
Abstract
This study was undertaken to determine the impact of shared decision-making when selecting a sedation option, from no sedation (local anesthetic), minimal sedation (anxiolysis with a benzodiazepine) or moderate sedation (benzodiazepine and opiate), for venous access device placement (port-a-cath and tunneled catheters) on patient choice, satisfaction and recovery time. This is an IRB-approved, HIPPA-compliant, retrospective study of 198 patients (18–85 years old, 60% female) presenting to an ambulatory vascular interventional radiology department for venous access device placement between 22 October 2014 and 7 October 2015. Patients were educated about sedation options and given the choice of undergoing the procedure with no sedation (local anesthetic only), or minimal or moderate sedation. Satisfaction was assessed through three survey questions. No sedation was selected by 53/198 (27%), minimal sedation by 71/198 (36%) and moderate sedation by 74/198 (37%). All subjects would recommend the option to another patient and valued the opportunity to select a sedation option. Post-procedure recovery time differences were statistically significant (p<0.0001) with median recovery times of 0 minutes for no sedation, 38 minutes for minimal sedation and 64 minutes for moderate sedation. In conclusion, patient sedation preference for venous access device placement is variable, signifying there is a role for shared decision-making as it empowers the patient to select the option most aligned with his or her goals. The procedure is well-tolerated, associated with high satisfaction, and the impact on departmental flow is notable because patients choosing no or minimal sedation results in a decreased post-procedure recovery time burden.
Keywords
Introduction
Over the past few decades, placement of venous access devices has shifted from the operating room to outpatient ambulatory centers. As a result, there has been a significant growth in short-duration vascular access procedures, including the placement of totally implanted venous access ports (TIVAPs) and partially implanted venous access devices (PIVADs) such as tunneled small bore central venous catheters. 1 Their utility in safely delivering chemotherapeutic drugs, supportive care, and enabling blood draws without requiring repeated venapunctures has facilitated care for patients requiring long-term venous access. 2
Procedural sedation comprises a continuum of states that range from minimal (anxiolysis) and moderate (conscious) sedation to deep sedation and general anesthesia, resulting in variable sedation practices. Moderate procedural sedation (combination of an opioid for pain control and a benzodiazepine, which serves as an anxiolytic while promoting amnesia) is used in the majority of these procedures.3–5 The disadvantages of sedation include the risk of increased cardiopulmonary complications, side effects, the need for an escort home, disruption of daily activities, time off work requirement, peri-procedure time (turnaround in the procedure room and occupancy of recovery area) and cost to the healthcare system. 6
There is a widespread assumption that patients who receive deeper sedation for brief procedures are more satisfied. Contrary to this belief, multiple publications report high levels of satisfaction and no differences in sedation scores or willingness to return for a repeat procedure whether the patient received local anesthetic, anxiolysis or intravenous moderate sedation during a procedure. 5 This suggests a lack of understanding about patient sedation preference, and led one author to conclude that since the procedure is well tolerated with each sedation option, conscious sedation should only be used selectively and not routinely. 7
With the range of clinically appropriate sedation options available, each with benefits and drawbacks, we posit that the level of sedation should be determined on a case-by-case basis taking into consideration patient pain tolerance, anxiety, expected discomfort and patient preferences through shared decision-making. Both the Affordable Care Act (ACA) and the Institute of Medicine (IOM) support the development of shared decision-making tools and techniques as a critical element of patient-centered care.8–11
Shared decision-making is a collaborative process where patients and providers make health care decisions together. During shared decision-making, providers present the treatment options available and empower the patient to be an active participant in selecting the therapy that is best aligned with his or her individual values and goals. 12
This study was undertaken to determine how employing shared decision-making when selecting a sedation option from no sedation (local anesthetic only), minimal sedation (anxiolysis with a benzodiazepine) or moderate sedation (benzodiazepine and opiate) for TIVAP and PIVAD placement impacts patient choice, satisfaction and recovery time.
Methods
Shared decision-making
In this institutional review board (IRB)-approved, Health Insurance Portability and Accountability Act (HIPPA)- compliant, retrospective study, 198 patients (18–85 years old, mean 60 years; 63% female, 37% male) who presented consecutively to a single-center, ambulatory vascular interventional radiology department for placement of a TIVAP or PIVAD between 22 October 2014 and 7 October 2015 were included in the study. Only those patients scheduled with vascular specialist MDC, who has taken a course on shared decision-making and whose standard practice is to employ sedation shared decision-making for sedation preference, were chosen for inclusion in this study. Shared decision-making was initiated by the operator for the case (MDC) following the three-step model proposed by Elwyn et al. 13 This discussion took place immediately prior to the procedure in a room off the pre-procedure work-up area. Family members were invited to be present for the discussion. Options were framed in the same way each time to achieve standardization. These included: (1) introducing the idea that there is choice in sedation and reasonable options available; (2) describing in detail the options available, including risks, benefits, alternatives, medications used, possible side effects from sedation (such as postoperative nausea, vomiting, and impaired cognitive function, coordination, and respiratory and spontaneous ventilation), and intra-procedure and recovery room expectations; and (3) supporting patients in the decision-making process, including encouraging discussion with the family, supporting deliberation about the pros and cons of each option, helping patients explore their comfort levels through asking about their goals for the experience and empowering them to make a decision consistent with their preference. The options presented included undergoing the procedure with no sedation (local lidocaine only), minimal sedation (anxiolysis with either intravenous midazolam or sublingual lorazepam) or moderate sedation (a combination of intravenous midazolam and fentanyl) (Table 1).
Sedation levels, options and agents.
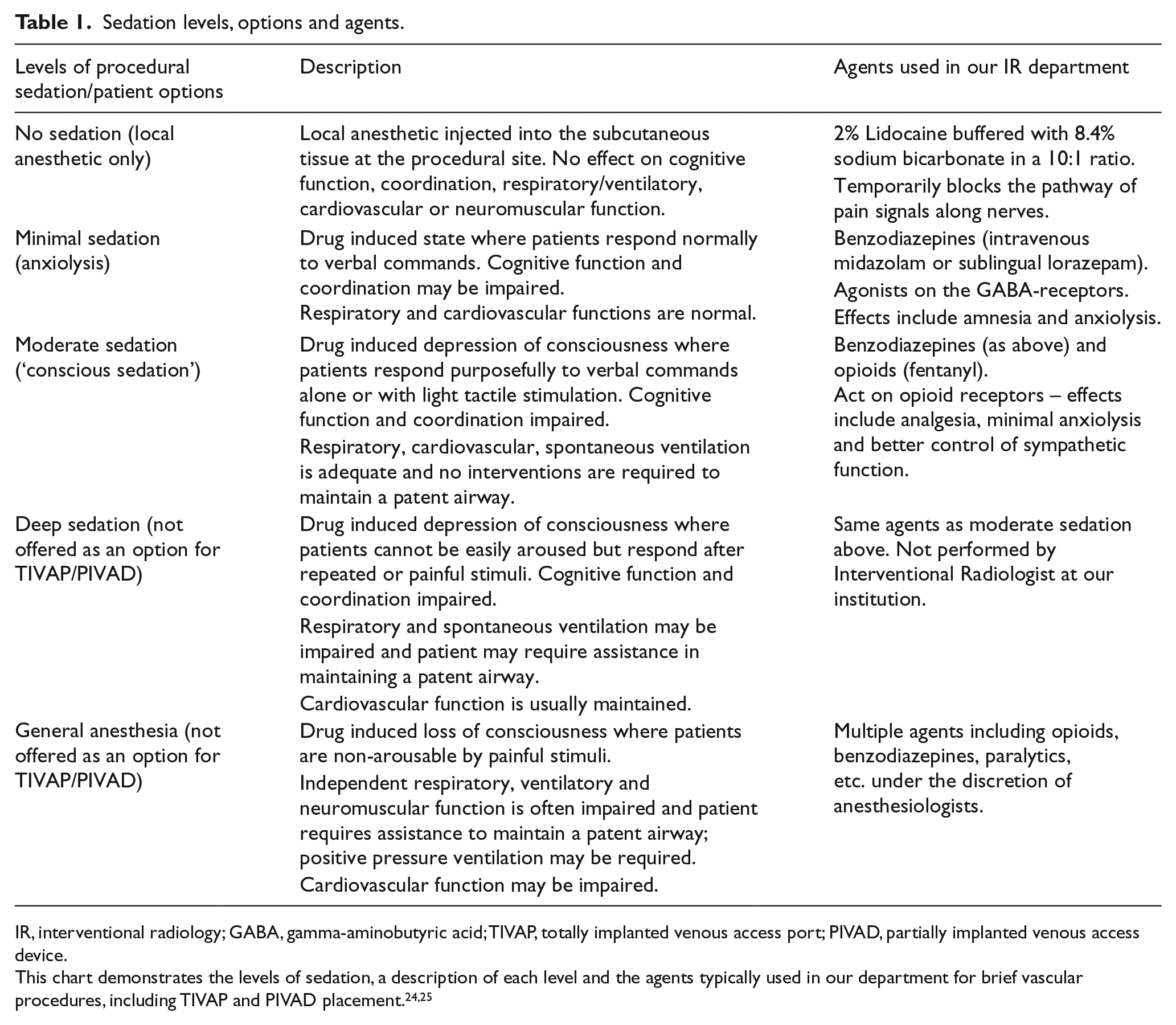
IR, interventional radiology; GABA, gamma-aminobutyric acid; TIVAP, totally implanted venous access port; PIVAD, partially implanted venous access device.
Sedation procedural details
All patients received 20 cc of 2% local lidocaine buffered with 2 cc of 8.4% sodium bicarbonate to anesthetize the procedural site. The amount of medication used for minimal sedation was selected based on patient preference of an oral benzodiazepine (0.5 or 1 mg sublingual lorazepam administered 15 minutes prior to the procedure) versus an intravenous benzodiazepine (1–4 mg IV midazolam) intraprocedurally titrated to minimal sedation. If intravenous sedation was preferred, the amount administered was determined using a standard sedation order set, which specified the following dosing: midazolam 0.5 mg IV push every 3 minutes × 2 doses and then 0.5–1 mg IV push every 3 minutes × 8 doses per need (PRN) titrated to minimal or moderate sedation; fentanyl 12.5 μg IV push every 3 minutes × 2 doses and 12.5–50 μg IV push every 3 minutes × 6 doses PRN given in combination with a benzodiazepine and titrated to moderate sedation. Interventional radiology nurses trained and certified in procedural sedation administered the intravenous medications as ordered and titrated the medication level to minimal or moderate sedation. With minimal sedation the aim was for the patient to be tired and sleepy but to respond appropriately to verbal conversation and sounds. For moderate sedation the aim was for the patient to be somnolent and sleeping but easily aroused with light tactile stimulation. Written informed procedural consent was obtained, which included a section on consent for procedural sedation including the risks, benefits, side effects and alternatives. All patients were offered ‘on demand’ sedation based on the discomfort of their experience. This meant they were instructed to request additional medications if they felt they needed them at any point.
Outcomes measures
Procedures were performed by a single licensed practitioner with 4 years of experience placing TIVAPs and PIVADs. Sedation option selection, completion under original sedation selection, sedation complications, adverse procedure events, intra-procedure time, time burden associated with post-procedure recovery on site, and patient satisfaction were tracked. Patients were discharged once their Aldrete procedural sedation recovery assessment score exceeded 10 points. The Aldrete scale is a validated tool used in our department as a measurement of recovery after sedation that includes gauging consciousness, activity, respiration, oxygen saturation, pain and blood pressure. A point value from 0 to 2 is assigned for each category and summed to get a total score. 14 A score of 10–12 indicates the patient is ready for discharge. In addition, the following criteria were met: hemoglobin oxygen saturation >93% or at pre-sedation baseline; mental status returned to baseline; protective reflexes intact; state of hydration adequate; cardiovascular function and airway stable; and mobility at pre-procedure baseline. If patients were stable and had received only local anesthetic they did not need to return to the recovery room and could be discharged home from the procedural suite after their nurse had reviewed all discharge instructions. An escort home was required if the patient received minimal or moderate sedation but not if the patient received no sedation (local anesthetic only). Prior to discharge, and as part of standard care and satisfaction assessments in this ambulatory center, patients were asked to complete a satisfaction survey asking them how they felt about three statements. Response choices were strongly agree, agree, uncertain, disagree and strongly disagree. The statements were: (1) I would recommend this sedation option to another patient; (2) I was satisfied and would choose this sedation option again; and (3) I valued the opportunity to be educated about the sedation options and participate in selecting the sedation option for my procedure (Table 2). Recovery room time was collected from the patient’s paper medical flow chart where nurses record the time in and time out of the recovery room.
Patient sedation satisfaction survey: ‘How strongly do you agree or disagree with each of the following statements?’
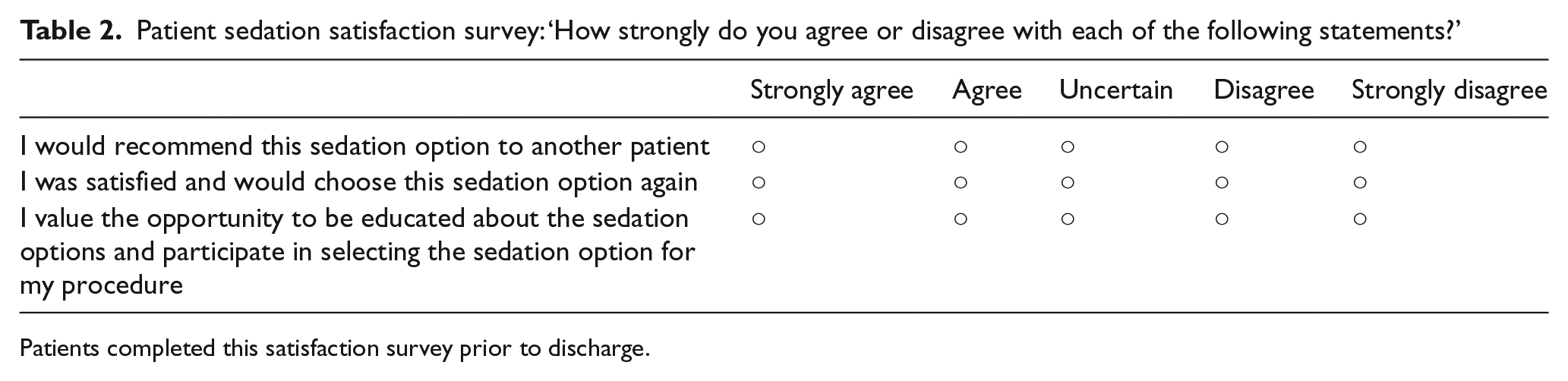
Patients completed this satisfaction survey prior to discharge.
Historical sedation practice
As a baseline and historical comparison to the time prior to employing shared decision-making, a chart review was performed on a sample of 59 patients who presented consecutively for PIVAD and TIVAP placements between 3 April 2013 and 1 July 2013. Both sedation type and the rationale for that sedation option were obtained from the procedure report.
Statistics
The Wilcoxon rank-sum test was used to compare the median recovery time between two sedation groups at a time and the Kruskal-Wallis rank test was used to compare the median recovery time among the three groups. The statistical software package STATA, version 14 (StataCorp LP, College Station, TX, USA) was used for all analyses, with a p-value < 0.05 considered to be statistically significant.
Results
No sedation (local anesthetic only) was selected by 53/198 (27%) patients, 36% female; minimal sedation was chosen by 71/198 (36%), 70% female; and moderate sedation was chosen by 74/198 (37%), 68% female. All patients completed the procedure with the option they initially selected without requiring a higher level of sedation.
A total of 22/198 (11%) patients had a PIVAD placed (a tunneled small bore central venous catheter), and of this subset of patients no sedation (local anesthetic only) was selected by 13/22 (59%) patients, 3/22 (14%) desired minimal sedation and 6/22 (27%) opted for moderate sedation.
There were 176 patients who had a TIVAP placed (port-a-cath), and of this subset of patients no sedation (local anesthetic only) was selected by 40/176 (22%) patients, 68/176 (39%) desired minimal sedation and 68/176 (39%) opted for moderate sedation.
Medication amounts for minimal sedation ranged from 0.5 mg sublingual lorazepam to 4 mg IV midazolam. Medication amounts for moderate sedation ranged from 1.5 mg IV midazolam with 75 μg IV fentanyl to 4.5 mg IV midazolam with 225 μg IV fentanyl.
The historical chart review of 59 patients who presented for PIVAD and TIVAP procedures between 3 April 2013 and 1 July 2013 revealed 4/59 (6.8%) patients underwent the procedure with no sedation, 6/59 (10.2%) patients underwent the procedure with minimal sedation and 49/59 (83%) underwent the procedure with moderate sedation.
All patients (198/198; 100%) agreed or strongly agreed that they were satisfied and would recommend their option to another patient. One patient (0.5%) was uncertain whether to choose the option of minimal sedation again, expressing a preference for a deeper level of sedation. The remaining 197/198 (99.5%) agreed or strongly agreed that they would choose their selected option again. All patients strongly agreed that they valued the opportunity to be educated about and participate in selecting a sedation option for their procedure.
Post-procedure recovery room time was collected from the nursing flow sheet for 156/198 (78.8%) of the patients. No documented recovery room time was available in 7/198 (3.5%) of the records that were located for review and the ○ remaining 35/198 (17.7%) recovery room charts could not be located.
Recovery time is a continuous variable and was examined across categories of sedation options. The mean post-procedure recovery time for no sedation (local anesthetic only) was 6 minutes (SD ± 11), it was 40 minutes (SD ± 19) for minimal sedation, and 65 minutes (SD ± 16) for moderate sedation. The median post-procedure recovery time for no sedation (local anesthetic only) was 0 minutes (as frequently patients were discharged directly from the procedural suite and did not go to the recovery room), 38 minutes for minimal sedation (anxiolysis), and 64 minutes for moderate sedation. The Kruskal-Wallis rank test p-value = 0.0001, indicating that the differences in the median recovery time between the three groups are statistically significant. The Wilcoxon rank-sum test comparing differences in the median recovery time between two groups at a time revealed p<0.0001 for the mild sedation and no sedation groups; p<0.0001 for the mild sedation and moderate sedation groups; and p<0.0001 for the no sedation and moderate sedation groups (Table 3).
Recovery room times.
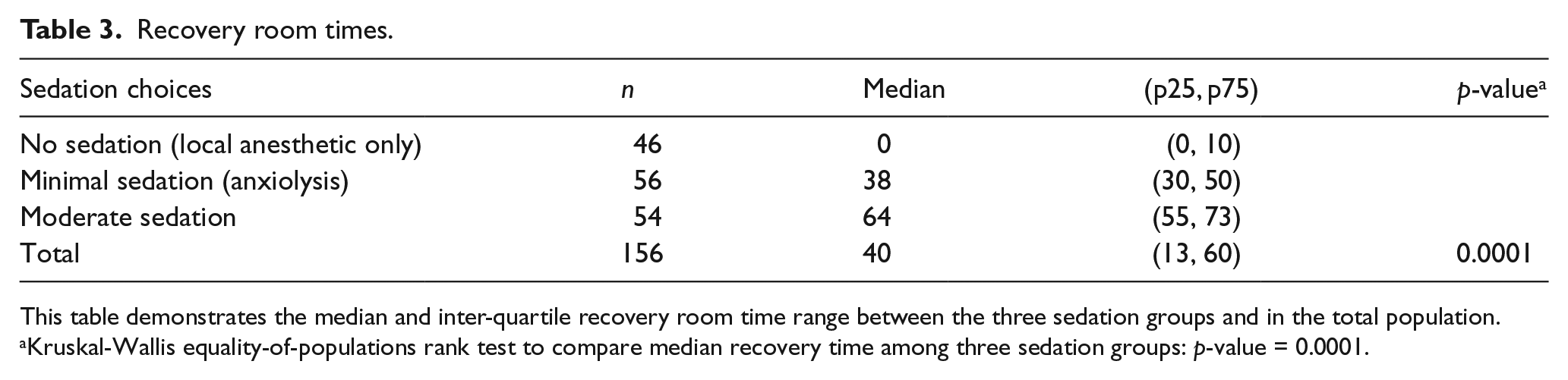
This table demonstrates the median and inter-quartile recovery room time range between the three sedation groups and in the total population.
Kruskal-Wallis equality-of-populations rank test to compare median recovery time among three sedation groups: p-value = 0.0001.
Discussion
An appropriate level of sedation should be acceptable to patients, enable their cooperation during the procedure and satisfy them as well as the proceduralist in order to provide optimum care. Sedation patterns for ambulatory vascular procedures are highly variable with differing amounts and levels of sedation as well as unique adjunctive methods being used for similar procedures in different institutions. Lang et al. 5 demonstrated that sedation selection is often determined by the habits and philosophies of the institution. Perhaps, surprisingly, neither patient anxiety/pain scores nor physician decision-making have been shown to universally affect drug utilization. 5
Historically, standard practice in our department was to place all venous access devices using moderate sedation with a combination of intravenous midazolam and fentanyl, as is evidenced by the vast majority of patients (49/59 (83%)) who underwent their procedures with moderate sedation prior to implementing shared decision-making. Only 10 patients in this historical group did not receive moderate sedation. The reason that 8/10 (80%) received an alternative form of sedation was not a result of shared decision-making, but rather a consequence of medical conditions that precluded safe administration of moderate sedation (i.e. opioid allergy, hypotension, significant pulmonary disease or multiple comorbidities). It was a rare exception (2/10 or 20%) that an alternate sedation option was selected as a result of the patient expressing a preference for it. This institutional philosophy is engrained in multiple ways, including through the fact that physicians, advanced practitioners, residents, fellows and nursing staff are trained to perform brief vascular access procedures with moderate sedation. This uniformity is reinforced through in-person and online competency training modules and lectures on administering moderate sedation. The use of standard medication order sets and pre-procedure paperwork with a readily available ‘moderate sedation’ check box encourages operators to select this as their default sedation plan, as alternative sedation options are not presented. This standard practice is further reinforced by the fact that patients present to the department with the expectation that they will receive moderate sedation as this is stated on their pre-procedure paperwork.
While moderate sedation was historically the standard practice at our institution, multiple studies looking at patient sedation experience for ambulatory vascular procedures indicate that patients who receive deeper sedation for brief procedures are not more satisfied. Both midazolam and midazolam with fentanyl were found to be satisfactory for coronary angiography with no difference in sedation scores, anxiolysis or patient and provider satisfaction levels. 15 Most patients experienced only low-level discomfort during diagnostic aortofemoral arteriography and expressed no difference in their willingness to return for a repeat procedure whether they received local, anxiolysis or intravenous moderate sedation. 16
This study and the aforementioned studies raise the question about whether moderate sedation is necessary and should be offered to patients for brief ambulatory vascular procedures like venous access device placement. Our sentiment is akin to that of Johnson, 17 who suggests that the goal of sedation for minimally invasive procedures is patient comfort, providing a safe and controlled environment, pain relief, minimizing negative psychological responses through relief of anxiety and fear, and decreasing complications by reducing patient movement and enabling cooperation in order to successfully and safely perform a procedure. Some patients do, in fact, require moderate procedural sedation in order to achieve this condition. So, while we do not advocate completely eliminating the option of moderate sedation for brief vascular access procedures, there is a need for a more patient-oriented approach to sedation that is individualized, involves a discussion about the various options and takes into consideration patient preferences, anxiety, pain tolerance, anticipated pain and length of procedure.
There are many non-pharmacologic methods that can act as a supplement or an alternative to sedation medications and successfully mitigate patients’ anxieties, reduce the amount of drugs needed and improve safety and speed of recovery. These include patient-focused approaches like offering the choice of music, hypnosis or anodyne imagery (conditioned relaxation, induction of a trance state and guided processing of the patient’s internal imagery).18–23 Despite the success of these techniques, placement of TIVAP and PIVAD in interventional radiology in the USA is performed primarily under procedural sedation using intravenous pharmacologic agents.3,4
The multiple proven methods to ease patient anxiety, including non-pharmacologic and a range of pharmacologic therapies, present an opportunity to employ shared decision-making so that patients can select the option that is most aligned with their comfort level. For instance, the ability to undergo TIVAP and PIVAD placement without sedation might be desirable for a patient who wishes to resume their activities immediately without limitation or prolonged recovery time. Furthermore, our institutional policy is that a patient who undergoes TIVAP and PIVAD placement without sedation can be discharged home without requiring an escort, which for many patients is desirable.
The impact of sedation choice on department flow is remarkable. Nurses noted that when patients underwent the procedure with local anesthetic it improved the overall efficiency (less need for nurse monitoring, a more rapid turnaround and a shorter recovery time), and they found discharge planning easier as amnesic effects were lessened.
Further evaluation looking at the amount of medications used and the cost associated with the different sedation scenarios could help understand the impact shared decision-making might have on health care costs.
Limitations
Limitations to integrating shared decision-making into an ambulatory vascular practice might include time constraints, lack of applicability to patient characteristics and the clinical situation. In addition, this project is limited by the fact that it was retrospective, was not randomized or blinded and included only one operator. The operator took a course on shared decision-making and, after a personal experience with a patient who was terrified of sedation and questioned why the procedure needed to be done with sedation, was influenced to the idea that there might be a gap in practice, and that shared decision-making, in regards to selecting a sedation option, could be beneficial. While the operator decided to incorporate shared decision-making as part of standard care for all patients presenting to her for vascular access device placement, other operators in the department performing vascular access device placement during this time were not included in this study because they did not employ shared decision-making as their standard of care. (Of note, two other operators have learned and are starting to incorporate shared decision-making as their standard practice.) Operator skill plays a substantial role in being able to perform these procedures without sedation, and the operator in this study is a vascular physician assistant who is highly specialized in venous access device placement, thus results may not be generalizable to other providers. These data refer only to shared decision-making regarding sedation prior to vascular device placement. Additional data would be needed to consider shared decision-making for other vascular procedures. Finally, this study was performed in a tertiary care academic medical center; a limitation might be difficulty in generalizing to other ambulatory vascular practice patterns.
Conclusion
TIVAP and PIVAD placement is well-tolerated under various sedation options, signifying a role for shared decision-making, which is associated with high patient satisfaction. The impact on departmental flow is also notable because patients choosing no or minimal sedation results in a decreased post-procedure recovery time burden.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.