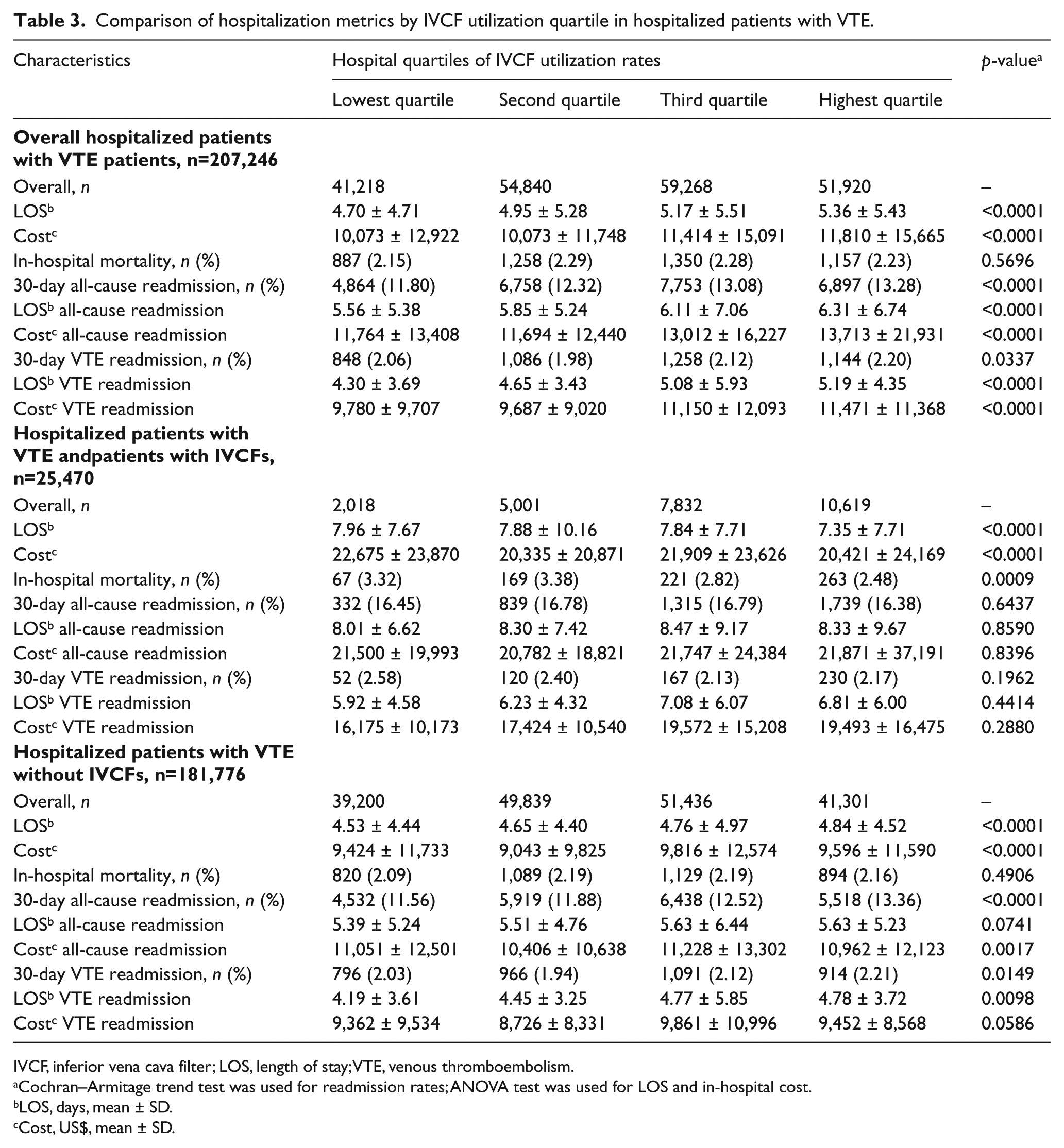
IVCF, inferior vena cava filter; LOS, length of stay; VTE, venous thromboembolism.
Cochran–Armitage trend test was used for readmission rates; ANOVA test was used for LOS and in-hospital cost.
LOS, days, mean ± SD.
Cost, US$, mean ± SD.
Patient characteristics stratified by utilization quartile are compared in Table 4. Higher proportions of patients with proximal, lower extremity DVT were significantly associated with higher utilization. There were significant trends of increased IVCF use for VTE patients with older age, higher proportions of patients undergoing thrombolysis and/or embolectomy, and a greater proportion with anemia. Medical comorbidities, such as hypertension, renal failure, and underling malignancy, directly correlated with higher IVCF utilization.
Comparison of IVCF utilization and patient case-mix characteristics by quartile, based on the hospital quartile of IVCF utilization.
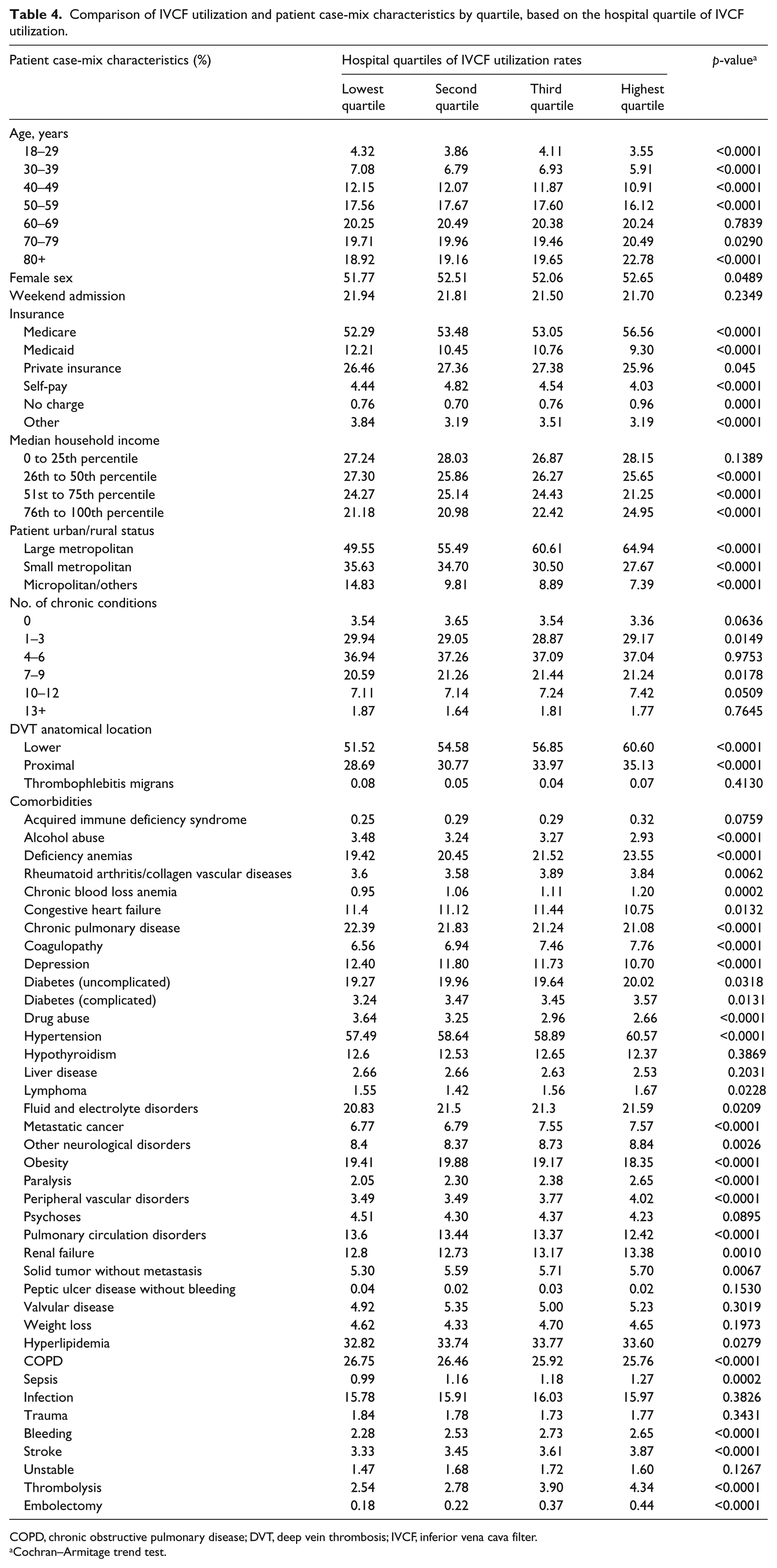
COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis; IVCF, inferior vena cava filter.
Cochran–Armitage trend test.
Discussion
Our results indicated wide variation in the hospitalization metrics across the hospital quartiles of IVCF utilization for VTE patients. IVCF utilization ranged from 0% to nearly 47%, with an overall utilization rate of 12.29% among VTE patients. The overall IVCF utilization rate of 12.29% is comparable to findings from prior studies on hospital variation.7,9,17 There were notable differences in hospital characteristics between quartiles of IVCF utilization rates, particularly when comparing IVCF utilization rates among privately owned hospitals versus government or other publicly owned hospitals. Additionally, higher IVCF utilization was associated with several patient-level factors, such as patient age and comorbidities, consistent with prior studies.7,9
The comparison of hospitalization quality of care metrics among strata of IVCF utilization added new depth to these current and prior findings. Hospitalizations for those receiving IVCFs were generally similar between IVCF utilization quartiles; however, there were some differences observed in lengths of stay, costs, and in-hospital mortality. Interestingly, the differences in quality of care metrics for VTE patients without IVCFs tended to be more pronounced between quartiles than those observed for the VTE patients with IVCF group, suggesting worse outcomes in these patients among hospitals in the highest quartiles. These findings also suggest that variations in care correlated with quartiles of IVCF utilization but do not show this effect in the intended patient group. It is also worth noting that the higher in-hospital mortality observed in the hospitals with the lowest rates of IVCFs may be indicative of hospitals performing the procedure that may not have adequate resources to care for these often complex patients compared to larger hospitals with a variety of specialty care services or trauma centers.
Previous studies have suggested that IVCF utilization rates could serve as a marker for low value or low quality of care.10,18,19 The evidence for IVCFs in VTE patients is mixed. In the PREPIC and PREPIC-2 clinical trials, no significant benefits were observed for IVCFs with anticoagulation versus anticoagulation alone across short and long-term outcomes.20–22 However, it can be argued that a population that can receive anticoagulation is not the intended population. Observational studies have shown improved short-term outcomes including lower in-hospital and 30-day mortality along with reductions in subsequent PE events for certain subgroups (i.e. stable PE patients and unstable elderly PE patients).23–26 Other studies have shown little to no benefit in these outcomes, with longer follow-up, and show a much higher risk of DVTs as well.13,27–29 Sarosiek and colleagues further suggested that the high utilization of IVCFs represents low quality of care, given that placement of IVCFs was a means to up-coding to increase reimbursement for a hospitalization. 18
IVCF utilization as a surrogate for low quality of care may be unjustified given that IVCF patients should, according to clinical guidelines,1–4 represent more severe VTE cases when compared with non-IVCF VTE cases. VTE patients requiring IVCFs tend to be sicker, have a higher prevalence of cancer, a history of or active bleeding, 30 along with a higher burden of medical comorbidities. Quality metrics of mortality, readmissions, costs, and lengths of stay did not differ between quartiles for IVCF patients with VTE – suggesting that there is little variation in care outcomes for IVCF patients between utilization quartiles. However, these metrics were different among non-IVCF patients by quartile. The interpretation of these findings deserves additional research to determine what relationship IVCF utilization has on quality of care for non-IVCF patients.
Limitations
To our knowledge, this study is the first national study to delineate the patient case-mix and hospital-level characteristics associated with IVCF use by hospital quartile among VTE patients. However, several limitations existed. First, NRD data did not contain geographic indicators for states or regions of the hospitalization, which limited the exploration of geographic variation. Second, multivariable analysis was not conducted in this descriptive study to control for patient case-mix and severity, which have been shown to capture most of the variability in IVCF utilization. Further accounting for case-mix through risk adjustment and standardization is needed to compare outcomes and is the subject of further research in our group. Additionally, there were limitations associated with the use of claims data, which typically included risk of conservative classification of diagnoses due to reliance on billing codes. An additional marker of quality of care for IVCF patients would include retrieval for non-permanent devices between hospitals as retrieval rates have been reported to be only 10–40%.18,31-33 However, retrieval is often done on an outpatient basis and would not be observable in inpatient discharge data.
Conclusion
Wide hospital-level variations in the use of IVCFs were found between a national sample of US hospitals, with observed differences in hospitalization outcome metrics for non-IVCF patients across quartiles but not IVCF patients. These findings suggest that high utilization of IVCFs may not be a valid surrogate for low value or low quality of care. Future study is needed to assess the association of IVCF utilization among VTE patients with quality of care within hospitals.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.