
Abstract
Objectives:
Endovascular treatment (EVT) is an alternative method used to treat isolated dissection of the celiac artery (IDCA). However, only a few mid-term results have been reported. This study aimed to analyze and compare the outcomes of endovascular and non-operative therapies for IDCA.
Methods:
Data from a cohort of consecutive IDCA patients enrolled in the study hospital between April 2012 and September 2020 were retrospectively reviewed. Demographic information, imaging features, treatment modalities, and follow-up results of celiac artery remodeling and adverse events were collected and analyzed.
Results:
A total of 87 patients were enrolled in the study. Stents were deployed in 68 patients, and non-operative treatment (blood pressure control and pain management) was continued in the remaining 19 patients who did not receive stenting; among these 19 patients, EVT failed in 6. The mean follow-up period was 37.3 (range, 10–85 months) and 44.0 (range, 9–80 months) months in the EVT and non-operative groups, respectively. During follow-up, the overall complete remodeling (absence of residual dissection with no false lumen or no intramural thrombus) rate was significantly higher in the EVT group than in the non-operative group (87.3% vs 7.1%, p<0.001). The incomplete remodeling (improved true lumen with malabsorption or partial thrombosis of the false lumen) rate was not significantly different between the EVT and non-operative groups (6.3% vs 14.3%; p=0.2984). Meanwhile, the adverse event-free survival rates were 89.0%, 67.0%, and 67.0% at 1, 3, and 5 years, respectively, in the EVT group compared with 39.7% and 29.8% at 1 and 3 years in the non-operative group (p<0.0001).
Conclusions:
EVT for IDCA may be considered an effective management option with a favorable clinical success rate, an encouraging complete remodeling rate, and a satisfactory adverse event-free survival rate. However, further evaluation with a long-term follow-up is required.
Clinical Impact
Endovascular intervention for isolated dissection of the celiac artery has attracted inadequate attention. In this retrospective study with comparative analysis of endovascular versus conservative therapy for isolated dissection of the celiac artery patients, a better complete remodeling rate and a higher adverse event-free survival rate were observed in the endovascular treatment (EVT) group during follow-up, indicating that EVT could be an effective management option for isolated dissection of the celiac artery.
Introduction
Isolated dissection of the celiac artery (IDCA) without associated aortic dissection has rarely been reported since the first case in 1987. 1 To the best of our knowledge, fewer than 200 IDCA cases have been reported in the literature, and the majority of these have been reported in a small case series. 2 However, an increasing number of case reports and retrospective studies have been published recently owing to advances in computed tomography angiography (CTA), suggesting that the incidence of IDCA was previously underestimated. Consensus in IDCA therapeutic strategy, together with etiology, natural course, and prognosis, remains controversial. 3 As recent literature suggested, non-operative management has yielded acceptable results.2–4 However, observation with or without anticoagulation and antiplatelet therapy still carries the risk of aggravation of dissection, which may result in malperfusion or life-threatening hemorrhage due to rupture of the dissecting aneurysm. 5
Endovascular repair has been widely applied in aortic and superior mesenteric artery dissection.6,7 The 2017 European Society for Vascular Surgery guidelines also recommend endovascular revascularization for symptomatic patients. 8 However, only a limited number of patients with IDCA underwent endovascular treatment (EVT).9,10 As a result, the prognosis and advantages of EVT have been underanalyzed, and the role of EVT in therapeutic strategies remains unclear. Herein, we report our mid-term follow-up results for patients with IDCA who underwent EVT or non-operative therapy and compare the differences in the results between these 2 treatment methods.
Patient Population and Methods
Population and Definitions
This retrospective study included consecutive patients diagnosed with IDCA at our institution between April 2012 and September 2020. The study protocol was approved by the institutional review board of the Ethics Committee of Zhejiang University (Hangzhou, China). The study was performed in accordance with principles of the declaration of Helsinki with approval of the patients involved. The follow-up closing date for all patients was May 2021. IDCA was defined as isolated dissection of the celiac artery (CA) with or without involvement of its branches. 11 IDCA was diagnosed based on spiral CTA findings such as intimal flap and/or thrombosis of the false lumen. Morphological classifications were analyzed as described in our previous study 5 as follows: type I, patent false lumen with both entry and re-entry; type II, “cul-de-sac” shaped false lumen without re-entry; type III, thrombosed false lumen with an ulcer-like projection; type IV, completely thrombosed false lumen without an ulcer-like projection; and type V, aneurysm development in association with dissection. Patients with concomitant aortic dissection or median arcuate ligament compression syndrome were excluded. Demographic information, imaging features, treatment modalities, and follow-up results of CA remodeling and adverse events were collected and analyzed. Technical success was defined as successful implantation of the stent or stent graft with coverage of the primary entry tear and reperfusion of the true lumen. 5 Complete remodeling was defined as the absence of residual dissection with no false lumen or no intramural thrombus on CTA. 9 Incomplete remodeling was defined as improved true lumen with malabsorption or partial thrombosis of the false lumen on CTA. 9 An aneurysm was defined as a focal CA diameter increase of >50% compared with the normal adjacent CA. 3 Adverse events included a patent or enlarged false lumen, aneurysm formation, true lumen occlusion, splenic infarction, liver dysfunction, and recurrent abdominal pain. The baseline characteristics of the study cohort are summarized in Table 1.
Characteristics of Patients With Isolated Dissection of the Celiac Artery.
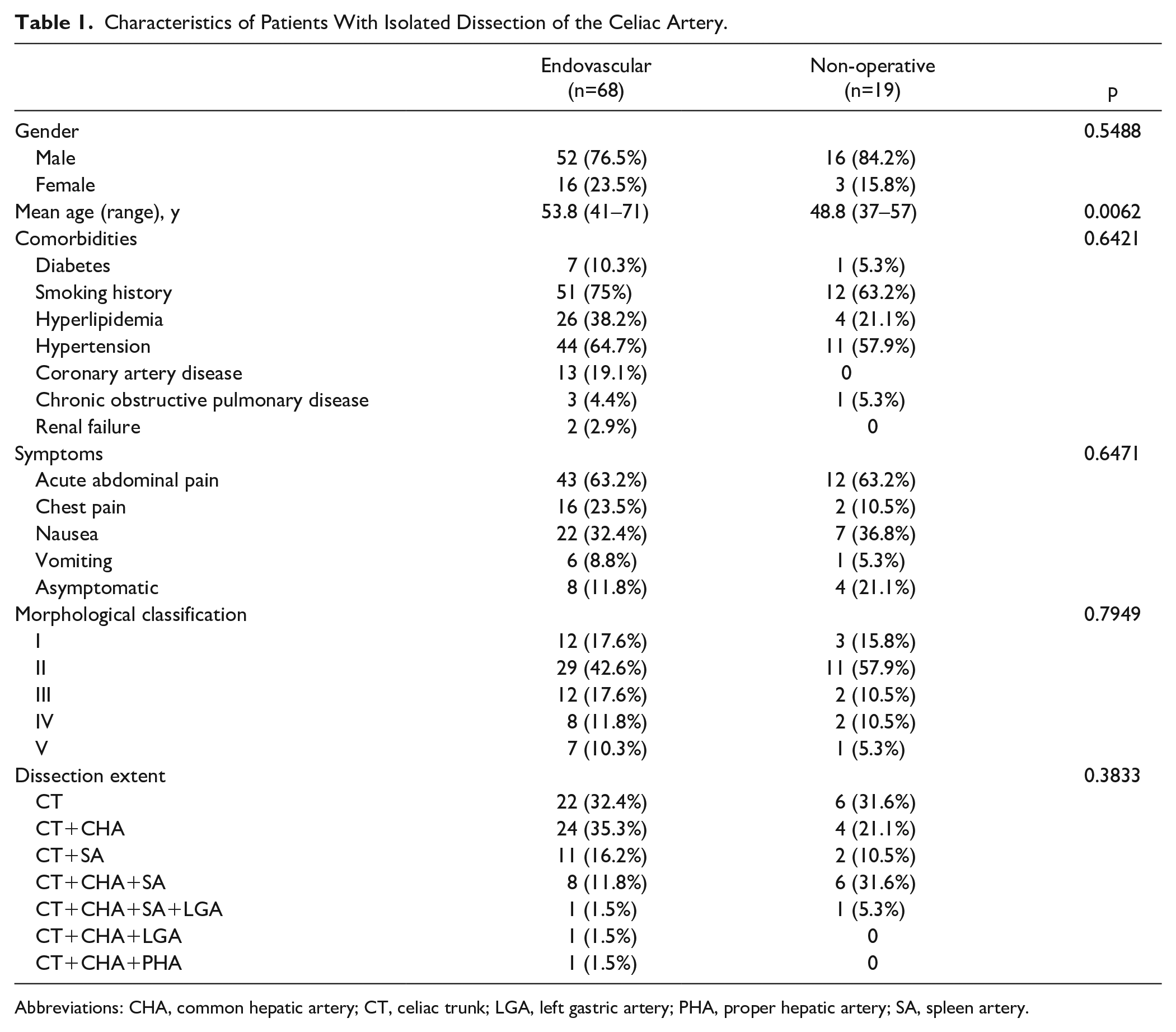
Abbreviations: CHA, common hepatic artery; CT, celiac trunk; LGA, left gastric artery; PHA, proper hepatic artery; SA, spleen artery.
Treatment Strategies
All patients underwent preoperative thin-slice CTA for diagnosis and initially received non-operative therapy that included blood pressure control and pain management. We shared a decision-making approach with the patients to discuss treatment strategies. The advantages and disadvantages of EVT and non-operative treatments were explained to the patients, and their wishes were followed. EVT was especially indicated in patients who presented with intractable abdominal pain, visceral malperfusion, or aneurysm development.
Technical Principles of EVT
EVT was performed under general or local anesthesia. Initially, a sheath was inserted via the femoral or brachial approach, and a bolus of 5000 IU of heparin was injected. Selective CA angiography was performed using a 4 F MPA catheter (Cordis, Miami Lakes, FL, USA), based on which the morphological classification and stent landing zone were verified. Covered or bare self-expanding stents were implanted in the true lumen of the CA with distal landing in the common hepatic artery (CHA) or trunk of the CA using a 0.035 guidewire (Amplatz Super Stiff, Boston Scientific, Marlborough, MA, USA) or 0.018 guidewire (V-18, Boston Scientific), with the aim of ensuring true lumen patency and sealing the entry tear to avoid aneurysmal dilation.
The technical principles of EVT largely depend on the aspect and location of the dissection. Covered stent is preferred especially when the tear is large and false lumen is patent with aneurysmal dilation. If the tear is small or even undetectable and false lumen is mostly or fully thrombosed, bare stent can also be considered. The benefits of enlarging the true lumen and the positive effect of bare stents on remodeling have been verified in the dissection of superior mesenteric artery.9,12 Owing to the tortuous anatomical configuration, stents in the celiac trunk and branches should be as flexible as possible. Thus, Viabahn (W.L. Gore Associates, Inc, Flagstaff, AZ, USA) was chosen as the endograft because of its superior flexibility. Nevertheless, the choice of the Viabahn length was often a problem because only 2 sizes (25 and 50 mm) were available in our facility. The 50 mm endograft was too long in most cases, while the 25 mm endograft could be difficultly deployed precisely. Therefore, certain patients underwent multiple or combined stent implantation (covered and overlapping bare stents). To obtain a landing zone that was as long as possible, the proximal ends of the stents were deployed 1 to 3 mm into the aorta. In addition, Pulsar-18 (BIOTRONIK SE & Co KG, Berlin, Germany) was accepted as the best bare stent because of its peak-to-valley design, and its thin struts provided the best flexibility among the 5 types of bare stents.
Post-balloon dilation was not routinely performed unless severe stent stenosis was evident. Additional coil embolization of an overwhelmingly large false lumen or aneurysm was performed if necessary. The final digital subtraction angiography was repeated to examine the coverage of the entry tear to false lumen and the improvement of the distal blood supply. After the procedure, low-molecular-weight heparin (100 U/kg, twice per day) was used for 3 days for anticoagulation, and dual antiplatelet therapy was prescribed for at least 6 months after hospital discharge, followed by mono-antiplatelet therapy as long-term therapy. Patients who refused EVT or underwent a failed endovascular attempt continued non-operative therapy.
Follow-up
All patients were evaluated after discharge at 1, 6, and 12 months and yearly thereafter. CTA was performed at every follow-up visit and relevant information was collected at each time point. Adverse events included recurrent abdominal pain, true lumen occlusion, in-stent restenosis, patent or enlarged false lumen, aneurysm formation, splenic infarction, liver dysfunction, and death.
Statistical Analysis
Statistical analysis was performed using the Student’s t test, chi-squared test, or Fisher’s exact test. The event-free survival rate and percentage of completely remodeled IDCA were calculated according to a Kaplan-Meier curve generated using GraphPad Prism version 5.0 (GraphPad Inc, La Jolla, CA, USA). Differences were considered statistically significant at p<0.05.
Results
Patients’ Characteristics
A total of 87 patients with IDCA were enrolled in this retrospective study. Demographic information is summarized in Table 1, and a flow diagram of patient selection is shown in Figure 1. The mean age was 53.8 years (range, 41–71 years) in the EVT group and 48.8 years (range, 37–57 years) in the non-operative group. In both groups, most patients were male (EVT, 76.5%; non-operative, 84.2%), and the most common comorbidities were hypertension (EVT, 64.7%; non-operative, 57.9%) and smoking (EVT, 75%; non-operative, 63.2%). Acute abdominal pain was the most prominent symptom in all symptomatic patients (EVT, 63.2%; non-operative, 63.2%). Other symptoms included nausea, chest pain, and vomiting. Overall, 12 patients who were incidentally diagnosed with IDCA by health examination or CT irrelevant to IDCA were asymptomatic. All patients underwent non-operative treatment as soon as a diagnosis of IDCA was suspected. The morphological classification based on CTA is summarized in Table 1. Type II was the major type of classification in both groups (EVT, 42.6%; non-operative, 57.9%), accounting for all patients. Representative images of the morphological classifications are shown in Figure 2.
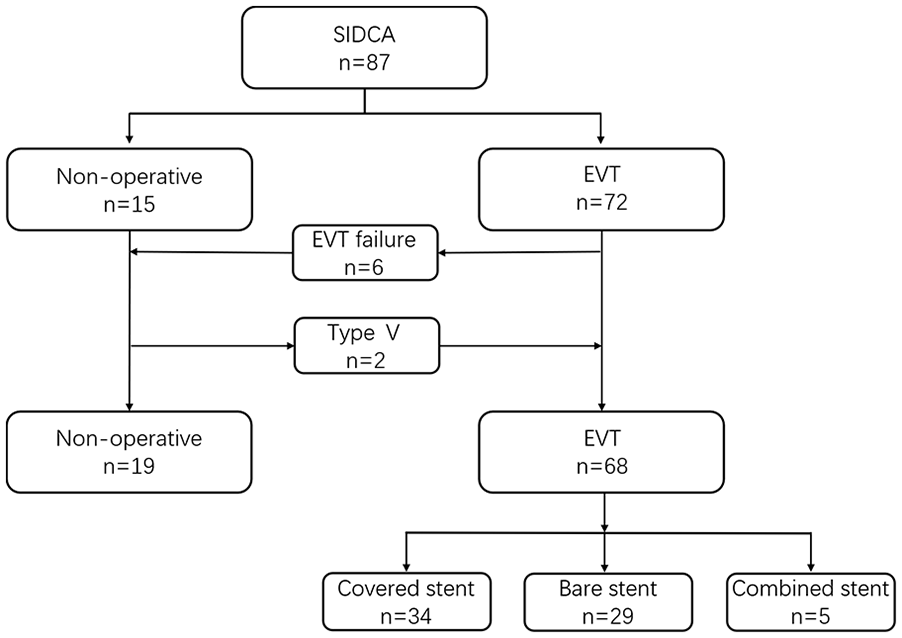
Patients flow chart. EVT, endovascular treatment; SIDCA, spontaneous isolated dissection of the celiac artery.
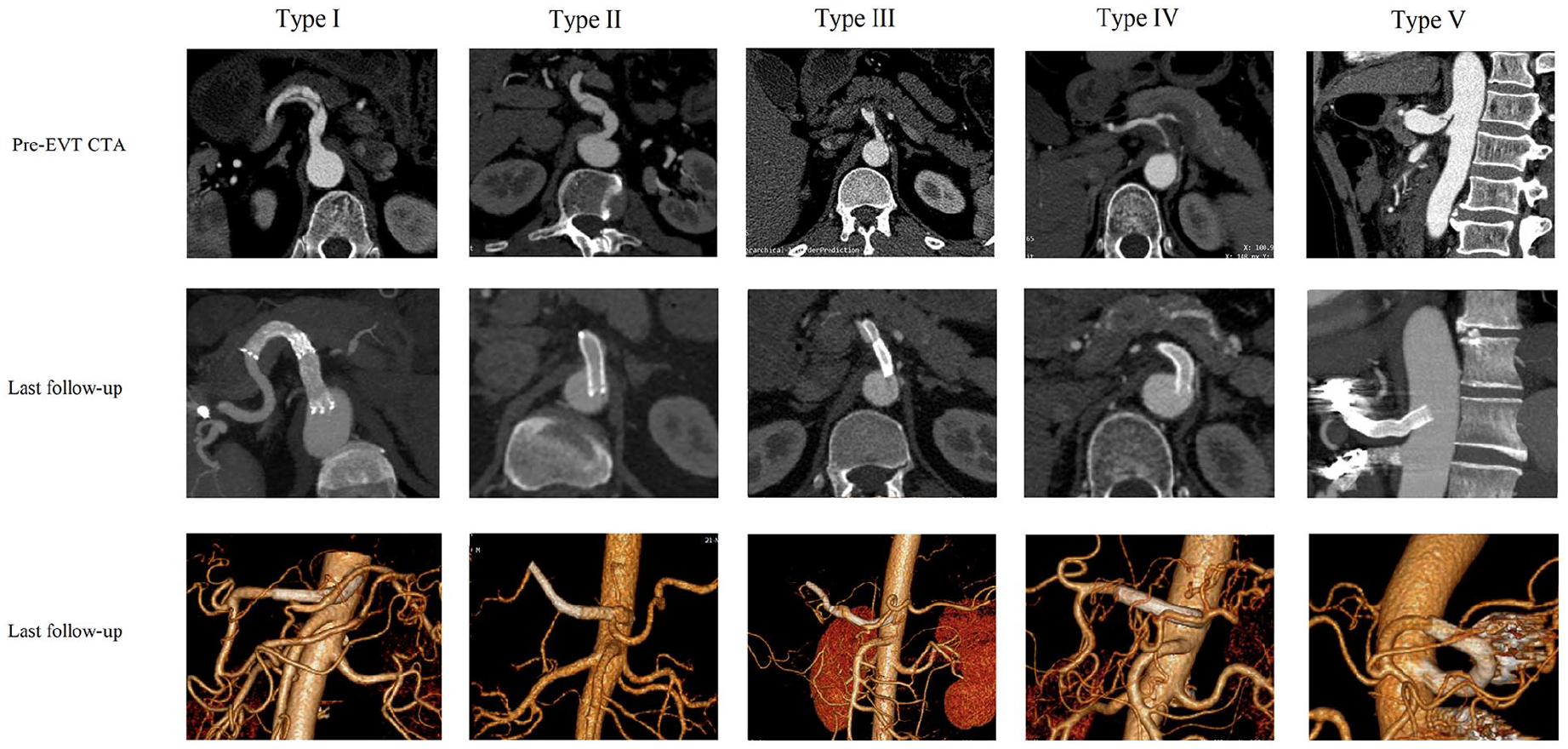
The morphological classifications of isolated dissection of the celiac artery (IDCA). The typical computed tomography angiography images before endovascular therapy and on last follow-up. EVT, endovascular treatment; CTA, computed tomography angiography.
Treatment Results
Following the initial non-operative therapy, 72 patients underwent EVT and 15 continued with the non-operative treatments. Overall, 6 patients (5 type IV, 1 type II) underwent failed EVT due to true lumen occlusion (n=4 [5.4%]) or subintimal tracking with failed re-entry (n=2 [2.7%]). All patients with failed EVT received conservative medical therapy after angiography alone and were included in the non-operative group. Two initial non-operative patients (type V) who had symptomatic relief and refused EVT underwent stent deployment because of recurrent abdominal pain. The EVT success rate was 91.9% (68/74). The left brachial and right femoral arteries were used as common vascular approaches, depending on the angle of the CA origin. The CHA was the preferred distal landing artery if the stent needed to cover the bifurcation. Overall, 34 patients received covered stents, and 29 received bare stents. The other 5 patients underwent combined covered and bare stent implantation. A total of 56 Viabahn covered stents were used. Pulsar-18 was the most commonly used bare stent (64.7%). Six patients (8.8%) underwent additional false lumen or splenic artery embolization during EVT. No immediate complications, such as pseudoaneurysms, were observed during EVT or before hospital discharge. The details of EVT are summarized in Table 2.
Details of Endovascular Therapy for Isolated Dissection of the Celiac Artery.
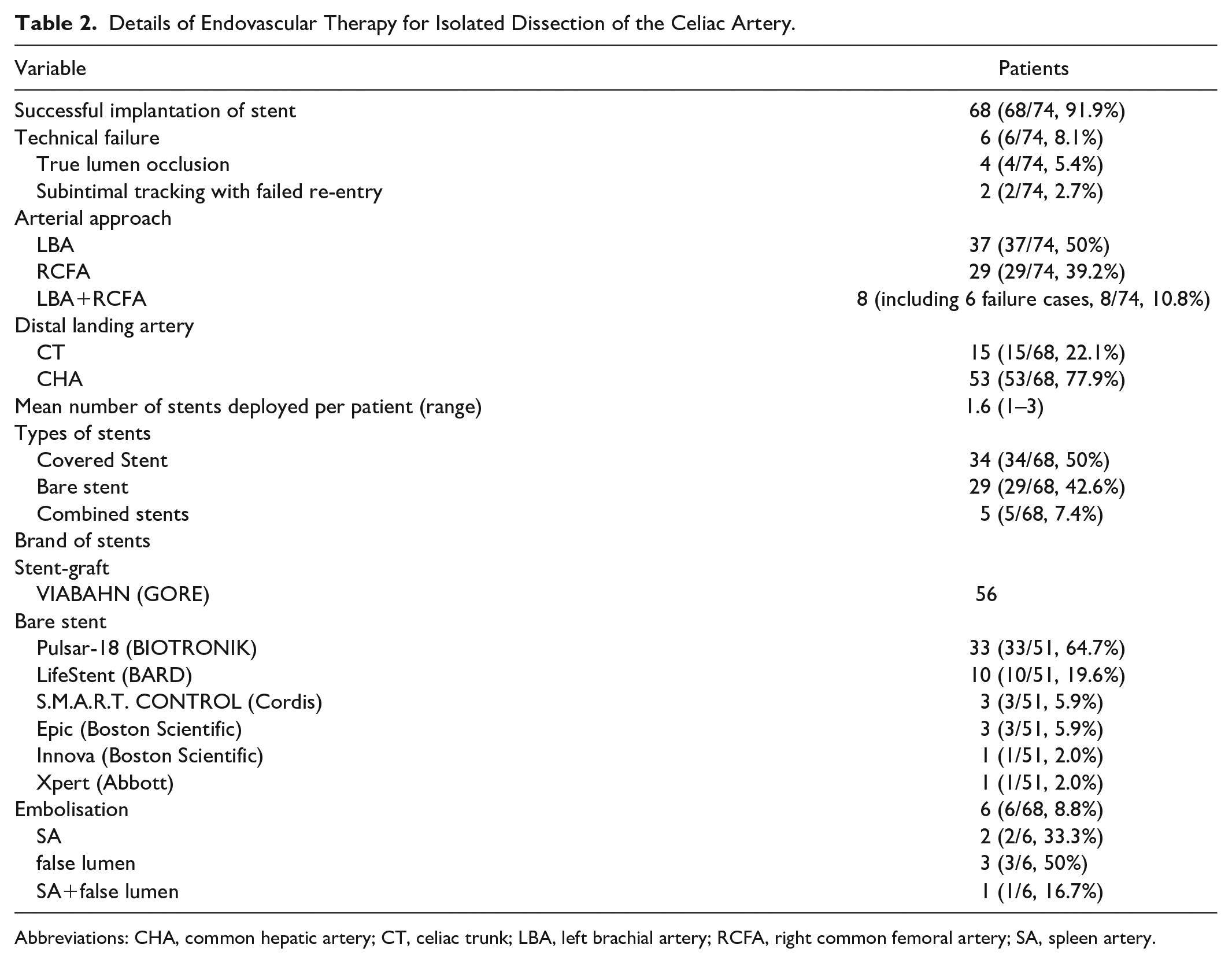
Abbreviations: CHA, common hepatic artery; CT, celiac trunk; LBA, left brachial artery; RCFA, right common femoral artery; SA, spleen artery.
Follow-up Outcomes
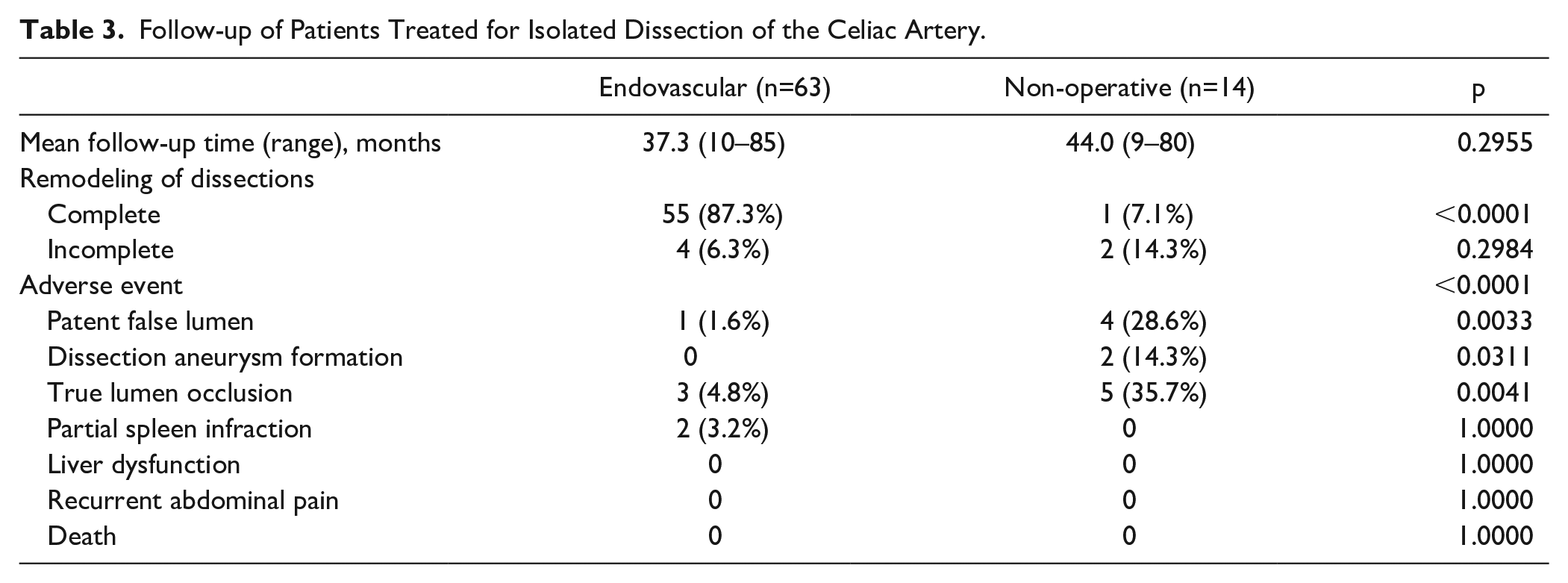
Summaries of the follow-up results are presented in Table 3 and Figure 3. The mean follow-up was 37.3 months (range, 10–85 months) in the EVT group and 44.0 months (range, 9–80 months) in the non-operative group (p=0.2955). Five patients in each group were lost to follow-up. No mortality was reported in the continuous follow-up of patients in either group. Overall, 57 patients in the EVT group achieved complete remodeling, which was significantly higher than that in the non-operative treatment group (55/63 [87.3%] vs 1/14 [7.1%]; p<0.0001). Most of the complete remodeling occurred within 1 month of stenting (Figure 3A). Complete remodeling rates were 81.8% (9/11) at 1 month, 84.2% (16/19) at 3 months, 86.5% (32/37) at 1 year, 86.2% (50/58) at 3 years, and 87.1% (54/62) at 5 years. Complete remodeling was not observed in the non-operative group within 1 year. Complete remodeling without stents (type IV) occurred only in 1 case at the 2-year follow-up, resulting in a poor complete remodeling rate (p<0.0001) (Figure 3A). Incomplete remodeling was rare in both groups (4 vs 2), and the difference was not statistically significant (6.3% vs 14.3%, p=0.2984). The incidence of adverse events (patent false lumen, aneurysm formation, and true lumen occlusion) at follow-up was also significantly lower in the EVT group (p<0.0001). One patient (type I) in whom 2 covered stents were implanted was examined for a patent false lumen 17 months after EVT due to type II endoleak. However, there were more patients with patent false lumen in the non-operative group (1.6% vs 28.6%, p=0.0033). Based on follow-up CTA findings, there were more patients with false lumen aneurysmal degeneration in the non-operative group than in the EVT group (0% vs 14.3%, p=0.0311). The true lumen occlusion rate was 4.8% (3/63), which was notably lower than that in the non-operative group (4.8% vs 35.7%; p=0.0041). In-stent occlusion was observed in 3 patients (2 type III, 1 type I) who underwent deployment of covered stents, bare stents, and combined stents, respectively. One type I patient who received combined stents did not adhere to the prescription of antiplatelet agents after discharge (1 month) and the stents were occluded at the proximal end. Two type III patients (1 bare stent and 1 covered stent) were diagnosed with in-stent occlusion at 9 and 20 months after EVT. Five type II patients in the non-operative group showed true lumen occlusion during follow-up. The true lumen was occluded within 1 year (1, 1, 7, 9, and 10 months, respectively) after onset, which indicated that the pressure of the true lumen may not be maintained without stenting in the type II classification. Two patients in whom covered stents were used without embolization were found to have partial splenic infarction; however, the difference was not statistically significant compared with the other group (p=1.00). No liver dysfunction, recurrent abdominal pain, or death was observed in either group. The adverse event-free survival rates were 89.0%, 67.0%, and 67.0% at 1, 2, and 5 years, respectively, in the EVT group compared with 39.7% and 29.8% at 1 and 3 years, respectively, in the non-operative group (p<0.0001) (Figure 3B).
Follow-up of Patients Treated for Isolated Dissection of the Celiac Artery.
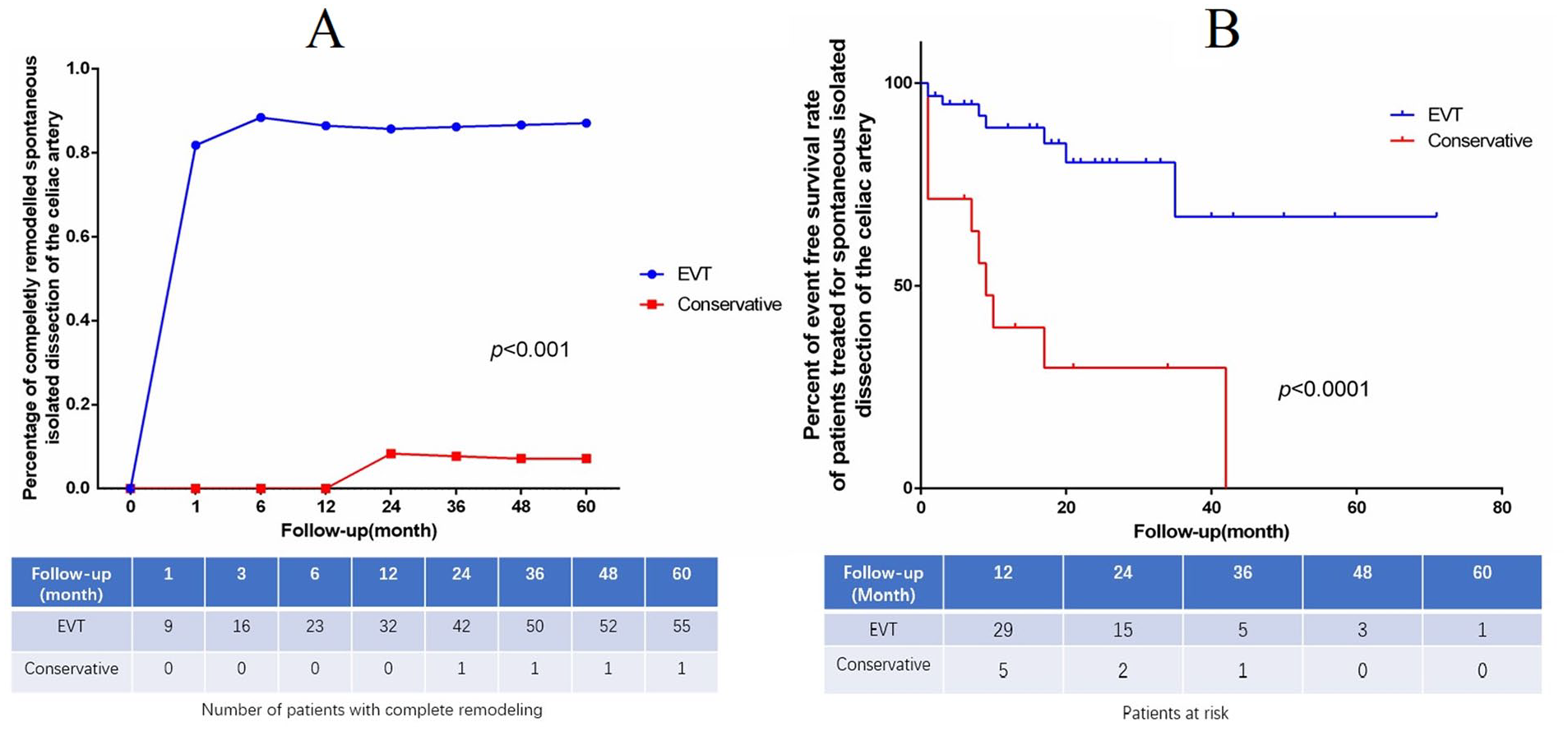
(A) Overall complete remodeling rate in both groups confirmed by computer tomography angiography. The number of patients with complete remodeling is given in table. (B) Cumulative Kaplan-Meier curve of adverse event-free survival rate of patients treated for isolated dissection of the celiac artery. EVT, endovascular treatment.
Discussion
In this retrospective study with comparative analysis of endovascular versus conservative therapy for IDCA patients, a better complete remodeling rate and a higher adverse event-free survival rate were observed in the EVT group during follow-up, indicating that EVT could be an effective management option for IDCA.
IDCA is a rare clinical phenomenon with limited research literature. Recently, it is being increasingly detected owing to advances in radiological technology. However, the underlying pathogenesis and etiology of IDCA remain unclear, although atherosclerosis, fibrodysplasia, medial degeneration, and vasculitis have been recognized as risk factors for spontaneous isolated visceral artery dissection. 13 Owing to the vague natural course of IDCA, the treatment strategy remains controversial. A few recent clinical studies have demonstrated that conservative medical treatment can be adopted if the general condition of the patient remains stable without signs of severe ischemic complications or ongoing hemorrhage.2–4 However, there is a lack of standardized and evidence-based consensus regarding the optimal medical therapy. Some studies regarded antiplatelet or anticoagulation as routine medical therapy,11,14 whereas others applied such therapy only to patients with thrombosis of the true lumen resulting in severely compromised blood flow or occlusion. 15 A previous Japanese study reported promising long-term outcomes even without antiplatelet or anticoagulation therapy. 16 Although patients in the non-operative management group achieved symptomatic relief, the therapeutic effect of non-operative treatment was merely based on the possibility of spontaneous remodeling or thrombosis of the false lumen. In the present study, although symptoms were relieved after medical treatment, 2 initial non-operative patients underwent stent deployment and were transferred to the EVT group because of recurrent abdominal pain after discharge. Moreover, CTA images of non-operative patients at follow-up were not satisfactory because of the patent and aneurysmal false lumen. A recent retrospective series study reported that 94.7% of patients showed no signs of remodeling during follow-up CTA. 2 Our previous study also revealed that the false lumen was only partially thrombosed or still patent in half of the patients in the medical treatment group. 5
The growing expansion of the false lumen carries the risk of rupture and malperfusion secondary to mechanical compression of the true lumen. Therefore, restoring true lumen flow and regressing the false lumen should be regarded as the primary aims of IDCA treatment. Endovascular intervention has attracted inadequate attention as an effective and minimally invasive therapy, even though it was first reported in 1995. 17 In a review published in 2014, only 2 of 88 patients underwent endovascular stenting. 18 In addition, a recent review reported that only 64 of 904 patients underwent EVT as the primary therapy. 9 The unclear natural course of IDCA and abdominal pain relief after initial non-operative treatment are the major causes of the insufficient EVT rate. However, we believe that the benefits of EVT have been underestimated. Our study revealed a significantly higher complete remodeling rate in the EVT group. Only 1 patient (type IV) in the non-operative group achieved complete remodeling after >1 year of non-operative treatment. Most patients in the EVT group experienced complete remodeling and were asymptomatic within 1 month; the percentage of complete remodeling remained >80% along with the follow-up increase. This indicated that patients with stents could experience markedly faster and more efficiently restored blood flow. Only 2 patients in the non-operative group exhibited a regressed false lumen and enlarged true lumen at the last follow-up visit, resulting in a higher (14.3% vs 6.3%) incomplete remodeling rate. We discovered that patients with intramural hematoma who received non-operative treatment exhibited a higher tendency for remodeling during follow-up, which was also supported by a previous retrospective study. 3 One type I patient with covered stents and 1 type III patient with combined stents demonstrated decrease in intramural hematoma compared with the initial imaging results. However, the intramural hematoma of the 2 patients were quite stable at 35 and 8 months of follow-up, respectively, leading to a tendency for barely complete remodeling. Overall, positive dynamic remodeling (complete + incomplete) was achieved in the EVT group, with a significantly higher rate than that in the non-operative group (59/63 vs 3/14; p<0.0001), which suggests that EVT exerts a greater repair effect and warrants further evaluation.
In the present study, the EVT group experienced fewer adverse events. Only 1 patient (type I) who underwent 2 covered stents implantation had a patent false lumen during follow-up because of type II endoleak from the left gastric artery originating from the false lumen. However, a patent false lumen was observed in 3 type II cases and 1 type I case in the non-operative group. Furthermore, dissection aneurysms were found in another 2 patients (1 type I and 1 type II) in the non-operative group, which is higher than that in the EVT group. This shows that non-operative treatment carries a risk of aneurysmal degeneration. Although these 2 patients were asymptomatic, EVT was still recommended. Both patients refused EVT and continued medical treatment in consideration of interventional risks. We inferred that aneurysm formation was not observed in previous studies, partially due to the small number of cases and the retrospective study design.2,4,15,16 Kim et al 3 recently reported 1 patient with an aneurysmal change in the antihypertensive group in a series of 28 non-operative treated patients, which implied that false lumen enlargement was not caused by hypertension. The results of our study suggest that morphological types I and II may contribute to aneurysmal changes due to false lumen patency.
The reason for the 2 in-stent occlusive patients who adhered to antiplatelet therapy was undefined. There was intramural hematoma in CHA with small true lumen diameter (2 mm/2.5 mm) on both preoperative CTA. Thus, we inferred that a narrow distal CHA may affect the hemodynamics of the stents and induce occlusion. True lumen occlusion of non-operative treatment has been occasionally reported. In a recent review, 6% of the pooled study population had late true lumen occlusion during follow-up. 9 Our results showed a higher true lumen occlusion rate (35.7%) in non-operative group, but the mechanism was still unknown. In addition, our data have verified the false lumen could enlarge even under antihypertension therapy. Interestingly, no splenic infarction was found in the 5 CA occlusive patients. Although the previously reported cases and patients in this study were asymptomatic, the long-term effects of CA occlusion remained unclear and should be evaluated. Partial splenic infarction was observed in 2 patients who underwent EVT for covered stents. We considered this a procedural complication despite the patent stents on follow-up. In addition, the difference was not statistically significant between the 2 groups. Fortunately, distal organ ischemia was not observed in the 6 patients who underwent additional embolization.
The present study had several limitations, the first of which was its retrospective design and lack of prospective data. Although the cohort size was large, the grouping was not randomized and the number of patients included in the control group was low. Further studies with better grouping, larger sample size, and longer follow-up durations are required to validate this treatment strategy. Another limitation was that there may be bias in the comparison of true lumen occlusion during follow-up between the 2 groups because some patients already had true lumen occlusion at the beginning of the enrollment in the non-operative group.
Conclusion
EVT for IDCA may be considered an effective management option, with a favorable clinical success rate, an encouraging complete remodeling rate, and a satisfactory adverse event-free survival rate. Nevertheless, further evaluation with long-term follow-up is required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81800405).