
Abstract
Fibromuscular dysplasia (FMD) is a vascular disorder about which little has been known until recently. Patients with FMD may suffer from hypertension, aneurysms, or strokes, as well as symptoms associated with local artery damage. As a result of advances in vascular medicine and growing outcomes registries, we now have a better understanding of the FMD disease process and epidemiology. Nevertheless, the consequences of FMD on patients’ day-to-day experiences and mental health status are not well understood. The purpose of this study was to begin to identify and characterize the experiences of living with FMD from the perspective of the patient using qualitative inquiry. Interviews with 19 FMD patients (18 female, 1 male) were conducted, audio-recorded, transcribed verbatim, and content analyzed. Individuals with FMD reported a complex array of psychological, physical, emotional, social, and health care concerns, which may be underdiagnosed. Findings suggest new opportunities for enhancing patient care.
Introduction
Fibromuscular dysplasia (FMD) is a non-inflammatory, non-atherosclerotic disease of the arteries. 1 Patients with FMD may suffer from hypertension, aneurysms, and strokes, as well as symptoms associated with local artery damage such as angina, or abdominal pain. 1 Although the epidemiology of FMD is largely unknown, 2 most patients (91%) diagnosed are women. 3
Prior to the organization of the United States Registry for Fibromuscular Dysplasia (US Registry for FMD) in 2009, research on FMD was limited. However, the US Registry for FMD now has more than 1400 patients enrolled across the country 4 and has inspired further registry-based research efforts around the world. Indeed, though little is known about the cause or prevalence of FMD,1,5 a great deal has been learned about the vascular sites most commonly affected, variations in disease presentation, and patient outcomes.
While it is difficult to overestimate the contributions of advancements in biomedical knowledge in treating FMD, other factors also contribute to FMD health outcomes but have received less attention. Specifically, little is known about the experience of living with FMD from the patient’s perspective. The goals of this study are to generate knowledge about the experiences of being diagnosed and living with FMD, to understand the self-reported influences of FMD on personal and social relationships and mental health, and how FMD changes the lives of those it affects.
Methods
Design
Qualitative methods are well-suited to illuminate a phenomenon about which little is known 6 and to gain insight and understanding about particular human experiences.7,8 Therefore, we used a qualitative descriptive approach to examine the experiences of people diagnosed and living with FMD.8,9
Sampling
Purposeful sampling, a form of non-probability sampling, was used to select study participants.10–14 This approach is appropriate for qualitative studies such as this one that concentrate in depth on a relatively small number of information-rich cases (i.e. those that can contribute substantially to the research question) for the purpose of offering insight and illumination about the phenomenon under study. 15 In other words, we were seeking participants who would be able to convey insight and provide rich descriptions about what it is like to be diagnosed and living with FMD. Further, we used a particular purposeful sampling strategy called snowball or chain sampling. This strategy involves asking well-placed people who we should talk to or who is knowledgeable about the topic under investigation.16–18 Vascular experts referred the authors to the Fibromuscular Dysplasia Society of America (FMDSA). In turn, the FMDSA Executive Director indicated that people who attend FMDSA annual meetings and have FMD are highly articulate and motivated to talk about their experiences. This made them an ideal group from which to sample. Consistent with standard qualitative methods, sample size was not determined a priori. Rather, participant enrollment and data collection continued until data saturation was achieved.10–14
Participant recruitment
Participants were recruited from among the patient registrants for the FMDSA Annual Meeting in Cleveland, OH in May 2014. The FMDSA is a non-profit organization dedicated to advancing FMD awareness, education and research. 4 The meeting draws leaders in FMD research from around the globe, as well as FMD patients. This study was reviewed by Institutional Review Boards at the University of Michigan and Eastern Michigan University; both boards deemed it exempt from ongoing review (HUM00084835, 140501P). Although consent documents were not required, the written informed consent of each study participant was obtained prior to their interview.
With permission from the FMDSA, registrants of the FMDSA meeting were electronically sent an invitation to participate through the conference registration system. The invitation outlined the purpose of the study and the inclusion/exclusion criteria: a diagnosis of FMD, at least 18 years of age, English speaking, ability to hear, ability to provide consent, and willingness to participate in a face-to-face interview. Interested subjects contacted the study team, who confirmed eligibility, informed participants that their interviews would be recorded, and scheduled face-to-face interviews during the meeting.
Procedures
Interviews were conducted before, during, and after the 3-day meeting in separate, private rooms, by two trained field researchers from different disciplines (public health and nursing). Prior to each interview, the researchers reviewed with participants the aim of the study, the need to audio record the interview, measures taken to preserve anonymity, and then obtained written consent.
A semi-structured interview guide (available as Supplementary material) was used to help participants tell their health and illness stories 19 of being diagnosed and living with FMD. 20 Semi-structured interview guides also serve to assist the interviewer with tracking topics and questions during the interview. They are not intended to function as questionnaires that pose precisely the same set of questions to each participant, and thus are not subject to validation in terms of reproducibility. Indeed, the term interview ‘guide’ 21 reflects the understanding that questions and topics of discussion will vary across interviews, and that the interviewer has discretion to pursue avenues of discussion that are unanticipated but may be useful to inform the larger research question. 22 Consistent with standard rigorous qualitative methods, our interview guide was informed by current literature, reviewed by an expert living with FMD and by vascular experts, and was revised based on their input.21,22
All interviews began with the icebreaker: ‘Tell me how you learned you had FMD’. Participants were encouraged to tell their illness story using prompts to facilitate the narrative.12,20,23 During the interviews, we took detailed field notes. At the conclusion of each interview, patients were offered an opportunity to provide any additional information and asked to provide limited demographic data (age, gender, marital status, living situation, and race). Interviews lasted an average of 45–90 minutes.
Data analysis
Transcript data were analyzed with conventional content analysis to identify themes, patterns and meanings.6,24 Of the three types of content analysis identified by Hsieh and Shannon, 6 conventional content analysis is most appropriate for use with exploratory study designs and when there is limited literature on the phenomenon under inquiry. Thus, it was the best choice for our method of analysis.
Preliminary data analysis was done concurrently with data collection. Data saturation – when no new concepts and categories appeared – occurred by the 13th interview. It is our practice to continue with several additional interviews after that point, to ensure data saturation was achieved. In this study, we interviewed all remaining volunteers because we had the time and interest to do so, and because the volunteer participants were eager to be interviewed.
All interviews were transcribed verbatim and the transcripts edited for accuracy. Transcripts were read repeatedly6,24 and independently by the authors to develop and note impressions of their content. Next, text was highlighted, line by line, that spoke to the experience of being diagnosed or living with FMD, as well as text that was reported with regularity or was surprising or compelling.6,25 These segments of data were assigned labels, and through an iterative process of collective discussion, they were eventually sorted into categories. Each category was given a name and themes were identified within and across interviews.
This study included several methods of rigor commonly used in qualitative inquiry. First, purposeful sampling was used to identify and select information-rich cases that would best illuminate the experiences of FMD patients.7,11 Second, interviews were conducted by two trained field researchers from different professional backgrounds, and transcripts were independently analyzed and discussed (triangulation). 26 During this process, research team members sought to bracket our own clinical, research, and personal experiences, and to remain aware of the influence these may have on data collection and analysis (reflexivity). 27 Finally, study results were presented the following year during the FMDSA Annual Meeting in 2015, which many study participants attended. Presentation and follow-up discussion during the meeting provided opportunities for member-checking. 28 Specifically, a number of study participants and many non-participants with FMD told us that our findings accurately captured their experiences. Such confirmation (i.e. member-checking) is a strong indicator of rigorous qualitative work.
Results
Sample characteristics
Of 126 FMDSA conference attendees in 2014, 57 self-reported as having FMD. In total, 22 eligible individuals responded to the electronic study invitation and all agreed to participate. However, owing to a high number of last-minute registrants (P Mace, personal communication, 28 April 2016), the actual proportion of subjects who responded to the invitation cannot be determined. Three interviews were excluded from the final analysis at the participants’ requests: two for personal reasons and the third out of personal concern that the experience of FMD could not be separated from a comorbid condition diagnosed at approximately the same time. Results presented here were derived from the remaining 19 participants.
Participant characteristics are summarized in Table 1. Although almost all patients were Caucasian, married, and female, ages and FMD experiences differed between patients. Both newly diagnosed FMD patients and those who had lived with FMD for up to 28 years were represented in this sample, with a median time since diagnosis of 6.0 years. Symptoms differed among participants: some reported a wide range and number, while others reported none. The majority described more than one arterial bed being affected, with more than half having both renal and carotid disease. Nearly half of the patient population experienced a vascular event, such as aneurysm, dissection, stroke, or transient ischemic attack. Other comorbid conditions were inconsistently reported. Specific data pertaining to events, management, and medications were beyond the scope of this study.
Self-reported demographics of interviewed FMD patients, n=19.
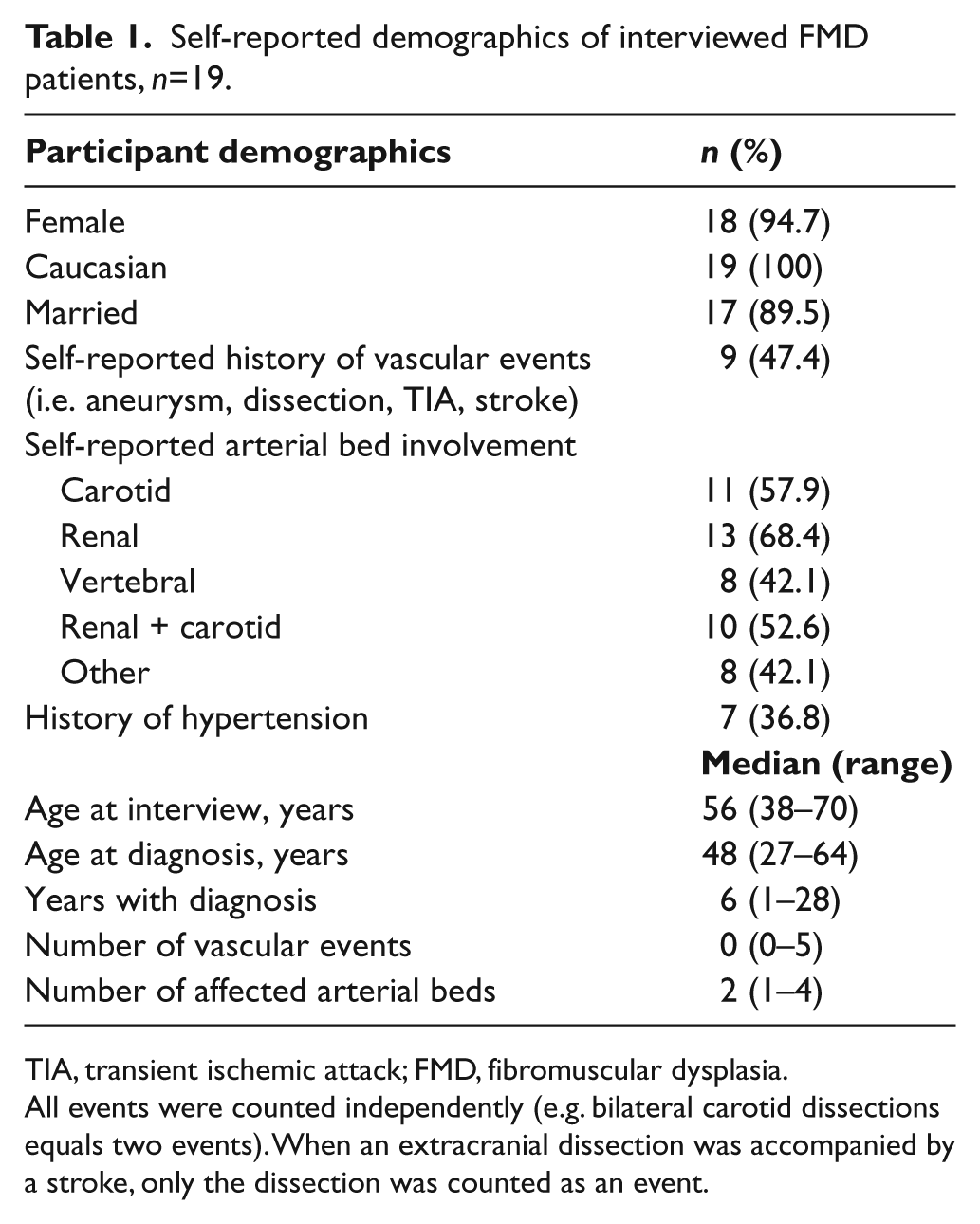
TIA, transient ischemic attack; FMD, fibromuscular dysplasia.
All events were counted independently (e.g. bilateral carotid dissections equals two events). When an extracranial dissection was accompanied by a stroke, only the dissection was counted as an event.
Results of content analysis
Conventional content analysis, as identified by Hsieh and Shannon, 6 revealed a complex array of physical (fatigue, pain, pulsatile tinnitus), psychological (anxiety, depression), and social (intimacy, disability) challenges that impact participants’ quality of life. Five themes captured these experiences: symptom burden, worries and concerns, experience of health care, loss and change, and resilience (Figure 1). Results for each theme are presented below, along with illustrative excerpts quoted from the data (Table 2). Details with the potential to identify participants were altered to protect their anonymity, without substantively changing the content.
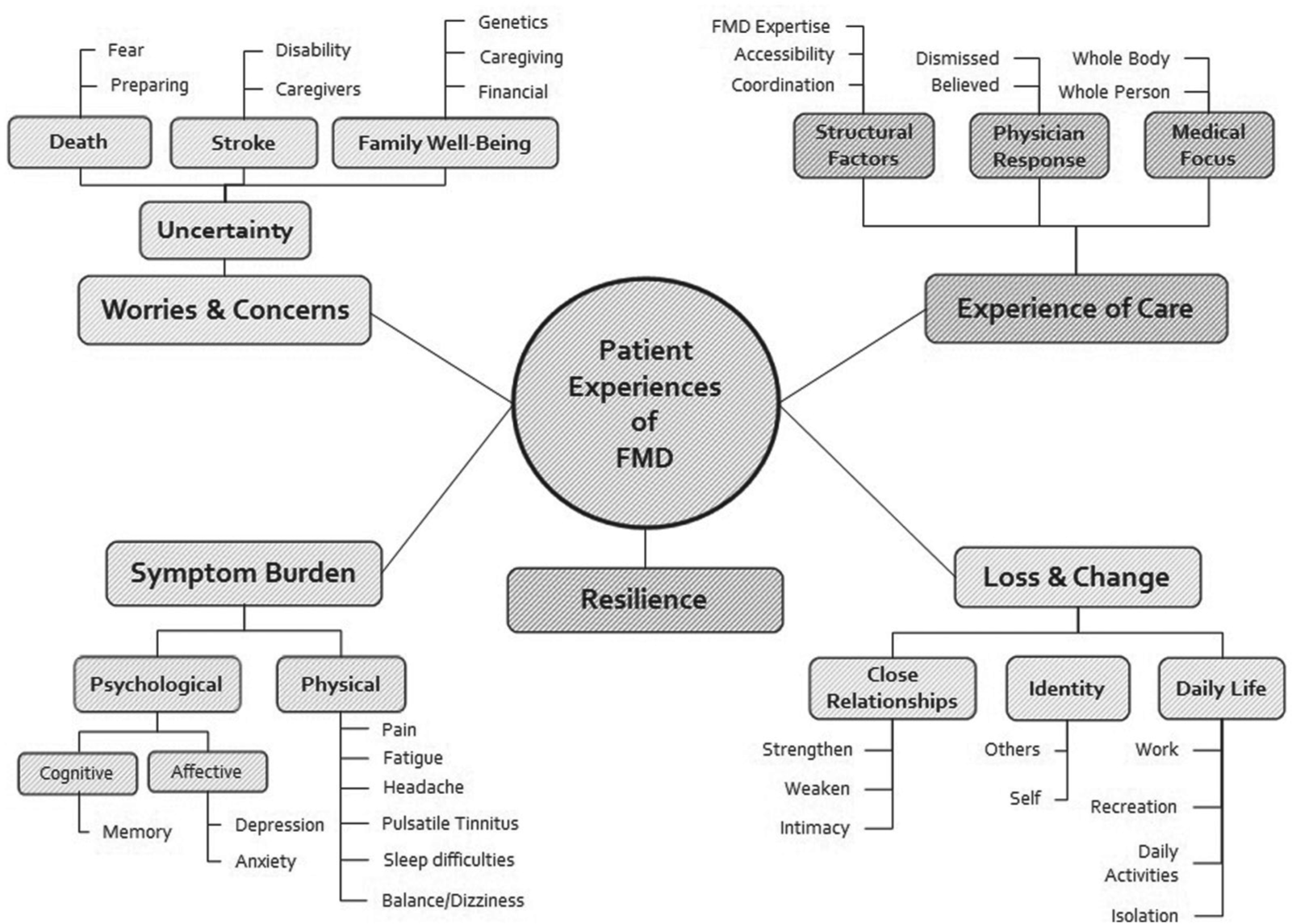
Experiences of FMD differed among patients, yet five common themes emerged that captured them: Worries and concerns, Experience with healthcare, Symptom burden, Loss and change, and Resilience.
Patient experiences of FMD: Selected excerpts from the interview transcripts.
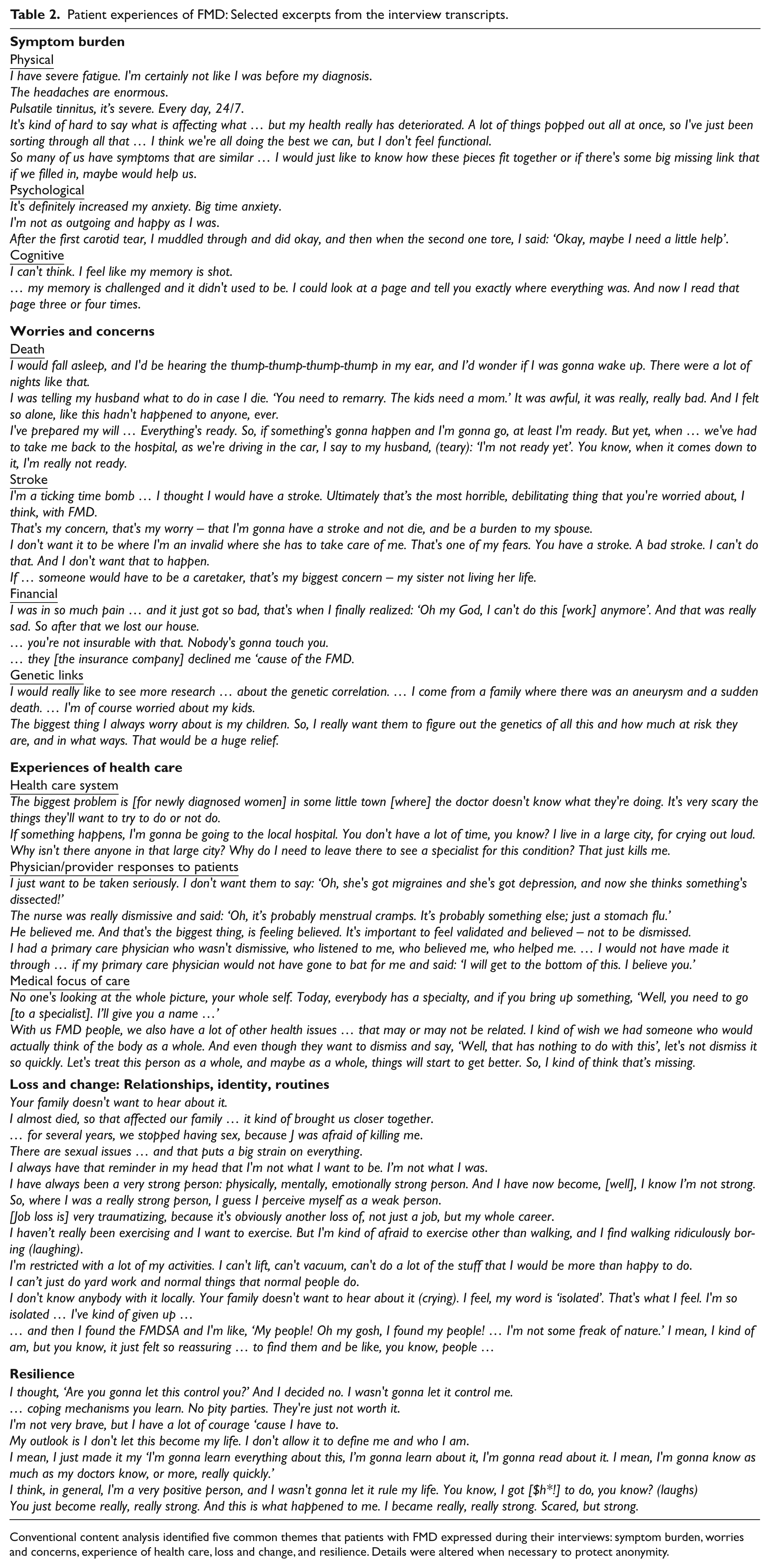
Conventional content analysis identified five common themes that patients with FMD expressed during their interviews: symptom burden, worries and concerns, experience of health care, loss and change, and resilience. Details were altered when necessary to protect anonymity.
Symptom burden
Participants reported a range of both physical and psychological symptoms. For some, symptoms are barely noticeable, but most reported multiple symptoms that are frequent, disruptive, and result in poorer health and limited ability to function. Participants often reported the experience of multiple symptoms as something they want to sort out, both in terms of etiology and treatment. Many hypothesized that their numerous and varied symptoms are inter-connected and related to a bigger picture of FMD that we have yet to understand.
With respect to psychological symptoms and cognitive function, most participants said that FMD has a negative impact on their mood or affect. Many specifically reported anxiety. Although anxiety was the predominant psychological symptom after an FMD diagnosis or event, some patients also reported depression. Reports of treatment for anxiety and depression varied – some were taking prescribed medication, but most were not. Cognitive difficulties were also reported, such as memory and concentration issues, though few participants reported evaluation for psychological or cognitive symptoms.
Worries and concerns
Participants shared that their biggest worries and concerns about living with FMD relate to the uncertainty it ushers into their lives. Uncertainties associated with death, stroke, and family well-being topped their lists. Participants reported fear of death, and some took active steps to prepare for it such as instructing family about their wishes and preparing wills. Despite these preparations, some reported they were not really ready for death.
Another top worry participants featured was stroke. One woman characterized herself as a ‘ticking time bomb’ in relation to it. Stroke was a concern not only because of the disability it may cause, but also because it might require loved ones to become caregivers.
Participants also reported concerns related to the potential impact of FMD on their families and loved ones. In particular, they shared concerns about financial matters, and genetic risks of passing FMD on to their children. Many of the participants were already experiencing financial impacts from FMD in that they were no longer able to work. Some had filed for disability benefits, and one family had even lost their home. Some participants attempted to secure financial protection through insurance, but were refused. Participants feared that FMD-related financial burdens might require their loved ones to take on caregiver roles and did not want that to happen. Participants also voiced concern about passing FMD on to their children and wanted to understand what their FMD means for their children and grandchildren. They expressed hope for future research that examines potential genetic links and said that such knowledge would bring relief.
Experiences of health care
Participants spent a lot of time sharing their experiences of health care. Descriptions clustered around structural factors in the health care system, physician response to their presentation of symptoms and questions, and a strictly medical focus to health care. Participants frequently identified structural factors, or factors that are inherent in the health care system, as influences on their health care experiences. Specifically, they note that many physicians they encounter lack expertise in FMD. Moreover, they report that the small number of physicians with expertise are often located long distances from their homes. For many, these factors create concern about their ability to access quality care.
Participants identified physicians’ responses to their concerns and symptoms as highly salient to their experience of care. Many reported that they frequently experience physicians and other providers as dismissive when they present their symptoms and concerns, and feel they are not believed. In contrast, being believed by the physician was reported less frequently, but was highly valued when it occurred. Being believed was valued not only because it is validating, but also because providers who believed patients were described as essential for patients to ‘make it’.
Participants also experienced FMD health care as medically focused, even though they reported that it affects so much more than a patient’s physical body. Many participants revealed a wish for care of the body as a whole, and of the body in the context of a whole self.
Loss and change
All participants in this study reported that FMD had changed their lives in terms of close relationships, their identity, or their daily life routines. Many indicated the changes were accompanied by loss. For some, FMD strained close relationships, while other families grew closer. FMD interfered with physical intimacy for many, often because both partners fear negative health consequences, creating a strain on relationships between partners.
An unexpected finding was the change in identity that was reported by so many. A number of participants noted that since their diagnosis others see them differently and they see themselves differently. Many spoke to being a different person now. For one grandmother, the things she could no longer do with her grandchildren were a reminder of how she has changed; others felt weak now, when they once felt strong.
All participants reported changes in their routine activities. There were varying degrees of limitation in work, recreation, and activities of daily living. Some participants became unable to work, stopped exercising or doing routine daily activities, and described the experience as isolating.
In contrast to feelings of isolation and not feeling like a normal person, many participants reported a sense of belonging and normalcy by connecting with others who have FMD through social media, conferences, and support forums.
Resilience
In the midst of the many serious challenges people with FMD reported, a spirit of resilience was also evident. After some time has passed post-diagnosis, participants discussed getting on with their lives and not letting FMD define them. Others suggested that they learned to cope, and found self-pity is not useful. Finally, after living with the diagnosis for some time, some reported that feeling scared co-exists with feeling strong.
Discussion
The goal of this study is to add to the growing body of knowledge about the experiences of being diagnosed and living with FMD. To the best of our knowledge, this study is the first to identify and characterize the experiences of people living with FMD, from their perspectives, using a qualitative approach. Findings reveal a complex array of experiences related to symptom burden, worries and concerns, health care services, loss and change, and resilience. These themes represent new knowledge about the psychosocial dimensions of FMD and suggest opportunities for enhancing patient care.
Results from our study are consistent with work on patients’ experiences of rare disease. Though, strictly speaking, FMD is no longer a ‘rare’ disease,1,29,30 patients with FMD experience similar psychological symptoms, worries, experiences with health care, and life losses and changes as do those with rare diseases that are chronic, degenerative, and may result in disability. 31 Additionally, they experience fear and uncertainty related to potential spontaneous events. Though some are able to cope without intervention, others may benefit from enhanced screening efforts and treatment plans that evaluate and follow through on mental health and psychosocial issues, as well as physical and vascular health. For example, individuals with FMD may benefit from social work assistance for anxiety and depression or medically related financial issues, as well as assistance with legal issues such as durable power of attorney and living wills. Our results also underscore the complexity of FMD, as evidenced by the wide range and number of FMD-related experiences participants reported. Thus, another opportunity to improve patient care may include new dedicated roles for care coordination and advocacy by a FMD-knowledgeable provider to monitor and coordinate care within and between institutions.
Participants in this study frequently reported feelings of being dismissed and not being believed by physicians and other providers, suggesting opportunities to help sensitize providers to the importance of empathy in response to their patients’ experiences. It is plausible that increased physician empathy would strengthen therapeutic alliance, which has been associated with improved health care outcomes in cardiovascular disease, diabetes, cancer, and the common cold.32–37 Empathetic providers have also been found to promote treatment compliance and enhance patient satisfaction. 38 In some cases, patient–provider relationships characterized by physician empathy have been associated with a greater sense of health among patients. 34 Our findings suggest that FMD patients need their providers to be empathic listeners. For many of our participants this study interview was the first time they had told their full story to an interested listener, and they described it as cathartic. 19
Our participants reported significant delays in diagnosing their FMD, consistent with the literature on FMD and rare diseases.1,31 Thus, interventions aimed at decreasing time to diagnosis are necessary first steps to improve patient care. Our findings suggest two urgent needs. First, primary care providers need FMD-specific education to enable earlier symptom recognition, screening, referrals, and management. Second, improved geographic distribution of FMD specialists is necessary to provide access to the expertise required for optimal care.
Limitations
Consistent with the purpose of this study, our results provide insight into the experiences of people living with FMD from their own perspectives. Our sample size of 19 interviews was small relative to the standards of quantitative methods; however, the sample size was adequate to achieve thematic saturation – the point when interviews are no longer generating new themes or information.39–41 Evidence indicates that 90% of new themes and ideas can be detected with 16 interviews; 42 this study included 19 interviews.
While our findings provide insight and generate hypotheses, they cannot be generalized beyond the study population. Larger-scale studies and those with controls are necessary to meet that purpose and are important for further analyses of the differences in experiences between newly diagnosed FMD patients and those with long-standing diagnosis, and between patients with an uncomplicated course and those with vascular events and complications. Such data generated from larger-scale studies would further increase knowledge and ability to provide a patient-centered approach to care.
Our findings provide a window into the experiences of FMD patients, which may not be that different from those described by this study sample. Our sample was not random, and it is possible that selection bias occurred, as patients who agreed to participate may systematically differ from those who did not volunteer. For example, the participants in this study were well enough to attend the FMDSA Annual Meeting and complete an interview, and had the means to do so. Thus, differences in income may have biased results, as well as differences in education and actual or perceived severity of the condition. We also relied on participants’ detailed reports to confirm a diagnosis of FMD. While questions were deliberately included in the interview guide to determine diagnosis, participant self-reports were not adjudicated. As a result, the demographic and epidemiologic differences noted between this study and published findings from the US Registry for FMD 4 are likely attributable to the sampling process. 43
Irrespective of the presence or absence of FMD, history of a neurological event, hypertension, and/or exposure to antihypertensive or psychoactive drugs may affect a patient’s quality of life and mental health. Therefore, future work to determine the unique impacts of FMD should include controls with these and other relevant conditions.
Conclusions
Our findings offer a nuanced understanding of the complexity of being diagnosed and living with FMD, from the perspectives of FMD patients, 20 which may prompt discussion about opportunities to improve patient care. FMD patients in this study desire care for a broad range of needs (medical and psychosocial) that impact their health and well-being. In particular, FMD patients want to be heard and believed by their physicians and other providers, they seek increased FMD education for primary care providers and better geographic distribution of FMD experts, and they desire care for the whole self. Future research is necessary to confirm these findings on a larger scale, and to test interventions for improved patient care.
Footnotes
Acknowledgements
The authors thank the FMDSA for allowing them to conduct research at their annual meeting, and the Michigan Clinical Outcomes Research and Reporting Program (MCORRP) for their assistance with the development and implementation of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sherry M Bumpus received a minor grant from the Josephine Nevins Keal Fund to support travel to present this research. Minnie Bluhm received a minor grant from Eastern Michigan University to provide release time and support for this research and also a minor grant from the Josephine Nevins Keal Fund to support travel to present this research.