
Abstract
We performed a meta-analysis to determine whether weekend admission and surgery for ruptured abdominal/thoracic aortic aneurysm (RAAA/RTAA) and acute aortic dissection (AAD) is associated with increased mortality. MEDLINE and EMBASE were searched from January 1946 to December 2016 using PubMed and OVID. Eligible studies were prospective or retrospective, comparative or cohort studies enrolling patients admitting or undergoing surgery for RAAA/RTAA/AAD and reporting mortality after weekend (including holiday) versus weekday admission/surgery. Our search identified 11 studies including a total of 166,195 patients. A pooled analysis of 13 adjusted odds ratios (ORs), one adjusted hazard ratio, and one unadjusted OR from all 11 studies demonstrated a statistically significant 32% increase in mortality with weekend admission/surgery (OR, 1.32; 95% confidence interval (CI), 1.20 to 1.45; p < 0.00001). Despite possible publication bias disadvantageous to weekend admission/surgery based on funnel plot asymmetry, adjustment for the asymmetry using the trim-and-fill method did not alter the significant association of weekend admission/surgery with increased mortality (OR, 1.21; 95% CI, 1.09 to 1.34; p = 0.0006). In conclusion, weekend admission/surgery for ruptured abdominal/thoracic aortic aneurysm and acute aortic dissection (AAD) may be associated with increased mortality.
Keywords
Introduction
Patients with ruptured abdominal/thoracic aortic aneurysm (ruptured AAA/TAA (RAAA/RTAA)) and acute aortic dissection (AAD) may be admitted to the hospital and then undergo emergency or urgent surgery on off-hours including weekends, holidays, and nights due to the sudden onset of diseases. Because of a shortage of staff1–3 and lack of experienced clinician expertise, 4 as well as inadequate subspecialty care 5 and therapeutic 6 or diagnostic procedures, 4 off-hour admission may be associated with increased mortality and other adverse outcomes, 7 which has been called the ‘off-hour effect’. 8 A previous meta-analysis 7 of 251 cohorts from 140 articles (including six data sets from five studies4,9–12 enrolling a total of 36,214 patients with aortic aneurysm) suggests that off-hour admission is associated with an increased mortality risk. Recent published studies, however, demonstrated no significant increase in mortality with weekend emergency/urgent open surgical repair (OSR) for AAA 13 and weekend admission for RAAA. 14 In the present article, we performed a meta-analysis to determine whether weekend admission and surgery for RAAA/RTAA/AAD is associated with increased mortality.
Materials and methods
Search strategy
All studies investigating associations of weekend admission/surgery for RAAA/RTAA/AAD with mortality were identified using a two-level search strategy. First, MEDLINE and EMBASE were searched from January 1946 to December 2016 using web-based search engines (PubMed and OVID). Second, relevant studies were identified through a manual search of secondary sources including references of initially identified articles and a search of reviews and commentaries. All references were downloaded for consolidation, elimination of duplicates and further analysis. Search terms included ‘weekend’, ‘aortic’, and ‘aneurysm’, ‘rupture’, or ‘dissection’.
Study selection and data extraction
Studies considered for inclusion met the following criteria: the design was a prospective or retrospective, comparative or cohort study; the study population was patients admitting or undergoing surgery for RAAA/RTAA/AAD; and outcomes included mortality after weekend (including holiday) versus weekday admission/surgery. Data regarding detailed inclusion criteria, duration of follow-up, and mortality were extracted from each individual study. Data were extracted in duplicate by two investigators (HT, TA) and independently verified by a third investigator (TU). Disagreements were resolved by consensus.
Statistical analysis
We conducted a meta-analysis of summary statistics from the individual studies. For each study, adjusted odds ratios (ORs) (if unavailable, alternatively hazard ratios (HRs)) and 95% confidence intervals (CIs) of mortality for the weekend versus weekday groups were extracted. When adjusted ORs/HRs were unavailable, data regarding mortality in both weekend and weekday groups were used to generate ORs and 95% CIs. Study-specific estimates of logarithmic ORs were combined using the random-effects model. We decided that ORs and HRs were similar enough to combine based on the judgement in the context of the aims of the present meta-analysis. 15 Between-study heterogeneity was analyzed by means of the I2 index, with values on the order of 25%, 50%, and 75% considered as low, moderate, and high heterogeneity, respectively. Funnel plot asymmetry was assessed mathematically using an adjusted rank-correlation test of Begg and Mazumdar 16 and a linear regression test of Egger et al. 17 As one of sensitivity analyses, we also performed the non-parametric ‘trim-and-fill’ procedure 18 to further assess the possible effect of funnel plot asymmetry in our meta-analysis. This method considers the possibility of hypothetical ‘missing’ studies that might exist, imputes their relative-risk estimates, and recalculates a pooled relative-risk estimate that incorporates the hypothetical missing studies as though they actually existed. All analyses were conducted using Review Manager version 5.3 (available from http://tech.cochrane.org/revman) and Comprehensive Meta-Analysis version 3 (Biostat, Englewood, NJ, USA).
Results
Search results
Of 20 potentially relevant articles screened initially, our search identified 11 eligible studies4,9–14,19–22 enrolling a total of 166,195 patients (Tables 1 and 2; Supplemental Tables S1 and S2). Seven studies were conducted in North America (five in the US9,12,13,19,20 and two in Canada4,22), two in Italy,10,11 one in England and Sweden, 14 and one in Poland. 21 Patients undergoing surgery were exclusively included in five studies13,14,20–22 and those with RAAA were exclusively enrolled in six.4,13,14,20–22 Only a study by Dueck et al. 22 included patients undergoing ‘after-hours’ RAAA repairs, which were defined as operations performed on week nights between 18:00 and 07:00, weekends, and holidays, and was determined with a supplemental fee code (E409 and E410) in the OHIP (Ontario Health Insurance Plan) database. In-hospital mortality was reported in nine studies,4,9–13,19–21 30-day mortality in one, 22 and 90-day mortality in one, 14 and we combined these as ‘early’ mortality. Because Glance et al. 13 reported four ORs (for subgroups of emergency open, urgent open, emergency endovascular, and urgent endovascular AAA repair) and Karthikesalingam et al. 14 provided two ORs (for patients in England and those in Sweden), 15 relative-risk estimates from 11 studies were available. We extracted 13 adjusted ORs,4,9–14,19,20 one adjusted HR, 22 and one unadjusted OR. 21
Study design.

Patients recorded as having their operation on the weekend if they were admitted on the weekend and underwent surgery on the day of admission.
AAA, abdominal aortic aneurysm; AAD, acute aortic dissection; CIHI, Canadian Institute for Health Information; COSHPDDDF, California Office of Statewide Health Planning and Development Discharge Data File; HES, Hospital Episode Statistics; NDH, National Discharge Hospital; NIS, Nationwide Inpatient Sample; OHIP, Ontario Health Insurance Plan; OPHRDC, Ontario Physician Human Resources Data Center; RAAA, ruptured AAA; RER, Region Emilia Romagna; SEDD, State Emergency Department Databases; SID, State Inpatient Databases; Swedvasc, Swedish Vascular Registry; TAA, thoracic aortic aneurysm.
Patient characteristics and mortality.
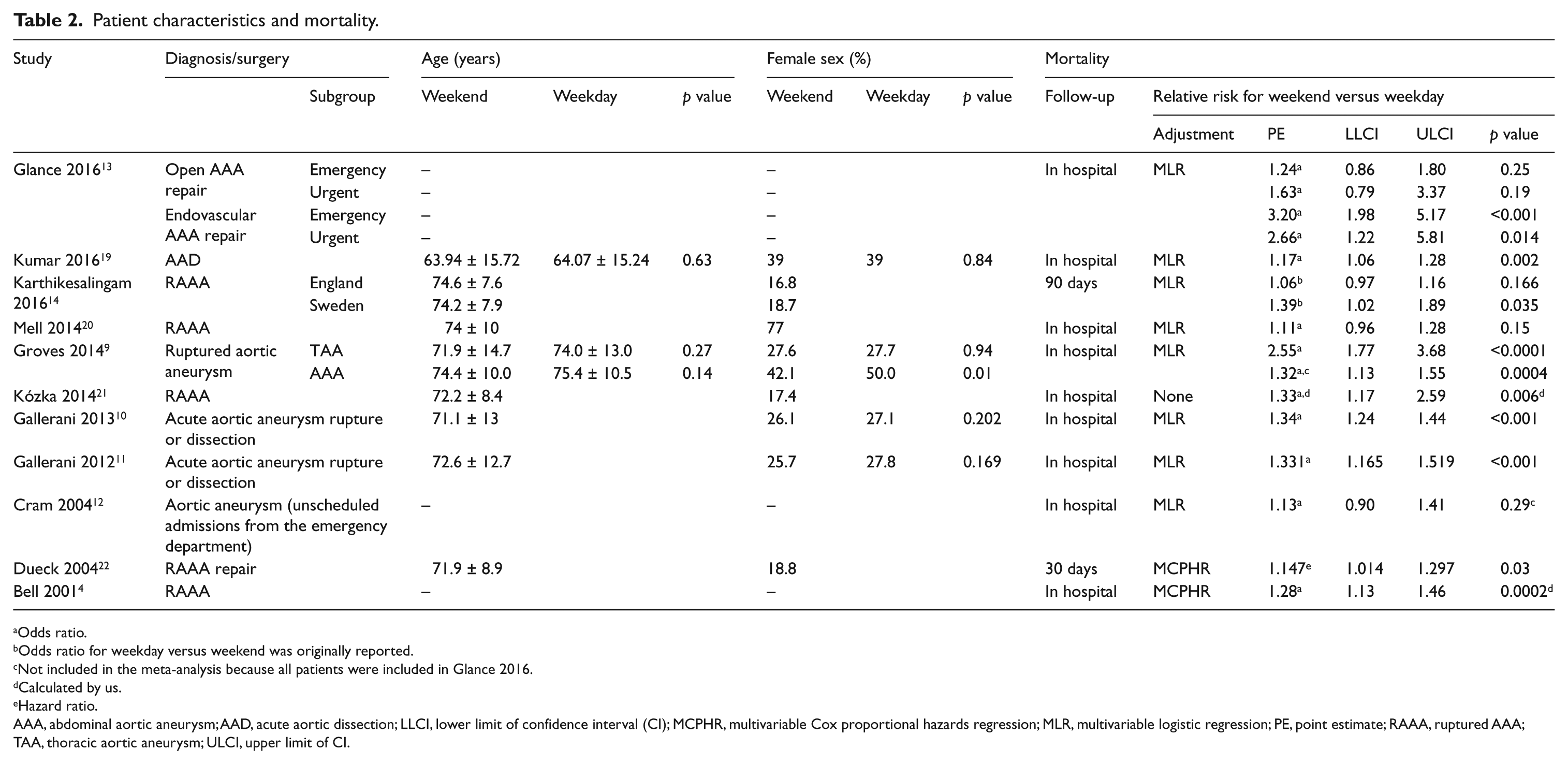
Odds ratio.
Odds ratio for weekday versus weekend was originally reported.
Not included in the meta-analysis because all patients were included in Glance 2016.
Calculated by us.
Hazard ratio.
AAA, abdominal aortic aneurysm; AAD, acute aortic dissection; LLCI, lower limit of confidence interval (CI); MCPHR, multivariable Cox proportional hazards regression; MLR, multivariable logistic regression; PE, point estimate; RAAA, ruptured AAA; TAA, thoracic aortic aneurysm; ULCI, upper limit of CI.
Main findings
A pooled analysis of 15 relative-risk estimates from all 11 studies4,9–14,19–22 demonstrated a statistically significant 32% increase in mortality with weekend admission/surgery (primary meta-analysis; OR, 1.32; 95% CI, 1.20 to 1.45; p < 0.00001; Figure 1). There was high between-study heterogeneity of results (I2 = 77%).
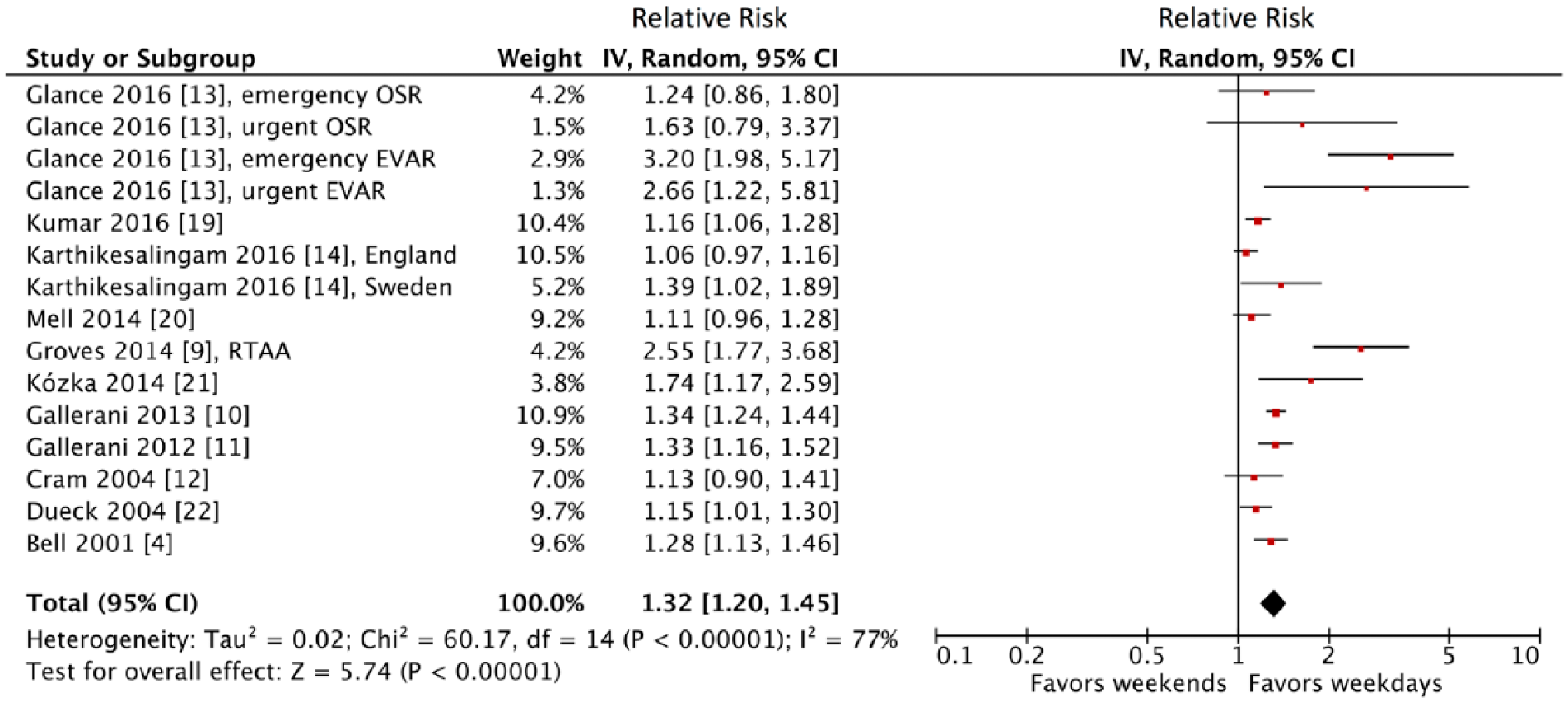
Forest plot of 15 relative-risk estimates of mortality from all 11 studies4,9–14,19–22 (primary meta-analysis). Numbers in brackets are reference numbers. CI, confidence interval; EVAR, endovascular aneurysm repair; IV, inverse variance; OSR, open surgical repair; RTAA, ruptured thoracic aortic aneurysm.
Sensitivity analyses
To assess the impact of qualitative heterogeneity in study design and patient selection on the pooled effect estimate, we performed several sensitivity analyses. We excluded the study by Dueck et al. 22 enrolling patients undergoing ‘after-hours’ (not only weekends and holidays but also week nights) RAAA repairs, and combining the remaining 14 relative-risk estimates generated a statistically significant result disadvantageous to weekend admission/surgery (OR, 1.35; 95% CI, 1.21 to 1.49; p < 0.00001). In general, exclusion of any single relative-risk estimate from the primary meta-analysis (one-study-removed meta-analysis) did not substantively alter the result (Supplemental Figure S1).
Seven studies were conducted in North America (five in the US9,12,13,19,20 and two in Canada4,22), two in Italy,10,11 one in England and Sweden, 14 and one in Poland. 21 Pooling 10 relative-risk estimates from the seven studies conducted in North America4,9,12,13,19,20,22 indicated a statistically significant disadvantage for weekend admission/surgery (OR, 1.37; 95% CI, 1.19 to 1.58; p < 0.001; I2 = 78%; Supplemental Figure S2).
Patients undergoing aortic repair were exclusively included in five studies.13,14,20–22 Combining nine relative-risk estimates from the five studies exclusively including patients undergoing surgery13,14,20–22 demonstrated a statistically significant increase in mortality with weekend admission/surgery (OR, 1.35; 95% CI, 1.15 to 1.89; p = 0.0002; I2 = 75%; Supplemental Figure S3).
Four studies9–11,19 enrolled both patients undergoing aortic repair and those not doing (Supplemental Table S1). In a study by Kumar et al. 19 enrolling exclusively patients with AAD, the overall utilization of surgical or endovascular aortic repair for all hospitalizations was 47.2%, and weekend hospitalization was associated with a significantly lower utilization of aortic repair compared with weekday hospitalization (adjusted OR, 0.76; 95% CI, 0.71 to 0.82; p < 0.001). Of the patients who underwent aortic repair, a significantly higher proportion was performed on the day of admission (day 0) for weekday compared with weekend admissions (55% vs 51%; p = 0.007), and this difference remained significant on day 1 (70% vs 67%; p = 0.007) and day 2 of hospitalization (74.5% vs 71.6%; p = 0.01). 19 Groves et al., 9 however, found no significant difference in the use of any procedural repair (endovascular or open repair) in those with RAAA (61.4% for the weekends vs 59.2% for the weekdays; p = 0.14) but did find that those admitted on the weekends with RTAA had significantly fewer procedural interventions (34.8% vs 49.4%; p < 0.001). In a study by Gallerani et al. 10 including AAD or aortic rupture, there was no significant difference in cardiovascular operations between weekend and weekday admission (50.7% vs 60.3%; p = 0.315). Also, in another study by Gallerani et al., 11 no weekend/weekday differences were found in the percentage of patients undergoing surgical procedure of repair, either for AAD (46.4% vs 47.1%; p = 0.788) or aortic rupture (75.1% vs 75.7%; p = 0.823). In total, of these four studies,9–11,19 aortic repair in the weekend group (46.6%) was performed significantly (p < 0.00001 by χ2 tests) less than that in the weekday group (51.1%). Although aortic repair was adjusted for using multivariable analyses in two10,19 of the four studies,9–11,19 the impact of aortic repair on early mortality was not reported.
Patients with RAAA were exclusively enrolled in six studies.4,13,14,20–22 Pooling 10 relative-risk estimates from the six studies exclusively enrolling patients with AAA4,13,14,20–22 generated a statistically significant result disadvantageous to weekend admission/surgery (OR, 1.32; 95% CI, 1.16 to 1.52; p < 0.0001; I2 = 74%; Supplemental Figure S4). Three studies9,11,12 included patients with RTAA as well as RAAA9,11,12 and AAD. 11 Only one study 9 of these reported the impact of weekend admission/surgery in patients with RTAA separately. Patients admitted on the weekend with ruptured aortic aneurysm had a greater than 2.5-fold increase in the odds of dying compared with those admitted on a weekday for RTAA (OR, 2.55; 95% CI, 1.77 to 3.68; p < 0.0001) and a 32% higher chance of death for RAAA (OR, 1.32; 95% CI, 1.13 to 1.55; p = 0.0004). 9
Combining 12 relative-risk estimates from the nine studies reporting in-hospital mortality4,9–13,19–21 indicated a statistically significant disadvantage for weekend admission/surgery (OR, 1.39; 95% CI, 1.24 to 1.55; p < 0.00001; I2 = 75%; Supplemental Figure S5).
Three studies9,13,14 enrolled both patients with RAAA undergoing open aortic repair and those doing endovascular aortic repair. In total, of these three studies,9,13,14 endovascular aortic repair in the weekend group (18.2%) was performed significantly (p < 0.00001 by χ2 tests) less than that in the weekday group (30.8%). Although endovascular aortic repair was adjusted for using multivariable analyses in only one 14 of these studies,9,13,14 the impact of endovascular aortic repair on early mortality was not reported.
We generated a funnel plot of the logarithm of relative-risk estimate versus the precision (reciprocal of standard error) for each study (Figure 2) to assess its asymmetry. Both the adjusted rank correlation test 16 (two-tailed p with continuity correction = 0.0048) and the linear regression test 17 (two-tailed p = 0.03) revealed funnel plot asymmetry disadvantageous to weekend admission/surgery, which raises the possibility of publication bias. Thus, we undertook a sensitivity analysis using the trim-and-fill method, 18 which conservatively imputes hypothetical negative unpublished studies to mirror the positive studies. The imputed five studies produce a symmetrical funnel plot (Figure 2). The pooled analysis incorporating the five hypothetical studies did not substantively alter the result of the primary meta-analysis and continued to show a statistically significant increase in mortality with weekend admission/surgery (OR, 1.21; 95% CI, 1.09 to 1.34; p = 0.0006).
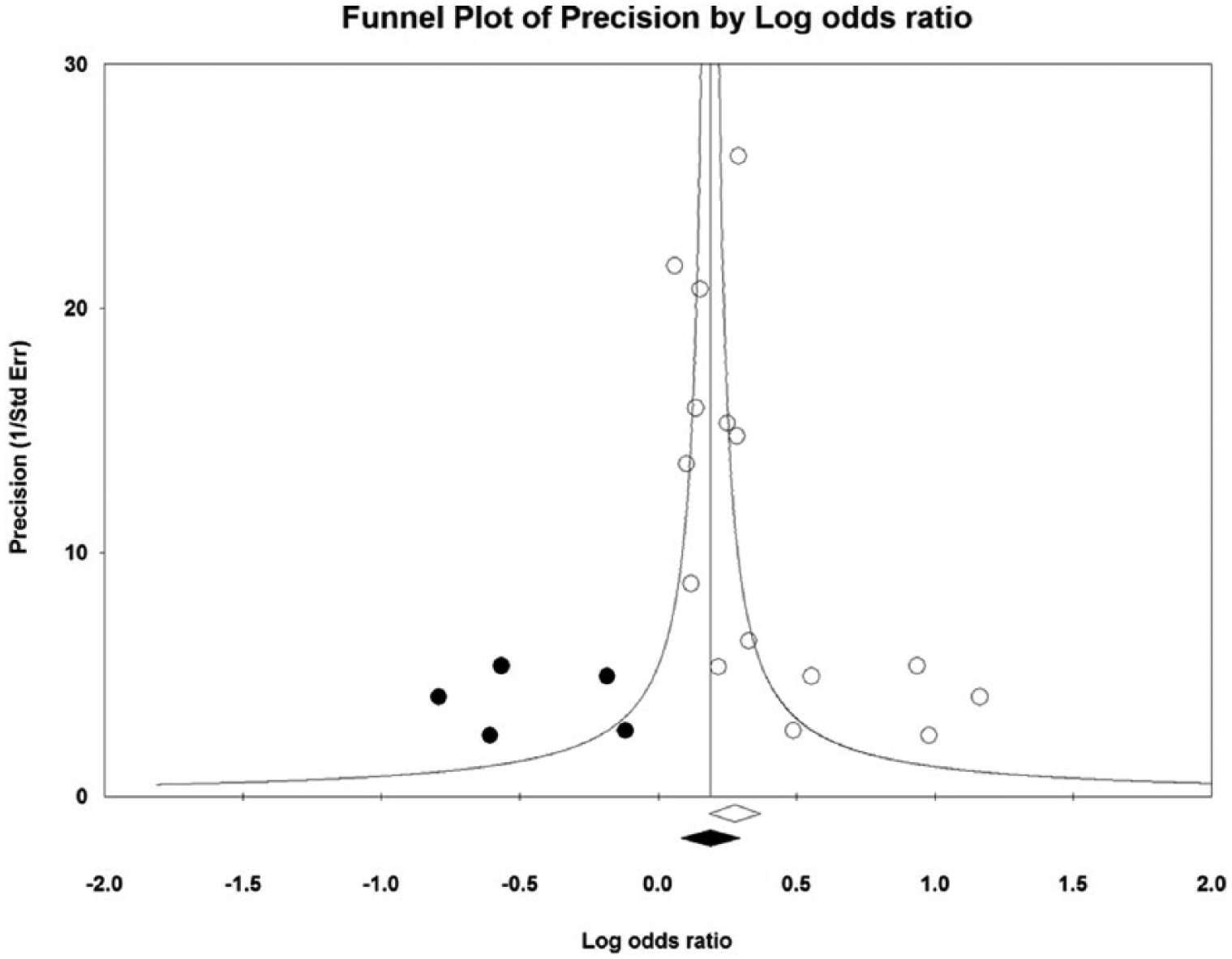
Funnel plot of the logarithm of relative-risk estimate versus the precision (reciprocal of standard error) for each study, with adjustment using the trim-and-fill method. 18 Open circles and an open rhombus denote identified studies and their summary measure, respectively. Closed circles and a closed rhombus denote estimated missing studies after adjustment for funnel plot asymmetry and the summary measure incorporating the hypothetical studies, respectively.
Discussion
The results of the present meta-analysis suggest that weekend admission/surgery for RAAA/RTAA/AAD may be associated with increased mortality, which was robust in sensitivity analyses. Despite possible publication bias disadvantageous to weekend admission/surgery based on funnel plot asymmetry, adjustment for the asymmetry using the trim-and-fill method 18 did not alter the significant association of weekend admission/surgery with increased mortality.
Findings from the meta-analysis 7 of 251 cohorts from 140 articles showed that off-hour (weekend and night) admission was associated with increased mortality for aortic aneurysm (OR, 1.52; 95% CI, 1.30 to 1.77) as well as some diseases (i.e. breast cancer, leukemia, respiratory neoplasm, pancreatic cancer, malignant neoplasm of genitourinary organs, colorectal cancer, pulmonary embolism, arrhythmia and cardiac arrest, lymphoma, renal failure, traumatic brain injury, heart failure, intracerebral hemorrhage, subarachnoid hemorrhage, stroke, gastrointestinal bleeding, myocardial infarction, chronic obstructive pulmonary disease, and bloodstream infections). Whereas, no association was found for other diseases (i.e. hip fracture, pneumonia, intestinal obstruction, aspiration pneumonia, peptic ulcer, trauma, diverticulitis, and neonatal mortality). 7 The present result (32% increase in mortality with weekend admission/surgery) is comparable to the finding (52% increase with off-hour admission) of the previous meta-analysis. 7 Although the previous meta-analysis 7 included six data sets from five studies for aortic aneurysm enrolling a total of 36,214, the present meta-analysis included 15 data sets from 11 studies for RAAA/RTAA/AAD including a total of 159,156 patients.
The weekend effect is a complex phenomenon that has major implications for the organization of health services, and its magnitude and underlying mechanisms have been subject to heated debate. 23 The off-hour (including weekends) effect may be exacerbated, particularly when optimal patient care requires an increase in medical resources. 7 There were significant off-hour effects for conditions such as malignancies and acute illnesses (including RAAA/RTAA/AAD), where the amount of medical resources required were great and advanced medical technology for diagnosis and treatments were required. 7 There are several plausible explanations for the weekend effect. First, as compared with weekday teams (of surgeons, anesthesiologists, and nurses), weekend call teams may have less expertize to care for specific surgical problems. 13 On weekends, on-call anesthesiologists and surgeons may respond to surgical procedures not typically covered on weekdays. 13
Second, in comparison with weekdays, attending anesthesiologists may cover more cases and supervise more extenders (nurse anesthetists or residents) on weekends, especially when patients requiring emergency surgery are added to the schedule. 13 When one of the cases develops an intraoperative complication on weekdays, decompression of the workload for an individual anesthesiologist is usually possible so as to focus his or her efforts on that case; whereas it may be impossible on weekends because the number of available staff is limited. 13
Third, weekend postoperative-care-unit staffing may be lower, and lower nurse-staffing levels are associated with worse outcomes. 13 There is a statistically and clinically significant association between registered nurse staffing (registered nurse-to-patient ratios) and adjusted ORs of hospital-related mortality, failure to rescue, and other patient outcomes, which is consistent in surgical patients and in intensive care units. 24 Non-emergent major surgery when performed on Friday, when compared with that performed on Monday through Wednesday, is associated with 17% higher adjusted odds of death within 30 days for patients who were admitted after surgery to regular hospital floors, 25 which fits with the hypothesis that the postsurgical-care quality is lower on weekends in comparison with weekdays. 13 The adjusted odds of death in the 30 days after elective surgical procedures were 44% and 82% higher if the procedures were carried out on Friday or at the weekend, respectively, compared with Monday, 26 which suggests that the effect of performing surgery on weekends differs from the impact of weekend postsurgical care. 13
Finally, the Accreditation Council on Graduate Medical Education (ACGME) regulations (limiting resident work-weeks to 80 hours or fewer and limiting continuous duty to 24 hours, with 6 additional hours for transfer of care) were associated with decreased short-term mortality among high-risk medical patients in teaching hospitals. 27 Physician hours spent working on the weekends in addition to regular weekday hours and physician fatigue may be associated with worse patient outcomes. 13 The ACGME regulations, however, were associated with improved outcomes in medical patients but not in surgical patients, which may be explained by the following: (1) surgical residency programs may not have altered their working conditions substantially; (2) if the number of surgical residents remained fixed and each resident worked less, the average number of available providers would decline; and (3) errors due to fatigue may have been counterbalanced by problems with transfers of care. 27
Limitations
Our analysis must be viewed in the context of its limitations. First, the present results may be influenced by a publication bias disadvantageous to weekend admission/surgery. Although this risk was minimized through an exhaustive search of the available literature, the statistical tests indicated publication bias. Adjustment using the trim-and-fill method, 17 however, still demonstrated a significant association of weekend admission/surgery with increased mortality.
Second, heterogeneity was observed among included studies. Heterogeneity across cohorts may result from differences in the healthcare system, care delivery models, staffing or resource availability, and types of facility in different countries.7,28 Discrepancies in patient demographics and different definitions of weekends or nights may also be causes of unexplained heterogeneity.7,29,30 In sensitivity analyses, however, excluding the study by Dueck et al. 22 enrolling patients undergoing ‘after-hours’ (not only weekends and holidays but also week nights) surgery (Supplemental Figure S1), pooling the seven studies conducted in North America4,9,12,13,19,20,22 (Supplemental Figure S2), combining the five studies exclusively including patients undergoing surgery13,14,20–22 (Supplemental Figure S3), pooling the six studies exclusively enrolling patients with AAA4,13,14,20–22 (Supplemental Figure S4), and combining the nine studies reporting in-hospital mortality4,9–13,19–21 (Supplemental Figure S5) did not significantly modify the estimated weekend effects.
Third, all of the included studies were conducted in North America4,9,12,13,19,20,22 and Europe,10,11,14,21 where the medical resources are relatively more adequate compared with low-/middle-income countries. Thus, it is unclear whether the results are generalizable to low-/middle-income countries, and future studies are required in resource-limited settings. 7
Finally, most of studies included in the present meta-analysis were conducted using several administrative data such as the CIHI (Canadian Institute for Health Information),4,22 the COSHPDDDF (California Office of Statewide Health Planning and Development Discharge Data File) 12 the HES (Hospital Episode Statistics), 14 the NDH (National Discharge Hospital), 10 the NIS (Nationwide Inpatient Sample),9,13,19 the OHIP (Ontario Health Insurance Plan), 22 the OPHRDC (Ontario Physician Human Resources Data Center), 22 the RER (Region Emilia Romagna), 11 the SEDD (State Emergency Department Databases), 20 the SID (State Inpatient Databases), 20 and the Swedvasc (Swedish Vascular Registry). 14 Using an administrative database makes it susceptible to errors in coding and temporal variability in coding practices, and not accessing clinical data including physiological, laboratory, and imaging data makes it impossible to adjust for clinical confounders. 19 Because the NIS specifies weekend versus weekday admission (and not the actual day of the week), researchers need to exclude patients who were admitted on the weekend and did not have their surgery on the day of admission to avoid misclassifying patients admitted on Sunday and undergoing their operation on Monday as weekend surgeries, which decreases the power of the analysis but is unlikely to have introduced a bias. 13
Conclusion
Weekend admission/surgery for ruptured abdominal/thoracic aortic aneurysm and acute aortic dissection may be associated with increased mortality.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.