
Abstract
Stroke is a leading cause of death among women in the United States, and women are more affected by stroke than men. With women living longer than men, women experience not only a higher incidence of stroke but also more negative outcomes. Despite its lethal impact and high morbidity rate, the road from innovative bench research to improved clinical outcomes has been slow. This review explores the differential physiology, epidemiology, and clinical presentation of stroke between men and women, as well as the current status of laboratory and clinical data.
Keywords
The University of Virginia School of Medicine designates this journal-based CME activity for a maximum of 1 AMA PRA Category 1 CreditTM per article. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Learners are expected to read this article along with any references and supporting material as appropriate, and complete the online post-test questions with an 80% pass rate to receive credit. Post-test questions are accessed through the member portal on the Society for Vascular Medicine (SVM) website (www.vascularmed.org). Please note that CME credits are only available to members of the SVM. This activity expires two years after the publication date, on April 1, 2019.
Heather Gornik has disclosed research support from AstraZeneca, intellectual property rights from Summit Doppler Systems, Inc, and intellectual property rights and stock/ownership from FlexLife Health (proceeds donated). Aditya Sharma has disclosed research support from National Institute of Health Sciences, AstraZeneca, Biomet Biologics, Portola Pharmaceuticals, and Pedra Technology. Valerie Clark has no financial affiliations to disclose.
Introduction
Worldwide, stroke is the third leading cause of death, as well as the leader in long-term disability etiology as of 2012. 1 In the United States specifically, according to the Centers for Disease Control and Prevention, stroke is the fourth leading cause of death, and accounts for 33% of potentially preventable deaths for individuals under 80 years of age between 2008 and 2010. 2 Notably, 60% of all stroke deaths involve women. 3 Population education programs in the last few years, such as the F.A.S.T program and Stroke Awareness Month, have increased the public’s knowledge and awareness of the incidence and impact of stroke in women. Additionally, current research indicates differences in how women and men present with stroke, but also how they are treated in an acute setting and how they respond to treatment methods. These disparities are of vital importance, given that targeted sex-specific therapies can help improve clinical outcomes and reduce the burden of disease in the population. Therefore, this review examines the variations between men and women in risk factors, epidemiology, presentation, treatment, and outcomes of stroke.
Classification and pathophysiology
Strokes are primarily classified as ischemic or hemorrhagic. Ischemic strokes are the most common (87% of all strokes) and occur due to obstruction of a blood vessel supplying the brain. They may be further sub-classified as thrombotic or embolic, depending on the site of occlusion. 4 Further complicating the classification process is that of cryptogenic stroke, a transient neurological event of obscure or unknown origin, which can account for up to 30% of all strokes, occurs most often in younger patients. 5 Given that cryptogenic stroke is a transitory event, the etiology is difficult to ascertain, resulting in difficulty selecting definitive treatment. 6 On the positive side, this category of cerebral infarctions has most often been isolated events with a low recurrence rate and good functional outcomes. 5 Table 1 highlights these and other stroke subtypes in a number of stroke classification systems. The algorithms vary from study to study, but they are all primarily based on clinical presentation, neurological signs, brain imaging findings, and ancillary testing results. Owing to the differences in methodology, these systems vary in algorithm complexity, equipment required to use them, and the percentage of strokes that fall into the cryptogenic category.
Varying stroke classification systems by western countries.

TOAST, Trials of Org 10172 in Acute ischemic Stroke Treatment; SSS-TOAST, Stop-Stroke Study TOAST; CCS, Causative Classification System; ASCOD, Atherosclerosis, Small vessel disease, Cardiac source, Other cause, Dissection; LAA, large artery atherosclerosis; CE, cardioembolism; SVO, small-vessel occlusion; OD, other determined; UD, undetermined.
Republished from Kim BJ, Kim JS, Ischemic stroke subtype classification: An Asian viewpoint. J Stroke 2014; 16: 8–17; Copyright © 2014 Korean Stroke Society; Reproduced with permission.
Physiologically, ischemic stroke is preceded by endothelial damage in cerebral blood vessels that causes inflammation and fatty deposit accumulation in arterial walls. The subsequent decrease in blood vessel diameter and vascular flow causes hypoxic and hypoglycemic conditions in the brain tissue, resulting in an ischemic core (blood flow < 10 mL/100 mg/min) and an ischemic penumbra (blood flow > 10, but less than 20 mL/100 mg/min).7,8 Neurons have significant functional loss in hypoxia-ischemia, as evidenced by the decreased adenosine triphosphate (ATP) production in the ischemic core neurons, thereby activating the ischemic cascade. The membrane ionic gradient is lost, leading to intracellular sodium and calcium increases; subsequent glutamate release further increases calcium influx via NMDA and AMPA receptors. 9 The resulting excitotoxicity leads to organelle and membrane swelling, loss of integrity, and ultimately necrosis. 8 In the ischemic penumbra, however, decrease in blood flow alone is not capable of inducing neuronal necrosis, but is sufficient to create an environment vulnerable to further insult. Ultimately, the adjacent ischemic core glutamate production leads to intracellular calcium accrual in the penumbra. This activates cellular enzymes such as calcium-dependent calpains and caspases, endonucleases, proteases and ATPases, causing increases in nitric oxide, arachidonic acid, and superoxide radicals that help cells die.8–12
In contrast, hemorrhagic strokes (13% of all strokes) are intracerebral or subarachnoid in nature and occur due to ruptured vessels. 13 Although less common than ischemic strokes, hemorrhagic strokes are more fatal to patients due to potential hydrocephalus, increased intracranial pressure, and blood vessel spasms.14,15 With regards to incidence, men are more likely to have ischemic strokes, 16 while women are at greater risk for subarachnoid hemorrhage. 17 These strokes are typically associated with chronic hypertension and/or vascular malformations, both of which may lead to vessel wall weakening or aneurysmal degeneration with rupture.
Blood build-up in the subarachnoid space or brain tissue can lead to infarction as well as brain tissue and vascular toxicity. 18
Before concluding this section, we will briefly touch on other causes of stroke, as they pertain to the scope of this review. Other arterial causes of acute ischemic stroke which are more common in women include fibromuscular dysplasia (FMD) and carotid dissection.19,20 These two entities may be found separately or be associated. Fibromuscular dysplasia is a non-atherosclerotic, non-inflammatory disease process of the blood vessels that can result in arterial stenosis, occlusion, aneurysm, or dissection.21,22 The etiology of FMD and its prevalence in the general population are not well understood, as the symptoms are non-specific and the disease is poorly understood. Studies have shown that women are affected more than men, in a 9:1 ratio. 23 Treatment for FMD may include medical therapy, surveillance, endovascular intervention, and surgery. Additionally, carotid dissection may occur in the setting of FMD, but also during pregnancy and the puerperium. 24 Internal carotid artery dissection, which may occur intracranially or extracranially, can also be spontaneous or associated with major or minor trauma. Any spontaneous dissection may have an association with a genetic, familial, or heritable disorder. A full discussion of these lesser occurring vascular diseases is beyond the scope of this review.
Finally, a relatively rare vascular disorder that is more prevalent in women is cerebral venous and sinus thrombosis.25,26 This subtype of stroke is more common in younger to middle-aged women (3:1 ratio women to men). The main sex-specific risk factor attributed to this differential incidence is oral contraceptive use. Women tend to develop an underlying thrombophilia, warranting routine testing. Generally, though, outcomes are excellent, a stark contrast from those seen in arterial strokes. 26
Epidemiology
Current population data indicates that 16.9 million individuals suffer from stroke yearly, equating to a global incidence of 258 per 100,000 per year. 27 Historically, from 1970 to 2008, population data indicates that in high-income countries, stroke events have decreased by 42%; in contrast, in low and middle-income nations, stroke incidence has increased over 100%. 28 However, even in nations with stroke incidence decline, the lifetime risk reduction is not proportional, and tends to be greater for men (19.5% to 14.5%) than women (18.0% to 16.1%). 29 Furthermore, as women age, they demonstrate greater risk than age-matched men due to mid-life stroke surges. 30 This is reflected in male-female incidence rate ratios decreasing from 1.49 (ages 35–44) to 1.21 (ages 75–84). 31
Women have higher lifetime stroke risk and have been found to have recurrent strokes more frequently than men. 3 This is partially explained by women’s greater life expectancy and that age is a non-adjustable risk factor; therefore, more women are living to ages where stroke risk is higher. Furthermore, women also have higher mortality rates from stroke than men. 32 A potential explanation for this trend is that the mean age of first stroke for men is 68.6 years, while it is 72.9 years for women. 31 According to the Centers for Disease Control and Prevention, men and women under the age of 45 have similar stroke mortality rates. 33 From this age on, women’s stroke mortality rate increases significantly, and although their rate is lower than age-matched men, the difference decreases with age. 34 A plausible explanation for this occurrence is the neuroprotective loss of estrogen post-menopausal women experience.35,36
These findings are qualitatively reflected in Table 2 and Figure 1. In Table 2, note that females over 20 years old have greater prevalence of stroke when compared to males (600,000 more cases annually but only 2.7% compared to 2.6% for men). However, it is instructive to note that females at all ages have far higher rates of new and recurrent attacks at all ages (53.5% vs 46.5% for men), higher mortality (58.4% vs 41.6% for men), and a greater number of discharges (530,000 to 485,000), indicating the effect it has on women. Furthermore, African Americans almost double the rates of prevalence in Caucasians; in both black and white individuals, women have greater rates of stroke. Finally, in Figure 1, we can see that regardless of race, younger women have fewer strokes than age-matched males. However, once women pass menopause, their rates of stroke are far greater than male rates, thus explaining the overall prevalence rates seen in Table 2.
Stroke incidence in various populations (2012 data).

NH, non-Hispanic.
These percentages represent the portion of total stroke incidence that applies to males vs females.
Estimates include Hispanics and non-Hispanics. Estimates for white individuals include other non-black races.
Republished with permission of Wolters Kluwer Health, Inc., from ref. 3; Copyright © 2015, American Heart Association, Inc.; Reproduced with permission.
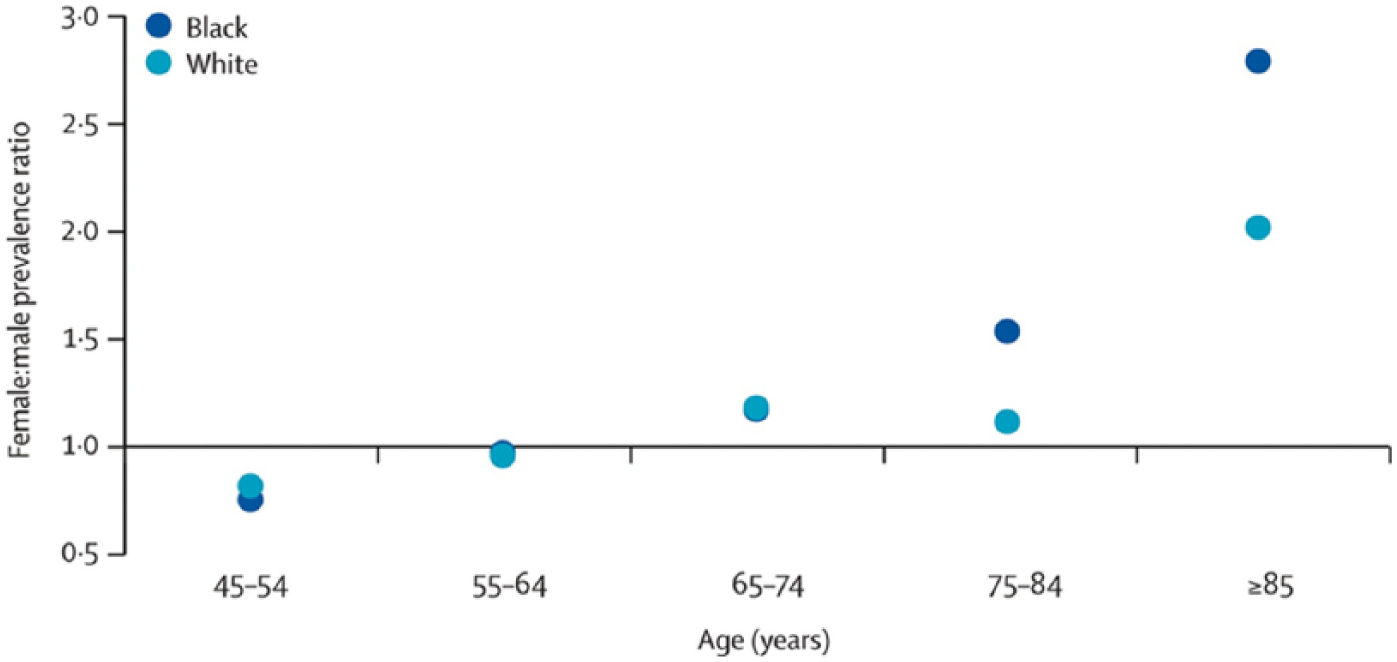
Stroke prevalence by sex. Republished from ref. 34; Copyright © 2008 Elsevier Ltd; Reproduced with permission.
Risk factors
Risk factor differences between men and women in part account for epidemiological findings in stroke incidence, prevalence, and mortality. A number of sex-non-specific modifiable risk factors exist, including atrial fibrillation and other cardiac conditions, hypertension, cigarette smoke exposure, alcohol consumption, physical inactivity, metabolic syndrome, and Type 2 diabetes mellitus.37,38 Non-modifiable risk factors exist as well, such as age (stroke rate doubles every 10 years after age 55), sex, family history, and being of African American descent.34,39,40 Figure 2 demonstrates the increase in the 10-year stroke rate for adult men and women as the number of comorbid conditions increases. Interestingly, women have lower 10-year rates of stroke without comorbidities, but a greater rate with four or more, implying that their stroke risk is more affected than in men.

Stroke risk by number of comorbidities. (AF, atrial fibrillation; CVD, cardiovascular disease.) Republished with permission of Wolters Kluwer Health, Inc., from ref. 3; Copyright © 2015, American Heart Association, Inc.; Reproduced with permission.
Many of the aforementioned modifiable risk factors are more common in males, but when considering only stroke patients, they are shown to increase stroke risk more in females (as noted in discussion of Figure 2). For example, while hypertension and atrial fibrillation are more common in men than pre-menopausal women, 41 females with these conditions have a greater stroke risk.42,43 Similarly, Type 2 diabetes mellitus more often presents in men with stroke; 44 again, the condition has a greater effect on increasing stroke risk in women. 45 With respect to metabolic syndrome, its presence doubled ischemic stroke risk in women, but had no statistically significant effect on men. 46
Sex-specific risk factors must be considered as well. For men, the most significant are alcohol and tobacco use, myocardial infarction history, and peripheral arterial disease. 42 Furthermore, reduced total testosterone levels in circulation have been associated with increased stroke incidence for men even after adjusting for common risk factors in cardiovascular disease. 47 Although the pathophysiological connection between testosterone and stroke occurrence is unclear, low testosterone levels have been linked to metabolic syndrome, Type 2 diabetes mellitus, and aortic arterial disease, which are all independent stroke risk factors. 48 With respect to women, the use of oral contraceptives is linked to increased risk of ischemic stroke, potentially due to the hypercoagulable states that are induced. 49 Similarly, pregnancy-related effects on hemodynamics (increases in pro-coagulant activity in maternal blood, decreases in anti-coagulant factors, and impaired fibrinolytic activity) predispose women to stroke. 50 Furthermore, menopause has been linked to metabolic syndrome onset 51 and increased blood pressure, 41 which have been theorized to be caused by drops in estrogen levels.
While most studies have focused on risk factors for stroke, the GIFA study assessed a cohort of older adults to ascertain prognostic variables for cognitive impairment, disability at discharge, and in-hospital mortality rates following acute cerebrovascular events: 52% were women in this robust dataset, but more than 50% of the patients enrolled with acute stroke were also female. Therefore their analysis noted that there was no difference associated with female sex and functional status or mortality after an acute stroke event. 52
Sex-steroid hormones
The menopause-related loss of estrogen’s neuroprotective effects sheds some light as to why there is a mid-life surge in stroke incidence in post-menopausal women. High levels of 17-β estradiol (E2) have been found to attenuate stroke effects in pre-menopausal women. 53 Estrogen binds vascular smooth muscle and endothelial receptors, 54 thus facilitating vasodilation through a number of pathways.53,55 Nitric oxide specifically regulates myogenic tone in cerebral vessel autoregulation to shield against blood flow fluctuations that can cause vessel damage and rupture. 55 Overall, blood supply in pre-menopausal women is better than in men during and after ischemic stroke, leading to lower infarct volumes.
Several studies have also demonstrated that 17-β estradiol directly influences neuronal cell survival in stroke. Specifically, it has been demonstrated that physiological levels of E2 inhibited injury-induced downregulation of bcl-2, resulting in increased cerebral cortex neuronal survival. 56 Furthermore, in middle cerebral artery occlusion, E2 has been shown to attenuate apoptosis processes such as caspase-3 activation, DNA fragmentation, and Akt kinase activation. 57 It is clear that estrogen plays a critical role in stroke outcomes, reducing infarct severity and regulating vascular tone.
Progesterone receptors also exist on vascular smooth muscle and endothelial cells,58,59 and their activation serves two functions. First, it decreases inflammation, 60 edema, 61 and oxidative stress, 62 subsequently leading to reduced cortical infarct. Second, they inhibit vascular smooth muscle proliferation, which is essential for atherogenesis. 63 In animal trials, micronized progestin has been shown to decrease stroke lesion volume; however, it also increased mortality after experimental stroke. 64 Future research conducted to ascertain the exact steroid-mediated mechanisms must consider factors such as timing of hormone exposure relative to menopause, differences in hormone preparation, and intrinsic stroke susceptibility to determine the viability of hormone replacement therapy.
Insulin-like growth factor (IGF), although not sex-specific in production levels, is similar to estrogen in the conferring of neuroprotective effects. The IGF system mediates a variety of anabolic and somatogenic effects and is produced by a myriad of cell types. 65 With respect to stroke, increased IGF levels have been connected to experimental hypoxic injury in areas of neuronal loss; specifically, microglia and astrocytes show increased post-ischemic production of IGF-1. 66 Low endogenous levels of IGF-1 have been also associated with increased stroke mortality. 67 More recently, studies on aging female rats have shown the neuroprotective post-stroke effect of IGF-1 treatment, which may reduce infarct volume,68,69 reduce cytokines and chemokines, and improve the blood–brain barrier stability. 70 Thus, the age-dependent decline of IGF-1 in middle-aged females 71 in conjunction with post-menopausal estrogen level drops may further serve to explain the stroke incidence and severity seen in older females. 72
Differential symptom presentation and associated treatment delays
Population-level studies on sex differences in stroke presentation have been limited. Available studies indicate that women display generalized symptoms more than men do, often presenting with non-traditional signs. 73 For example, in ischemic stroke, women more often have disorientation, generalized weakness, mental status changes, 74 headache, pain, and changes in consciousness. 75 Furthermore, women have been found to present with urinary incontinence, visual deficits such as diplopia, and dysphasia. 42 On the other hand, men more commonly present with nystagmus and sensory abnormalities. 74 These findings are relevant because they impact the treatment methods care providers choose; in turn, this affects patient outcomes.
As with symptomatic presentation differences between men and women, there has been minimal conclusive research on the effect of symptomatic presentation differences on pre-hospital delays between men and women. Various studies have noted that women arrive later than men,76–80 that women arrive sooner than men,81,82 and that there is no significant difference. 83 The reasons for these arrival time delays have been attributed to sex, 82 with studies noting that it may be in part due to women presenting with more non-traditional signs, which could account for greater delays in arrival to the emergency department and potential misdiagnosis.
According to many studies though, women are significantly older than men at stroke onset 31 and, thus, are more likely to be living alone or in an institution during a stroke episode. 84 Given that the response of nearby individuals is a key element in reducing delay time, 79 it is evident that living alone is thus positively correlated with increased pre-hospital delays. 85 As of now, a consensus has not been reached regarding if there are sex-dependent delays, and if they do exist, what are the reasons behind these delays. Nevertheless, it is evident that further research is necessary. In the meantime, healthcare providers must be aware of potential differences between men and women in order to choose appropriate treatment methods.
Treatment modalities
Hospital-based studies have been inconclusive as to ascertaining whether or not sex-dependent differences exist in the use of certain treatments. More convincing is the evidence that has been found regarding sex-dependent treatment effectiveness in women and men. With respect to frequency of use, women have been found to be less likely to get brain imaging, Doppler examination, echocardiograms, and angiography than age-adjusted men. 42 Another study found similar discrepancies in diagnostic procedures ordered for men and women, where women were less likely to receive echocardiography, angiography, cardiac monitoring, and lipid investigation; however, age-adjusted analyses found these differences to be insignificant except in the case of lipid investigation. 86
Carotid procedures are performed at very high rates in the United States. Carotid stenting has become an increasingly popular choice over carotid endarterectomy (CEA) in high-risk individuals; as noted in Figure 3, CEA rates continue to drop. Regarding interventions for carotid stenosis specifically, some of the recent trials comparing CEA and carotid artery stenting (CAS) have demonstrated sex-specific outcome variances. For example, carotid endarterectomy is performed less in women than in men, even after adjusting for age and comorbidity. 87 This conclusion is debated by other studies though, given that variation has been attributed to higher perioperative risk in women. 88 In addition, the disparity may be that men simply have a greater prevalence of carotid artery disease. 89 One study specifically found that when counting only procedures done for confirmed carotid artery occlusive disease, the differences between rates of CEA were negligible between the sexes. 90 Overall, men do tend to benefit more, given that only women and men with higher than 70% symptomatic stenosis receive similar long-term benefits. 88 Furthermore, in women without stroke risk factors other than carotid artery stenosis, CEA was not beneficial for women with 50–69% stenosis. 88 This finding may also explain why care providers may choose not to use the therapy as frequently in women, especially for those with less than a high-grade stenosis. 88

Rates of carotid endarterectomy versus carotid artery stenting. Republished with permission of Wolters Kluwer Health, Inc., from ref. 3; Copyright © 2015, American Heart Association, Inc.; Reproduced with permission.
In the recent prospective randomized trial Carotid Revascularization Endarterectomy versus Stenting Trial (CREST), sex differences were examined. 91 This robust trial found that the periprocedural risk of events was higher in women who underwent CAS compared to CEA, whereas there was little difference seen in outcomes among men. Whether or not this difference was due to differential decision-making remains to be studied. In a very recent study utilizing the Agency for Healthcare Research and Quality National Inpatient Sample and State Ambulatory Services Databases, 1.7 million patients who underwent CAS or CEA over a 14-year time frame were analyzed. 92 A major finding was that for risk-matched patients, with both asymptomatic and symptomatic carotid disease undergoing CAS, female sex was an important variable associated with worse outcomes including higher stroke risk and inpatient mortality. Conversely, women, as well as men, undergoing CEA in this study had superior outcomes. Therefore, more work is needed to identify specific populations who will benefit from carotid intervention and why, exactly, do sex differences exist.
Some therapies are offered at similar rates to both men and women, but differences exist in the benefits conferred. For example, men benefit more than women in stroke unit care even after shorter stays. 93 Furthermore, although men and women are admitted to rehabilitation centers at equivalent rates, women have reduced functional recovery after stroke. 94 Additionally, stroke-related medication has been ascertained to be used less frequently in women. 34 Surprisingly, though, aspirin reduced ischemic stroke risk in women, but had minimal effects in men. 95 The exact underlying mechanism for this finding has not been determined, but one study indicates that it is due to sex hormone interaction with thrombosis. 96 Similar to aspirin, warfarin treatment was found to be lower in women upon admission and at discharge. 84 Nevertheless, warfarin treatment for women with atrial fibrillation-induced stroke showed greater risk reduction than in men. 93
While the aforementioned treatments are utilized, the only FDA-approved therapy for stroke is intravenous (IV) recombinant tissue plasminogen activator (rt-PA). 97 However, thrombolytics have been used at different rates based on sex. One large, retrospective study performed in a community hospital noted that male sex increased the likelihood of IV rt-PA usage. 98 These findings are alarming when considered in conjunction with epidemiological findings that stroke incidence in women is higher than in men. More concerning is that, with respect to IV rt-PA treatment differences, the primary reason for non-treatment was delayed presentation. 99 Given that women also have a greater likelihood to display diffuse non-specific symptoms, live alone, receive different diagnostic procedures, and experience significant delays in obtaining care in the hospital, this further reduces the possibility of them getting appropriate and timely care.
Therefore, future research needs to focus on developing treatments that are both effective in women and have longer therapeutic windows, given the potential delays in presentation for women. This is particularly important for preclinical studies as well, where novel neuroprotectants are initially tested. Recent studies using experimental models show that candidate compounds may be neuroprotective for stroke in one sex and not the other, as in the case of nitric oxide and poly(ADP-ribose) polymerase (PARP) inhibitors, 100 which are protective for stroke in males but not females, or caspase inhibition 101 or anti-Let7f, 102 which are protective in females but not males. Inclusion of clinically valid characteristics in experimental studies such as age, sex, and other comorbid disease will increase the likelihood of discovering effective stroke drugs.
Stroke outcomes
Post-stroke outcomes are poorer for women than for men. However, care must be taken in reviewing outcomes studies due to the variety of confounding variables that may be present. These include but are not limited to pre-stroke functionality, social support, demographics, and living conditions. On average, women experience more severe strokes 103 and have longer hospitals stays. 104 As a result, they have higher stroke-related mortality. 104 If they do survive the initial event, a higher percentage of women than men remain permanently disabled. 105
Consequently, this results in lower post-stroke quality of life. A stroke-specific quality of life scale measuring physical functional levels found that women scored lower than men. 73 Stroke-related outcomes also include reductions in mental health, and it has been shown that women are more likely to have post-stroke depression than men. 106 It should be noted that this may be ascribed to decreased social support, considering that women are more isolated than men at older ages. Nevertheless, this is a critical issue given that depression has been found to increase mortality, 107 decrease functional recovery, 108 and considerably undermine quality of life. 109
These changes can, in part, explain the reduced quality of life that women experience. The fact that women also more frequently require assistance with activities of daily living further contributes to understanding the quality of life scores. One study found that women had reduced odds, compared to men, of achieving activity of daily life independence 3 months after being discharged. Interestingly, these differences were not due to age at which stroke occurred or other clinical traits. 73 Supporting this research, another group found that women were more likely to be disabled, single, and in an assisted living home than men were 3–6 months after stroke. 110 These studies serve as strong evidence as to why women have higher dependency after strokes and more discharges to nursing homes. 111
Conclusions
Current research, albeit significant in the absolute number of studies, is still lacking based on the controversial and conflicting findings. The data are fairly solid and consistent regarding the epidemiology and outcomes of stroke in men and women, with women facing greater rates of stroke at older ages and worse outcomes. However, much work remains to be done in the identification of how men and women present differently following a stroke, both with regards to symptoms and signs as well as to presentation times. Table 3 summarizes the major salient findings in this review along with specific references supporting these results. Furthermore, research needs to focus on the differential response of care providers based on the sex of the patient, and how it can be standardized to offer equivalent levels of care. Finally, more research is needed to determine if and how sex-specific steroids confer neuroprotection against stroke. These topics are essential to understanding the differences identified in stroke outcomes for women and men.
Summary of Sex Differences in Stroke.
