
Abstract
Pulmonary Embolism Response Teams (PERTs) have emerged to provide rapid multidisciplinary assessment and treatment of PE patients. However, descriptive institutional experience and preliminary outcomes data from such teams are sparse. PERT activations were identified through a retrospective review. Only confirmed submassive or massive PEs were included in the data analysis. In addition to baseline variables, the therapeutic intervention, length of stay (LOS), in-hospital mortality, and bleeding rate/severity were recorded. A total of 124 PERT activations occurred over 20 months: 43 in the first 10 months and 81 in the next 10. A total of 87 submassive (90.8%) and massive (9.2%) PE patients were included. The median age was 65 (51–75 IQR) years. Catheter-directed thrombolysis (CDT) was administered to 25 patients, systemic thrombolysis (ST) to six, and anticoagulation alone (AC) to 54. The median ICU stay and overall LOS were 6 (3–10 IQR) and 7 (4–14 IQR) days, respectively, with no association with any variables except a brain natriuretic peptide (BNP) >100 pg/mL (p=0.008 ICU LOS; p=0.047 overall LOS). Twelve patients (13.7%) died in the hospital, nine of whom had metastatic or brain cancer, with a median overall LOS of 13 (11–17 IQR) days. There were five major bleeds: one in the CDT group, one in the ST group, and three in the AC group. Overall, (1) PERT activations increased after the first 10 months; (2) BNP >100 pg/mL was associated with a longer LOS; (3) rates of mortality and bleeding did not correlate with treatment; and (4) the majority of in-hospital deaths occurred in patients with advanced cancer.
Keywords
Introduction
Pulmonary embolism (PE) is the third leading cause of cardiovascular mortality in the United States, behind only stroke and myocardial infarction. 1 For these latter conditions, institutions have employed rapid response teams, which coordinate the management and intervention for these critical and complicated patients. Similarly, in the past 5 years, Pulmonary Embolism Response Teams, or PERTs, have emerged to rapidly triage PE patients.2–4
PE management is complicated by the varying presentations, treatment risks, paucity of data for certain interventions and sub-conditions, and uncertain guideline recommendations. While future clinical trials and registries will address some of these issues, critical decision-making will continue to be in the hands of local experts that comprise such a team.
These teams have an opportunity to collect relevant data that can inform treatment decisions and algorithms, hospital policy, and future research. While there are numerous retrospective and prospective studies examining a specific treatment for severe PE (e.g. catheter-directed therapy, systemic thrombolysis, surgical embolectomy),5–7 there are few reports on the experience of individual PERTs. We accordingly created a retrospective database of submassive and massive PE patients triaged by our PERT and report on our process and in-hospital outcomes.
Methods
PERT and operations
The Weill Cornell Medical College (WCMC) PERT is comprised of representatives from Cardiology, Cardiothoracic Surgery, Interventional Radiology, and Pulmonary/Critical Care. Activations occur by way of a pager (x12568 or x1CLOT) that is known throughout the hospital system. The pager is carried by the Pulmonary/Critical Care consultative service, as it takes in house calls 24 hours/day, 7 days/week. The Pulmonary/Critical Care physician examines the patient and then determines whether multidisciplinary decision-making is necessary. If the Pulmonary/Critical Care team deems that the PE is low risk, no other team members are involved. If the PE is deemed to be submassive or massive, consults to Interventional Radiology and Cardiothoracic Surgery are initiated. Consulting teams place a consult to ‘Pulmonary Embolism Advanced Care’, and the formal recommendation from the PERT is entered under this consult as an electronic note. These notes were queried for inclusion in this retrospective registry.
The WCMC algorithm for therapeutic escalation (catheter-directed thrombolysis, systemic thrombolysis, surgical embolectomy) has been previously described. 4 Briefly, prior to creation of the PERT, there was no consensus among providers caring for PE, nor was there a treatment escalation pathway. The members of the WCMC PERT reviewed the literature and developed algorithms for treatment escalation. We agreed the following factors would prompt consideration for therapeutic escalation: (1) massive PE (hypotension) or (2) submassive PE with a concerning clinical exam (tachycardia >100 beats/minute, pallor, respiratory distress, signs of hypoperfusion), elevated lactate, syncope, severe right ventricle dysfunction by echocardiography, severe exertional limitation (unable to ambulate or marked increase in tachycardia and/or worsening hypoxia with ambulation), or poor clinical trajectory (i.e. worsening or non-improving course on anticoagulation).
Subjects
This retrospective data review was approved by the institutional review board. We identified 124 patients who received formal consultations from our PERT between 1 January 2013 and 31 August 2014. After this time, patients were consented for a prospective registry; thus, the last patients included in this retrospective analysis were treated by August 2014. This list was queried to identify which of these patients met the criteria for massive or submassive PE, based on the presence of hypotension (massive) or right heart dysfunction and/or biomarker elevation without hypotension (submassive). Right heart dysfunction was defined as right heart dilation, hypokinesis, or a systolic pulmonary artery pressure greater than 35 mmHg on echocardiography. Biomarker elevation was defined by a positive troponin assay or a brain natriuretic peptide (BNP) >100 pg/mL. 8 A total of 87 patients met the criteria above to be included in our analysis (Figure 1). Baseline data are listed in Table 1. The simplified Pulmonary Embolism Severity Index (sPESI), used in PE risk stratification in the European Society of Cardiology PE guidance document, 9 was calculated according to the original publication. 10
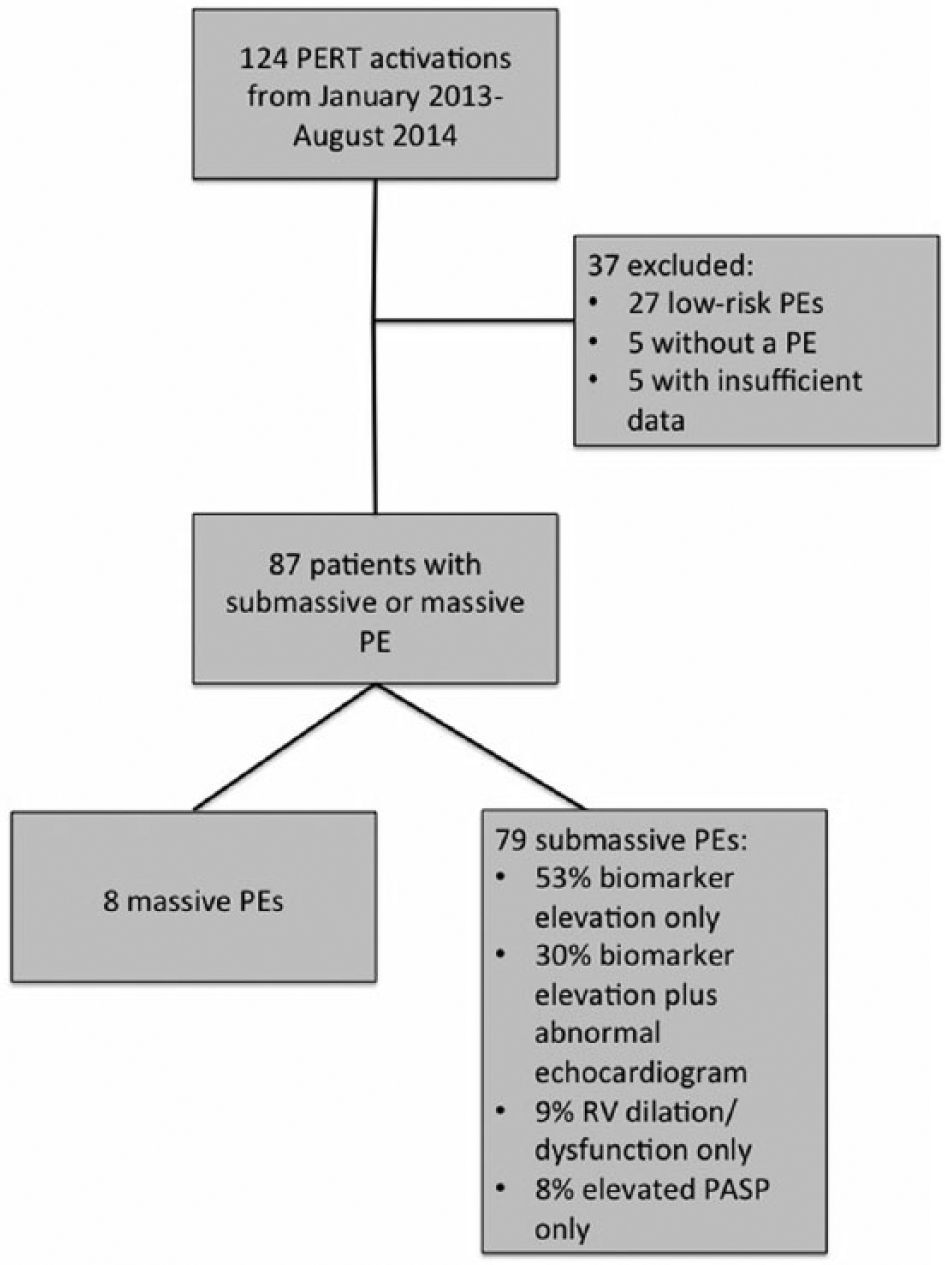
Flow diagram of the 124 activations that occurred between 1 January 2013 and 31 August 2014. PERT, Pulmonary Embolism Response Team; PE, pulmonary embolism; RV, right ventricle; PASP, pulmonary artery systolic pressure.
Baseline characteristics and outcomes.
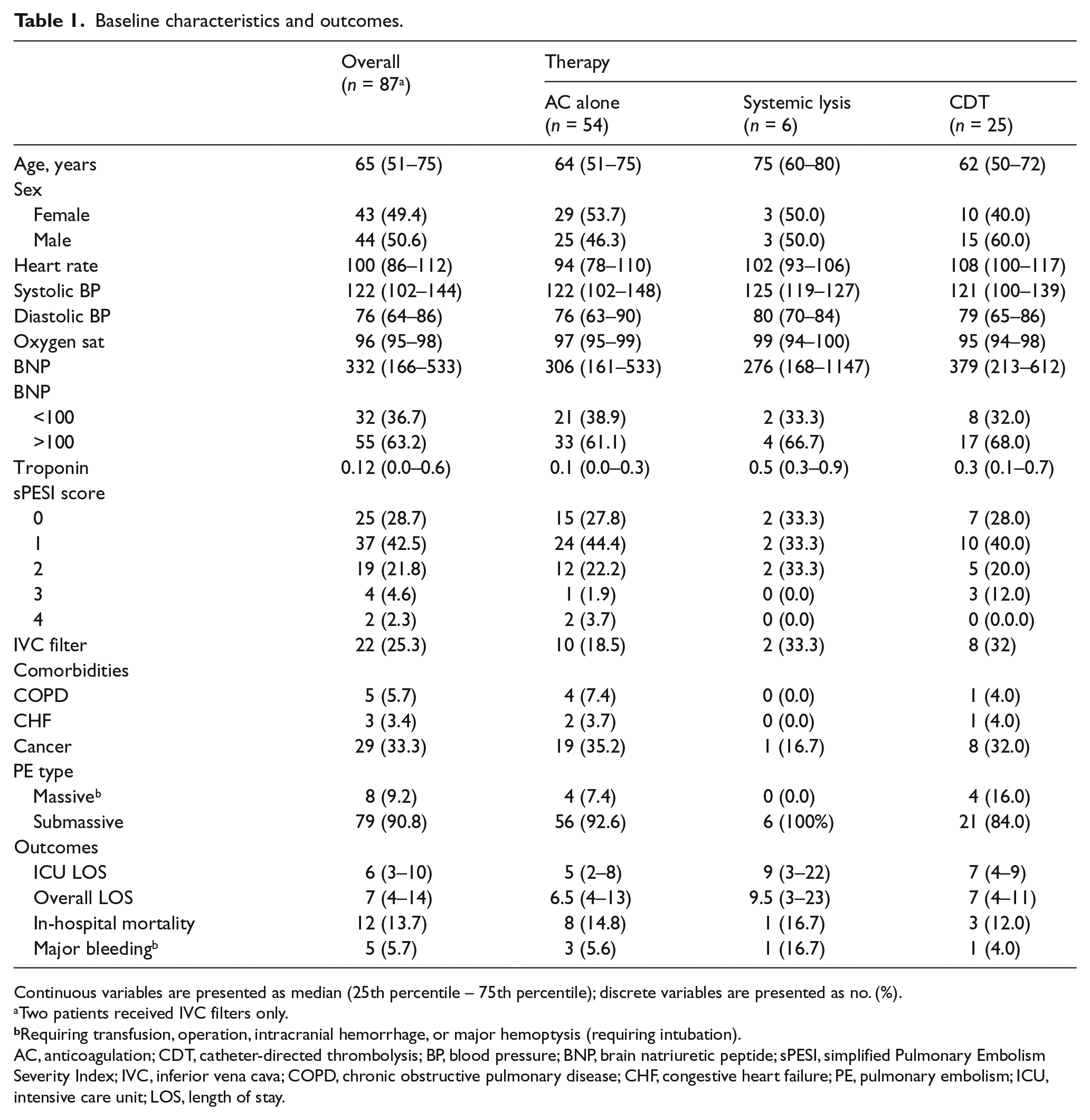
Continuous variables are presented as median (25th percentile – 75th percentile); discrete variables are presented as no. (%).
Two patients received IVC filters only.
Requiring transfusion, operation, intracranial hemorrhage, or major hemoptysis (requiring intubation).
AC, anticoagulation; CDT, catheter-directed thrombolysis; BP, blood pressure; BNP, brain natriuretic peptide; sPESI, simplified Pulmonary Embolism Severity Index; IVC, inferior vena cava; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; PE, pulmonary embolism; ICU, intensive care unit; LOS, length of stay.
Interventions
Anticoagulation alone was defined by the sole administration of one of the following anticoagulants: heparin, warfarin, enoxaparin, dalteparin, fondaparinux, rivaroxaban, and/or apixaban. Systemic thrombolysis (ST) was defined as the administration of 100 mg of recombinant tissue plasminogen activator (rt-PA) infused intravenously over 2 hours or as a bolus in the setting of cardiac arrest. Catheter-directed thrombolysis (CDT) was defined as the placement of multi-sidehole infusion catheters within pulmonary artery thrombus, through which rt-PA was administered.6,11 Both ultrasound-assisted catheters (Ekowave; BTG Corp., Conshohocken, PA) and standard infusion catheters (Unifuse; Angiodynamics, Latham, MA, USA or Cragg-McNamara, Medtronic, Minneapolis, MN) were employed. We administered 18–24 mg of rt-PA at a total dose of 1 mg/hour (0.5mg/hour/catheter for two catheters) through the catheter(s), with concomitant infusion of subtherapeutic heparin (goal partial thromboplastin time (PTT) <2 times the institutional norm). Mechanical techniques (thrombus maceration) were used in a single patient who became hypotensive upon induction of anesthesia; the rest of the patients undergoing CDT received thrombolytic drug infusion only, without maceration or aspiration. The rate of inferior vena cava (IVC) filtration was also recorded.
Outcomes
The following outcomes were obtained from the electronic medical record: length of stay (LOS) in the intensive care unit (ICU), overall LOS, in-hospital mortality, major bleeding (defined as bleeding requiring transfusion, major hemoptysis requiring intubation, intracranial hemorrhage, or operation), and procedural complications.
Statistical analysis
Descriptive statistics (i.e. mean, standard deviation, median, range, frequency, and percent) for demographic and clinical variables were reported to characterize the entire study cohort and by the following subgroups: anticoagulation-only, systemic lysis, and CDT (Table 1). A multivariable negative-binomial regression model was used to control for the following variables that would potentially affect the overall LOS and ICU LOS: the performance of CDT, heart rate on admission, O2 saturation, sPESI score (0 vs 1–4), BNP (⩾100 vs ⩽ 100 pg/mL), and troponin (positive or negative). All p-values are two-sided with statistical significance evaluated at the 0.05 alpha level. All analyses were performed in SAS software, Version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
PERT operations and activations
Of the 124 activations, 43 occurred in the first 10 months (January to October 2013) and 81 occurred in the next 10 months (November 2013 to August 2014). January 2014 had the most activations (15) followed by July 2014 (11) and November 2013, December 2013, and August 2014 (nine apiece) (Figure 2A). During the study, 40% of the CDT interventions were performed in a 4-month period from October 2013 to January 2014, with an additional spike of three cases in June 2014 (Figure 2B). One CDT case was performed in the 20 months preceding the formation of the PERT based on a query of the electronic record.
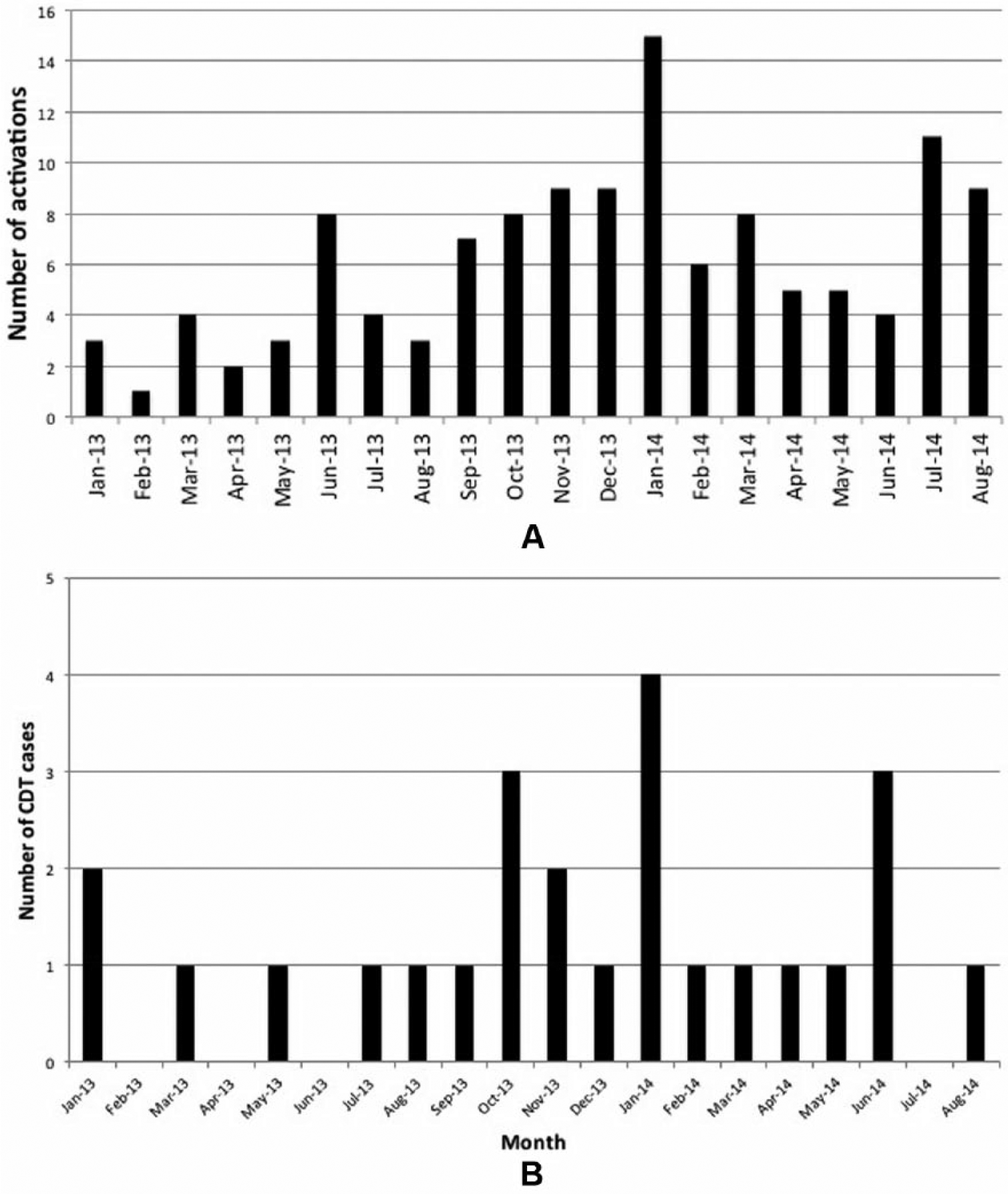
(A) Number of activations per month over the 20-month study period. (B) Number of catheter-directed thrombolysis (CDT) cases per month over the 20-month study period.
Baseline data
The overall cohort was 49.4% female and averaged 65 years of age (Table 1). No significant differences in age, sex, blood pressure, oxygen saturation, biomarkers, or sPESI score were identified between patients who received CDT and those who received anticoagulation. Patients who underwent CDT had a significantly faster mean heart rate at admission than those who received anticoagulation (108 beats/min, IQR 100–117 beats/min vs 94 beats/min IQR 78–110 beats/min, p = 0.006). The majority of patients had an sPESI score of 1 or greater. Relatively few had known underlying chronic obstructive pulmonary disease (COPD) or congestive heart failure (CHF), although a large minority carried a diagnosis of cancer. A total of 90.8% of patients fit in the submassive PE category, and the rest were in the massive PE category. There was no association between the rate of IVC filter placement and treatment allocation. Two patients received IVC filtration only.
Outcomes (length of stay, death, bleeding, procedural complications)
The median ICU stay and overall LOS were 6 and 7 days, respectively. Patients who underwent CDT did not differ from those who did not in median ICU LOS (7 vs 5 days, p = 0.1036) or overall LOS (7 vs 6.5 days, p = 0.8980). Negative binomial regression results (incidence rate ratio (IRR), standard error, and p-value) are shown in Tables 2 and 3. An elevated BNP (⩾100 pg/mL) was associated with an 88% increase in ICU LOS (IRR = 1.88 (1.2, 3.0), p = 0.008) and a 50% increase in overall LOS (IRR = 1.5 (1.01, 2.2), p = 0.047) after controlling for CDT, heart rate, oxygen saturation, sPESI score, and troponin. None of the other variables showed an association with LOS.
Negative binomial regression predicting intensive care unit length of stay.
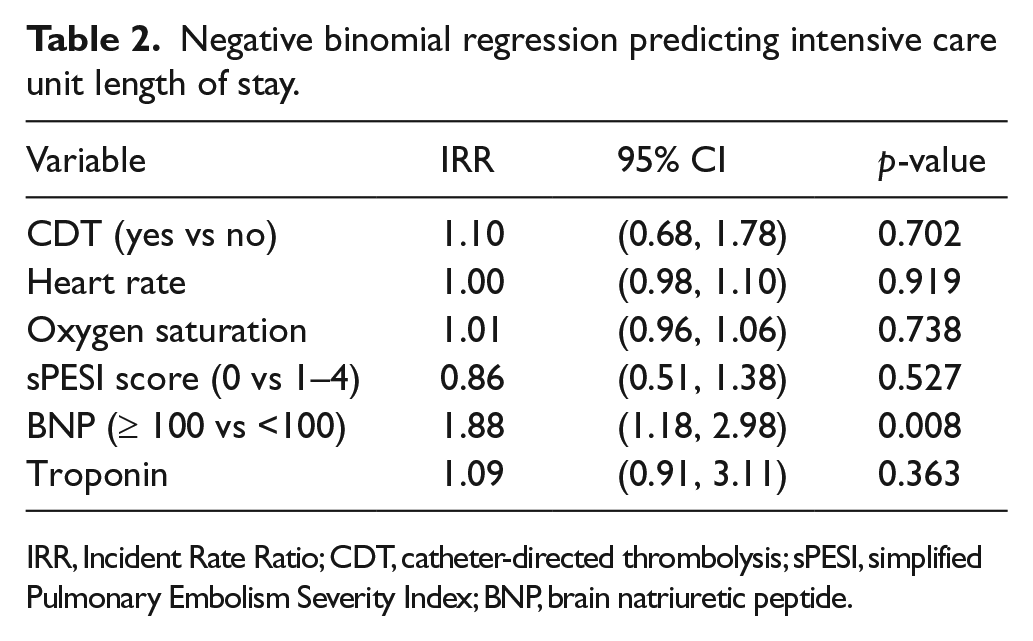
IRR, Incident Rate Ratio; CDT, catheter-directed thrombolysis; sPESI, simplified Pulmonary Embolism Severity Index; BNP, brain natriuretic peptide.
Negative binomial regression predicting overall length of stay.
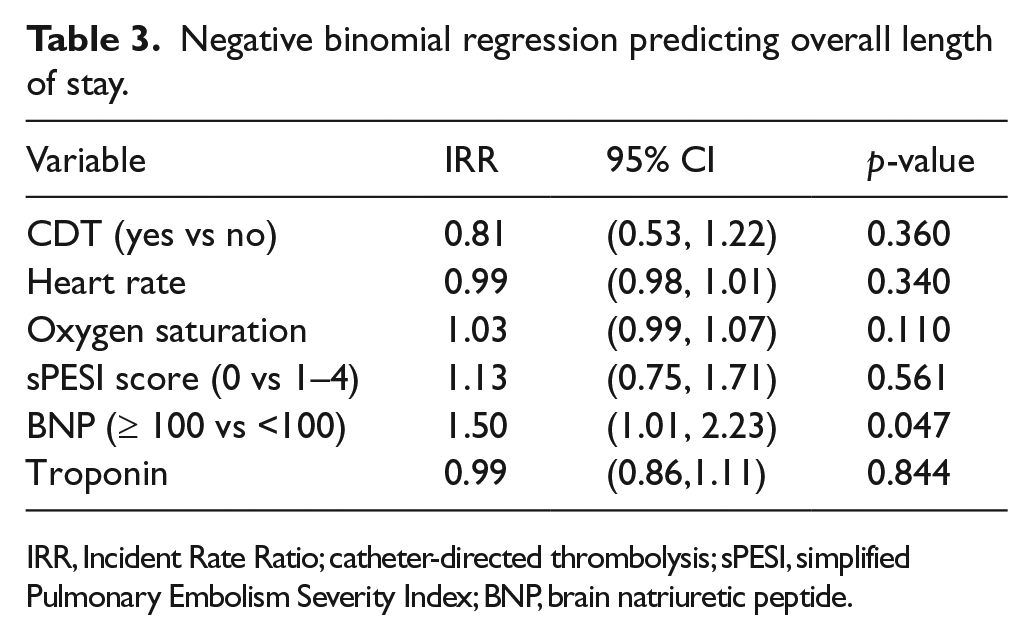
IRR, Incident Rate Ratio; catheter-directed thrombolysis; sPESI, simplified Pulmonary Embolism Severity Index; BNP, brain natriuretic peptide.
Twelve patients died, and there was no significant mortality difference based on treatment allocation. Seven out of eight of those who died in the hospital without thrombolytic therapy carried diagnoses of metastatic cancer or primary brain cancer. The single mortality in the ST group was attributed to metastatic cancer. One of the patients who underwent CDT had a recurrent fatal massive PE 1 week after the CDT procedure. At the time of CDT, he received an IVC filter. At 23 hours into the CDT infusion, he suffered an episode of major hemoptysis requiring intubation and cessation of anticoagulation. A second borderline submassive/massive CDT patient became hypotensive upon induction of general anesthesia and progressed to cardiopulmonary collapse, and catheter-directed measures were insufficient to rescue him. A third CDT patient was eventually diagnosed with severe chronic thromboembolic pulmonary hypertension and died of progressive cor pulmonale.
The overall rate of major bleeding was 5.7%, with one intracranial hemorrhage (subdural) in the ST group, one major hemoptysis in the CDT group requiring cessation of anticoagulation (patient described above), and three bleeds requiring transfusion in the AC alone group.
One vascular complication happened in the CDT group: a common femoral artery pseudoaneurysm was noted on follow up, likely due to inadvertent arterial puncture. This complication was successfully managed with a percutaneous thrombin injection.
Discussion
The first 20 months of the WCMC PERT saw 124 activations, out of which 87 were submassive or massive PEs. The initial 10 months, as expected, had fewer activations than the last 10, likely because of increased awareness and acceptance of the PERT. We did not ask consulting services to screen for submassive or massive PEs; rather, we encouraged them to activate the PERT if they were concerned about the patient’s clinical status and were either suspicious or had documentation of a PE. Thus, 27 activations were low-risk and five did not have PEs. Requiring more stringent activation criteria (e.g. patients must be submassive or massive) would be less resource intensive, but would risk missing some severe PEs.
The best mechanism to activate the PERT has not been firmly established. Having multiple disciplines quickly assess a patient takes significant coordination and organization. While some PERTs have tried to accomplish this conference via web-based applications, we chose to have the Pulmonary/Critical Care service perform the initial evaluation and consult the services individually as it deemed fit. It is unclear from our analysis whether this workflow delayed definitive therapy. However, for submassive PE, there is considerable debate regarding the timing of therapeutic escalation beyond anticoagulation, so it should not be routinely equated to acute stroke or myocardial infarction. Massive PE, on the other hand, is an immediate life-threatening condition that should be addressed promptly. Ultimately, comparisons between multiple PERT models will hopefully reveal the most effective, efficient, and clinically impactful process to address submassive and massive PE.
Acute care and hospital LOS are important metrics for hospitals. 12 Thus, interventions that significantly affect LOS, either positively or negatively, will receive increased attention. The literature shows that LOS following PE ranges from 5 to 11 days.13–17 If a PERT participates in the care of a patient for the duration of the hospitalization (which was not true for the WCMC PERT), then it can give discharge recommendations and potentially impact LOS. However, a PERT may also impact LOS based on how it manages severe PE. Our PERT employed CDT for a large percentage of cases, and we therefore analyzed the effect of CDT on LOS and found no association, in contrast to other studies that found a shorter LOS with CDT.18,19 We also found no correlation with severity at presentation (assessed by hemodynamics and the sPESI score). In fact, of the risk factors analyzed, only an elevated serum BNP was associated with increased LOS. Elevated BNP has been associated with a 10% risk of death and a 23% risk of an adverse clinical outcome, 20 although it has a low positive predictive value for early mortality. 21 It does, however, have a high negative predictive value for early mortality, 20 and the European Society of Cardiology guidelines suggest that patients with normal BNPs may be good candidates for earlier hospital discharge. 9 It is also notable that the ICU LOS is similar to the overall LOS, implying that patients are discharged from the hospital soon after leaving the ICU at our institution.
The in-hospital mortality of 13.7% is higher than the recently cited in-hospital unadjusted mortality of 5%. 22 The likely reason is enrichment of this study with patients with massive and submassive PE. Of the patients that died in our analysis, 75% had diagnoses of advanced cancer (metastatic or brain), and these patients had the longest LOS. It is unlikely that a PERT would significantly impact mortality or LOS in this population. Clinically significant bleeding rates in the CDT group were low, comparable to the anticoagulation group, and appear lower than the major bleeding rate seen in the SEATTLE II study (10%) 6 ; however, fewer patients were included in our analysis, and our study is insufficiently powered for a true comparison. Systemic thrombolysis was uncommonly used due to our institutional preference for CDT. One patient did have a subdural hemorrhage following ST.
The PERT model has been described previously, but data from PERTs have been relatively scarce. The largest series was published by Kabrhel et al., and included an analysis of 314 confirmed PEs, 72% of which were severe (submassive or massive). 23 A total of 11% were treated with thrombolytics (CDT or systemic), compared with 36% in our series. The overall 30-day mortality rate was 12%, though they do not explicitly report overall in-hospital mortality, making a comparison challenging. That being said, our in-hospital mortality of 13.7% is similar to the mortality rate in their series, in spite of 29% of their cohort being in the low-risk category. PERTs can expect, therefore, to contend with a relatively high mortality rate, given that they are frequently consulted for the more tenuous PE patients. Bleeding for CDT in their series was low (4% within 7 days of the procedure), similar to our analysis. They did not assess LOS. While similarities are present between the two analyses, the propensity for our institution to use CDT highlights the differences in practice that will likely be seen when comparing PERTs at different hospitals. In this regard, the clearest change in practice after creation of our PERT was the increase in CDT cases (1 vs 25 in the 20 months before and after PERT creation, respectively). Possible reasons include: (1) increased recognition and awareness of severe PE; (2) the inclusion of Interventional Radiology in the discussion of severe PE cases; and (3) the concern prior to the publication of the PEITHO trial 5 that submassive PE patients were at higher risk for short-term mortality.
Limitations
The study was limited by its retrospective nature, incomplete records in the electronic medical records, and lack of long-term follow up. As this study is a descriptive and retrospective examination of a single PERT, it cannot be used to recommend the routine implementation of a PERT for the management of PE. Moreover, the model of the WCMC PERT is different than other models, which may impact the generalizability of our outcomes. The study also focused on submassive and massive PE, so outcomes for low-risk PE were not assessed. Additionally, while the PERT model became widely accepted at WCMC, it is likely that some submassive and massive PE patients were not triaged and managed by the PERT and were missed by this analysis. Based on the number of beds at our institution, we expect 60 submassive PEs per year and 100 over 20 months. Our PERT managed 79 submassive PEs, so we may have been unaware of, or not consulted for, 20% of the submassive PEs that may have occurred over that time period. Given the lower number of activations in the first 10 months, the majority of the ‘missed’ severe PEs likely occurred in these months.
Conclusion
In conclusion, our retrospective analysis showed that: (1) activations increased 10–12 months after inception; (2) BNP >100 pg/mL was associated with a longer LOS; (3) rates of mortality and bleeding did not correlate with treatment allocation; and (4) the majority of in-hospital deaths occurred in patients with advanced cancer, and these patients had the longest LOS. Our data highlight the need for better comparative research to determine whether PERTs improve clinical outcomes and are cost-effective.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AS has a research grant from Penumbra, Inc., administered through the department of radiology at New York University.