
Abstract
Splanchnic vein thrombosis (SVT) and cerebral vein thrombosis (CVT) are two manifestations of unusual site venous thromboembolism (VTE). SVT includes thrombosis in the portal, mesenteric or splenic veins, and the Budd–Chiari syndrome. CVT encompasses thrombosis of the dural venous sinuses and thrombosis of the cerebral veins. Unusual site VTE often represents a diagnostic and therapeutic challenge because of the heterogeneity in clinical presentation, the limited evidence available in the literature on the acute and long-term prognosis of these diseases, and the lack of large randomized controlled trials evaluating different treatment options. This narrative review describes the approach to patients with SVT or CVT by examining the diagnostic process, the assessment of potential risk factors and the appropriate anticoagulant treatment.
Keywords
CME Accreditation Statement
The University of Virginia School of Medicine designates this journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit™ per article. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Learners are expected to read this article along with any references and supporting material as appropriate, and complete the online post-test questions with an 80% pass rate to receive credit. Post-test questions are accessed through the through the Society for Vascular Medicine website (www.vascularmed.org/VMJ-CME). Please note that CME credits are only available to members of SVM with a journal subscription. This activity expires 2 years after the publication date, on December 1, 2019.
Heather Gornik has disclosed research support from AstraZeneca, intellectual property rights from Summit Doppler Systems, Inc., and intellectual property rights and stock/ownership from FlexLife Health (proceeds donated). Aditya Sharma has disclosed research support from National Institute of Health Sciences, AstraZeneca, Biomet Biologics, Portola Pharmaceuticals, and Pedra Technology. Valerie Clark has no financial affiliations to disclose.
Introduction
Unusual site venous thromboembolism (VTE) refers to uncommon thrombosis occurring in venous districts outside the veins of the lower extremities and the pulmonary arteries, and includes, among others, thrombosis in the splanchnic and the cerebral veins.
Unusual site VTE represents a diagnostic and therapeutic challenge because of the heterogeneity in clinical presentation, the limited evidence available in the literature on the acute- and long-term prognosis of these diseases and the lack of large randomized controlled trials evaluating different treatment options.
The aim of this narrative review is to describe the approach to patients with splanchnic vein thrombosis (SVT) or cerebral vein thrombosis (CVT), with a specific focus on the: (1) diagnosis of thrombosis and definition of thrombus extension through specific diagnostic imaging tests; (2) evaluation of potential thrombotic risk factors in order to classify the thrombosis as provoked or unprovoked; (3) early initiation of anticoagulation and decisions about treatment duration.
Splanchnic vein thrombosis
SVT encompasses portal vein thrombosis (PVT), mesenteric vein thrombosis (MVT), splenic vein thrombosis (SpVT) and the Budd–Chiari syndrome (BCS). PVT is the most frequent manifestation of SVT, with incidence rates of 3.78 cases in males and 1.73 cases in females per 100,000 inhabitants; whereas BCS is the least common disease, with incidence rates of 2.0 cases in males and 2.2 cases in females per million inhabitants. 1 SVT has a peak incidence in the 50s and a prevalence of male sex (approximately 60%), except for BCS which occurs more frequently in the 40s and has a prevalence of female sex (approximately 65%).2,3
Clinical manifestation and diagnosis
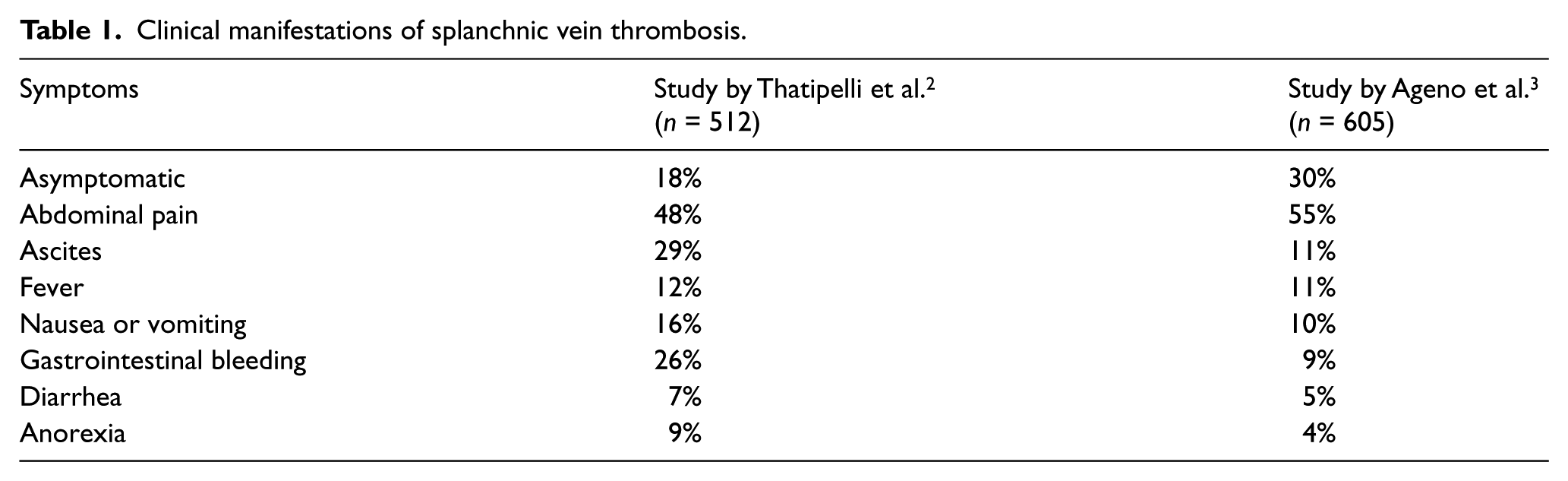
Clinical manifestations of SVT are heterogeneous, showing some differences according to the site of thrombosis. Furthermore, symptoms are non-specific and they may resemble other abdominal diseases. The most common symptoms are: abdominal pain (reported in 40% of PVT and more than 60% of MVT); upper or lower gastrointestinal bleeding (reported in around 25% of patients with acute PVT or SpVT); and ascites (reported in more than 70% of patients with BCS).2,4 Some symptoms are triggered by portal hypertension, such as splenomegaly, hypersplenism, ascites and gastroesophageal varices.4,5 Other non-specific symptoms include fever, nausea or vomiting, diarrhea and anorexia.2,3
Furthermore, acute MVT can be associated with intestinal ischemia in approximately one-third of patients. 6 BCS can be fulminant in approximately 5% of patients, presenting with hepatic encephalopathy and extensive hepatocellular necrosis. 4
Finally, approximately 30% of SVT are asymptomatic, mostly incidentally detected at computed tomography (CT) scans performed in patients with liver cirrhosis or solid cancer.7,8 Clinical manifestations of SVT are reported in Table 1.
Clinical manifestations of splanchnic vein thrombosis.
D-dimer does not have a role in the diagnosis of SVT due to its low specificity and the high percentage of false positive results, especially in patients with cancer or liver cirrhosis. 9 Therefore, the diagnosis of SVT relies on different imaging tests: abdominal Doppler ultrasound (US), CT angiography and magnetic resonance (MR) angiography, with specific protocols for the venous phase and for the area of interest. The diagnostic approach to SVT is summarized in Table 2.
Summary of the diagnostic approach to splanchnic vein thrombosis.
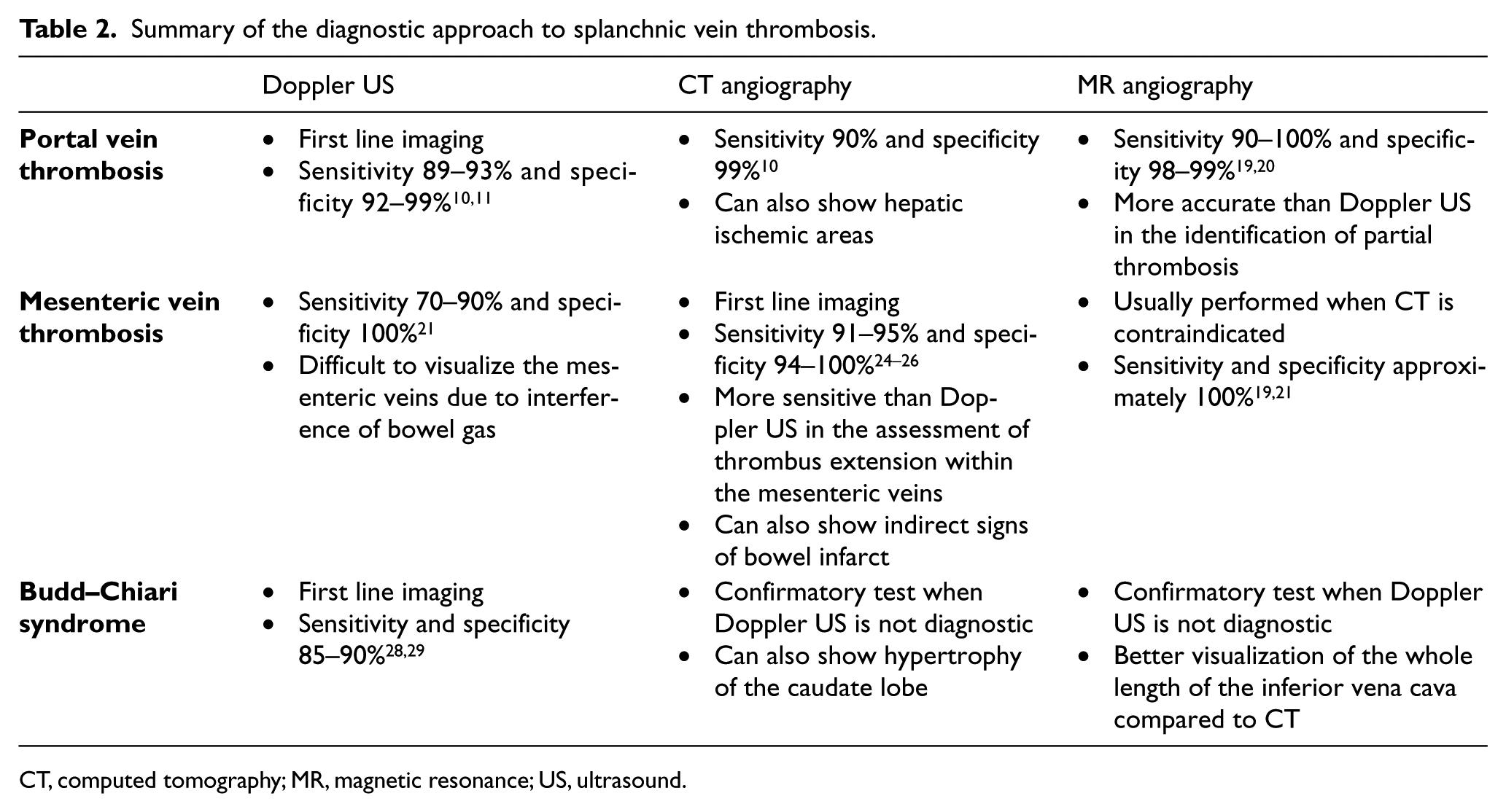
CT, computed tomography; MR, magnetic resonance; US, ultrasound.
Portal vein thrombosis
Doppler US is the imaging of choice for the diagnosis of PVT, with a sensitivity of 89–93% and a specificity of 92–99%.10,11 Doppler US can show the absence of flow in the portal vein, as well as the hyperechogenic thrombus inside the lumen or the presence of collateral circulation. 12 In chronic PVT, Doppler US can show the cavernomatous transformation of the portal vein, which consists of several serpiginous porto-portal collaterals to preserve the hepatopetal flow.13,14 Doppler US has the advantages of being widely available (e.g. also as bedside imaging) and relatively inexpensive; however, it is an operator-dependent imaging method and the accuracy can be limited by body habitus and the presence of bowel gas. 15
CT without contrast can display the thrombus within the portal vein, which is hyperdense if it occurred within a month and afterwards it becomes isodense or slightly hypodense. 16 CT with contrast and CT angiography can show the filling defect in the portal vein. Furthermore, the ischemic areas in the liver appear as increased enhancement during the arterial phase and decreased enhancement during the portal phase. 17 CT angiography has been reported to have a sensitivity of 90% and a specificity of 99% 10 ; however, it involves the use of ionizing radiations and iodinated contrast agent, with potential renal toxicity and allergic reactions. 15
At MR imaging, the thrombus in the portal vein appears isointense on T1-weighted images and hyperintense on T2-weighted images. 18 MR angiography is more accurate than Doppler US in the identification of partial thrombosis and has a sensitivity of 90–100% and a specificity of 98–99%.18–20 Compared to Doppler US, CT and MR have the additional advantage of providing information about the cause of thrombosis (such as infection, inflammation, cancer). MR angiography has a better soft tissue resolution than CT, does not involve ionizing radiations and uses a paramagnetic contrast agent with a better safety profile. However, MR angiography can overestimate the severity of stenosis, has a low sensitivity for the detection of calcifications and visualization of stents, and requires a long time to complete the scan (e.g. 30–60 minutes). 15
Mesenteric vein thrombosis
For the detection of MVT, Doppler US has a low sensitivity (70–90%). 21 Mesenteric veins are difficult to visualize with the Doppler US, since a poor acoustic window can result from the overlying intestinal gas.22,23 An experienced ultrasonographer can usually evaluate the segment of the superior mesenteric vein near the spleno-portal confluence. 18
Therefore, CT angiography and MR angiography are the standard diagnostic imaging tests for the diagnosis of MVT. CT can show the thrombus within the mesenteric veins and can also provide indirect signs of bowel infarct (such as the thickening of the intestinal wall). 22 CT has a sensitivity of 91–95% and a specificity of 94-100% .24–26 MR has sensitivity and specificity of approximately 100% for the evaluation of the mesenteric vessels and is usually performed when CT is contraindicated.18,19,21
Conventional angiography is performed only when the other imaging tests are inconclusive or with the purpose of administering transcatheter vasodilators or thrombolytics. 22 In the presence of intestinal infarction, emergency laparoscopy or laparotomy can be needed to resect the necrotic tract. 18
Budd–Chiari syndrome
For the diagnosis of BCS, Doppler US is the first line imaging since it is very accurate when performed by an experienced ultrasonographer, showing sensitivity and specificity of approximately 85–90%.27–29 Doppler US can show the thrombus in the hepatic veins or supra-hepatic inferior vena cava, the absence of flow or the retrograde flow in the hepatic veins, and the presence of intrahepatic collaterals, the latter being the most specific sign of BCS.18,30,31 A Doppler US imaging of BCS is presented in Figure 1.
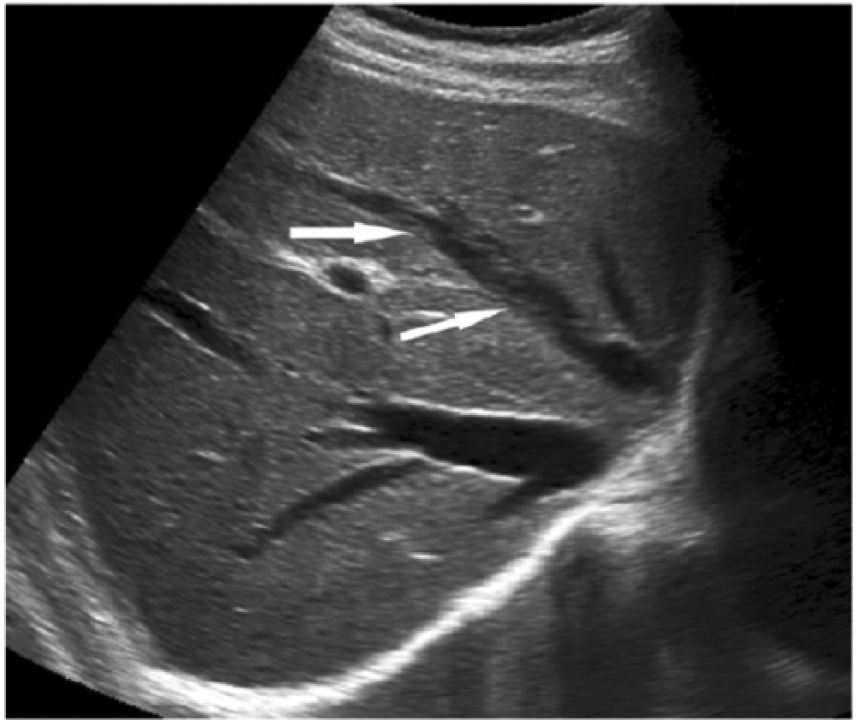
Doppler ultrasound image of a Budd–Chiari syndrome. The arrows show thrombosis in the middle hepatic vein. (Reprinted from Clinical Imaging, volume 40, Faraoun SA, Boudjella Mel A, Debzi N, Benidir N, Afredj N, Guerrache Y, Bentabak K, Soyer P, Bendib SE, Budd-Chiari syndrome: An update on imaging features, 40: 637–646; Copyright © 2016, with permission from Elsevier.)
Abdominal CT and MR are confirmatory tests when Doppler US is not diagnostic. They can show the occlusion of the hepatic veins, the hypertrophy of the caudate lobe and the presence of intrahepatic collateral veins.27,30,32 MR allows better visualization of the inferior vena cava, but it is more expensive and less readily available than CT. 33
Being an invasive examination, hepatic venography is recommended only when the other radiological findings are inconclusive. Nevertheless, venography can also allow pressure measurement to plan for surgical or transjugular shunts. 28 Liver biopsy is not necessary to confirm the diagnosis of BCS. However, it can be useful when radiological imaging tests are still uncertain, especially in rare forms of BCS with involvement of small hepatic veins and patent large veins.27,34
Assessment of risk factors
Abdominal cancer (such as pancreatic, hepato-biliary and gastrointestinal) and hepatic cirrhosis are responsible for approximately 50% of SVT.2,35 In fact, up to 10–20% of patients with hepatic cirrhosis can develop a thrombosis in the portal vein. 36 SVT can also be a marker of occult cancer: in a Danish cohort of SVT patients, the 3-month risk of solid cancer was 8.0% and the risk of myeloproliferative neoplasm (MPN) was 0.7%. 37 Considering non-malignant, non-cirrhotic SVT, MPNs are the most frequent systemic risk factors for SVT, reported in approximately 40% of patients with BCS and 30% of those with PVT. 38
Among the local risk factors, SVT can be associated with abdominal inflammatory diseases or infections (such as inflammatory bowel disease, pancreatitis, cholecystitis, appendicitis, hepatic abscess in 10–30% of cases), abdominal surgery (such as splenectomy, cholecystectomy, liver transplant in around 10% of cases) and abdominal blunt trauma (e.g. after a motor vehicle accident).2–4,39
Therefore, we suggest investigating patients with SVT for the presence of hepatic cirrhosis, solid cancer or local risk factors and, after excluding abdominal diseases, it is recommended that patients with SVT should be screened for the JAK2 V617F mutation, which is considered the molecular marker of MPN. 40
Among thrombophilic disorders, inherited deficit of the natural anticoagulants (antithrombin, protein C and protein S) are difficult to identify because their synthesis is already reduced by the liver dysfunction. However, a recent meta-analysis reported a prevalence of this disorder in 2–6% of patients with PVT and 2–4% of those with BCS. 41 Prothrombin G20210A mutation is more frequently detected in patients with PVT, while factor V Leiden mutation in patients with BCS. 4 Owing to the low prevalence of inherited thrombophilia in SVT patients and the unknown clinical relevance of this finding, routine testing in all patients with SVT is not suggested.
Pregnancy and puerperium are common risk factors in Asian countries, while the use of oral contraceptives is more frequently reported in Western countries. 42 Furthermore, the presence of multiple concomitant risk factors is common in patients with SVT. Finally, approximately 15–30% of SVT occurs in the absence of known risk factors and is classified as unprovoked.2,35
Anticoagulant treatment
Establishing the optimal treatment in patients with SVT can be challenging. 43 It is difficult to balance between the risk of potentially life-threatening thrombotic complications, such as the development of bowel ischemia – which is associated with a 30-day mortality rate of 20% 6 – and the risk of hemorrhagic complications, such as gastrointestinal or variceal bleeding, which can be triggered by portal hypertension, hypersplenism and thrombocytopenia. 2 Furthermore, patients with underlying cancer or liver cirrhosis simultaneously have a prothrombotic predisposition and a further increased risk of bleeding.
The 2012 guidelines of the American College of Chest Physicians (ACCP) recommend anticoagulation in patients with symptomatic SVT, while they suggest no anticoagulation in patients with asymptomatic incidentally detected SVT. 44 However, in the latter, anticoagulation is encouraged in the presence of other factors, such as acute extensive thrombosis, thrombosis progression, or active cancer. 44 Data from an international registry showed that the anticoagulant treatment in SVT patients was a protective factor both for the development of recurrent thrombosis and for bleeding complications, 35 and that in real life clinical practice 62% of incidentally detected SVT received anticoagulant treatment. 7 Among incidentally detected SVT, the use of anticoagulant treatment was more common in those with previous VTE, recent abdominal surgery, MPN or multiple veins thrombosis, and less common in those with hepatic cirrhosis or thrombocytopenia; 7 thus, we suggest a decision be made on an individual basis and considering also the risk of bleeding.
According to the ACCP guidelines, after the initial treatment with heparin, the majority of patients with SVT are potential candidates for vitamin K antagonists (VKAs), while continuous parenteral treatment is suggested if active cancer, hepatic disease or thrombocytopenia is present. 44 Data from real life clinical practice show that approximately two-thirds of anticoagulated patients are switched to VKAs. 3 Factors associated with the long-term use of parenteral anticoagulation were incidentally detected SVT and bleeding risk factors (such as solid cancer, liver cirrhosis, anemia and thrombocytopenia), while patients of a younger age with multiple veins thrombosis, unprovoked SVT or SVT secondary to permanent risk factors (such as MPN) were more frequently switched to VKAs. 3 An analysis of patients with SVT on VKA treatment followed by anticoagulation clinics showed that VKAs are associated with a low rate of major bleeding complications (1.24 per 100 patient-years, 95% CI: 0.75–2.06). 45
The direct oral anticoagulants (DOACs) have not been extensively evaluated yet in patients with SVT and, therefore, they are not included in current recommendations. Several case reports46–48 and a series of 94 patients treated with different DOACs at different dosages, of whom 75% were for SVT, 49 provide some preliminary data on the efficacy and safety of these drugs in SVT patients, showing a low rate of complications. There is an ongoing pilot study assessing the safety and efficacy of rivaroxaban in patients with acute SVT (NCT02627053) and a randomized controlled trial comparing rivaroxaban with no treatment for the prevention of recurrent thrombosis in patients with chronic PVT (NCT02555111).
The treatment duration according to ACCP guidelines is based on criteria similar to usual site VTE: 3 months are suggested in patients with SVT secondary to transient risk factors (such as surgery, abdominal infections or hormonal treatment), while extended treatment is suggested in patients with unprovoked SVT or SVT secondary to persistent risk factors (such as MPN) and low bleeding risk. 44 The guidelines of the American Association for the Study of Liver Disease (AASLD) suggest long-term anticoagulant treatment also for patients with MVT or BCS in the absence of contraindications. 27 The Baveno VI consensus recommend a more conservative approach, with anticoagulation given for at least 6 months. 34 Data from patients treated with VKAs show that, after discontinuation of the anticoagulant treatment, patients with SVT secondary to persistent risk factors had a higher risk of recurrent thrombotic events (10.2 per 100 patient-years, 95% CI: 4.2–24.4), followed by patients with unprovoked SVT (2.4 per 100 patient-years, 95% CI: 0.6–9.6), while the risk was very low in patients with SVT secondary to transient risk factors. 50 In particular, liver cirrhosis was associated with an approximately eightfold increased risk of recurrent thrombotic events. 50 Recommendations from current guidelines about anticoagulant treatment in SVT are summarized in Table 3, while the overall approach to SVT is represented in Figure 2.
Summary of current guidelines for the anticoagulant treatment of splanchnic and cerebral vein thrombosis.
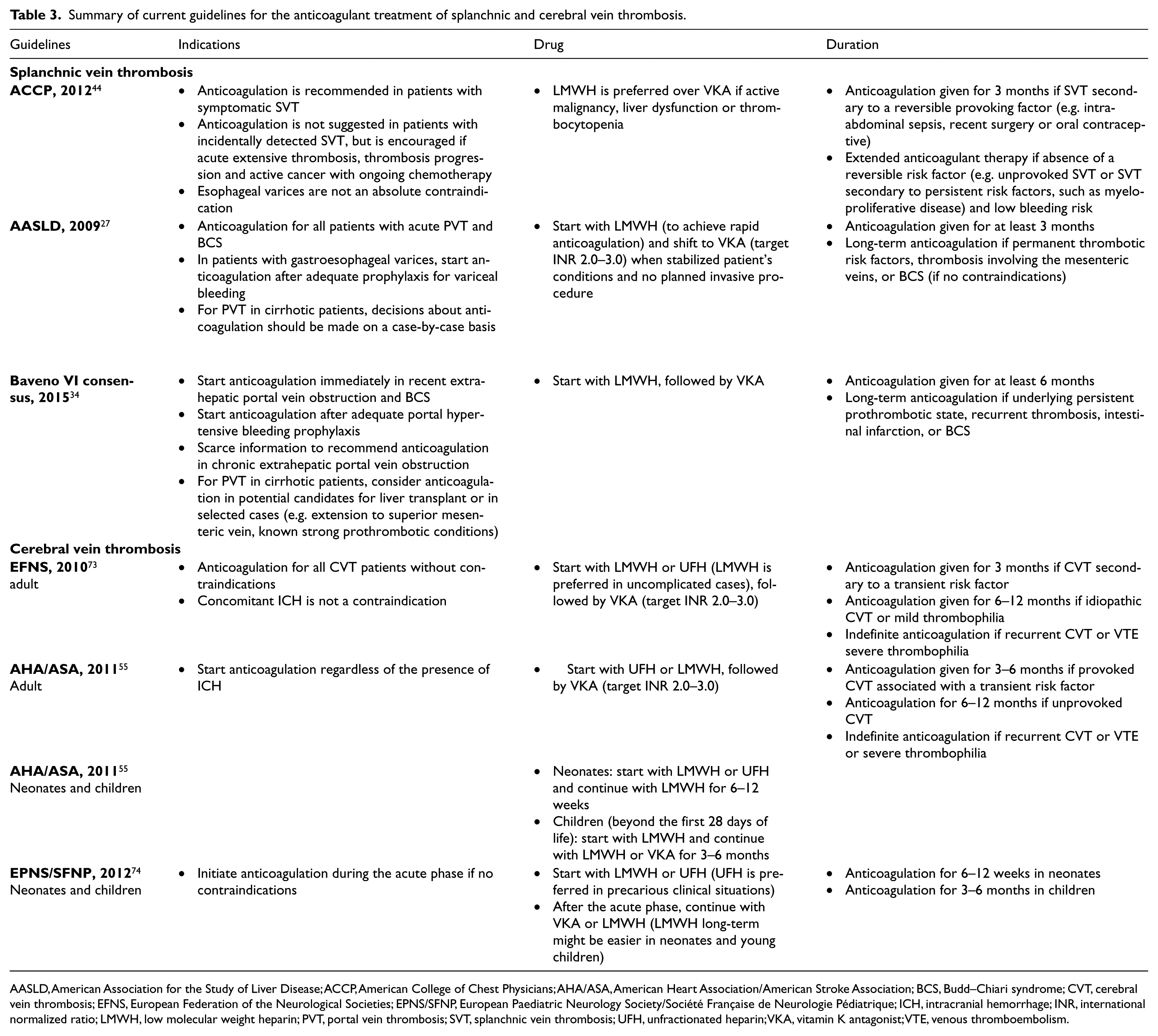
AASLD, American Association for the Study of Liver Disease; ACCP, American College of Chest Physicians; AHA/ASA, American Heart Association/American Stroke Association; BCS, Budd–Chiari syndrome; CVT, cerebral vein thrombosis; EFNS, European Federation of the Neurological Societies; EPNS/SFNP, European Paediatric Neurology Society/Société Française de Neurologie Pédiatrique; ICH, intracranial hemorrhage; INR, international normalized ratio; LMWH, low molecular weight heparin; PVT, portal vein thrombosis; SVT, splanchnic vein thrombosis; UFH, unfractionated heparin; VKA, vitamin K antagonist; VTE, venous thromboembolism.
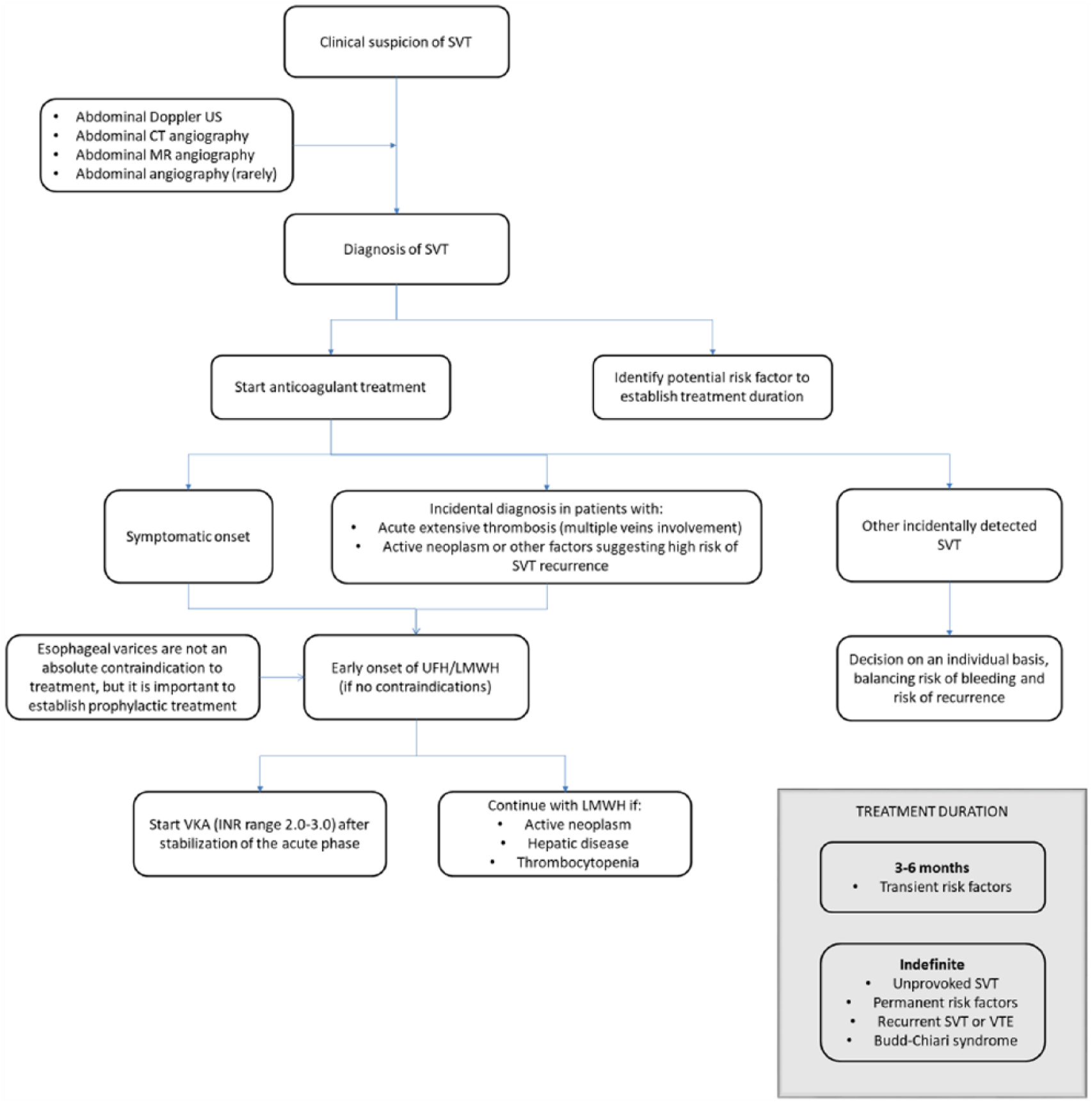
Approach to splanchnic vein thrombosis.
Patients with SVT secondary to liver cirrhosis are a special subgroup of patients, showing a particularly high incidence of both thrombotic and bleeding complications. On one hand, they have a reduced synthesis of coagulation factors, low platelet count and presence of esophageal varices; on the other hand, the prothrombotic predisposition is known to increase with the severity of the hepatic disease. 51 Preliminary results from a recently published meta-analysis showed that the anticoagulant treatment obtained high rates of complete portal vein recanalization and reduced the probability of thrombosis progression, with a small incidence of major bleeding complications. 52 However, lacking direct comparative data between anticoagulated and not anticoagulated cirrhotic patients, these data should be interpreted with caution. Nonetheless, all guidelines agree that esophageal varices do not represent an absolute contraindication to the anticoagulant treatment, but it is crucial to establish prophylactic treatment with beta-blockers or endoscopic band ligation.27,34,44
Finally, BCS is a particularly severe manifestation of SVT, often necessitating different lines of treatment. In addition to early anticoagulation, medical therapy can require the addition of diuretics, salt restriction and paracentesis. If there is clinical deterioration, invasive procedures (such as local thrombolysis, angioplasty with stent, placement of a surgical porto-systemic shunt or a transjugular intrahepatic porto-systemic shunt) should be considered. In case of failure, patients are candidates for liver transplantation. 33
Cerebral vein thrombosis
CVT encompasses thrombosis of the cerebral veins (cortical or deep veins) and thrombosis of the dural venous sinuses (such as superior sagittal, lateral or transverse, straight, sigmoid, and cavernous sinuses). CVT has an estimated annual incidence of three to four cases per million adults and five to seven cases per million children.53,54 Furthermore, CVT is the cause of 0.5–1% of strokes. 55 However, the diagnosis of CVT has increased recently due to the improvement of highly sensitive and non-invasive neuroimaging. CVT usually occurs in the 40s and shows a clear prevalence of females (approximately 75% of cases).56,57
Clinical manifestations and diagnosis
Clinical manifestations of CVT are variable and not specific, and they can resemble other cerebral diseases. The most common symptoms are: headache (80–90% of patients); focal or generalized seizures (40%); papilledema (30%), which can carry also diplopia and visual loss; less common symptoms are altered consciousness, focal neurological deficits, dysarthria or aphasia.53,55 Furthermore, there are some differences in the pathogenesis and clinical presentation of thrombosis in the cerebral veins and thrombosis in the dural venous sinuses.
Signs and symptoms of a thrombosis in the cerebral veins are mainly due to cerebral edema: thrombosis of deep cerebral veins can manifest with coma, altered mental status and paraparesis, while thrombosis of the cortical veins can manifest with seizures or sensitive motor deficits. 58
Signs and symptoms of a thrombosis in the dural venous sinuses are mainly due to intracranial hypertension, such as headache, papilledema and vomiting. However, there are also some differences according to the location – for instance, hemiparesis or seizures (thrombosis of the superior sagittal sinus); aphasia (thrombosis of the left lateral sinus); periorbital edema, orbital pain, proptosis, and paralysis of eye movements (thrombosis of the cavernous sinus); and encephalopathy (thrombosis of the straight sinus).53,55,58
The role of d-dimer in CVT diagnosis is still uncertain. Although d-dimer has been reported to have a sensitivity of 93.9% and a specificity of 89.7%, it can provide false negative results in patients with limited sinus involvement, isolated headache or longstanding symptoms. 59 Therefore, the diagnosis of CVT relies on different neuroimaging tests: cerebral CT and MR angiography with specific protocols for the venous phase and for the area of interest.
The first line investigation is CT angiography, since it is available also in emergency situations and it can be helpful to rule out other diseases (such as stroke, brain cancer or abscess). CT angiography can show the intraluminal filling defects due to thrombus in a venous sinus or in a cerebral vein (the latter is also known as the empty delta sign).60,61 Other signs, like the hyperdense thrombosed cortical vein (the cord sign) or the hyperdense thrombosed superior sagittal sinus (the dense triangle sign), are rare but they can also be seen on an unenhanced CT. 60 CT can be normal in up to 25–30% of patients with CVT.60,61
MR is currently the gold standard for the diagnosis of CVT. MR is better than CT in detecting thrombosis in the cerebral veins; however, it is hampered by its limited availability and the long time needed for the scan.62,63 It is the combination of plain MR and MR angiography that confirms the diagnosis of CVT. In fact, plain MR shows the abnormal signal in a venous sinus or cerebral vein, but is limited by flow artifacts which can result in false positive results; while MR angiography shows the absence of flow, but is not able to differentiate between thrombosis and anatomical variants.60,63,64 The thrombus has a different appearance on MR according to its evolution: in the first 5 days (acute phase) it is isointense on T1-weighted images and hypointense on T2-weighted images; in the next 10 days (subacute phase) it is hyperintense on both T1 and T2-weighted images; afterwards, the thrombus signal is progressively reduced and the appearance depends on the recanalization or organization of the thrombus.61,65
Intra-arterial angiography was previously the gold standard for CVT diagnosis, since its spatial and temporal resolution are better than CT or MR. 66 However, being an invasive examination, nowadays it is performed only in particular situations, such as when CT and MR provide inconclusive results or in order to perform thrombolysis.
Assessment of risk factors
Several risk factors for CVT are specific to the female sex, thus explaining why 75% of CVT occur in women.56,57 Oral contraceptives are reported in 40–50% of women with CVT, pregnancy (especially during the third trimester) or puerperium in 10–20%, and hormonal replacement therapy in 3–4%.56,57,67
Another common risk factors in adults is thrombophilia (35–40% of cases).56,57 A meta-analysis of case–control studies reported a three times increased risk of CVT with factor V Leiden, nine times with prothrombin G20210A mutation, and four times with hyperhomocysteinemia. 68 Furthermore, few studies also reported an association between CVT and other thrombophilic mutations (deficiency of protein C, protein S, antithrombin and antiphospholipid syndrome). 68 The association of thrombophilic mutations with the use of oral contraceptives can further increase the risk of CVT. 69 Despite the strong association between inherited thrombophilia and CVT, the clinical relevance on the risk of recurrent VTE is still a matter of debate and therefore routine testing in all CVT patients is not suggested. 70
It was recently reported that CVT can be the first manifestation of a MPN. In fact, the JAK2 V617F mutation was found in 6.6% of patients with CVT. 71 However, the association between CVT and MPN remains controversial: the prevalence of CVT in patients with MPN is less than 1%, and, vice versa, the prevalence of MPN in patients with CVT is approximately 4%. 72
Local risk factors for CVT have also been reported, such as mechanical causes (e.g. head injury, central venous catheter placed into the jugular vein, or neurosurgical procedures, reported in 3–5%) or infections (e.g. otitis, mastoiditis, sinusitis, meningitis, reported in about 10% of cases). In particular, otitis and mastoiditis can provoke thrombosis of the adjacent sigmoid and transverse venous sinuses, while sinusitis of the ethmoid and sphenoid paranasal sinuses can provoke thrombosis in the cavernous venous sinuses. 53 Although reported only in a minority of patients (around 2%), central nervous system neoplasms are another possible local risk factor. 57 Owing to the low prevalence of malignancy in CVT patients, routine screening for malignancy in all CVT patients is not suggested.
The most common risk factors in children are: thrombophilia (32%), dehydration (25%), perinatal complications (24%) and infections (18%). 54
Finally, 15–20% of CVT occur without predisposing risk factors and are classified as unprovoked. 53
Anticoagulant treatment
Anticoagulant treatment has a crucial role in CVT, with the aim to avoid thrombus extension and to favor local resolution. However, possible complications include the development of intracranial hemorrhage (ICH) or other site major bleeding. In order to establish the most appropriate treatment, the etiology of the thrombosis (unprovoked vs provoked) as well as the severity of clinical presentation (number of involved veins, neurological sequelae) should be kept in consideration.
The 2010 guidelines of the European Federation of the Neurological Societies (EFNS) and the 2011 guidelines of the American Heart Association/American Stroke Association (AHA/ASA) recommend starting the anticoagulant treatment with dose-adjusted intravenous unfractionated heparin (UFH) or body-weight adjusted subcutaneous LMWH, followed by VKAs with an international normalized ratio (INR) target range of 2.0–3.0.55,73 The 2012 guidelines of the European Paediatric Neurology Society/Société Française de Neurologie Pédiatrique (EPNS/SFNP) also recommend starting during the acute phase in neonates and children with heparin, which can be followed by VKAs, although monitoring in this population might be more difficult. 74 Current guideline recommendations about anticoagulant treatment in CVT are summarized in Table 3, while the overall approach to CVT is represented in Figure 3.
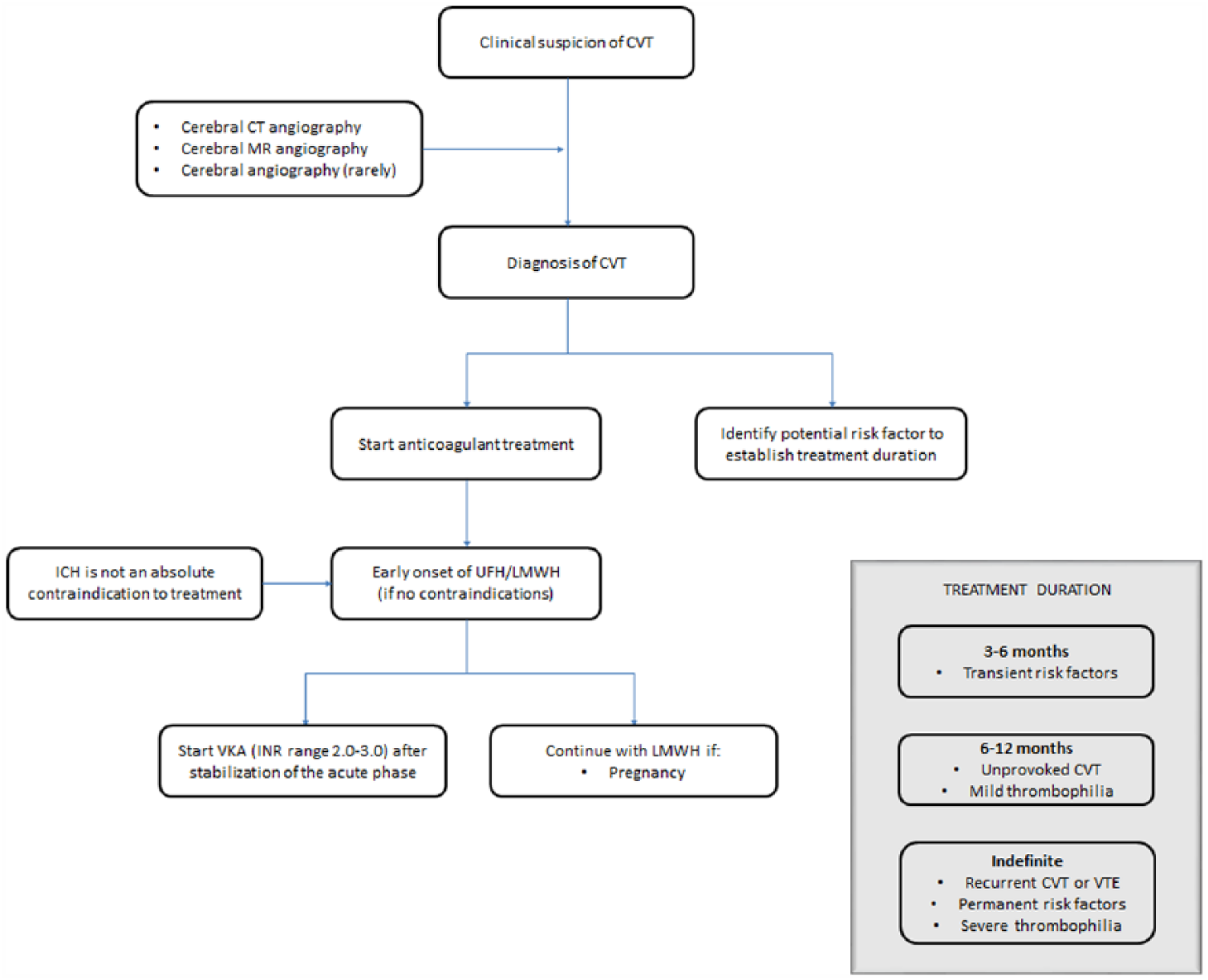
Approach to cerebral vein thrombosis.
There are only two small randomized controlled trials that have evaluated the effectiveness and safety of heparin, either UFH or LMWH, for the treatment of CVT. 75 Pooled results showed that the anticoagulant treatment, compared to control, was associated with a trend towards reduced risk of death or dependence, without any new symptomatic ICH observed during treatment. 75 Data from cohort studies show that 83–85% of patients are anticoagulated during the acute phase.56,57
A concomitant ICH is reported in 25–39% of CVT patients,56,57 but guidelines are concordant that it should not be an absolute contraindication to anticoagulant treatment.55,73 In these patients experts’ consensus recommend administering anticoagulants with a short half-life (such as UFH or LMWH) and to postpone the introduction of VKA after stabilization of the clinical and neuroradiological conditions. 76 The DOACs have not been extensively evaluated in CVT patients and, therefore, they are not included in current recommendations, but a number of case reports or case series have been published. An ongoing randomized clinical trial is comparing dabigatran etexilate with warfarin for the secondary prevention of CVT (NCT02913326).
Treatment duration depends on the etiology of the thrombosis: CVT secondary to transient risk factors should be treated for at least 3 months; unprovoked CVT for 6–12 months; whereas an indefinite treatment duration is suggested for recurrent CVT or in the presence of severe thrombophilia.55,73 The recommended treatment duration is 6–12 weeks for infants and 3–6 months for children. 74 The risk of recurrent VTE after CVT was reported to be approximately 2.4 per 100 patient-years, with the majority of events occurring after anticoagulant treatment discontinuation (3.5 per 100 patient-years). 56 The following risk factors for thrombosis recurrence have been identified: male sex,77,78 severe thrombophilia, 77 previous VTE, 56 and MPN. 78 Recanalization rates are high in CVT patients and usually occur within the first few months after the index event.79,80 However, the association between recanalization and clinical outcomes is still debated;79,80 therefore, recanalization status is currently not evaluated when deciding on the anticoagulation duration.
Asymptomatic incidentally detected CVT cases are less common than incidentally detected SVT, and there are no specific studies or recommendations available in the literature; therefore we suggest a similar approach to symptomatic CVT, taking into consideration the risks and benefits of the anticoagulant treatment.
Systemic or local thrombolytic therapy in cohort studies was associated with a high risk of ICH (7.6%) and high mortality rates (9.2%, half of which were due to the development or worsening of ICH). 81 Therefore, thrombolytic therapy should be considered only for patients with clinical deterioration despite adequate anticoagulant treatment and without any alternative cause of deterioration.55,73
Finally, other treatments might be needed according to the clinical conditions (such as antiepileptic drugs in patients with seizures; diuretics, lumbar puncture, ventriculo-peritoneal shunt or decompressive surgery in patients with severe intracranial hypertension; antibiotics in patients with underlying infections).55,73
Conclusion
The approach to patients with SVT or CVT can be more difficult than usual site VTE due to the lower incidence rates of unusual site VTE the heterogeneous and non-specific clinical manifestations, and the uncertainties about the optimal anticoagulant treatment initiation and duration.
The diagnosis of SVT and CVT relies mainly on imaging tests (such as Doppler US, CT and MR), considering the lack of specific clinical algorithms and the limited role of d-dimer in these diseases. Identifying potential thrombotic risk factors and understanding the pathophysiology of SVT and CVT are essential in order to establish the most appropriate anticoagulant treatment. Conventional anticoagulant therapies (such as UFH, LMWH and VKA) are still the main options, since novel direct oral anticoagulants have not been extensively evaluated yet in these patients. Parenteral anticoagulation is usually administered during the acute phase and most patients are switched to VKA after clinical stabilization. Prolonged LMWH can be considered in particular situations (such as active neoplasm, hepatic disease, thrombocytopenia or pregnancy). Current guidelines suggest basing the anticoagulant treatment duration on criteria similar to usual site VTE: 3–6 months for patients with SVT or CVT provoked by transient risk factors; longer than 6 months and often indefinite for patients with permanent risk factors, unprovoked thrombosis, or recurrent VTE. However, since SVT and CVT are heterogeneous diseases, which include also a special subgroup of patients (such as cirrhotic patients with SVT and severely thrombophilic patients with CVT), and they carry a high risk of life-threatening bleeding complications (such as variceal bleeding and ICH, respectively), treatment initiation and duration should surely be individualized.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: WA has received a research grant from Bayer to support a clinical study in patients with splanchnic vein thrombosis; NR has no relevant conflicts to declare in relation to this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.