
Abstract
Spontaneous isolated celiac or superior mesenteric artery (SMA) dissection (SICMAD) is a rare clinical entity. Not much is known about the natural history and appropriate treatment. We retrospectively queried a prospectively collected institutional radiology database for all patients diagnosed with SICMAD from 1990 to 2017. We identified 42 arteries in 40 patients (83.3% male), mean age 54.8 ± 10.9 years, consisting of 24 celiac arteries and 18 SMA. SMA lesions were longer than celiac lesions (5.15 ± 3.81 vs 2.38 ± 1.40 cm, p = 0.008). Thirty-one patients had follow-up; mean follow-up was 4.9 ± 4.8 years. Morphologic improvement was seen in 20 (48%) arteries. Sakamoto IV lesions were more likely to remodel (OR: 11.26, 95% CI: 1.13, 588.26, p = 0.039), and Sakamoto II lesions less likely to remodel (OR: 0, 95% CI: 0.00, 0.93, p = 0.05). Patients received an average of 2.35 scans during follow-up. Symptom resolution occurred in all symptomatic patients, and 16% of patients had recurrence of symptoms. Follow-up CT scans revealed a stable arterial diameter for the majority of patients. In conclusion, the majority of patients with SICMAD improve with medical therapy alone. Aneurysmal dilatation is uncommon.
Keywords
Introduction
Spontaneous isolated celiac or superior mesenteric artery (SMA) dissection (SICMAD) is a rare clinical entity, with only 143 published reports identified by a recent review. 1 Furthermore, the reported incidence was only 0.06% based on a series of autopsy cases. 2 Nonetheless, increased use of computed tomographic angiography (CTA) imaging has the increased potential to diagnose SICMAD in both symptomatic and asymptomatic patients. 3
While the clinical presentation of SICMAD is well documented, the natural history, including recurrent symptoms, aneurysmal change, vessel remodeling, and dissection progression, have not been well defined.4–6 Also, to date, there are no consensus guidelines regarding the best management of patients presenting with SICMAD. Treatment options include blood pressure control, antiplatelet therapy, anticoagulation, endovascular stenting, and surgical repair. 7 There have been published reports advocating for both conservative4,8 and invasive 9 interventions. Optimal medical therapy is also disputed; there is no consensus regarding antiplatelet therapy versus anticoagulation.8,10 As this question has been investigated in other dissected arterial beds, such as carotid and vertebral arteries, further studies may suggest that one therapy is superior. 11
The objective of this study is to investigate the natural course of SICMAD, specifically in relation to clinical outcomes, radiographic vessel remodeling, dissection progression and aneurysmal dilatation, and to report these outcomes in relation to treatment strategy.
Methods
We retrospectively queried a prospectively collected institutional radiology database for all patients found to have isolated celiac and SMA dissections, defined as presenting without concomitant aortic dissection or trauma at Massachusetts General Hospital between January 1990 and March 2017. The Institutional Review Board at the Massachusetts General Hospital approved the study protocol; patient consent was not required. We identified patients with SICMAD by searching for terms related to mesenteric artery dissection (i.e. ‘SMA dissection’, ‘superior mesenteric artery dissection’, ‘celiac artery dissection’, etc.). Patients were excluded if the dissection occurred in the setting of trauma, iatrogenic injury, or concomitant aortic dissection.
Patient baseline characteristics, presentation, concomitant diagnosis, treatment, and outcomes were extracted via chart review. Treatment was defined as antiplatelet therapy, anticoagulation, endovascular treatment, surgical treatment, or conservative therapy, which consisted of blood pressure control and vascular risk factor management. Fibromuscular dysplasia (FMD) was defined by angiographic (invasive or non-invasive) appearance of FMD, which is available in previously published literature. 12
All imaging studies were reviewed for accuracy by an independent radiologist blinded to baseline characteristics and clinical outcomes (author: SG). SICMAD was considered confirmed if evidence could be found in a multidetector CT scan or digital subtraction angiography. Both SMA and celiac artery dissections were classified according to Sakamoto et al.’s classification 13 (Figure 1) – type I: patent false lumen with both entry and re-entry; type II: ‘cul-de-sac’ blind-ending false lumen without re-entry; type III: thrombosed false lumen with ulcer-like projection; and type IV: thrombosed false lumen without ulcer-like projection. Dissection length, vessel diameter, ostial involvement, and the presence of stenosis were also recorded. Stenosis was defined as a lumen diameter reduction of greater than 50%.
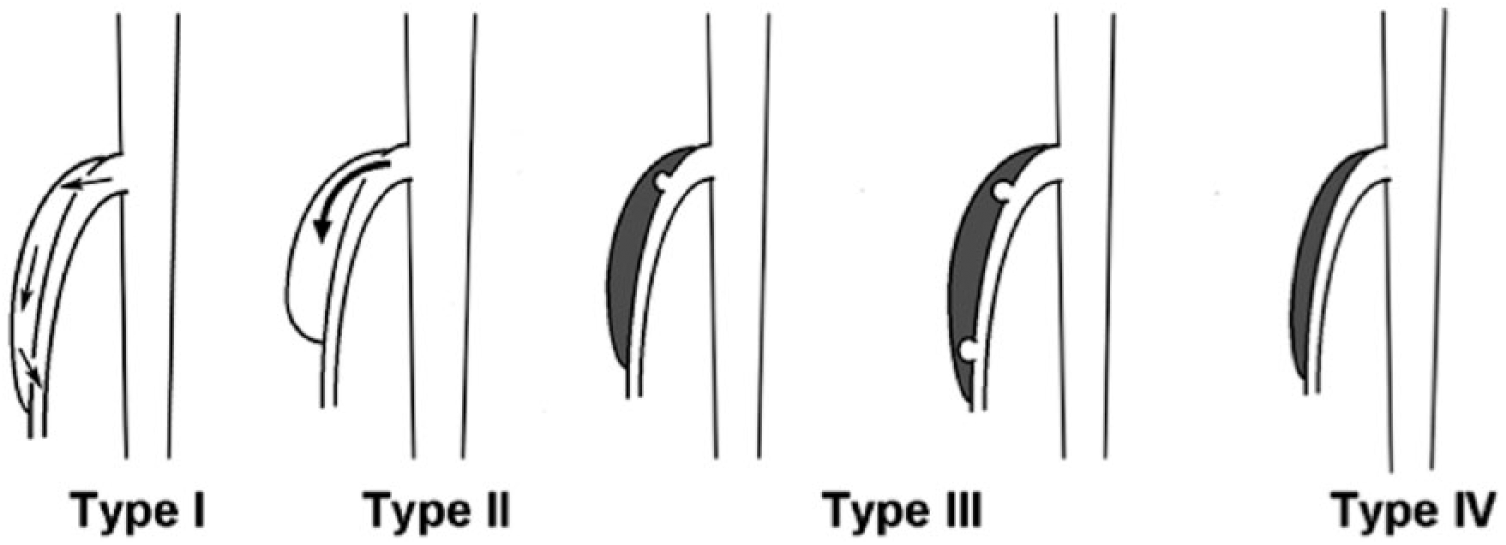
Sakamoto classifications. Type I: patent false lumen with both entry and re-entry; type II: ‘cul-de-sac’ blind-ending false lumen without re-entry; type III: thrombosed false lumen with ulcer-like projection; and type IV: thrombosed false lumen without ulcer-like projection. (Reprinted from ref. 13, Copyright © 2007, with permission from Elsevier.)
Outcomes evaluated at the initial encounter included resolution of symptoms, need for invasive intervention, and bleeding. Outcomes evaluated during the follow-up period, after discharge, included recurrent symptoms, graft or stent patency, re-intervention, aneurysmal degeneration with indication for repair (defined as outer wall diameter greater than 2.0 cm as measured by repeat CT), vessel remodeling, subsequent dissection in other arterial beds, and death. Vessel remodeling was defined as morphological change of the vessel, radiographically between the time of presentation and repeat imaging. Complete vessel remodeling was defined as a complete regression of the previously present dissection resulting in a normal appearing vessel. Partial remodeling was defined as regression of the dissection without complete normalization and was determined by an independent radiologist. Remodeling was defined separately from aneurysmal changes and stenosis.
Statistical analysis
Descriptive statistics were used to report the various variables. Chi-squared tests for categorical variables and t-test for continuous variables were conducted when appropriate. A p-value <0.05 was considered significant. Data were analyzed with R version 3.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Overall, SICMAD was detected in 42 arteries in 40 patients (83.3% male), mean age 54.8 ± 10.9 years, including 24 celiac arteries and 18 SMA. There were no significant differences between the celiac and SMA cohorts (Table 1). Twenty-five (59.5%) dissections occurred in patients with hypertension (HTN), and 17 (40.5%) occurred in patients with hyperlipidemia (HLD). Fourteen (33.3%) dissections occurred in smokers. The prevalence of other cardiovascular risk factors was low (Table 1). Two male patients had evidence of FMD (Figure 2). Of note, 87.5% of patients had imaging of other vascular beds to assess for additional vascular pathology: 75% had thoracic imaging, 22.5% had vascular imaging of the neck, and 37.5% had intracranial imaging. No patient was diagnosed with a connective tissue disorder with vascular manifestations; nine patients were evaluated by a geneticist and three underwent genetic testing. At the time of diagnosis, 10 patients had evidence of aneurysmal disease in other arterial beds, including four with multiple aneurysms: abdominal aorta (n=4), thoracic aorta (n=4), iliac arteries (n=4), infrainguinal arteries (n=2), splenic artery (n=1), and an intercostal artery (n=1). Abdominal pain was the most common presenting symptom, associated with 28 (66.7%) lesions; 14 (33.3%) lesions were asymptomatic. One patient complained of post-prandial abdominal pain. No patient presented with bowel necrosis or arterial rupture.
Patient characteristics, chief complaint, and radiographic characteristics.
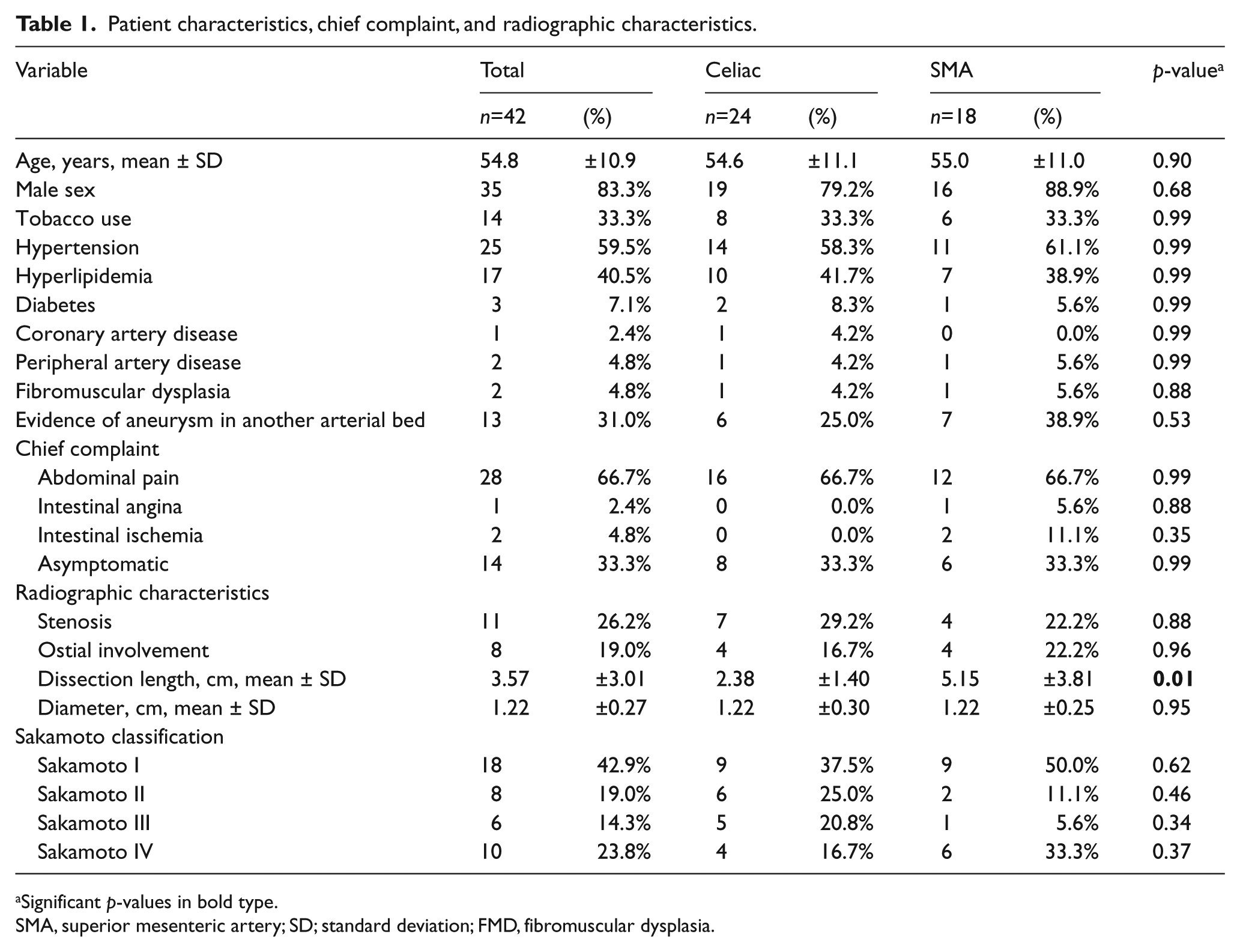
Significant p-values in bold type.
SMA, superior mesenteric artery; SD; standard deviation; FMD, fibromuscular dysplasia.
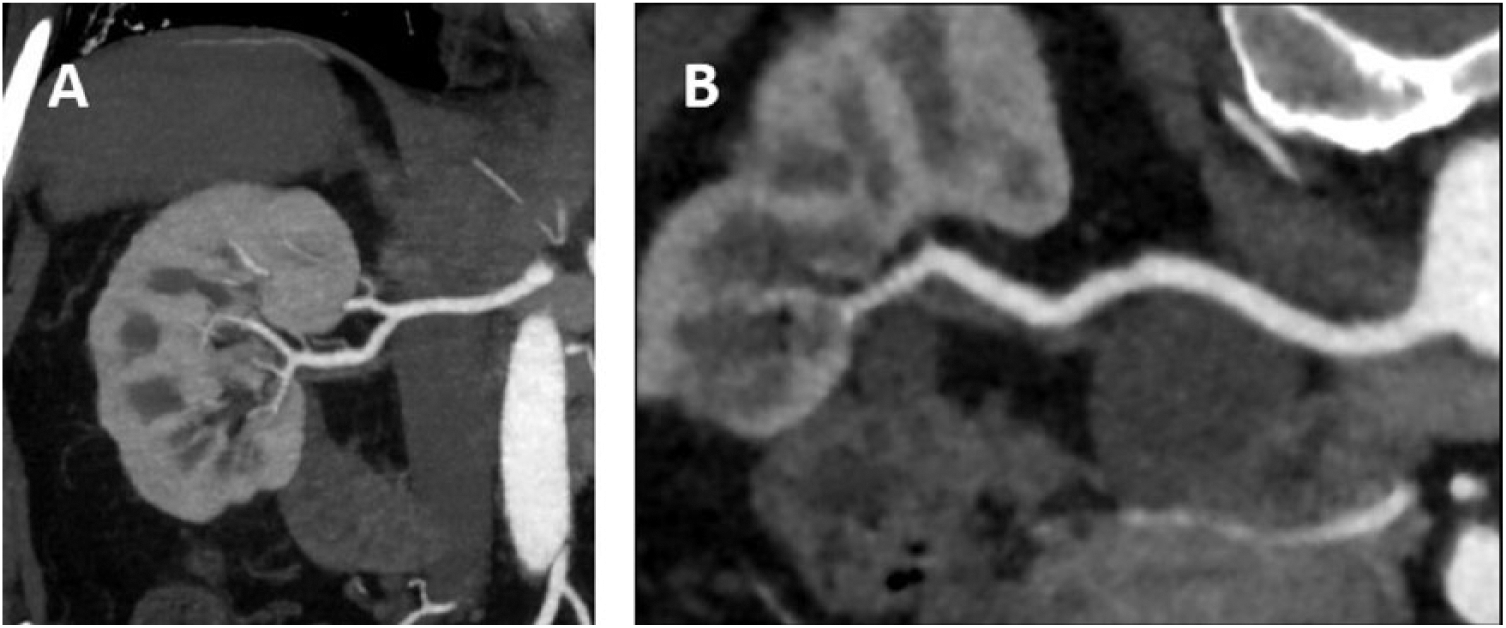
(A) Computed tomographic angiography showing beading in the inferior branch of the right renal artery. Cortical thinning, a result of infarction, can be seen in the inferior pole. (B) Reformat of the right renal artery revealing beading in the distal portion, is consistent with fibromuscular dysplasia.
Most patients (42.9%) presented with Sakamoto type I lesions. The average vessel diameter at time of diagnosis was 1.22 ± 0.27 cm. Eight arteries had ostial involvement, and the average length of dissection was 3.57 ± 3.01 cm; significantly longer in SMA lesions (SMA 5.15 ± 3.81; celiac 2.38 ± 1.40, p = 0.008). Stenosis was found in 11 arteries (26.2%).
Eighteen lesions were treated with antiplatelet therapy, 13 with anticoagulation, four with both, and seven with neither. One patient was treated with an endovascular stent, and no patients underwent open surgical intervention. The mean length of anticoagulation therapy was 7.75 months, but four patients were placed on anticoagulation indefinitely.
Thirty-one patients had follow-up; the mean follow-up was 4.9 ± 4.8 years. Morphologic improvement was seen in 48% of arteries, 19.7 ± 14.7 months after diagnosis.
Table 2 displays factors associated with vessel remodeling and recurrent dissection. Sakamoto type IV lesions (Figure 3) were more likely to undergo remodeling (p=0.039), and asymptomatic lesions and Sakamoto type II lesions were less likely to undergo remodeling (p=0.010 and p=0.050, respectively). There was a trend towards remodeling in stenotic arteries (p=0.053). No factors were predictive of recurrent symptoms. Follow-up with CT scans were available for 31 arteries; patients received an average of 2.35 scans during follow-up. Figure 4 (A and B) displays the vessel diameter on follow-up CT scans over time for SMA and celiac artery dissections, respectively; the majority of arteries measured 1.5 cm or less on CT scans. Only one artery ever measured greater than 2.0 cm. The figures also suggest that vessel diameters are relatively constant over time.
Factors associated with vessel remodeling and recurrent dissection a .
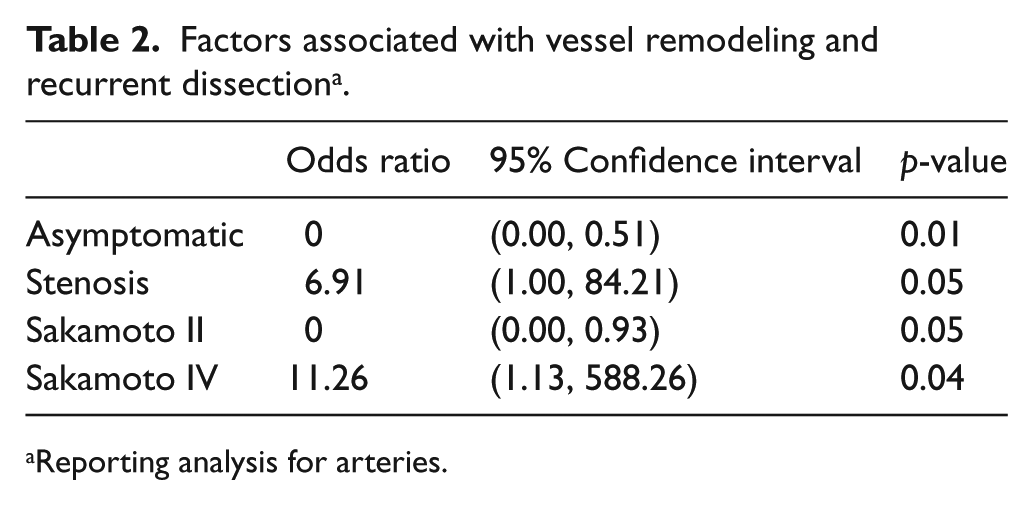
Reporting analysis for arteries.
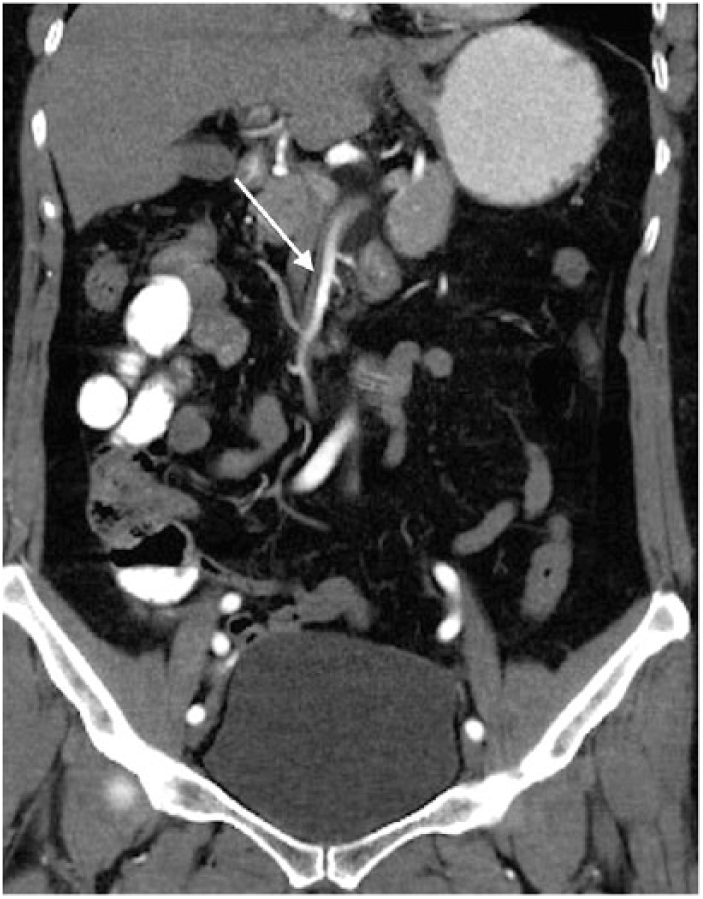
Computed tomographic angiography coronal images depicting dissection of the superior mesenteric artery (arrow) consistent with Sakamoto type IV dissection.
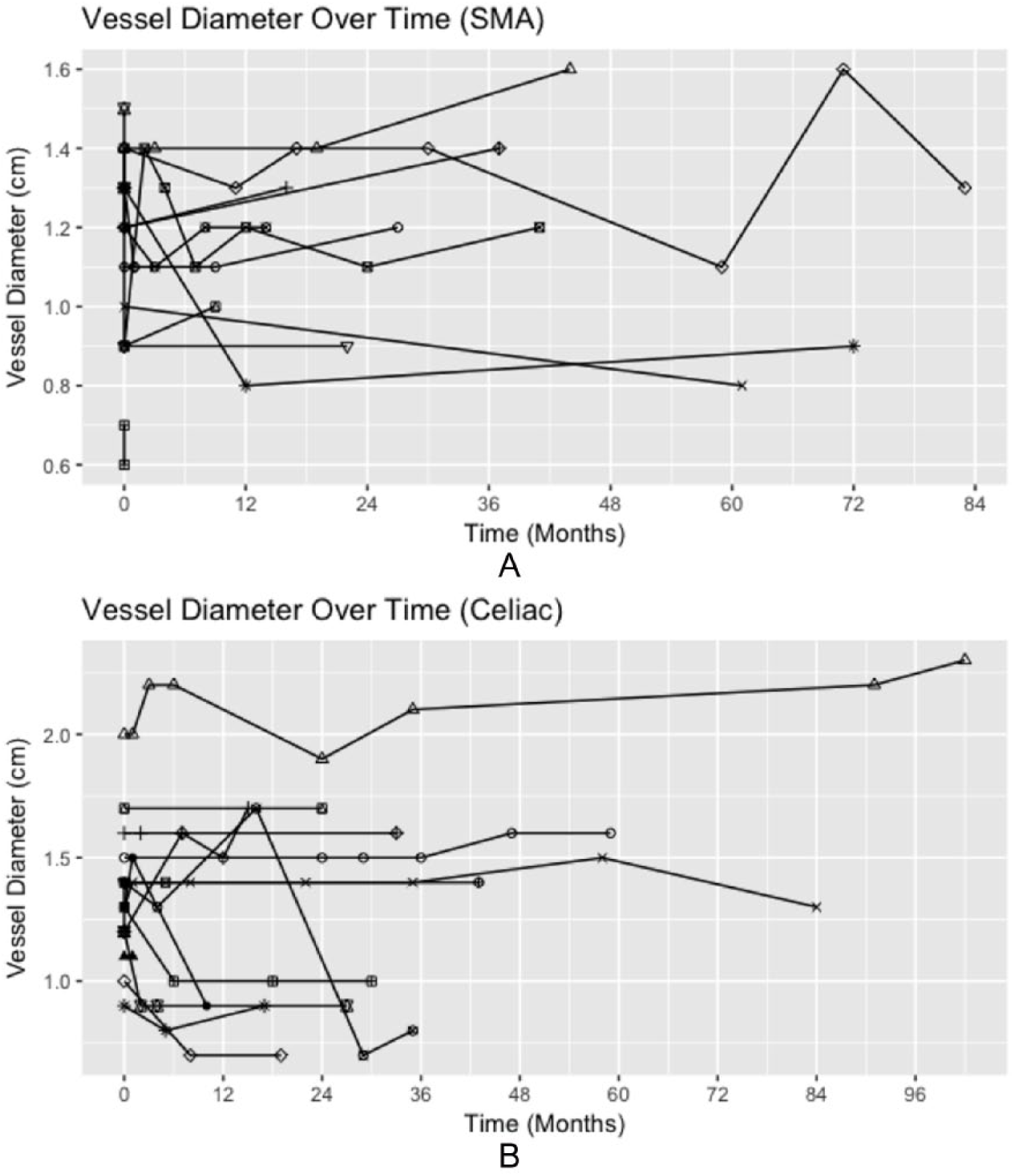
Vessel diameter on follow-up computed tomographic (CT) scans over time for (A) superior mesenteric arteries and (B) celiac arteries, with each line and associated shape representing an artery and each dot representing a follow-up CT scan.
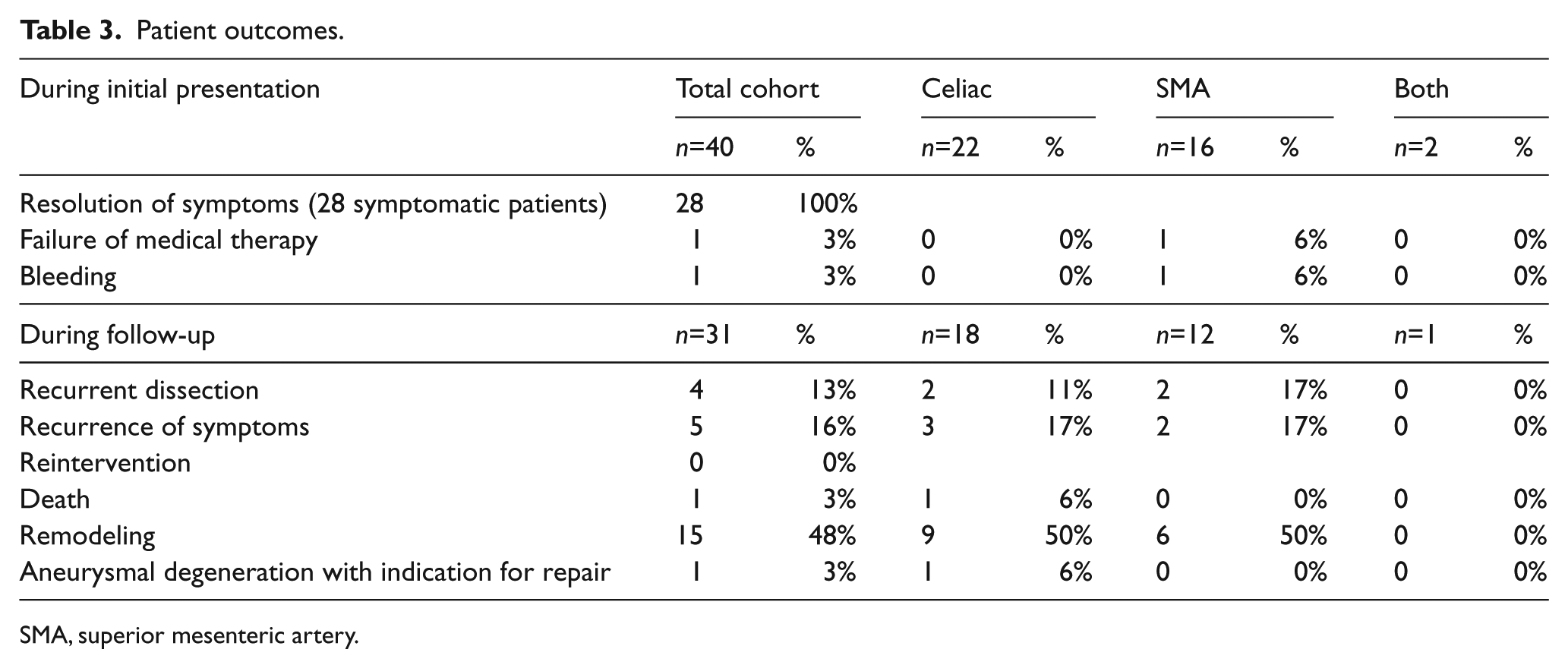
Outcomes are presented in Table 3. Resolution of symptoms occurred in all symptomatic patients. One patient failed medical therapy due to persistent pain and had a covered stent placed for his SMA dissection. The only bleeding complication occurred in the same patient, as he developed an access site hematoma, post-procedure. Five patients had recurrence of symptoms 0 to 101 months from the date of diagnosis, yet none of these patients had new radiographic findings with recurrent symptoms. During the follow-up period, one patient underwent an attempted intervention for intermittent, recurrent abdominal pain in the setting of aneurysmal dilatation, but a stent could not be placed and the procedure was aborted; the pain subsided without further intervention. Four patients had dissections in other vascular beds, post-diagnosis, and two patients suffered multiple dissections: carotid dissections (n=3), including one patient with bilateral carotid dissections, vertebral dissection (n=1), and splenic artery dissection (n=1) (Table 2). One patient died during the follow-up period for causes unrelated to SICMAD.
Patient outcomes.
SMA, superior mesenteric artery.
Discussion
In this comparatively large series of North American SICMAD patients followed over nearly 5 years, all patients displayed clinical improvement or stability. This was true for both SMA and celiac arteries, uniquely illustrating similar clinical outcomes between the two arteries.
Our patient population shared characteristics with those of previously published reports: age of presentation in the sixth decade of life, more commonly male, and with a low prevalence of cardiovascular risk factors.3,4,14 The prevalence of HTN in our cohort was higher than other reports. It is important to consider that 70% of previously reported patients originated from Asia and, while we cannot confirm this, differences in patient characteristics may reflect different disease prevalence among populations. 1
The majority of literature published on SICMAD focuses on SMA dissections rather than celiac dissections: 495 versus 88 cases, respectively, in a recent review. 1 Our cohort included 24 celiac artery dissections, which is a large experience of celiac artery dissections compared to contemporary series.15,16 We acknowledge that while comparatively large, our small dataset does not allow for definitive conclusions to be drawn. However, aside from length of dissection, our data show no significant differences between the SMA and celiac groups.
Long-term concerns of SICMAD include extension of the dissection, aneurysmal degeneration, and chronic patient symptoms. While avoiding these potential outcomes is central to the management of SICMAD patients, data to guide optimal management strategy are lacking. Han et al. published a series of 52 consecutive patients treated with anticoagulation and noted complete remodeling in 41.7%. 8 In our series, 48% of arteries had some degree of morphological improvement, but only three arteries achieved complete remodeling. While acknowledging the small size of our dataset, no differences in clinically significant outcomes were noted among patients treated with anticoagulation versus antiplatelet agents, which is consistent with a large, recently published series. 17 Thus, while anticoagulation is thought to reduce the risk of thrombosis in the setting of exposed tissue factor, further studies are needed to evaluate its benefit in SICMAD.
One of the most commonly cited indications for invasive intervention in SICMAD is aneurysmal dilation greater than 2.0 cm, which is also the major cited justification for continued surveillance in asymptomatic patients.1,7,18 While there have been case reports and small case series documenting the occurrence of celiac and SMA artery aneurysm rupture,19,20 the true rate of rupture in SMA and celiac artery aneurysms in unknown. The recommendation of a diameter greater than 2.0 cm as an indication for repair is based on data for splenic artery aneurysms. 21 We observed no ruptures and only one artery greater than 2.0 cm in our series over a follow-up of nearly 5 years. The largest change in diameter was 0.5 cm during follow-up, and minimal or no change was seen in the majority of arteries. While previous publications did not include changes in diameter on every follow-up CT scan, they also reported aneurysmal changes to be rare. 17 Nonetheless, in the current series, patients received an average of 2.35 CT scans, with some patients receiving as many as seven. Given the radiation and contrast exposure associated with CTA and that the majority of arteries do not undergo significant dilation, we try to minimize the use of CTA as a routine long-term follow-up modality. Our practice is to monitor using CTA until 1-year post-diagnosis and to monitor with duplex ultrasound after that in asymptomatic patients.22,23 Patients who experience a recurrence of symptoms undergo a CTA evaluation for anatomic changes in the dissected arteries. However, we recognize the need for further studies regarding the ideal imaging regimen for these patients.
While multiple algorithms have been suggested,1,7 there is no consensus treatment paradigm for SICMAD. Previous publications have advocated for medical management as first line. 1 Such therapy includes cardiovascular risk factor optimization, antiplatelet therapy, anticoagulation, or both. Interestingly, some authors have advocated for cardiovascular risk factor optimization without antiplatelet therapy or anticoagulation, and have reported excellent results.4,15 In our series, 97% of patients did not require invasive intervention. It is our practice to offer invasive intervention for persistent pain despite medical therapy or for patients presenting with abdominal catastrophes such as rupture or bowel infarction. Notably, given the limitations of our dataset, it is difficult to prescribe a definitive threshold for intervention, as only one patient underwent invasive intervention in our cohort. One patient in our series underwent successful stenting due to persistent pain. Further studies are needed to identify the possible advantages of one therapy over another.
Other than treatment strategy, radiographic characteristics may be relevant to long-term outcomes. In the current cohort, most arteries displayed a Sakamoto type I dissection. Previously, Park et al. published a series in which they found that Yun type II arteries (either patent true and false lumen without re-entry or patent true lumen but thrombosed false lumen) were more likely to undergo remodeling. 4 In our cohort, we found that Sakamoto type IV arteries were significantly more likely to remodel and that Sakamoto type II arteries were significantly less likely to remodel, suggesting that the classification system may have some predictive utility.
A gap in the care of SICMAD patients is the paucity of data regarding etiology, which is a result of the lack of pathologic specimens, as open surgical intervention is uncommon. Potential etiologies have been reported, including atherosclerosis, medial degeneration of the arterial wall, and arteriopathies. 24 Most specifically, segmental arterial mediolysis (SAM) has been suggested as a potential cause of SICMAD,19,25 but without pathologic data, it is a diagnosis of exclusion.
Limitations
The major limitation of this study is that it is small, non-randomized, and retrospective, making it difficult to draw firm conclusions regarding treatment and follow-up strategies. It is possible that some patients had vascular pathology that was not diagnosed, as not all patients had imaging of other arterial beds or genetic testing. However, given the rarity of SICMAD and the comprehensive objective nature of our data, we believe that it represents an important addition to the available literature.
Conclusion
In our series, the vast majority of patients with SICMAD improve with medical therapy alone, and the majority of dissected arteries did not exhibit aneurysmal dilation during follow-up. This represents a gap in care that may be addressed by more conservative use of CTA imaging as a surveillance tool for patients with SICMAD.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.