
Abstract
Patients with abdominal aortic aneurysms (AAA) are more prone to develop popliteal artery aneurysms (PAA), but the prevalence is not well known. Our aim was to investigate the prevalence of PAA in patients with AAA, and to determine whether a certain risk factor profile is more commonly found in patients with concurrent aneurysms. All AAA patients (ICD code I71.3, I71.4) attending the outpatient clinic at the Karolinska University Hospital between 2011 and 2013 were included in the study cohort (n=465); 48% (225) had been subjected to an ultrasound or computed tomography scan of their popliteal arteries. In these patients, three definitions of PAA were considered (⩾ 10.5, ⩾ 12, ⩾ 15 mm), although the overall analysis is based on PAA ⩾ 12 mm. The mean age was 70.7 years (SD 7.5), 89% were men, and the mean AAA diameter was 47 mm (SD 14). The prevalence of PAA was 19% (n=43) by definition ⩾ 12 mm, and 11% (n=25) with 15 mm. Claudication was more frequently found in AAA patients with PAA than patients without PAA. Sensitivity between clinical examination and radiology was 26%, and the specificity for clinical examination was 90%. In conclusion, owing to the high prevalence of PAA in AAA patients, described by us and others, the low cost and risks associated with ultrasound and the poor sensitivity at clinical examination, all women and men with AAA should undergo one radiological examination of their popliteal arteries.
Introduction
Popliteal artery aneurysm (PAA) is a relatively rare disease in the population, 1 although it is the most frequently found arterial aneurysm after abdominal aortic aneurysm (AAA).2,3 The prevalence of AAA in the general population is approximately 1.5–2.5%.4,5 The prevalence of PAA is estimated to be 0.1–1% in the general population, with the majority of patients being elderly men.6–10 The presence of other aneurysms, especially in the abdominal aorta, is a major risk factor associated with PAA.10,11 Heart disease, stroke and smoking have also been reported to be more commonly found in this patient group.2,8,10 It is estimated that more than 50% of patients with bilateral PAA also have a coexisting AAA,8,10,12 but the prevalence of PAA in patients with AAA is not well known; in a few reports it varies between 0% and 10% (Table 1, Figure 1).2,12,13 A population-based AAA screening program has been launched in a few countries, including Sweden, to detect AAA in men in order to prevent rupture and death, which can introduce an increase in the number of men with AAA subjected to surveillance programs at vascular departments.14,15
Reports on the prevalence of PAA in AAA patients, including the present report.
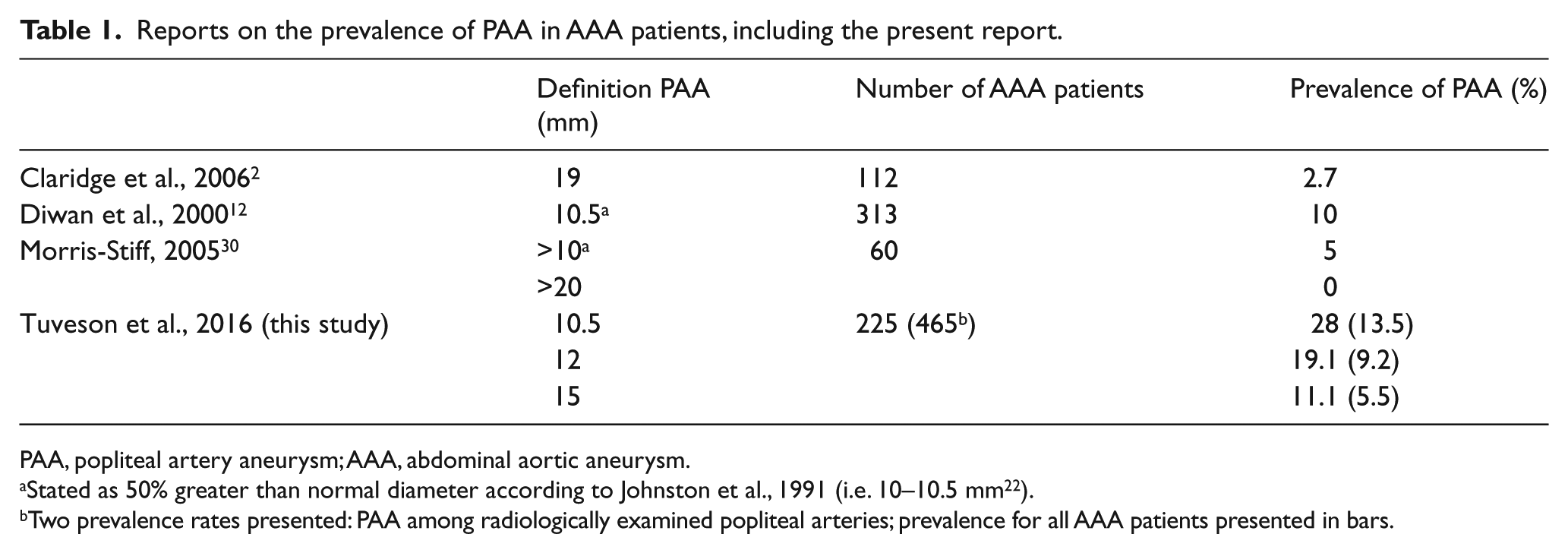
PAA, popliteal artery aneurysm; AAA, abdominal aortic aneurysm.
Stated as 50% greater than normal diameter according to Johnston et al., 1991 (i.e. 10–10.5 mm 22 ).
Two prevalence rates presented: PAA among radiologically examined popliteal arteries; prevalence for all AAA patients presented in bars.
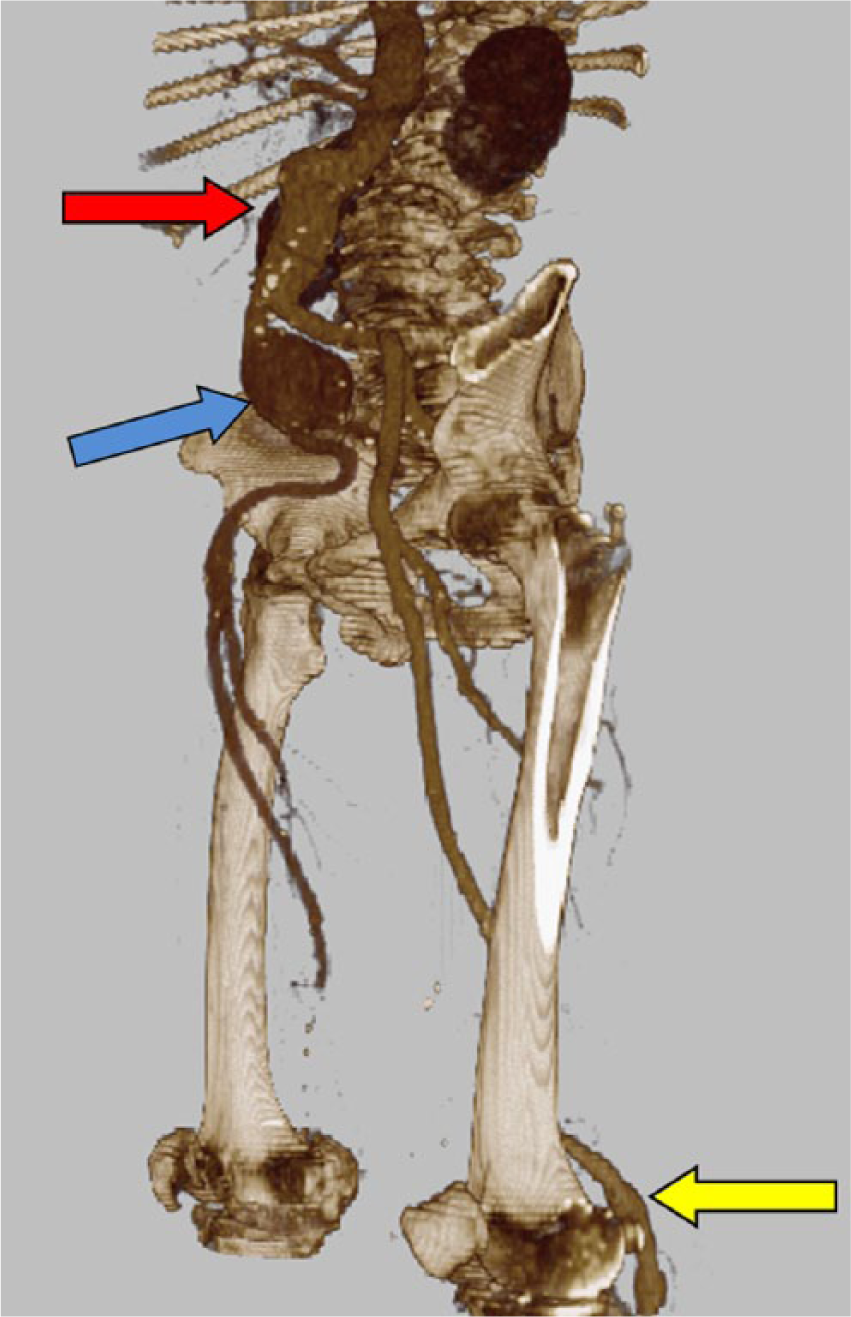
Abdominal aortic aneurysm (red arrow, top), right iliac aneurysm (blue arrow, middle) and popliteal occlusion (right side) and popliteal aneurysm (left side; yellow arrow, bottom) in the same patient, with a reconstructed, subtracted computed tomography angiogram.
Since the majority of PAAs are asymptomatic, they are often diagnosed with acute symptoms, such as acute limb ischemia, which can have devastating consequences; the amputation rate is reported to be approximately 20% in this group of patients.2,16 In contrast to an AAA, the diameter of a PAA is not a verified predictor for the evolvement of complications. 3 There is also an ambiguity regarding clinical and radiological examinations, and timing of treatment.8,11 No guidelines regarding surveillance intervals have been published; however, some reports on growth have been published.3,8,17,18 It is also unclear if specific definitions for diameter criteria or surveillance should be developed for women. 19 It is critical to further investigate the true prevalence of PAA in patients with AAA since this group of patients is more prone to develop peripheral aneurysms.2,12 The aim of this study was to define the prevalence of PAA in patients with AAA, and investigate if a specific subset of AAA patients more commonly has a concurrent PAA.
Methods
This was a retrospective population-based cohort study including all patients with the diagnostic code for non-ruptured and ruptured AAA (I71.4 and I71.3) that visited the outpatient clinic at the Department of Vascular Surgery, Karolinska University Hospital, Stockholm, Sweden between January 2011 and December 2013. A total of 476 patients were registered to have an AAA in the hospital chart (Take Care, web-based hospital chart system), but 11 were excluded due to a wrong diagnosis. A total of 465 patients were eligible and included.
One reviewer (VT) investigated medical charts for all eligible patients and two second reviewers (HL, RH), blinded to the results of the first investigator, validated a random sample which showed 100% accuracy between charts and extracted data (30 complete charts, 6%). The identified variables were collected from the medical charts and included the diameters of AAAs and PAAs, height, weight, current medication, ankle pressure, results of blood tests, diseases, heredity for AAA, smoking habits, radiological examinations including ultrasound, clinical examination of the popliteal artery and other patient characteristics. Data from previous visits were used when variables could not be found at the index visit. Results from reports on ultrasound and computed tomography (CT) scans were included. Duplex ultrasound for AAA surveillance at our institution uses the leading-edge to leading-edge method; however, for PAA the outer-to-outer technique is most commonly used (personal communication with technician) due to smaller diameters and often a lack of atherosclerotic plaques. Gold standard surveillance for PAA is duplex ultrasound; a correct estimation of thrombus volume or extent in a majority of patients is not possible to perform. CT angiograms are gold standard for preoperative evaluation and give a high validity for thrombus estimations; however, few patients were subjected to this. Therefore, the extent of thrombus is not included in the analysis.
Definitions
Three alternative definitions of PAA were used: (1) 50% or greater of the average popliteal artery diameter, approximately 7 mm: hence 10.5 mm12,19–22; (2) ⩾ 12 mm 23 ; and (3) ⩾ 15 mm.2,10,24,25 An AAA was defined as an infrarenal diameter ⩾ 30 mm. 22 A thoracic artery aneurysm (TAA) was defined as a former TAA diagnosis or a diameter exceeding 37 mm. 26 Age was defined as the patient’s age at the first visit to the outpatient clinic; hypertension and hyperlipidemia were defined as being pharmacologically treated; smoking status was defined as a previous or present smoker; obesity as a body mass index (BMI) > 25 kg/m2; kidney disease as a creatinine value exceeding 130 μmol/l; chronic obstructive pulmonary disease (COPD) and stroke if defined by physician or stated by patient; cancer was defined as previous or present malignant disease; heart disease was defined as ischemic heart disease including angina pectoris (AP), acute myocardial infarction (AMI), heart failure, atrial fibrillation (AF) or heart valve disease. Ankle pressure (mmHg) measurements from the primary visit to the outpatient clinic were used; however, 118 patients had missing values because they were primarily on an AAA outpatient visit.
Catchment area
Stockholm has more than 2 million inhabitants and has two centers for vascular surgery; the centers are responsible for care in the west and east parts of the county (50% each). The male population is, since 2010, invited to a single ultrasound screening for AAA at 65 years. The prevalence of AAA in Sweden is < 1.5%; during the observation period 179 men were identified in the program. 4 Patients with AAA are systematically referred and surveyed at these vascular centers; general practitioners do not care for the surveillance of this patient group. This study includes the patients with AAA at the outpatient clinic of the Karolinska University Hospital. The study was approved by the Regional Ethics Board in Stockholm, Sweden, and informed consent was not called for.
Statistics
Comparison between groups was performed with the independent t-test, since the data were normally distributed. Distribution of categorical data was tested with Fisher’s exact test. Statistical significance was defined as a p-value less than 0.05. Statistical analysis was performed using IBM SPSS software (version 22; IBM Corp., Somers, NY, USA).
Results
Study group
A total of 465 patients were eligible and included in the study; patient characteristics are presented in Table 2. A majority were men (89%, 413). The mean age was 70.7 years (range 50–91); women were older than men (mean age 74.1 vs 70.3, p=0.01). The mean AAA diameter was similar in women and men (46.7 mm vs 47.3 mm, p=0.77) and 47.2 mm for both sexes. No differences were seen in smoking habits or co-morbidities among men and women (data not shown).
Patient characteristics for all patients with AAA, plus patients who did or did not have a radiological examination of the popliteal arteries.
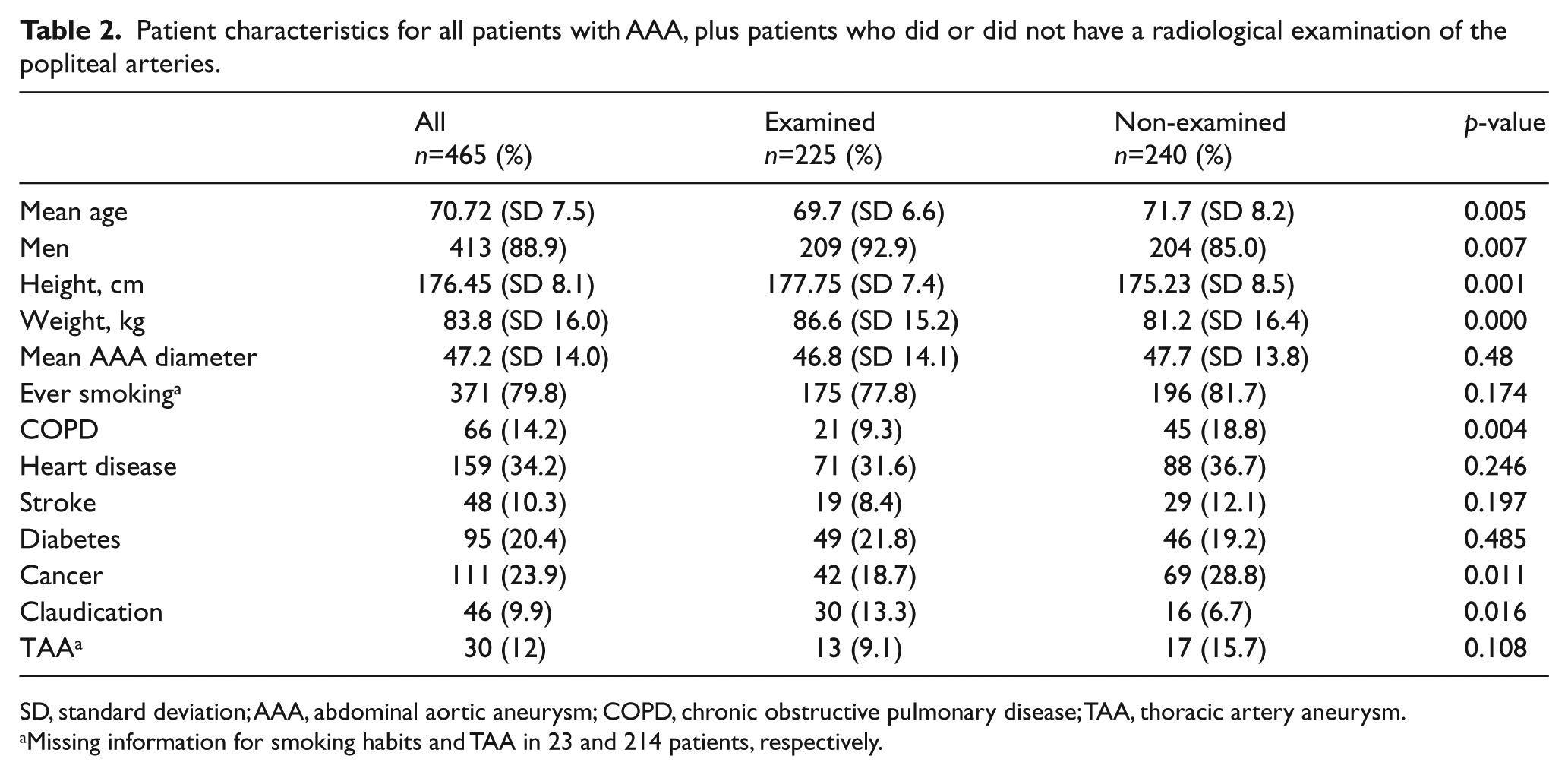
SD, standard deviation; AAA, abdominal aortic aneurysm; COPD, chronic obstructive pulmonary disease; TAA, thoracic artery aneurysm.
Missing information for smoking habits and TAA in 23 and 214 patients, respectively.
Radiological examined
A total of 448 patients (96.3%) were clinically examined for PAA, and 225 (48%) were subjected to a radiological examination of the popliteal arteries (Figure 2, Table 2). One-fourth of the patients with a positive clinical examination had a radiologically confirmed PAA (n=34, 26%), and 10% of the normal clinical examinations had a PAA (9/94). This gives a sensitivity of 26% and a specificity of 90% from the clinical examination for PAA (Figure 2).
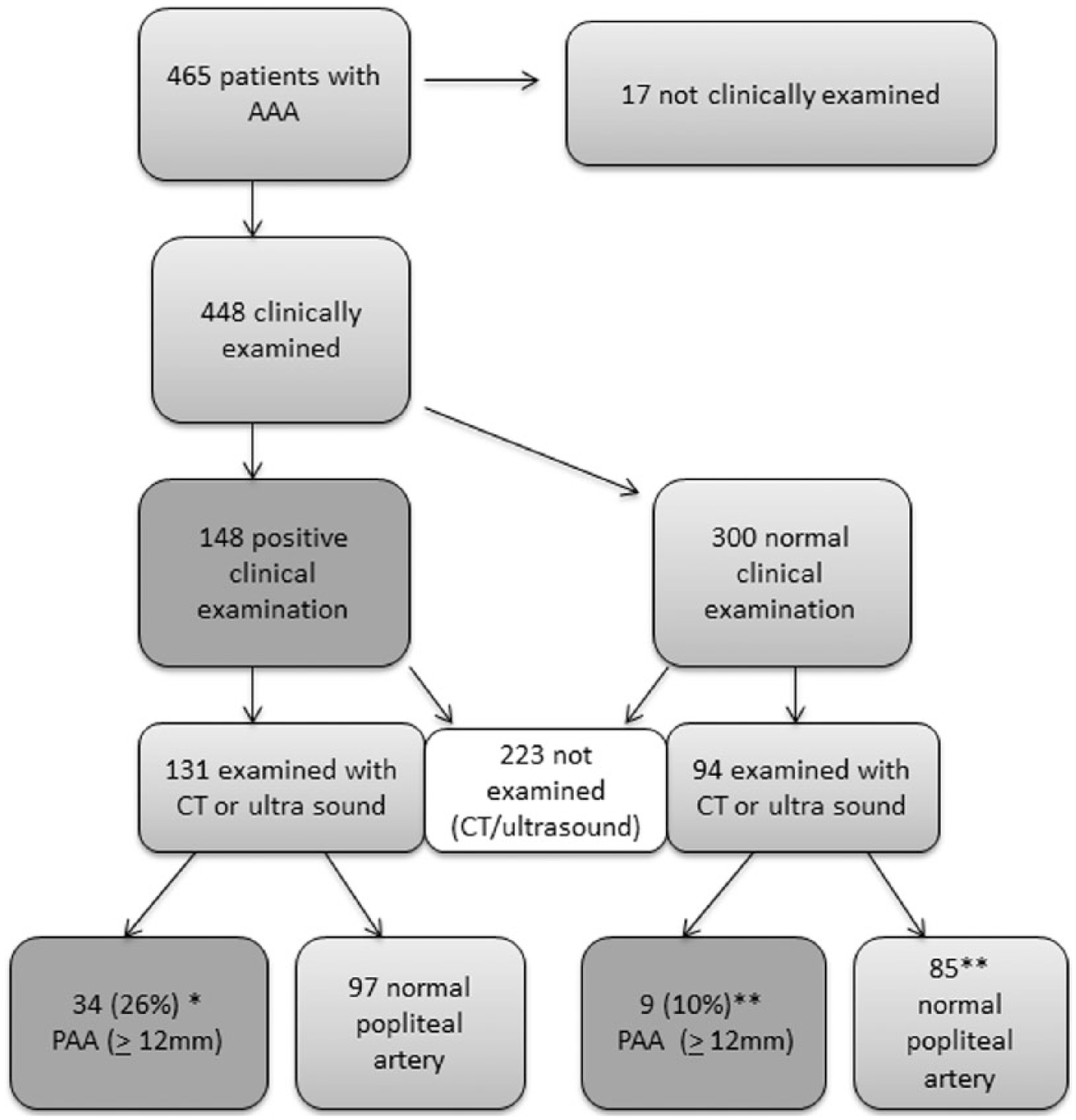
Findings at the clinical examination in the outpatient clinic and at the radiological examination (computed tomography or ultrasound), presented as patients, not limbs, with popliteal artery aneurysm (PAA). PAA is defined here as > 12 mm. The correlation between clinical findings and radiology is defined as true positive and false positive presented. *True positive, sensitivity of clinical examination, 26% (34/131); **false positive, specificity of clinical examination, 90% (85/94).
The patients who were not subjected to radiological examination were older (mean age 71.7 vs 69.7 years, p=0.005), and the proportion of women was higher among the non-examined patients (15% vs 7%). The non-examined patients had more COPD and cancer and less claudication. No other differences were seen between the two groups (Table 2).
Prevalence of PAA
PAA prevalence varies accordingly when different definitions are applied: of all 225 examined patients, 28% (n=63) had a PAA ⩾ 10.5 mm, 19% (n=43) had a PAA ⩾ 12 mm and 11% (n=25) had a PAA ⩾ 15 mm (Table 3). A majority of the patients with PAA were men (n=41). Among the minority of radiologically examined women, 12% had a PAA. The data presented below are based on the PAA defined as ⩾ 12 mm in the examined cohort. A total of 67 aneurysms were found in 43 patients, a majority had bilateral disease (24 bilateral vs 19 unilateral disease). The mean PAA diameter was 19.9 mm (12–100 mm). Claudication occurred more frequently in patients with PAA (p=0.009) than among patients with only AAA (25.6% vs 10.4%), and PAA patients also differed in mean ankle pressure (Table 4). No differences in the aneurysm diameter or prevalence of co-morbidities (COPD, heart disease, stroke, cancer, diabetes) were found (data not shown). In total, 26% were treated for their PAA (n=11 of 43).
Prevalence of PAA in women and men with AAA examined radiologically, defined as 12, 15 or 20 mm in diameter (n=225).
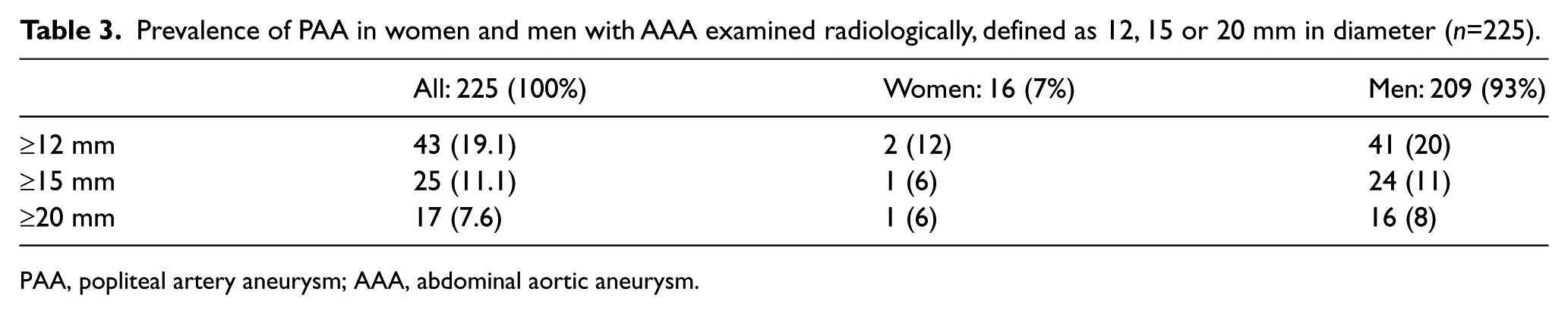
PAA, popliteal artery aneurysm; AAA, abdominal aortic aneurysm.
Patient characteristics for all radiologically examined patients with AAA only or AAA and PAA.
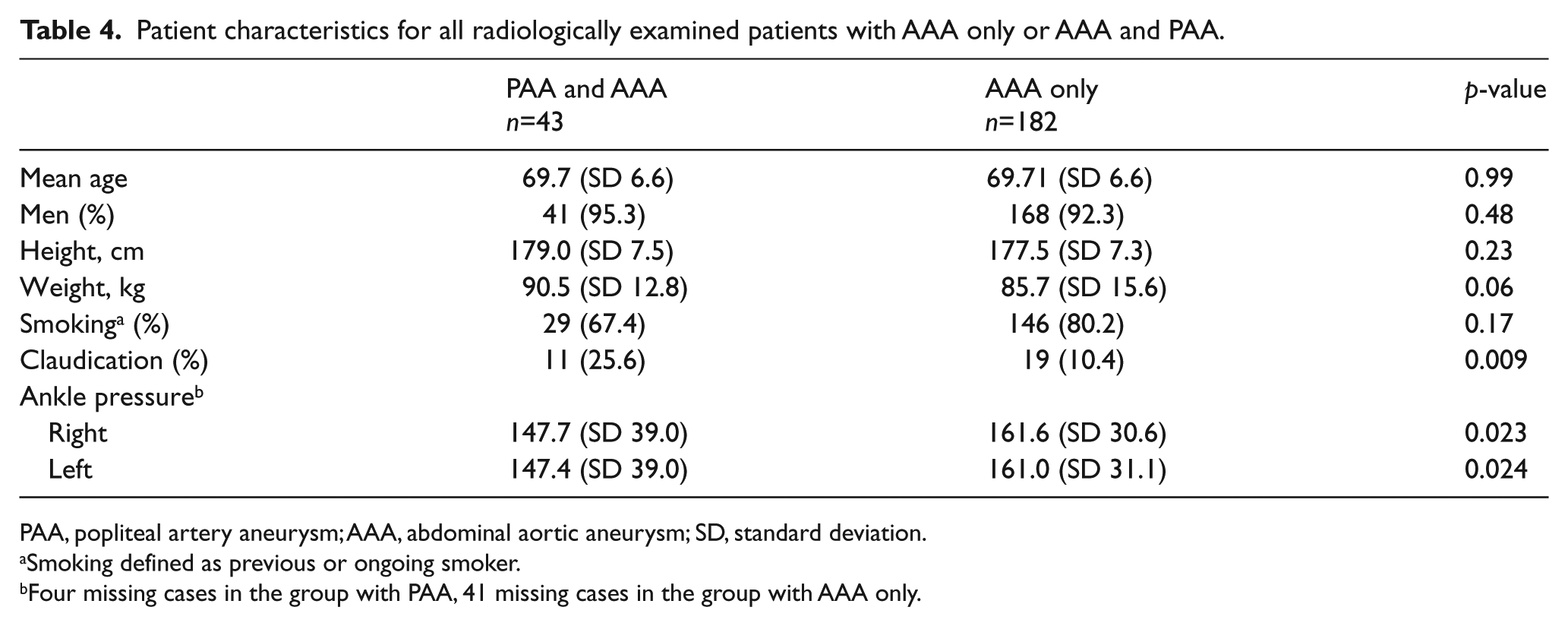
PAA, popliteal artery aneurysm; AAA, abdominal aortic aneurysm; SD, standard deviation.
Smoking defined as previous or ongoing smoker.
Four missing cases in the group with PAA, 41 missing cases in the group with AAA only.
Diameter of AAA and PAA
Among the radiologically examined patients, 57% (n=129) had an AAA diameter below 50 mm, and 43% (n=96) had an AAA diameter ⩾ 50 mm. The distribution of PAA between the groups was similar, regardless of the definition (PAA ⩾ 12 mm: 19% small vs 20% large AAA, p=0.823; PAA ⩾ 15 mm: 8.5% small vs 15% large AAA, p=0.153).
Discussion
This study shows that almost one-fifth of patients with AAA who had been subjected to a radiological examination of their popliteal artery also had a PAA. Clinical examination was a poor predictor for PAA, with 26% false positives and 90% false negatives. Claudication was more commonly found in this subgroup. There was no correlation between the diameter of the AAA and prevalence of PAA.
The lack of a contemporary and accepted definition of disease within the PAA field makes comparisons on definitions, prevalence and surveillance difficult.1,6,7,13,20 The majority of previous studies on patients with PAA include only treated or symptomatic patients, and the majority are quite small, single-center series.11,25,27 The definition of a PAA varies – between 1.5 times the normal artery diameter and larger than 20 mm in different studies – which makes all comparisons difficult (Table 1).2,10,19–21,23,24,28,29
Since the definition of 10.5 mm has not been commonly used, and could be controversial, we defined a PAA as ⩾ 12 mm.19,20,30 Our study shows a higher prevalence than the few previous reports within the field; however, if non-examined patients are included in the nominator, the prevalence decreases.2,12,30 Claridge et al. 2 presented a prevalence of 2.7%, corresponding to 7.6% in our dataset (Table 1). Another study based on a male AAA screening program reported a prevalence of 4.3%, but large variations due to different criteria are found here. 30 Diwan reported 10% in a larger study based on 313 AAA patients 12 (Table 1). The definition of a PAA of ⩾ 19 mm, used in some reports, is a too-strict lower limit for surveillance because some patients can suffer from acute events below this threshold.10,20,23
Could the risk factor distribution be different, or does the baseline AAA diameter correlate with the PAA prevalence rates? The distribution of risk factors in our study corresponds well with other studies.19,24 In Claridge’s and Diwan’s material, the mean abdominal aortic diameter varied between 34.5 and 58 mm, compared to 47 mm in our study.2,12 There was no correlation between AAA diameter and prevalence of PAA in our dataset, which indicates that AAA diameter should not influence the surveillance protocols for PAA.
The group with PAA had claudication to a greater extent compared to the group with only AAA. This could be interpreted as a complimentary possible predictor for which to screen patients, but could also depend on a selection bias in our study. Patients with symptoms could more commonly have been referred to radiology. However, the two groups did not differ from each other in regard to AAA diameter and other co-morbidities, which corresponds to earlier studies. 12
A majority of the study population was clinically examined in the popliteal fossa, but almost 10% of patients with a ‘negative’ clinical examination had PAA at radiology. This corresponds to other reports, and the findings altogether support that the ‘gold standard diagnostic method’ is radiological examination. Clinical examination has a high degree of uncertainty and holds a large number of both false positive and negative cases.12,23
The gender aspects are rarely addressed within the field, and several older series report 0–9% of women with PAA.11,25,27,29 Even if there were few women, 12% of the examined women had PAA, which should support that future surveillance programs for PAA in AAA patients also include women.
Growth rates and surveillance intervals for PAA patients have been poorly addressed previously.3,10,17,18 The growth rate is difficult to assess, due mainly to methodological problems, but one can probably summarize the reports on growth as follows, and adopt surveillance protocols accordingly: < 20 mm = 1.5 mm/year, 20–30 mm = 3 mm/year, and > 30 = 3.7 mm/year.3,10,17,18 Our department has surveillance protocols for PAA > 12 mm, with 3-year intervals for the smallest aneurysms, modified accordingly when larger diameters are registered. One-fourth of the identified PAA patients had elective vascular surgery for their PAA during the study period, emphasizing the seriousness of the disease.
The non-examined patients were older and had a higher proportion of women and diseased patients than the examined group. This finding indicates that we should not exclude older patients and women from further radiological examinations. This could be a clinically relevant decision in selected cases, though possibly not to such an extent.
Limitations
Analysis of PAA patients is difficult due to a lack of standardized definitions for the disease; in order to address this, several definitions are included.8,19,21 Guidelines for the surveillance of this subset of aneurysm patients is scarce, in contrast to AAA patients, often resulting in random follow-up by the surgeon in charge of AAA supervision. The number of AAA patients under observation at our institution is large, but still almost half of these had not undergone a radiological examination of their popliteal artery, which affects the possibility of defining the true prevalence. This is a possible problem commonly found for this patient group. The analysis is mainly presented for the radiologically examined patients, which could introduce a bias, since these patients may have symptoms which led to an examination. To exclude a high risk of differences between the groups, baseline data on the examined and non-examined groups, as well as the prevalence, is presented, and a low degree of differences are detected. AAA patients in the outpatient clinic do not always have an ankle pressure recorded. Owing to the retrospective design, this cannot be retrieved or added.
Conclusion
In conclusion, considering the high prevalence of PAA in the AAA patient group, we suggest that all men and women with AAA, and an acceptable life expectancy, should undergo a single radiological examination of PAA, preferably with ultrasound. Clinical examination as a sole diagnostic tool for PAA is again proven to be insufficient.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Stockholms Läns Landsting, ALF / Hjärt-Lungfonden 10.13039/501100003793.