
Abstract
This study compares procedural complications and clinical outcomes between subintimal crossing versus intraluminal crossing during endovascular treatment of infrainguinal peripheral artery chronic total occlusions (CTO). We identified 1335 CTO interventions in 1001 patients from the multicenter Excellence in Peripheral Artery Disease (XLPAD) registry from January 2005 to October 2015. Outcomes included 30-day and 12-month all-cause death, non-fatal myocardial infarction or stroke, peripheral artery stent, or vessel, thrombosis (ST), need for any target limb endovascular or surgical revascularization, target limb major amputation and procedural complications. A subintimal crossing technique was necessary in 388 lesions (27% overall in 1335 lesions; 34% (n=351) in 1023 femoropopliteal lesions, and 12% (n=37) in 312 infrapopliteal lesions, p<0.01) with a lower procedural (p<0.01) and technical (p<0.01) success than the intraluminal in both femoropopliteal and infrapopliteal interventions. There were no significant differences in procedural complications, major adverse cardiac events, or clinically driven target limb revascularization at 1 year between the two groups, except a higher residual dissection rate in the subintimal crossing group than the intraluminal group in femoropopliteal target vessels (p = 0.04).
Keywords
Introduction
Chronic total occlusions (CTO) represent a challenging subset of lesions in lower extremity peripheral artery endovascular interventions. CTOs are associated with a higher failure rate during attempted lesion crossing, peripheral artery dissection, perforation or loss of collaterals, and other adverse patient and lesion outcomes. 1 An alternative crossing technique, known as the extraluminal recanalization or subintimal crossing technique, has been developed and successfully employed. 2 The subintimal crossing technique involves the creation of an extraluminal passage between the intimal and medial or adventitial layers of the target artery that bypasses the occluded segment of the vessel. 3 Thus, the intentional subintimal technique involves extending a dissection plane into the subintimal space. It has been used as an effective recanalization method for crossing peripheral artery CTOs. 4 Passage of a guidewire or crossing device into the subintimal space can also be unintentional and requires bail-out techniques to re-enter the distal target vessel true lumen to successfully complete the procedure.
While prior studies have examined patency rates and complications for each crossing technique separately, 5 few have conducted a comparative study of patient outcomes following lower extremity peripheral artery endovascular intervention between intraluminal and subintimal crossing techniques to recanalize infrainguinal peripheral artery CTOs. This study compares patient, lesion, and procedural characteristics, along with 30-day and 12-month clinical outcomes, as well as periprocedural complications between the intraluminal and subintimal crossing techniques for femoropopliteal and infrapopliteal peripheral artery CTOs, using retrospective data from the multicenter Excellence in Peripheral Artery Disease (XLPAD) registry (NCT01904851).
Methods
Data from the XLPAD registry catalogues procedural information and outcomes of consecutive infrainguinal peripheral artery interventions performed at 11 centers in the United States between January 2005 and October 2015. Details of this ongoing registry have been previously published. 6 All procedural images are adjudicated by the Veterans Affairs North Texas angiographic and ultrasound core laboratory. Baseline features, demographics, laboratory values, medical therapy and procedure data, and patient outcomes are recorded in the registry.
Patients were categorized into two groups based on the techniques utilized to cross infrainguinal peripheral artery CTO lesions: intraluminal (true lumen) and subintimal groups. Assignment to a crossing strategy was based on operator description indicated in the registry data capture form. However, final assignment of a case to a crossing strategy was based on the following criteria: (a) subintimal crossing: defined based on either use of a re-entry device, specific operator description of distal true lumen re-entry with a guidewire, or extraluminal passage of a guidewire confirmed by intravascular ultrasound (IVUS) imaging performed at the discretion of the operator; (b) intraluminal crossing: in the absence of any of the above criteria defining subintimal crossing, the procedure was assigned to the intraluminal group.
Technical success was defined as crossing the CTO and placement of a guidewire or crossing device in the distal true lumen confirmed by either angiography or IVUS. Procedural success was defined as successful treatment of the CTO lesion with ⩽30% angiographic residual stenosis without complications. The crossing technique employed was at the discretion of the operator.
Patient outcomes included patient adverse events at 30 days and 12 months post-procedure and include: all-cause death, non-fatal myocardial infarction (MI) or stroke, peripheral artery stent, or vessel, thrombosis (ST), the need for any target limb endovascular or surgical revascularization, and target limb major amputation. Periprocedural complications included residual dissection, access-site or retroperitoneal hematoma, bleeding diathesis, distal embolization, perforation, or the need for emergency surgery. Peripheral artery ST, complications, and adverse events are defined based on the established XLPAD registry criteria. 6
Analyses were conducted separately by target vessel, femoropopliteal and infrapopliteal artery locations treated during the endovascular intervention.
Descriptive statistics are reported and Cochran-Mantel-Haenszel (CMH) statistics were used for overall association of crossing techniques with categorical baseline patient and lesion characteristics and outcomes. |Standard residual| >3 was set as a criterion for a true association for baseline characteristics with more than two categories. Two-sided t-tests were conducted to examine a crossing technique group difference in continuous baseline characteristics. Kaplan-Meier curves were used to conduct time to event analysis and log-rank chi-squared statistics w used to compare a median time of event between intraluminal and subintimal CTO crossing technique groups. A p-value <0.05 was set for statistical significance. SAS software, Version 9.4 (SAS Institute Inc., Cary, NC, USA) was used for all statistical analyses.
Results
This study identified 1335 CTO lesions from 1179 procedures to examine crossing technique associations with procedural success and patient outcomes in 1001 unique patients. An intraluminal crossing technique was used in 71% (n=947) of CTO lesions and the remaining were crossed using a subintimal technique (n=388, Figure 1). Within the subintimal crossing group, approximately 20% used IVUS and 80% (n=314) used a re-entry device. About 17% of the subintimal crossings (n=68) were for a bail-out indication (n=63 in femoropopliteal and n=5 in infrapopliteal locations). Patient baseline characteristics are described in Table 1.
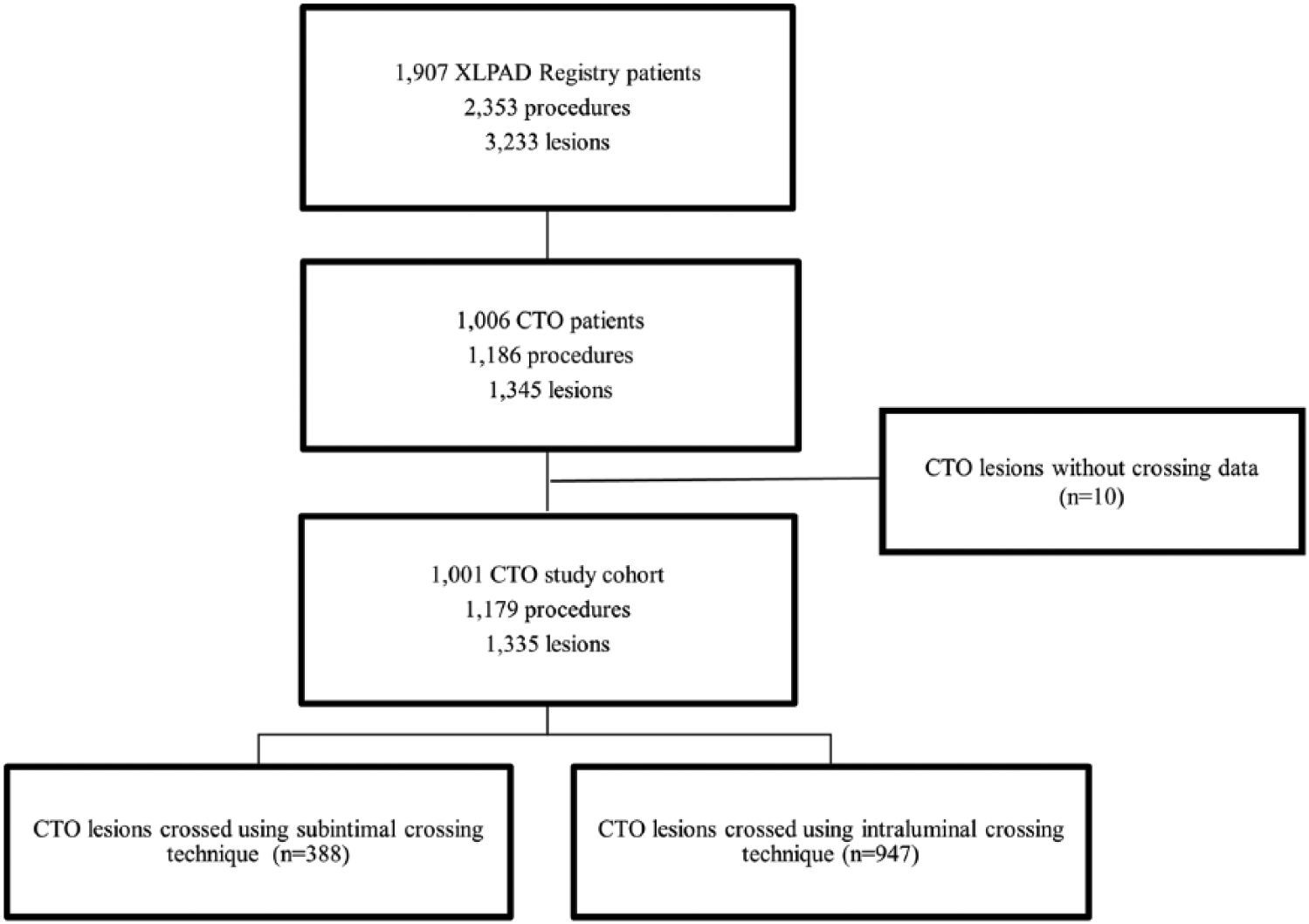
A flow chart of the study data selection: chronic total occlusion (CTO) lesion and crossing technique.
Baseline patient and lesion characteristics by chronic total occlusion (CTO) crossing technique groups (intraluminal versus subintimal groups).
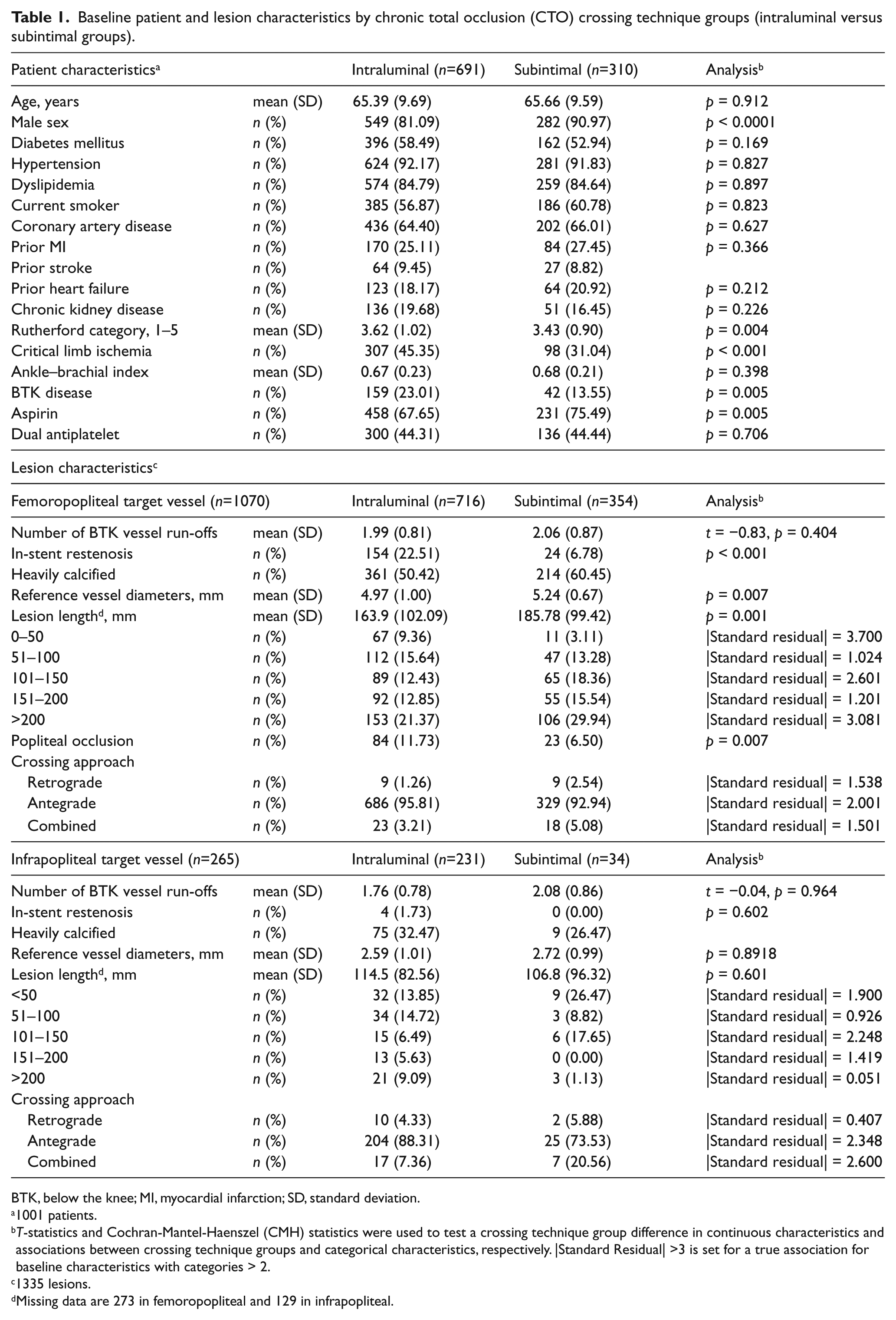
BTK, below the knee; MI, myocardial infarction; SD, standard deviation.
1001 patients.
T-statistics and Cochran-Mantel-Haenszel (CMH) statistics were used to test a crossing technique group difference in continuous characteristics and associations between crossing technique groups and categorical characteristics, respectively. |Standard Residual| >3 is set for a true association for baseline characteristics with categories > 2.
1335 lesions.
Missing data are 273 in femoropopliteal and 129 in infrapopliteal.
While there were no differences in most baseline patient characteristics between the intraluminal and subintimal crossing technique groups, the subintimal group was less likely to have critical limb ischemia (CLI) and below the knee (BTK) disease. A subintimal crossing technique was used more frequently in the femoropopliteal target vessel (34.3%), but significantly less frequently in the BTK vessels (11.9%; p < 0.0001).
Further analysis was stratified by femoropopliteal versus infrapopliteal target vessel interventions (Table 1). When considering femoropopliteal target vessels only (n = 1070 lesions treated), use of the subintimal crossing technique was also less frequently used for treating occluded in-stent restenosis lesions. The subintimal crossing group had significantly longer lesions, but larger reference vessel diameters and a greater number of BTK run-off vessels compared with the intraluminal crossing group (Table 1). For infrapopliteal target vessel interventions (n = 265 lesions treated), there were no significant group differences in any of the baseline lesion characteristics between the intraluminal and subintimal crossing technique groups (Table 1). Duration of procedure and fluoroscopy times were significantly longer in the subintimal crossing group; however, there were no significant differences in periprocedural complications between the two groups (Table 2).
Procedure characteristics and treatment modality by target vessel.
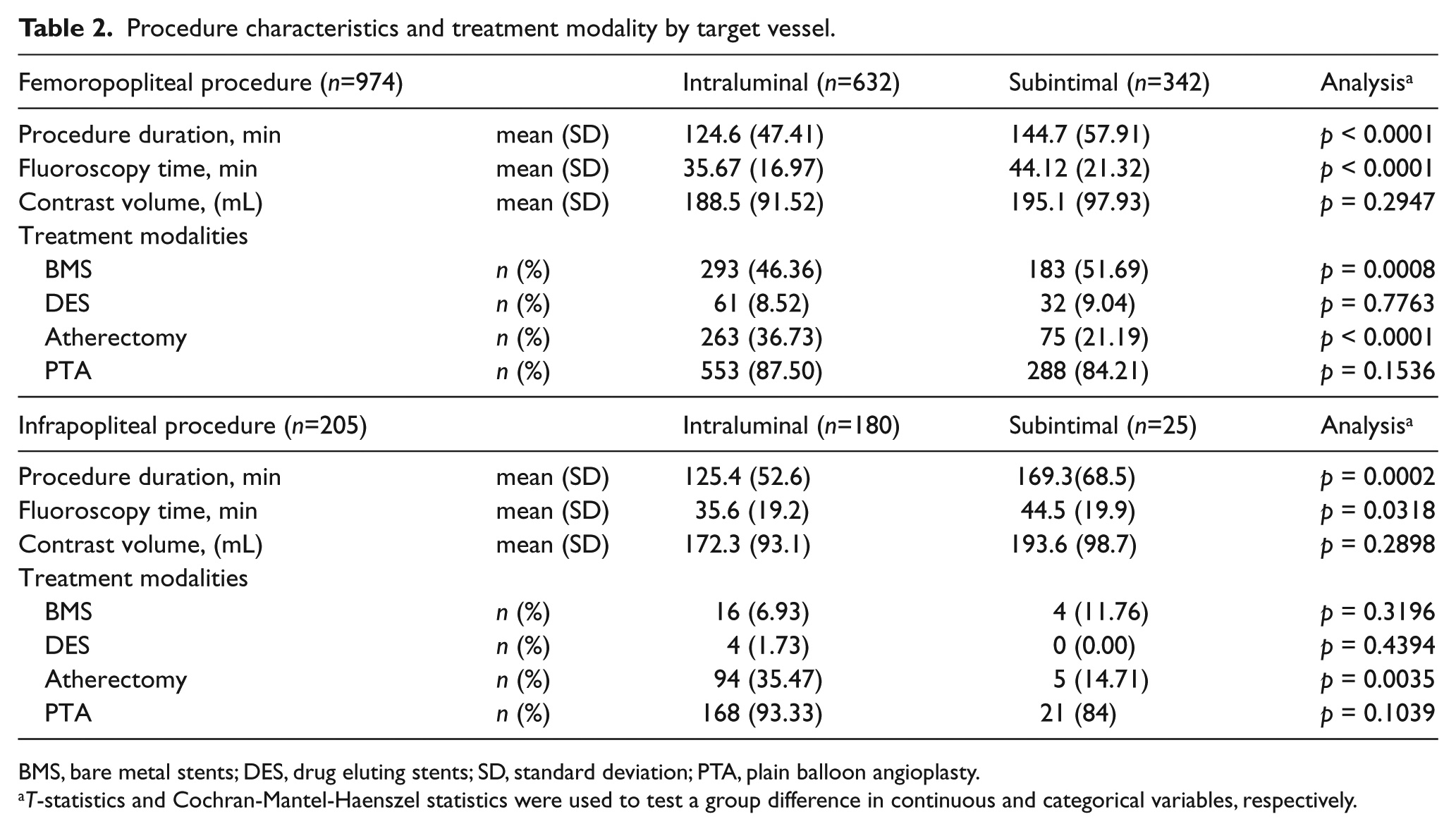
BMS, bare metal stents; DES, drug eluting stents; SD, standard deviation; PTA, plain balloon angioplasty.
T-statistics and Cochran-Mantel-Haenszel statistics were used to test a group difference in continuous and categorical variables, respectively.
Bare metal stents (BMS) use was significantly more often in the subintimal group relative to the intraluminal group in treating femoropopliteal disease, while drug-eluting stents (DES) use was at a similar rate. There were no differences in the use of stents when treating infrapopliteal disease CTOs. For femoropopliteal and infrapopliteal disease, atherectomy use was significantly more prevalent in the intraluminal group than the subintimal group (Table 2). The rates of subintimal crossings were similar with the use of either antegrade or retrograde tibiopedal access for crossing femoropopliteal or infrapopliteal CTOs (Table 2).
Technical failure (12.6% vs 7.9%, p = 0.0186, femoropopliteal disease; 28.0% vs 7.8%, p = 0.0018, infrapopliteal disease) and procedural failure (14.6% vs 10.1%, p = 0.0383, femoropopliteal disease; 32.0% vs 8.9%, p = 0.0008, infrapopliteal disease) rates were significantly higher with subintimal crossing in treating both femoropopliteal and infrapopliteal diseases than with intraluminal crossing. There were no group differences in procedural complications between the two crossing groups except a significantly higher rate of residual dissection in the subintimal group (3%) compared to the intraluminal group (1%, p = 0.0356; Table 3) treating femoropopliteal disease. Thirty-day outcomes between the two crossing groups were similar in both femoropopliteal and infrapopliteal diseases (online Supplementary Figures 1 and 2).
Periprocedural complications by target vessel.
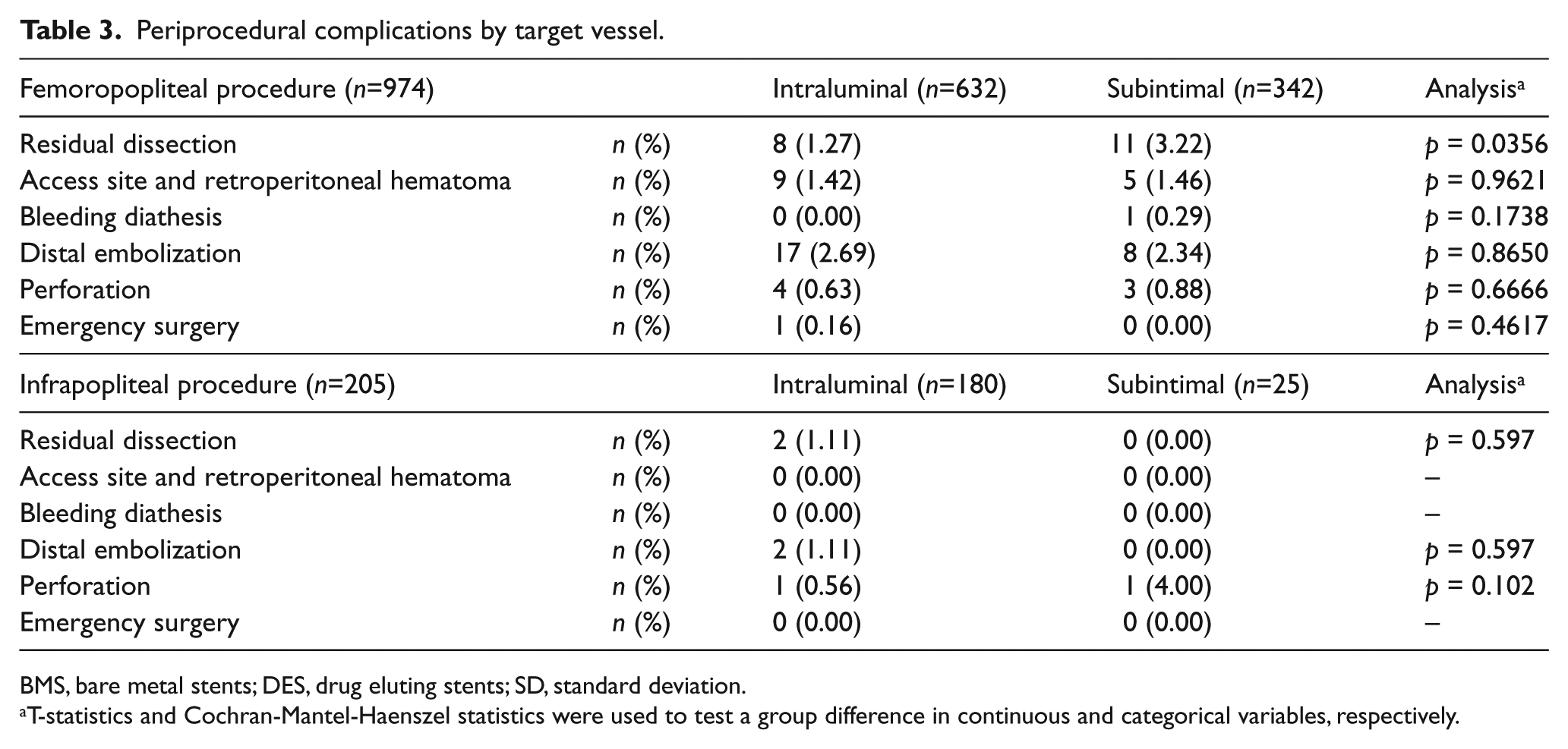
BMS, bare metal stents; DES, drug eluting stents; SD, standard deviation.
T-statistics and Cochran-Mantel-Haenszel statistics were used to test a group difference in continuous and categorical variables, respectively.
For both femoropopliteal and infrapopliteal target vessel interventions, there were no significant group differences in rates of death, non-fatal MI or stroke, or repeat revascularization at 12 months between the intraluminal and subintimal groups (Figures 2 and 3). Kaplan-Meier analyses showed no significant differences between the two crossing groups in the median time to death (log rank χ2 = 0.09, p = 0.7670, femoropopliteal; log rank χ2 = 0.99, p = 0.3199, infrapopliteal), non-fatal MI or stroke (log rank χ2 = 0.02, p = 0.8658, femoropopliteal; log rank χ2 = 2.56, p = 0.1095, infrapopliteal), or target limb endovascular or surgical revascularization events in 12 months (log rank χ2 = 0.53, p = 0.4678, femoropopliteal; log rank χ2 = 0.34, p = 0.5616, infrapopliteal). There were no significant group differences in 12-month ST rates between the two crossing technique groups in either femoropopliteal (Figure 2) or infrapopliteal interventions (Figure 3).
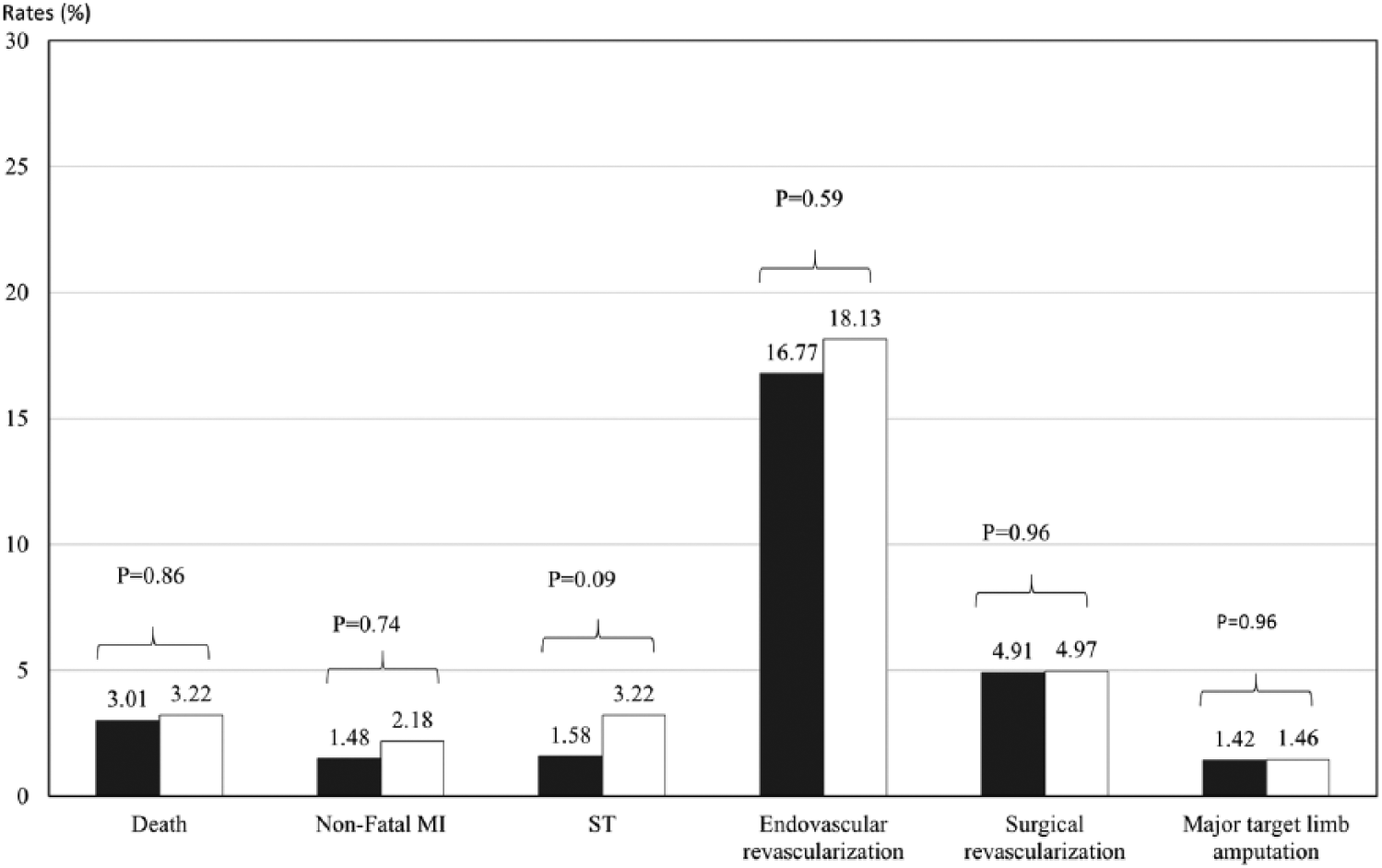
Twelve-month adverse event rate by crossing technique in femoropopliteal target vessel.
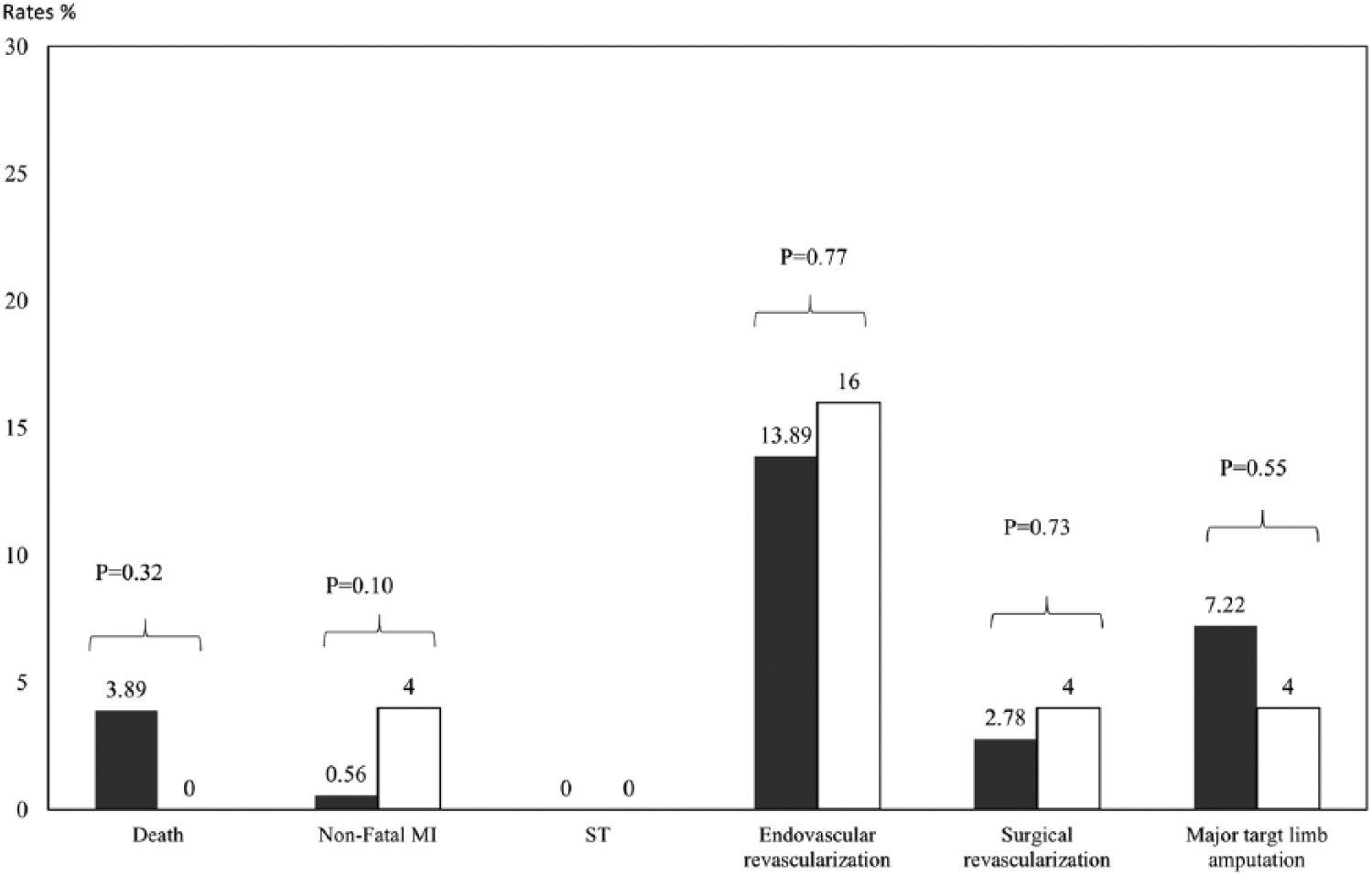
Twelve-month adverse event rate by crossing technique in infrapopliteal target vessel.
Discussion
Crossing of infrainguinal peripheral artery CTOs involves passage of a guidewire, catheter or a CTO crossing device through the proximal cap, body of the total occlusion, distal cap and entry into the true lumen distal target vessel. A hardened proximal or distal cap, long lesion length and failure to re-enter the distal true lumen are frequent challenges encountered by operators during CTO interventions. Often, the guidewire takes the path of least resistance and dissects the vessel intima and enters into the subintimal space. Traditionally, the subintimal crossing technique was used as a bail-out crossing strategy after failure to cross intraluminally. However, as minimally invasive approaches to treat long and occluded segments of infrainguinal arteries have become commonplace and routine, the subintimal approach is sometimes adopted preferentially by operators to cross CTO lesions. Baseline characteristics that predict use of the subintimal crossing technique are presence of collaterals at the proximal stump, heavy calcification, long occluded lesions and full length tibial artery occlusions. 7 The technical difficulty in subintimal crossing of long CTOs commonly arises with re-entry into the distal true lumen, 8 which can be overcome with use of re-entry devices – Outback™ (Cordis, Miami Lakes, FL, USA), Pioneer™ (Medtronic, Minneapolis, MN, USA), Enteer™ (Medtronic), and OffRoad™ (Boston Scientific Corporation, Marlborough, MA, USA) – specifically designed for subintimal re-entry.
In our study, about 30% of CTO lesions were crossed subintimally. Given the retrospective capture of these data in the registry, the decision to employ a subintimal crossing technique prior to the start of the procedure based on baseline lesion characteristics cannot be confirmed. However, about 17% of the subintimal crossing was a bail-out strategy in our study. The subintimal technique was more frequently employed in longer CTO lesions and with bigger vessel diameters at baseline. And, as expected, its use was less frequent during crossing of occluded in-stent restenotic lesions. The subintimal group had significantly higher stenting and residual dissection rates. Although the residual dissection rates were low, this observation may be due to the fact that all areas of dissections, especially non-flow-limiting, may not have received a stent scaffold.
While there were no significant differences in 30-day or 12-month mortality, non-fatal MI or stroke, ST, or repeat revascularization events between subintimal and intraluminal crossing groups, utilizing the subintimal technique was associated with longer procedures, and higher technical and procedural failure rates.
Soga et al. compared intraluminal versus subintimal crossing techniques in long lesions (>10 cm) and found no significant differences in patient outcomes, but decreased duration of procedure with the subintimal crossing technique. In contrast, we observed an increased procedure duration and fluoroscopy time in the subintimal group. This difference could most likely be due to the use of the subintimal crossing technique for more difficult CTO procedures, involving longer lesion lengths. 9 The mean lesion length in the subintimal crossing group in our study was significantly higher than in the intraluminal group in both the studies; however, in the study by Soga et al., the analysis was conducted from a prospective database based on an intent-to-treat principle. In contrast, our study includes a retrospective cohort of subintimal crossing with a guidewire or crossing device.
We also observed similar 30-day and 12-month ST rates between the subintimal and intraluminal groups. Ishihara et al. have reported a similar Zilver PTX ST rate with intraluminal and subintimal crossing of femoropopliteal CTOs. 10
The presence of a pre-existing stent or in-stent restenotic lesions provides a clear fluoroscopically identifiable target for crossing and hence it is not surprising that the subintimal crossing technique is less frequently used for such lesions. It is nevertheless an invaluable approach when the occluded previously stented segment has multiple levels of complex stent fractures or other structural deformations that preclude intraluminal crossing.
Limitations
Our study from a large adjudicated observational peripheral artery intervention registry has important limitations associated with retrospective data capture and therefore we are unable to define the intent of the subintimal approach, intentional versus bail out, leading to possible overestimation of the technical success of the intraluminal approach. In addition, retrograde CTO crossing is under-represented in our study, although it is being increasingly used in contemporary clinical practice.
Conclusion
In conclusion, the results of this study indicate that the subintimal crossing strategy to traverse infrainguinal peripheral artery CTO is often employed to tackle more complex lesions. Subintimal crossing can be successfully performed with low periprocedural complications, and favorable short and intermediate term clinical outcomes, compared with an intraluminal approach.
Footnotes
Acknowledgements
The authors of this manuscript would like to acknowledge the contributions of Nicolas W Shammas, MD, Mazin Foteh, MD, Shirling Tsai, MD, Mujtaba Ali, MD, Mazen Abu-Fadel, MD, Osvaldo S Gigliotti, MD, Ian Cawich, MD, Gerardo Rodriguez, MD, PhD, Dharam Kumbhani, MD, Tayo Addo, MD; and Michael Luna, MD and Tony S Das, MD for their contributions to the XLPAD registry. We also acknowledge the support of the University of Texas Southwestern Medical Center for their support in establishing and managing the REDCap database software utilized in the XLPAD registry (Academic Information Systems NIH grant UL1-RR024982).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Prasad – research grants: Medtronic, Osprey Medical; speaker bureau: Astra Zeneca, Gilead. Dr Armstrong – consulting/advisory board: Abbott Vascular, Boston Scientific, Cardiovascular Systems, Medtronic, Spectranetics. Dr Brilakis – consulting/speaker honoraria: Abbott Vascular, Asahi, Boston Scientific, Elsevier, Somahlution, St Jude Medical, Terumo; research support: InfraRedx, Boston Scientific; spouse is an employee of Medtronic. Dr Banerjee – research grants: Boston Scientific, The Medicines Company; consulting/speaker honoraria: Gilead, St Jude, Cordis, Boehinger Ingerheim, Sanofi, Medtronic; ownership: Mdcare Global (spouse); intellectual property: HygeiaTel. Drs Kondapalli, Jeon-Slaughter, Lu, Xu, and Khalili report they have no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the registry received funding through a research grant from Boston Scientific Corporation.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.