
Abstract

Longevity is a vascular question, which has been well expressed in the axiom that man is only as old as his arteries. To a majority of men death comes primarily or secondarily through this portal. Osler W. The Principles and Practice of Medicine, 3rd Edition, 1898.
Unfortunately, the above comment from Sir William Osler still harkens true. However, over the past 25 years of practicing cardiovascular medicine, I was fortunate to see many impressive medical breakthroughs and honored to have helped with some. Medical research, like any endeavor, is not perfect and mistakes can happen that slow progress, or, rarely, it is serendipity that reveals a new unexpected finding. The following highlights my lessons learned from the trials and tribulations of medical research. My full medical memoir is included as a supplement online.
How is medical research advanced?
In college, I realized that scientific discovery is very intriguing. In addition to biology, I also majored in philosophy, a discipline that seeks ultimate answers to ultimate questions. A philosophy professor at Boston College with a PhD in theology and biology taught a course on scientific discovery and insight into how knowledge is advanced. One scientist that he discussed was Imre Lakatos, a Hungarian who lived from 1922 to 1974, who was known for introducing the concept of the ‘research programme’ in his methodology of scientific research (Figure 1). The Lakatosian Research Programme describes a framework whereby there are hard core principals at the center and new ideas or auxiliary hypotheses are advanced based on those core principals. For example, the theory of gravity is a core principal and astrophysics advancements are based on Newton’s ideas. Although serendipity certainly occurs in scientific discovery, medical knowledge generally moves forward based on strong, previously validated core principals.
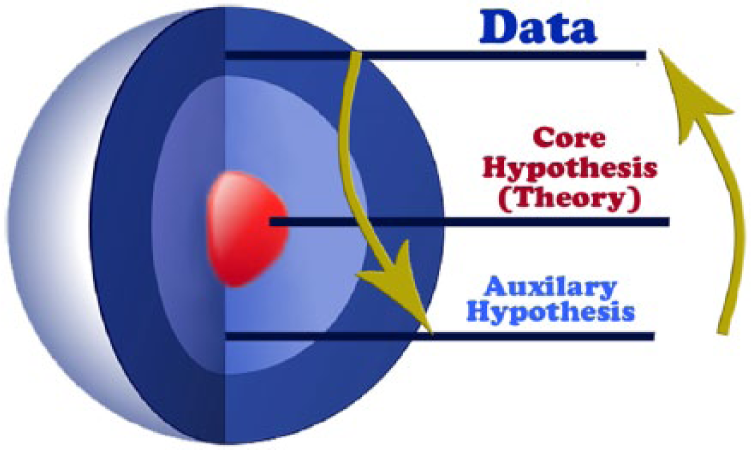
Lakatosian Research Programme. Illustration used with permission from John G Mohler.
A hypothesis is an essential starting point for a scientific investigation.
The hypothesis chosen has to be ‘answerable’ in the time frame of the experiment and the grant.
The experimental findings become part of core science as others confirm your findings.
Publish your study. If you do not publish it, you never did it.
Serendipity can advance medical knowledge
During my internship, I approached the Chairman of Medicine and Chief of Cardiovascular Disease at Georgetown University, Dr Charles Rackley, to discuss research ideas and mentorship. Dr Rackley was pursuing the clinical significance of a presumed molecule called endothelial-derived relaxing factor (EDRF), which was thought to promote dilation of arteries that may be abnormal in the setting of atherosclerotic disease. I assisted a cardiovascular fellow, Dr Frederick Kuhn, in recruiting and consenting patients and helping with the study protocol. During a cardiac catheterization, patients received an injection of a blood vessel dilator called acetylcholine and we found that those with atherosclerotic plaque had a paradoxical constriction of the artery rather than dilation as seen in healthy people. Furthermore, the constriction was most prominent when the high density lipoprotein (HDL) cholesterol was low. 1 As commonly seen with interesting study results, there were many other questions. In this case, why does having low HDL result in abnormal vascular function? And the more immediate question, what is the molecular structure of EDRF?
The race for the Nobel Prize was on around the world. The challenge was to determine the structure and production of EDRF. Three scientists, Drs Furchgott, Ignarro, and Murad, won the Nobel Prize in Medicine in 1998 for discovering that EDRF is nitric oxide. Dr Furchgott’s laboratory reported that if the lining of the endothelium is damaged, the artery constricts rather than dilates. This finding was serendipitous as the endothelium in one experiment was accidentally damaged, which revealed this surprise finding.
Do not ignore data that go against your hypothesis.
If an unusual observation occurs, see if you can repeat it.
All experiments should have a proper control to verify results.
Association does not determine causality
In 1993, observational studies supported the hypothesis that antioxidant vitamins reduce the risk of heart attack.2,3 At that time, Drs Daniel Steinberg, Joseph Witzum, and Peter Reaven at University of California, San Diego showed that oxidized low-density lipoprotein (LDL) cholesterol accumulated in the intimal layer of the artery wall more than non-oxidized LDL, due to a process called lipid peroxidation. 4 They hypothesized that perhaps antioxidants such as vitamins E and C could reduce LDL incorporation in the atherosclerotic plaque and prevent heart attacks.
The National Institutes of Health (NIH)-supported General Clinical Research Center granted me pilot funding to develop a simple test to measure LDL peroxidation and therefore detect cardiovascular risk. A byproduct of oxidation is generation of the hydrocarbon pentane in the breath. I worked with a scientist at a company who developed a mobile, briefcase-size gas chromatography (GC) machine that measured hydrocarbons, such as pentane, in industrial factories and fields. We had people breathe into an impermeable mylar bag, and the contents were inserted into the GC machine. I quickly learned that a controlled amount of pentane needed to be spiked into the machine, as there were hydrocarbons in the ambient air in the laboratory. It turned out that cigarette smokers had very high levels of breath pentane associated with lipid peroxidation. 5 Also, smokers had low levels of vitamins E and C in the blood. I speculated that cigarette smoking put a high demand on antioxidants, causing them to be depleted and therefore lower in the blood. However, a literature search revealed previous publications showing low blood levels of vitamins E and C in the diet of smokers. A typical smoker has a cigarette and cup of coffee in the morning, but no fruit – not even throughout the rest of the day. I thought: ‘Perhaps it is the combination of poor diet and oxidants in cigarette smoke that increases lipid peroxidation and cardiovascular risk’.
I then asked the question: ‘Could vitamins E and C reduce lipid peroxidation in cigarette smokers as measured with breath pentane and blood biomarkers?’. If it worked, perhaps it would lower the risk of heart attack and stroke in smokers. A small clinical study we conducted comparing vitamins E and C with placebo supplementation did not result in pentane reduction, indicating that cigarette smoke is an overwhelming oxidant stress. 6 Smoking anything, including cigarettes, cigars, or marijuana, will never be safe. The evidence is clear that cigarette smoking takes at least 10 years off your life. Large randomized clinical trials did not show a benefit of vitamins E and C to reduce heart attack and claudication symptoms.7,8
All good experiments are based on a solid testable hypothesis.
You may come up with ideas that need to be tested at the laboratory bench to support a clinical trial.
A randomized clinical trial is needed to confirm epidemiological findings.
Smoking anything is really bad for you.
Is calcification good, bad, or just ugly?
In conjunction with my mentor, Dr David Hathaway, we reported that bone-promoting proteins, including osteopontin, are present in diseased human aortic valves. 9 The nuances of conducting molecular research were taught to me by a post-doc, Dr Leonard Adam, who was working in Dr Hathaway’s laboratory. I learned quickly that similar to cooking food, research protocols are best served with experience.
After identifying bone-promoting proteins and osteoblast-like cells in aortic valves, I thought: ‘Could there be actual bone in the aortic valve?’. The calcium accumulation in the valve was described in the early 1900s as hydroxyapatite crystal. I took my idea to Dr Fred Kaplan, an expert in bone disease in the Orthopedic Surgery Department at Penn, and Dr Frank Gannon, a pathologist at Penn. We examined calcified valves removed at the time of heart surgery and identified ossification (bone formation), bone morphogenetic proteins (BMPs), and inflammation in calcified aortic valves. 10 We also detected cartilage in the calcified valves. In a similar study of atherosclerotic carotid plaques in the neck, bone formation was also present. 11 However, it is important to understand that experiments that show an association do not necessarily show causality. Interestingly, the amount of calcification in the valve was not as predictive of progression of disease as the inflammatory biomarker C-reactive protein (CRP). This led me to speculate if calcification in the vascular system is good, bad, or just ugly? 12
It is clear that coronary artery calcification on a computed tomography (CT) scan indicates the presence of atherosclerotic plaque and is associated with increased risk of heart attack. 13 One hypothesis is that calcification in arteries is not an innocent bystander but part of the pathological risk. An alternative hypothesis is that calcification of the coronary and carotid arteries is a biomarker of atherosclerotic disease but does not increase risk of plaque rupture and thrombosis.
In conjunction with my vascular surgery and pathologist colleagues at Penn, we conducted a study evaluating carotid artery atherosclerotic plaques removed at surgery. 11 The heavily calcified carotid plaques with minimal active inflammation were not associated with stroke, but the carotid plaques with inflammation and little calcification were the most dangerous. Current clinical data indicate that dystrophic calcification and bone formation in atherosclerotic plaques do not increase the risk of cardiovascular events but may be protective. Of note, a CT scan showing coronary calcification indicates the presence of atherosclerotic disease and increased risk of heart attack, but it is not necessarily the calcium that is bad.
Learn from experts in other areas of medicine to advance your ideas.
Association does not necessarily indicate causality.
Learn from research done in domains other than your own and apply the ideas to further your hypothesis.
Clinical equipoise can only be disproven with a randomized study
Another major research focus of mine was investigating the pathological mechanisms underlying claudication due to peripheral artery disease (PAD) and the testing of novel therapeutic approaches. Current treatment of claudication is initially a walking exercise program and, if not successful, consideration for revascularization. There are many studies showing the benefit of a walking exercise rehabilitation program for patients with claudication, but only a few studies compared exercise to revascularization with a stent. Dr Alan Hirsch and Dr Tim Murphy asked me to be a co-investigator on an NIH supported CLEVER study evaluating three treatments: the medicine cilostazol alone, cilostazol with exercise rehabilitation, or cilostazol with iliac artery revascularization. The recruitment of patients for the study was relatively difficult, as many physicians and patients thought opening up the iliac artery with a stent would be much better than exercise or medicine alone, and therefore, there was no equipoise. The results showed that patients who participated in a 6-month exercise rehabilitation program actually walked further on a treadmill than the other two groups. 14 The exercise group and the iliac stent group had improved quality of life compared to the cilostazol-alone group.
A randomized trial is needed to determine if equipoise is present for two therapies.
In a clinical trial where exercise is a treatment, it is vital to keep track of the amount of treatment each patient did during the study.
It is hard to improve on normal
Data indicate that an inflamed plaque is much more likely to rupture and cause a heart attack or stroke. An ongoing hypothesis is: ‘Will reducing plaque inflammation reduce rupture and adverse cardiovascular events?’. In conjunction with scientists at GlaxoSmithKline (GSK), including Dr Andrew Zalewski and Dr Colin MacPhee, Dr Robert Wilensky and I tested a new anti-inflammatory drug called darapladib on diabetic pigs with high cholesterol. The drug inhibits an enzyme called lipoprotein-associated phospholipase A2 (Lp-PLA2), which is bound to LDL and causes inflammation when entering the intimal layer of the artery. The pigs were given darapladib or placebo, and their blood vessels were stained for atherosclerotic plaque. Dr Wilensky showed me the slides without my knowledge about the randomization. It was very obvious which pigs received the study drug, and I joked, ‘We do not need a statistician to help with this study’. These impressive results 15 led to a phase 2 study. Along with Dr Andrew Zalewski, Dr Christie Ballantyne, Dr Michael Davidson, and others, we showed that the drug had a good safety profile. 16
The phase 3 study protocol was a placebo controlled trial in patients treated with current medical treatment, including statins, and irrespective of Lp-PLA2 levels. After reading the protocol, I was worried that the statin drugs would lower LDL and therefore the bound Lp-PLA2 would result in ‘normal’ enzyme levels and create a population that would not respond to the drug. To the credit of GSK, a committee was organized to ensure that all patients received optimal ‘background’ medications. I served on the committee and the mission was accomplished, as the overwhelming majority of patients were treated with statins, aspirin, blood pressure-lowering drugs, and diabetes drugs. Although darapladib lowered the number of heart attacks, it did not significantly change the combined primary endpoint, which included death. 17 Thus, it was considered a ‘negative’ trial. After years of work, the results were incredibly disappointing and GSK stopped studying the medication. I speculate that if only patients with elevated Lp-PLA2 levels were enrolled in the study it may have been a positive outcome. The problem with this idea is that a large number of patients would have to be screened and potentially be unable to take statin drugs due to side effects. The cost of this approach would likely be prohibitive. This research experience led me to coin the phrase, ‘It is hard to improve normal’.
Relhom’s law (first put forth by my father): all good ideas are met with resistance, and the corollary is – if an idea is met with no resistance, rethink it. (By the way, Relhom is Mohler spelled backwards.)
Background medical treatment that affects the target molecule may significantly confound the study.
It is hard to improve on normal.
Conclusion
There is no ‘I’ in research, as it takes a team to discover new cures in medicine. I listed several of the clinical investigators I worked with over the years, as I could not have done it alone. It gave me great joy to work with them. The next time you hear about a new discovery or treatment in the news, please recognize that it took many, many hard-working and dedicated people to make that happen.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.