
Abstract
With growing use of drug-coated balloons (DCB) for femoropopliteal (FP) artery interventions, there is limited information on rates of real-world adjunctive stent use and its association with short and long-term outcomes. We report on 225 DCB treated FP lesions in 224 patients from the Excellence in Peripheral Artery Disease (XLPAD) registry (NCT01904851) between 2014 and 2016. Cochran–Mantel–Haenszel and Wilcoxon rank sum statistics were used to compare stented (planned or ‘bail-out’) versus non-stented DCB treated lesions. Stents were implanted in 31% of FP DCB interventions. Among the 70 stents implanted, 46% were for ‘bail-out’ indications and 54% were planned. Lesions treated with stents were longer (mean 150 mm vs 100 mm; p < 0.001) and less likely to be in-stent restenosis lesions (10% vs 28%; p=0.003). Stenting was significantly more frequent in complex FP lesions, including chronic total occlusions (66% vs 34%; p < 0.001). For bail-out stenting, interwoven nitinol stents were the most common type (50%) followed by drug-eluting stents (34%) and bare-metal stents (22%). There were no differences in peri-procedural complication rates or 12-month target limb revascularization rates (18.6% vs 11.6%; p=0.162) or 12-month amputation rates (11.4% vs 11%; p=0.92) between lesions where adjunctive stenting was used versus lesions without adjunctive stenting, respectively. In conclusion, in a contemporary ‘real-world’ adjudicated multicenter US registry, adjunctive stenting was necessary in nearly a third of the lesions, primarily for the treatment of more complex FP lesions, with similar short and intermediate-term clinical outcomes compared with non-stented lesions.
Keywords
Introduction
Approximately 8.5 million American adults are affected by peripheral artery disease (PAD), and femoropopliteal (FP) artery disease accounts for more than 50% of such cases.1,2 FP artery disease can lead to either lifestyle-limiting claudication or critical limb ischemia (CLI).3,4 Traditionally, surgical therapy has been considered the optimal treatment for FP lesions, but with the development of new technologies the majority of these lesions are now treated with an endovascular first approach.5,6 Until recently, the majority of endovascular interventions included stenting and percutaneous transluminal angioplasty (PTA). 6 With the evolving use of drug-coated balloons (DCB), these devices are now used in a significant number of endovascular interventions, since they provide improved long-term outcomes compared to PTA, while decreasing the need for permanent scaffold implantation.7–11 DCB are associated with FP patency rates comparable to primary stenting for the treatment of de novo FP PAD.7,8,12 However, in a significant proportion of FP DCB interventions, a vascular scaffold placement may be necessary to treat vessel recoil, significant dissection, or otherwise suboptimal angioplasty.12–14 However, little is known about the differences in procedural and long-term outcomes between stented and non-stented FP lesions treated with DCB. Our aim in this study was to examine the prevalence of adjunctive stent use during DCB angioplasty, and to report any differences in outcomes based on this procedural approach.
Methods
The Excellence in Peripheral Artery Disease (XLPAD; NCT01904851) multicenter registry includes consecutive cases of patients undergoing endovascular interventions between 2005 and 2016. All available patients from the enrolled site are entered to XLPAD. Patients who have multiple interventions are entered only the first time and future interventions are not considered separate entries. For this study, we extracted all the DCB cases for the treatment of FP disease entered to XLPAD from the participated sites at the time of the analysis (225 FP lesions in 224 patients). There were no other exclusion criteria. The protocol for the XLPAD registry was approved by the institutional review boards of the participating centers.
Pertinent subject data (including baseline demographic and clinical characteristics as well as lesion characteristics, procedural details, and up to 12-month follow-up) were collected retrospectively using the electronic medical records of each participating site by experienced abstractors and entered into an online REDCap data capture software. The VA North Texas Angiography and Ultrasound Core Laboratory was used to analyze the angiograms of the enrolled patients from all the sites. The core lab analysts reviewed in detail the lesion and procedural characteristics. This included validation of treated lesion characteristics entered earlier in the data collection process and entry of new data for missing variables. Variables such as lesion length, reference vessel diameter, in-stent stenosis, chronic total occlusion status, heavy calcification, diffuse disease and below the knee vessels runoff were always confirmed by the core lab. When there was a disagreement between the core lab and the initial entry, the core lab values were chosen. Follow-up was available up to 12 months after the index procedure. Core lab analysis was performed for outcomes such as stent thrombosis and in-stent restenosis when available, but not for patients where the outcome was amputation or death. Core lab analysis was not used to adjudicate adverse events. Instead, this was done by the research personnel of each enrolled site.
Two DCB types were used: Lutonix® (BARD Peripheral Vascular, Inc., Tempe, AZ, USA) and IN.PACT AdmiralTM (Medtronic, Santa Rosa, CA, USA)). The DCB technique used was at the discretion of each operator, but in general it included pre-dilation with a goal vessel preparation of residual stenosis < 30% prior to DCB angioplasty. DCBs were inflated to nominal pressure for 3 minutes, as per the instructions for use. Baseline patient and lesion characteristics and procedural characteristics were compared between DCB treated lesions where adjunctive stenting was used and lesions treated without stent implantation. Primary outcomes of interest included procedural complications (dissections, perforations, bleeding diathesis, emergency surgery, distal embolization, retroperitoneal and access site hematoma, and acute renal failure) as well as 30-day and 12-month target limb repeat endovascular or surgical revascularization (TLR), and target limb major or minor amputations. Secondary outcomes included 30-day and 12-month mortality, non-fatal myocardial infarction, and stroke. There were no composite endpoints.
Statistical analysis
Continuous variables are described with mean and standard deviations and categorical variables are described with absolute and relative frequencies. Cochran–Mantel–Haenszel (CMH) statistics and the two-sided Wilcoxon rank sum test were used to compare categorical and continuous variables, respectively. When a categorical variable had more than two values, a n × m contingency table with an absolute value of standard residual (|standard residual|) was used to test a true association between adjunctive stenting and the pertinent variable. Statistical significance was set as a p-value < 0.05. All analyses were performed using SAS 9.4 software (SAS Institute, Cary, NC, USA).
Results
In total, 225 FP DCB endovascular interventions from the XLPAD registry were included in this study. The average age was 67 years, while the majority was male (88%) and Caucasian (71%), with a high prevalence of hypertension (84%) and hyperlipidemia (80%) at baseline. Medtronic’s IN.PACT Admiral (75%) was used more frequently than Bard’s Lutonix (26%). Among FP DCB interventions, adjunctive stenting was used in 31% (n=70). There were no significant differences in demographic or clinical characteristics between the two groups (Table 1). Stenting was less likely to be adjunctively used in Lutonix DCB revascularization (16%) than in IN.PACT Admiral DCB (37%). FP lesions that were treated with adjunctive stent revascularization strategies were longer (mean: 152 mm vs 100 mm; p < 0.0001), less likely to be in-stent restenosis lesions (10.0% vs 27.7%; p=0.003), but more likely to be chronic total occlusions (CTOs) (65.7% vs 33.6%; p < 0.001) and with diffuse disease (65.7% vs 48.4%; p=0.016) compared with lesions treated with DCB, but without stents. The prevalence of severe calcification was similar between the two groups (30.0% vs 29.7%; p=0.961).
Baseline patient and lesion characteristics (lesion-level analysis).
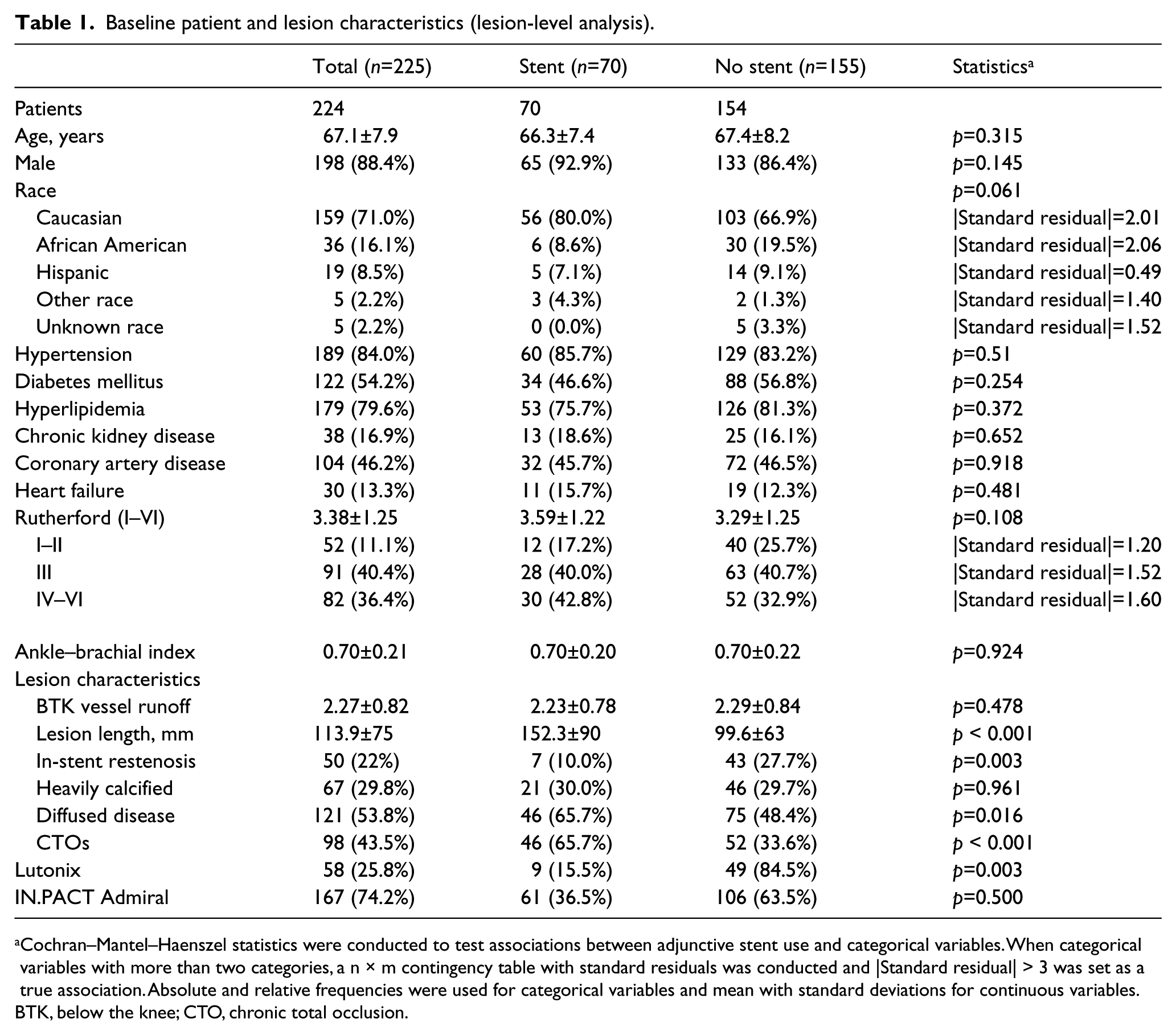
Cochran–Mantel–Haenszel statistics were conducted to test associations between adjunctive stent use and categorical variables. When categorical variables with more than two categories, a n × m contingency table with standard residuals was conducted and |Standard residual| > 3 was set as a true association. Absolute and relative frequencies were used for categorical variables and mean with standard deviations for continuous variables.
BTK, below the knee; CTO, chronic total occlusion.
A total of 46% of the lesions were treated with atherectomy devices. The atherectomy rate was similar between the adjunctive stenting and the non-stenting groups. The majority of atherectomy devices were used adjunctively with PTA for lesion preparation and pre-dilation (88.4%). Among lesions treated with adjunctive stenting, 46% were for a bail-out indication. Among the adjunctive stenting group, in 86% (n=60) of the interventions, a single stent was used, while in 14% more than two stents were placed. Among lesions treated with bail-out stenting, interwoven nitinol stents were used in 50%, drug-eluting stents (DES) in 34% and bare-metal stents (BMS) in 22% (Table 2). In cases treated with a planned stent revascularization strategy, DES was the most common (45%), followed by interwoven nitinol stents (37%) and BMS (24%). There were no significant differences in the lengths of lesions treated with either planned or bail-out stenting (140 mm vs 167 mm; p=0.340).
Adjunctive strategies and devices used between bail-out and planned stent revascularization strategies in DCB and stent FP interventions.
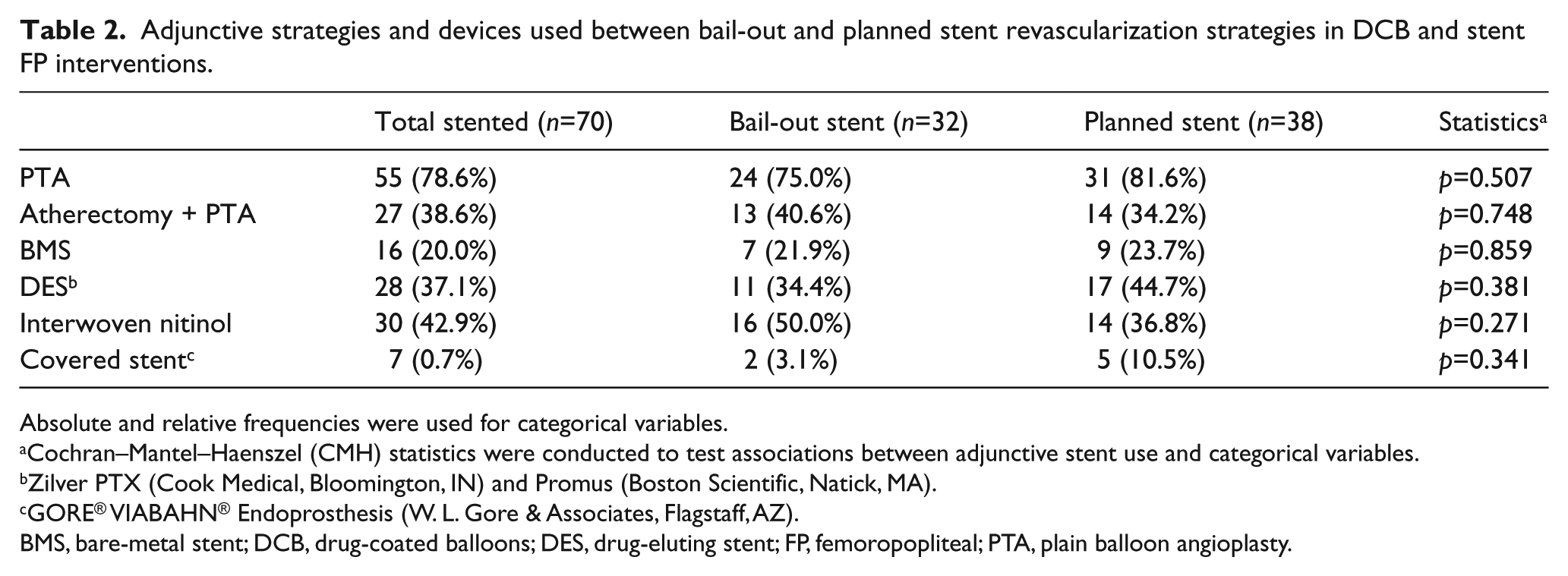
Absolute and relative frequencies were used for categorical variables.
Cochran–Mantel–Haenszel (CMH) statistics were conducted to test associations between adjunctive stent use and categorical variables.
Zilver PTX (Cook Medical, Bloomington, IN) and Promus (Boston Scientific, Natick, MA).
GORE® VIABAHN® Endoprosthesis (W. L. Gore & Associates, Flagstaff, AZ).
BMS, bare-metal stent; DCB, drug-coated balloons; DES, drug-eluting stent; FP, femoropopliteal; PTA, plain balloon angioplasty.
Adjunctive stenting was significantly associated with non-flow limiting dissections (18.6% vs 4.5%; p < 0.001) and had a borderline association with flow limitingdissections (4.3% vs 0.7%; p=0.056). There were no other differences in procedural complications between the two groups. The 30-day or 1-year outcomes did not differ significantlybetween the two groups (Table 3). However, there was a trend towards a lower 30-day TLR rate in the non-stented group (0.7% vs 4.3%; p=0.056). The 12-month TLR rate was numerically higher in the adjunctive stenting group compared with the non-stented group (18.6% vs 11.6%; p=0.162). Both major and minor amputation rates were similar between the two study groups (Table 3). There were no differences between the different stent types in procedural complications or 30-day and 12-month outcomes (Supplementary Table A).
Procedural complications and 30-day and 12-month outcomes between lesions treated with DCB and adjunctive stenting versus lesions treated with DCB only.
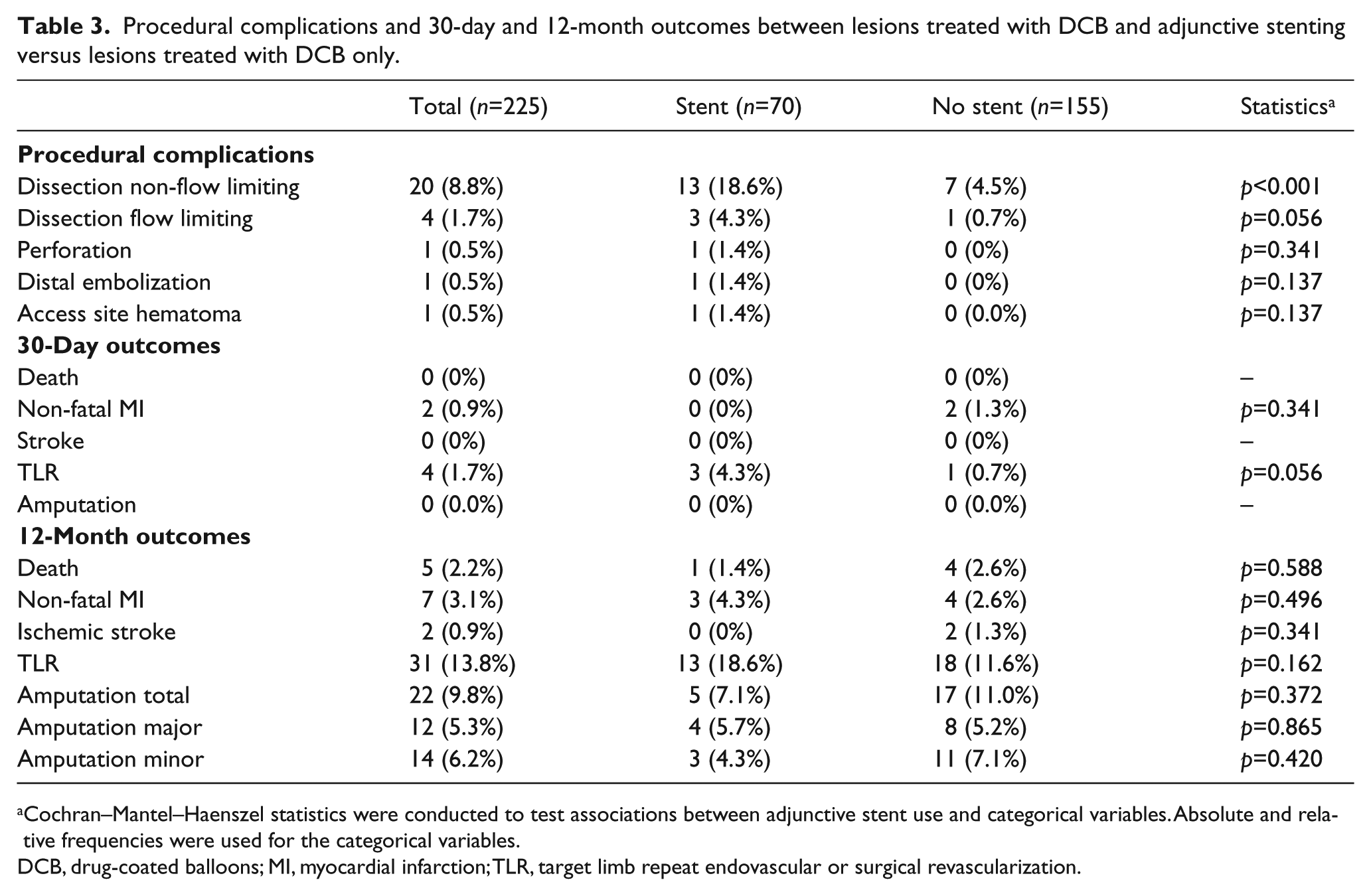
Cochran–Mantel–Haenszel statistics were conducted to test associations between adjunctive stent use and categorical variables. Absolute and relative frequencies were used for the categorical variables.
DCB, drug-coated balloons; MI, myocardial infarction; TLR, target limb repeat endovascular or surgical revascularization.
Discussion
This study utilized patients enrolled in the XLPAD registry who were treated with DCB for FP artery lesions. Our main findings were the following: (i) lesions treated with adjunctive stenting were longer, less likely to be restenotic, and more likely to be CTOs and diffusely diseased; (ii) among the stented lesions, planned stenting (54.3%) was relatively more frequent compared to bail-out stenting (45.7%); (iii) the most common types of stents used were interwoven nitinol stents and DES; and (iv) other than non-flow limiting dissections, there were no statistically significant differences between the two groups in procedural complications or early or late outcomes.
Traditionally, endovascular treatments of the superficial femoral artery segment are challenging as it is repeatedly exposed to dynamic forces such as flexion, longitudinal and lateral compression, and torsion. 15 For years, PTA was the standard treatment strategy for endovascular intervention of the FP segment, while the use of primary stenting (with the use of older generation stents) did not significantly improve the durability of endovascular intervention compared to PTA with provisional stenting.16–19 With the evolving use of new therapeutic strategies, there are currently better options to improve both acute and long-term patient outcomes.16,20–23 Interwoven nitinol stents, due to their high radial force and flexibility, have also helped to overcome many of the disadvantages associated with self-expanding bare-metal nitinol stents.24–27 However, certain procedural limitations associated with stent placement, such as the need for meticulous vessel preparation and careful stent diameter selection, continue to exist. Moreover, stents are associated with the risk of fracture and can increase the neointimal hyperplastic response and result in restenosis and the need for additional interventions in the future.28–32 DCBs address many of these concerns, offering a valuable alternative, even for the more complex lesions. Published data support that DCBs lead to superior mid- and long-term clinical outcomes compared to PTA for FP lesions,33–35 even if the evidence level for long real-world lesions is limited.36–38
Even with DCB use, the need for stenting of some lesions remains. 39 The rates of provisional stenting among DCB treated FP lesions range from 4.1% to 27% in clinical trials and from 11% to 23.3% in two real-world studies from Italy and Germany respectively.33,38,40–42 Bail-out stenting was 14.2% in our DCB treated FP lesions, while the total rate of adjunctive stenting (bail-out or planned) was 31%. These rates are higher than those reported by the clinical trials. The criteria for stent implantation were usually at the discretion of each operator, but in the majority of cases the decision to implant a stent was due to the presence of significant residual dissection despite prolonged DCB angioplasty. Residual hemodynamic gradients were not routinely measured. Therefore, the criteria to place stents after DCB angioplasty represent real-world decision making for anatomically complex lesions. The rate of stenting in Lutonix cases was 15.5% versus 36.5% for In.PACT Admiral. While we cannot be sure that the differential stent rate was not related to the specific type of DCB, we believe it is most likely that the lower stent rate with Lutonix balloons was due to use of this DCB type in less complex lesions, leading therefore to a lower bail-out stent rate. This can be also supported by the fact that in our registry, the majority of Lutonix cases were performed earlier in the course of DCB use in the US when operators were relatively more reluctant to use DCBs in complex lesions. We believe that the two DCBs would perform equally in a larger and more homogeneous sample. We also demonstrated that lesions, where adjunctive stenting was used, were more complex (e.g. longer lesions, more CTOs, and diffusely diseased vessels). Adjunctive stenting was less likely to be used for in-stent restenosis, which is consistent with the concept of avoiding an extra metal layer for cases where a stent is already present.6,43,44 DES were the implanted stents in 34% of the cases. These arteries thus received double the amount of anti-proliferative medications. Even if the evidence on this topic is still low, preliminary data from the XLPAD registry presented recently show that technical and procedural successes and 1-year outcomes are similar between lesions treated with a DCB, and DES versus lesions treated with DCB and nitinol stents. 45
The degree of calcification was another important factor in our study. In almost 30% lesions, calcification was graded as severe, while the majority of our lesions had at least moderate calcification. The calcification severity in our cohort may justify the use of atherectomy devices in 46% of the lesions.9,46 Previous reports have suggested that the combination of DCB with orbital atherectomy could be a sufficient treatment option for these lesions. 9 The high rate of atherectomy used in our real-world cohort is justified by the belief of our operators that atherectomy devices and, subsequently, optimal vessel preparation, significantly improve DCB outcomes in calcified and complicated (restenosis, CTOs, diffusely diseased) vessels.9,23
In one prior analysis, Zeller et al. showed that the group treated with DCB (± stents as needed) resulted in non-inferior clinical outcomes (freedom from TLR and event free survival) when compared with the stented group for lesions longer than reported by our group. 12 These results support the use of DCB with provisional stenting for long FP lesions. 12 Our study adds to these findings by providing supportive evidence to indicate that among DCB treated FP lesions, those that are eventually stented (bail-out or planned) do not differ in outcomes compared with non-stented lesions.
Study limitations
The results of our study should be interpreted in the context of several limitations associated with real-world studies, including operator and case selection bias, and non-randomized allocations of treatments. Our overall sample size is limited, which hinders a direct comparison of bail-out stenting versus only DCB treated lesions. The small sample size of our study also made a propensity score matched analysis not feasible. 47 The stented group of our study was significantly smaller (70 vs 155) compared to the DCB only group. This can be explained by the real-world design of our study. One of the major advantages associated with DCBs is that they reduce the need for bail-out stenting. Owing to the drug-eluting substances, they offer similar long-term results with stented FP arteries and this is why, in the majority of the DCB interventions for FP lesions, interventionalists try initially not to place a stent. Given the observational design of XLPAD, whether or not stenting was planned or bail-out is a data entry point filled retrospectively and thus subject to limitations compared to a randomized design where such a differentiation (bail-out vs planned) would be more trustworthy. Another limitation of our study is that we do not present data on patency rates and target lesion revascularization. For patency rates, we think that in observational, real-world studies, harder endpoints (such as TLR) are more accurate, especially with the population included in this study (the majority of the included patients come from VA hospitals; with veterans who receive the majority of their care within the VA system, outcomes such as TLR are accurate and difficult to miss in the data collection process). Instead of target lesion revascularization, we present data on target limb revascularization. This is based on the design of the XLPAD registry (data were collected for target limb and not target lesion revascularization). In most studies, there is a close relationship between target lesion revascularization and target limb revascularization, given that restenosis is the most likely mechanism of failure requiring re-intervention at a year. In addition, XLPAD collects only 12-month follow-up outcome data and longer follow-up data are missing in the manuscript. The strength of our study is that the included population represents a more complex group of patients with FP PAD with long lesions and CTOs representative of real-world use of DCBs in contemporary US clinical practice in contrast to randomized clinical trials.
Conclusions
Our results indicate that adjunctive stenting with DCB treatment in real-world FP interventions is needed in almost one-third of cases, mainly in lesions of greater complexity. Interestingly, there were no differences in procedural or short and long-term outcomes between stented and non-stented FP lesions. Future well-designed, prospective, ‘real-world’ studies or RCTs are needed in order to further examine whether adjunctive stenting in DCB treated FP lesions can alter either procedural outcomes, devices needed (lesion preparation with cutting balloon or atherectomy devices, bail-out stenting, complications) and short- and long-term clinical outcomes.
Supplemental Material
VMJ775593_Supplementary_Table – Supplemental material for Adjunctive stent use during endovascular intervention to the femoropopliteal artery with drug coated balloons: Insights from the XLPAD registry
Supplemental material, VMJ775593_Supplementary_Table for Adjunctive stent use during endovascular intervention to the femoropopliteal artery with drug coated balloons: Insights from the XLPAD registry by Damianos G Kokkinidis, Haekyung Jeon-Slaughter, Houman Khalili, Emmanouil S Brilakis, Nicolas W Shammas, Subhash Banerjee and Ehrin J Armstrong in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Brilakis: Honoraria: Abbott Vascular, Asahi, Cardinal Health, Elsevier, GE Healthcare, and St Jude Medical; Research grants: InfraRedx and Boston Scientific; spouse is employee of Medtronic. Dr. Shammas: Research and Educational Grants from Boston Scientific. Dr. Banerjee: Honoraria: Medtronic, Gore, CSI; Research grants: Boston Scientific Corporation, Merck; Intellectual property: Mdcareglobal, HygeiaTel. Dr. Armstrong is a consultant to Abbott Vascular, Boston Scientific, Cardiovascular Systems Incorporated, Medtronic, and Spectranetics.
Funding
The authors disclosed the following financial support for the research, authorship, and/or publication of this article: National Institutes of Health (CTSA Grant No. UL1-RR024982). The Excellence in Peripheral Artery Disease (XLPAD) registry is supported by University of Texas Southwestern Medical Center and Boston Scientific Corporation.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.