
Abstract
Peripheral artery disease (PAD) is associated with poor health status (symptoms, functioning, quality of life (QOL)). Whether sex differences exist in PAD-specific health status is unknown. In patients presenting to a specialty clinic with new-onset or recent exacerbation of PAD, we examined sex differences as assessed by the Peripheral Artery Questionnaire (PAQ). The Patient-centered Outcomes Related to TReatment Practices in Peripheral Arterial Disease: Investigating Trajectories (PORTRAIT) study is a multicenter, international prospective study of patients with new or worsening PAD symptoms. Baseline characteristics and mean PAQ scores were compared among women (n=481) and men (n=793) before they underwent treatment. The independent association of sex with health status was assessed with multivariable linear regression. As compared with men, women were less often Caucasian, married and employed, and more often lacking health insurance, living alone (36.2% vs 23.6%, p<0.001), had depression and avoided care due to cost (17.0% vs 12.3%, p=0.018). Women and men were of a similar age and education level, and had similar ankle–brachial index (ABI) values (0.7 ± 0.2 in both groups, p=0.052). Female sex was independently associated with lower PAQ scores on all domains (physical functioning adjusted mean difference of −8.40, p<0.001; social functioning adjusted mean difference of −6.8, p<0.001; QOL adjusted mean difference of −6.7, p<0.001), although no differences were observed in treatment satisfaction (adjusted mean difference −0.20, p=0.904). Despite similar ABIs, women presenting with symptoms of PAD had poorer PAD-specific functioning as compared with men, impacting all major health status domains, independent of socio-economic and clinical characteristics.
Introduction
Peripheral artery disease (PAD) affects ~8 million Americans over 40 years of age with rising rates among the elderly and among women.1–3 A comprehensive systematic assessment of PAD mortality and disability-adjusted life years (DALYs) has shown that mortality and disability rates associated with PAD have increased over the last 20 years, which has been even greater among women than men. 4
Patients with PAD report profound limitations in all domains of health that are worse than among those with chronic pulmonary disease and heart failure;5,6 however, little is understood about factors that influence health status (symptoms, functioning, and quality of life) in patients with PAD and whether these factors are similar for women and men with claudication. Studies that looked at the impact of PAD on patients’ health were often small,7,8 used generic instruments, and none of these studies have looked at PAD-specific health status in women in larger populations.
The Patient-centered Outcomes Related to TReatment Practices in Peripheral Arterial Disease: Investigating Trajectories (PORTRAIT) study was designed to examine the characteristics of patients with new or worsening PAD symptoms as well as the variation in practice patterns of evidence-based PAD treatments, and to study its impact on health outcomes. We used the PORTRAIT study data to examine sex differences with regards to disease-specific and overall health status at the time of presentation to a vascular specialist. A better knowledge of sex differences in patients’ PAD-specific health status can lay the foundation for developing strategies to achieve sex-specific cardiovascular risk reduction and improve health outcomes in women with PAD.
Methods
Patient population and study design
PORTRAIT is a multicenter, international prospective study of patients presenting to a vascular outpatient clinic with new or worsening claudication. PORTRAIT included patients based on ankle–brachial index (ABI) criterion regardless of whether their symptoms were typical or atypical. For typical symptoms, we adopted the Rose claudication definition.9,10 As a longitudinal study, PORTRAIT was designed to address quality of care and health status outcomes in patients with PAD, with an ultimate goal to create evidence-based management algorithms that would tailor therapy to individual patients. Patients aged 21 years or older, consulting a PAD specialist (vascular surgeon, vascular medicine specialist, radiologist or cardiologist) with a new-onset or a recent exacerbation of exertional leg symptoms, and an abnormal resting ABI (⩽0.90) 11 or a significant drop in post-exercise ankle pressure of ⩾20 mmHg, 12 were included. New onset PAD was defined as no prior documented diagnosis of PAD. Exacerbation of symptoms was defined as a positive history of PAD with no prior invasive procedure in the ipsilateral symptomatic leg within the year that precedes presentation. Those with a non-compressible ABI, critical limb ischemia, who did not speak English/Spanish/Dutch, who were hard of hearing, or were unable to provide informed consent were excluded. No patients completed the questionnaire in Spanish; 30% of patients (n=383) completed the questionnaire in Dutch. The Dutch version underwent extensive validation work both from a psychometric standpoint as well as from a clinical perspective.13,14 Patients hard of hearing were excluded (n=23) due to the requirement of serial phone interviews for follow-up data.
Patients were enrolled upon first visiting the PAD clinic, before treatment was started. The PORTRAIT study was approved by the institutional review boards (IRBs) of all participating centers. Written informed consent or telephone consent was obtained according to a protocol that was approved by the IRBs of the participating sites. Study coordinators at each center performed the baseline interview at the outpatient clinic or over the phone and documented demographic, clinical and treatment information from patients’ medical records and obtained information about patients’ socio-economic, psychosocial and health status from standardized interviews. Information about age, sex, risk factors, comorbid conditions and race/ethnicity was obtained from patients’ medical records. Baseline data included degree of claudication (Rutherford grade I, categories 1, 2 or 3) 15 and resting ABI for all patients. Follow-up interviews were performed by phone at 3, 6 and 12 months, and records from all cardiovascular hospitalizations were obtained for documentation of admission, procedures and treatment that occurred during follow up. Data management was facilitated by an integrated, internet-based, data collection infrastructure (Velos eResearch; Velos Inc., Fremont, CA, USA), which was secure and compliant with HIPAA regulations.
Health status measurement
The construct that we are measuring in this study is PAD-specific health status, which is multidimentional. Health status consists of domains referring to patients’ symptoms, physical functioning and quality of life (QOL) as it relates to their health. In order to assess the impact of PAD on population health we used a validated tool: the Peripheral Artery Questionnaire (PAQ). 16 The PAQ is a 20-item questionnaire that assesses six health status domains relevant to patients with PAD: symptoms, recent changes in symptoms, physical limitations due to claudication, treatment satisfaction, social functioning, and QOL. A summary score is calculated as the average of the physical limitations, symptoms, QOL, and social functioning scores. Scores range from 0 to 100; higher scores indicate less functional limitation, fewer symptoms, better treatment satisfaction, higher social functioning and better QOL. 17
Generic health status was assessed with the EQ-5D, 18 which is a validated generic instrument that uses five different dimensions of health assessment (mobility, self-care, usual activities, pain or discomfort, and anxiety/depression) and a visual analogue scale (VAS) that rates individuals’ perception of their overall health. EQ-5D can be used as a summarized index to measure health status from a patient’s perspective.
Data analysis
Baseline characteristics were assessed in all patients according to sex, including demographics, socio-economic factors (marital status, educational level, living alone, employment status, financial status), clinical comorbidities (cardiovascular risk factors, kidney disease, lung disease, chronic back pain, osteoarthritis), medication use, depression, access to care, severity of claudication, and ABIs.
Baseline characteristics and mean PAQ scores were compared in women versus men using Student’s t-test for continuous variables and chi-squared or Fisher’s exact tests for categorical variables. Symptoms and individual PAQ domains and PAQ summary scores were assessed according to sex. Hierarchical, multivariable linear and logistic regression models were performed to incorporate baseline variables including sex and their effect on PAQ scores and typical presentation, respectively.
Missing data
Missing information on one or more covariates was present for 308 (24.2%) patients; 16 patients were missing more than one value. Missing data were electronic medical record (EMR) related (such as undocumented BMIs). Missing covariate data were assumed to be missing at random and were imputed using multiple imputation methods. The imputation model consisted of all variables used in the multivariable model. Analyses were replicated on five imputed data sets and pooled to obtain final model estimates. All analyses were conducted using SAS v9.4 (SAS Institute, Inc., Cary, NC, USA) and IVEware (Institute for Social Research, Ann Arbor, MI, USA). Statistical significance was evaluated at a two-sided significance level of <0.05.
Results
A total of 1275 patients were enrolled between June 2011 and October 2015 at 16 participating sites including nine US centers, six centers in the Netherlands and one center in Australia. Of the 1275 patients, 1162 (91.1%) met the resting ABI inclusion criterion. The remaining 113 patients (8.9%) were included based on the post-exercise drop in ankle pressure. Of those who were included based on post-exercise results, 81% used the motorized treadmill test, 2% used the Six-Minute Walk test, and 17% used the active pedal plantar flexion test.
Among PORTRAIT participants, 1274 patients had complete PAQ data at baseline, of whom 481 (38%) were women. One patient missing all components of PAQ was excluded. The baseline demographics and social determinants of health according to sex are shown in Table 1, PAD-related variables at presentation according to sex are shown in Table 2, and comorbidities and medications at baseline according to sex are shown in Table 3. Men and women had a similar age, level of education, and medical history including heart failure, angina, diabetes, atrial fibrillation, stroke, chronic kidney disease, cancer, and chronic back pain. Men and women also had similar Rutherford class of claudication and ABI results (Table 2).
Baseline demographics and social determinants of health.
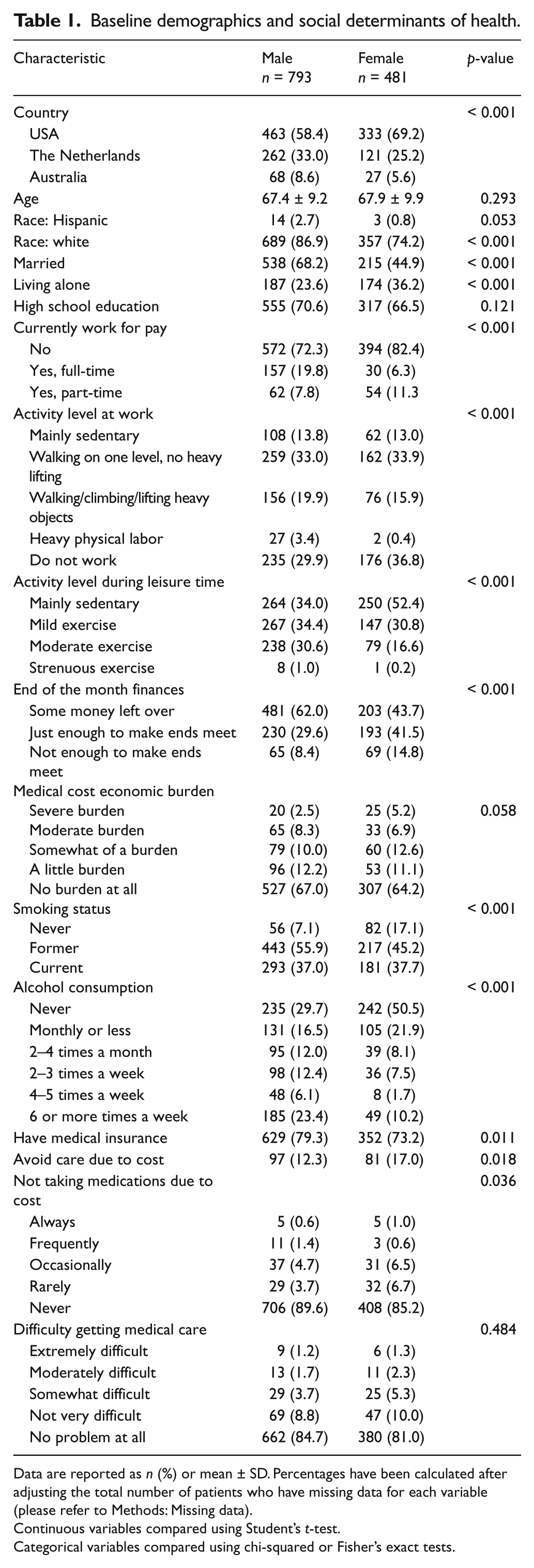
Data are reported as n (%) or mean ± SD. Percentages have been calculated after adjusting the total number of patients who have missing data for each variable (please refer to Methods: Missing data).
Continuous variables compared using Student’s t-test.
Categorical variables compared using chi-squared or Fisher’s exact tests.
Peripheral artery disease variables at presentation.
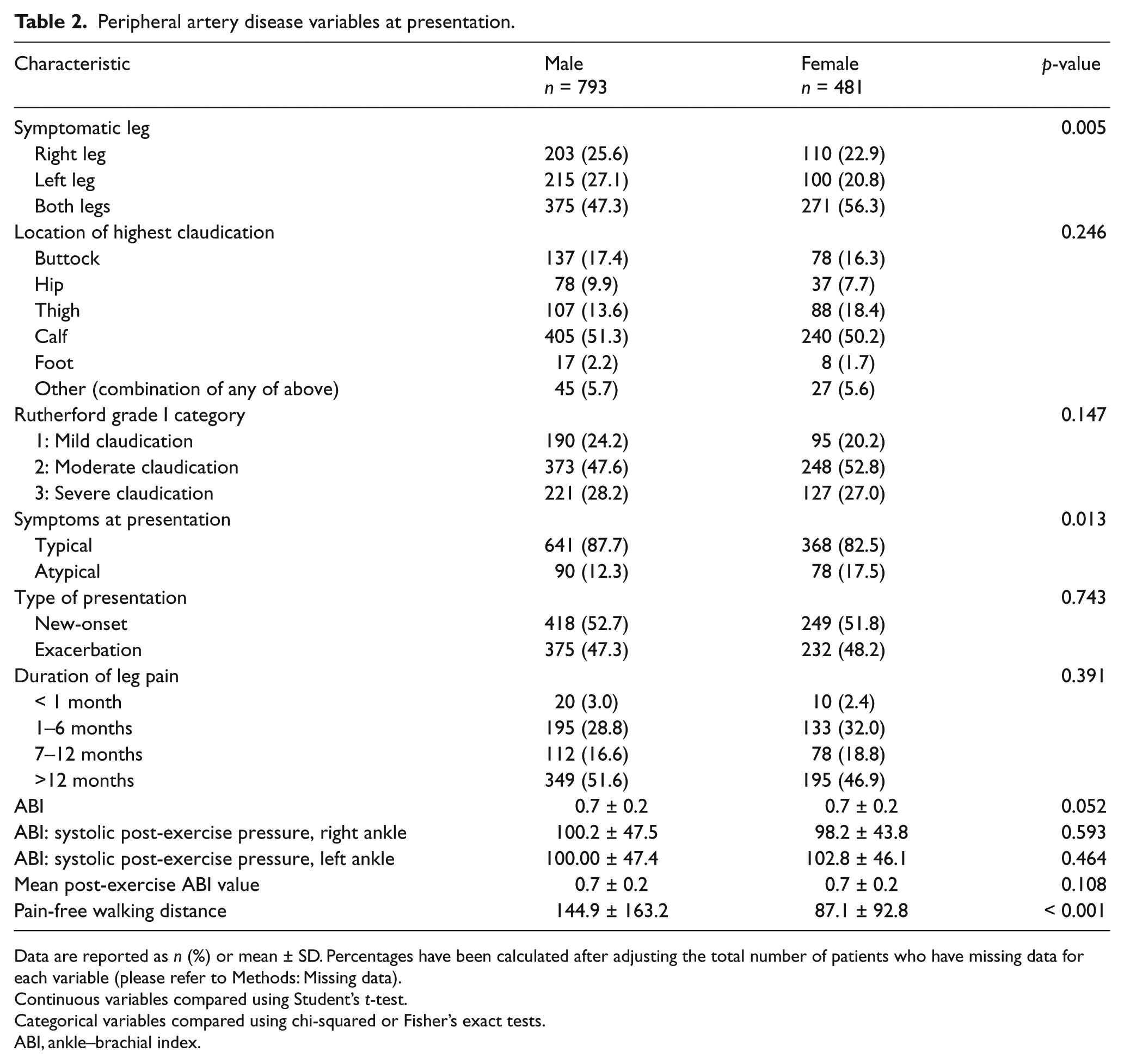
Data are reported as n (%) or mean ± SD. Percentages have been calculated after adjusting the total number of patients who have missing data for each variable (please refer to Methods: Missing data).
Continuous variables compared using Student’s t-test.
Categorical variables compared using chi-squared or Fisher’s exact tests.
ABI, ankle–brachial index.
Baseline comorbidities and medication use.
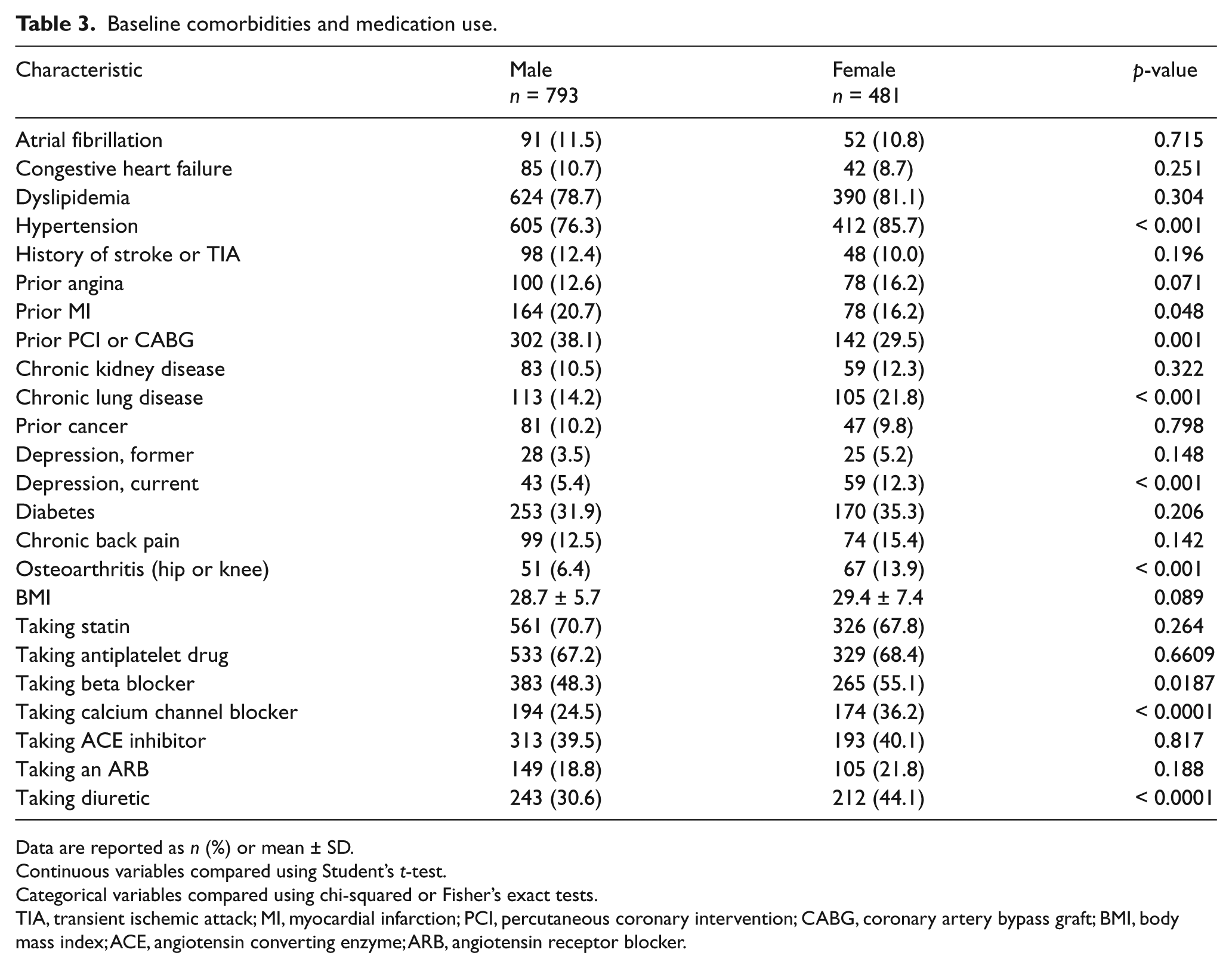
Data are reported as n (%) or mean ± SD.
Continuous variables compared using Student’s t-test.
Categorical variables compared using chi-squared or Fisher’s exact tests.
TIA, transient ischemic attack; MI, myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; BMI, body mass index; ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker.
Compared with men, women were less often Caucasian, married and employed, and more often lacking health insurance, lacking access to care, living alone, had financial concerns, chronic lung disease, and more likely to have depression. Scores for the PAQ domains are presented in Table 4. Women had significantly lower scores, indicating more disability in all domains except treatment satisfaction (Table 4).
Baseline Peripheral Artery Questionnaire (PAQ) scores.

Data are reported as n (%) or mean ± SD.
Continuous variables compared using Student’s t-test.
Categorical variables compared using chi-squared or Fisher’s exact tests.
With regards to symptoms at presentation, women had higher rates of bilateral claudication in comparison with more unilateral claudication in men, and lower PAQ symptoms score (adjusted mean difference −7.2, CI: 9.90–4.50; p<0.001). Although our primary numbers identified more women presenting with atypical symptoms, an adjusted multivariable regression model showed rates of typical versus atypical symptoms at time of presentation were similar in both women and men (men vs women odds ratio (OR) 1.35, p=0.12). Women and men had similar rates with regards to the location of highest claudication at time of presentation including buttock, hip, thigh, calf, foot, or other, which refers to any combination of these locations (Table 2).
When all PAQ scores were examined using adjusted multivariable regression models, female sex was found to be independently associated with lower PAQ scores in all domains including the PAQ Summary score, QOL, Physical Functioning, Social Functioning, and Symptoms score (Figure 1). No sex differences with regards to health status as measured by the generic health questionnaire EQ-5D were observed (66.7 ± 18.8 vs 65.5 ± 20.0, p=0.287).
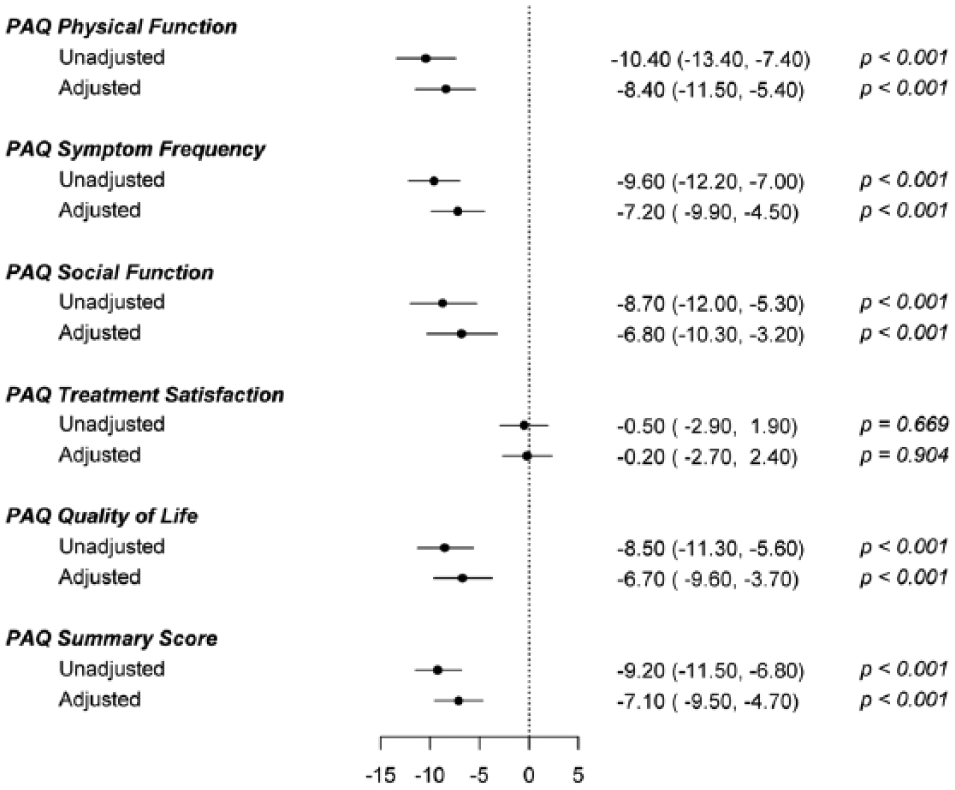
Sex differences in peripheral arterial disease (PAD) health status measures, females versus males. (Model adjusted for age, race, high school education, marital status, living alone, smoking status, insurance, financial status, ankle–brachial index, obesity, current depression, history of heart failure, hypertension, angina, cerebrovascular disease, back pain, osteoarthritis, and myocardial infarction.) PAQ, Peripheral Artery Questionnaire.
Discussion
Women with PAD historically have been described as having fewer symptoms, atypical symptoms and more disability related to comorbidities. 19 Our findings suggest that despite similar ABIs and class of claudication, and independent from clinical background, women with claudication are more symptomatic, have poorer physical functioning and social functioning, and higher depression rates as compared with men. However, no difference was seen with regards to treatment satisfaction, which refers to satisfaction with the PAD evaluation process, and the generic EQ-5D health score. The importance of our study is that it is the first to assess the association between sex and disease-specific health status measures in PAD.
At the time of PAD diagnosis, treatment decisions are based on clinical presentation; therefore, understanding the differences in disease presentation between men and women and the gender-specific impact of disease on patients’ health status is important and could lead to sex-specific diagnostic and treatment algorithms.
Prior studies demonstrated that women with PAD have greater walking impairment, diminished QOL, and poorer physical and mental health as compared to men;20–22 however, these studies were small, limited to a few centers and did not use disease-specific instruments to quantify patients’ health status – an important limitation given the incremental information provided by disease-specific instruments. Furthermore, quantifying the impact of PAD from the patient’s perspective is an essential component of evaluating new pharmacologic and revascularization treatments and to help improve outcomes. 23 Studies that have examined the effect of PAD on health related QOL from the patient’s perspective indicated the need to establish a foundation of systematic PAD-specific assessment in this population.24,25 Because of that, it became essential for researchers to find a disease-specific questionnaire capturing several health domains relevant to PAD to address this problem. The PORTRAIT study used the PAQ as a disease-specific health status measure that provides a standardized assessment of the impact of PAD on population health as seen from the patient’s perspective (symptoms, functioning and QOL). 16
To better understand the impact of disease on patients’ health in general and on women in particular, we examined subjects’ health functioning from physical, socio-economic and psychological stand points. Women with PAD were more physically impaired despite having similar ABIs and class of claudication when compared to men. This may have resulted from the higher incidence of bilateral claudication in women. Rates of chronic back pain were similar in both sexes, but women were more likely to have osteoarthritis, which in part could have led to worsening their mobility. But physical impairment is not the only contributor to poor QOL. Socio-economic status can have equally important ramifications for QOL. Women were less likely to have full-time jobs, more likely to struggle financially to make ends meet, and more likely to live alone when compared to men. Higher depression rates among women in this patient population have historically been documented 26 and may be partly explained by the social and economic struggle these women face. It has been demonstrated that living alone, eating alone and having a low income are associated with high depression rates, especially in females and elderly individuals.27,28 It is conceivable that the higher prevalence of depression in women with PAD may help explain a worse QOL. 5 We believe that the impaired triangle of physical, socio-economic and psychological functioning may help provide explanations as to why we observe a poorer QOL in women with PAD. However, because we only saw a partial attenuation of the association between female sex and worse health status outcomes after adjusting for these factors, future efforts should further identify factors that may help to explain the sex disparities in PAD-specific health status that were documented in patients presenting with new or worsening of PAD symptoms. For now, raising the awareness for the socio-economic challenges that these women face and improving detection and treatment of the mental health burden may be an important avenue to look into to optimize our PAD management strategies.
Limitations
One of the limitations to this study is that results cannot be generalized to patients without symptoms or more severe manifestations of PAD, such as critical limb ischemia. Another important limitation is the potential for unmeasured confounding. While we have included a wide array of socio-economic, clinical and psycho-social variables, we were not able to completely explain the sex differences in PAD-specific health status.
Conclusions
At the time of presentation for vascular specialty care, women with new or worsening claudication have poorer PAD-specific functioning, impacting all major health status domains, than their male counterparts. Importantly, these discrepancies were not explained by differences in clinical PAD severity as outlined by severity of claudication and ABIs. The implications of this observation regarding the management of women with PAD will require further study.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mazen Roumia: nothing to disclose; Herbert Aronow: nothing to disclose; Peter Soukas: research/research grant – Bard, Cordis Endovascular, Mercator, Spectranetics, WL Gore; Kensey Gosch: nothing to disclose; Kim Smolderen: nothing to disclose; John Spertus: consultant fees/honororia – Amgen, copyright for the Seattle Angina Questionnaire (SAQ), Kansas City Cardiomyopathy Questionnaire (KCCQ) and the Peripheral Artery Questionnaire (PAQ), Janssen, Novartis, Regeneron, United Healthcare Scientific Advisory Board; ownership interest, interest/partnership principal – Health Outcomes Sciences; research/research grants – American College of Cardiology Foundation, Lilly; J Dawn Abbott: Data Safety Monitoring Board – Pfizer.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: research reported in this manuscript was partially funded through a Patient-Centered Outcomes Research Institute (PCORI) award (IP2 PI000753-01; CE-1304-6677); The Netherlands Organization for Scientific Research (VENI grant no. 916.11.179); and an unrestricted grant from WL Gore & Associates, Inc. (Flagstaff, AZ, USA).
The statements in this manuscript are solely the responsibility of the authors and do not necessarily represent the views of the PCORI, its Board of Governors or Methodology Committee.
All manuscripts for the PORTRAIT study are prepared by independent authors who are not governed by the funding sponsors and are reviewed by an academic publications committee before submission.
The funding organizations and sponsors of the study had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.