
Abstract
Cardiac rehabilitation (CR) has proven morbidity and mortality benefits in cardiovascular disease, which directly correlates with exercise performance achieved. Many patients in CR exercise at sub-optimal levels, without obvious limitations. Occult lower-extremity peripheral artery disease (PAD) may be a determinant of diminished exercise capacity and reduced benefit obtained from traditional CR. In this prospective study of 150 consecutive patients enrolled in Phase II CR, we describe the prevalence of PAD, the utility of externally validated screening questionnaires, and the observed impact on CR outcomes. Abnormal ankle–brachial indices (ABI) (<0.9 and >1.4) were observed in 19% of those studied. The Edinburgh Claudication Questionnaire was insensitive for detecting PAD by low ABI in this population, and the Walking Impairment Questionnaire and a modified Gardner protocol demonstrated a lack of typical symptoms with low levels of activity. Importantly, at completion of traditional CR, exercise improvement measured in metabolic equivalents (METs) was worse in those with a low ABI compared to those with a normal ABI (+1.39 vs +2.41 METs, p=0.002). In conclusion, PAD is common in patients in Phase II CR and often clinically occult. Screening based on standard questionnaires appears insensitive in this population, suggesting a need for a broad-based screening strategy with ABI measurements. In this study, undiagnosed PAD significantly attenuated improvements in exercise performance, which potentially has bearings on future clinical events.
Introduction
Lower-extremity peripheral artery disease (PAD) is common in the United States, reaching a prevalence of approximately 4.6% in the general adult population. 1 This prevalence increases to an estimated 20–40% in patients with known coronary artery and cerebrovascular disease.2–4 The use of traditional risk factors for PAD is helpful in identifying those to screen in the general population, and include diabetes mellitus (DM), hypertension (HTN), dyslipidemia (DLD), obesity, tobacco use, and advanced age. 5
Symptoms and functional impairment arise from intermittent or chronic leg ischemia leading to claudication, but many patients have atypical symptoms or no apparent symptoms at all. It is estimated that only 10% of patients with PAD experience a classically described claudication. 1 Importantly, patients without these prototypical symptoms tend to have lower functional capacity than those with claudication, as measured by a 6-minute walk test or walking speed. 6 One potential explanation for this observation is that patients may unknowingly limit their activity and halt exercise prior to provoking symptoms. 7 In addition to lifestyle-limiting morbidity, the presence of PAD is also associated with a markedly increased risk of cardiovascular mortality. 8
Despite the high burden of disease and clinical consequences of lower-extremity PAD, it is often unrecognized and undervalued by patients, primary care physicians, and cardiologists.9–12 Consequently, there has been keen interest in developing universal screening strategies for patients at high risk for PAD, which includes the cardiac rehabilitation (CR) population. The ankle–brachial index (ABI) is commonly used for screening and is non-invasive. An ABI <0.9 has approximately 90% sensitivity and 95% specificity for angiographically significant PAD.13,14 New recommendations also suggest including patients with an ABI >1.40, representing non-compressible and calcified arteries, as diagnostic for PAD. 14 However, this group of patients does not necessarily have obstructive arterial and flow-limiting disease. Overall, screening for asymptomatic PAD would be valuable if it identifies patients in whom early risk factor modification or treatment would provide benefit.
In the setting of CR, there may be additional benefits of identifying occult PAD. Supervised walking exercise therapy has clearly been shown to improve total walking distance and delay the onset of claudication. 15 Similarly, strong outcomes evidence exists that exercise-based CR reduces total and cardiovascular mortality in addition to lowering morbidity.16–21 These benefits correlate with improvement in exercise capacity that is achieved during the rehabilitation program, highlighting the importance of processes that limit overall performance status during exercise training. However, the incidence of occult PAD in the CR population has not been carefully studied. Consequently, PAD screening and exercise prescriptions targeted for PAD are not commonly employed in current CR programs. This traditional CR programming employs a variety of endurance exercises and strength training aimed at increasing general exercise tolerance, but only some of which may overlap with PAD-focused exercise recommendations that typically are focused on the lower extremities and employ aerobic exercise to symptomatic endpoints. Strength training may be utilized in both cardiac and PAD programs, but is also typically of different focus. We hypothesized that the presence of occult PAD may be a determinant in limiting a patient’s functional benefit from traditional exercise-based CR.
In this study, we therefore aimed to describe the overall prevalence of an abnormal ABI (<0.9 or >1.4) among patients enrolled in a representative CR program and assess the effect of obstructive PAD (ABI <0.9) on patient outcomes as measured by improvement in exercise capacity. Secondary aims were to assess the utility of screening questionnaires in detecting obstructive PAD in patients enrolled in CR, and to assess the effects of PAD on low levels of activity.
Methods
This is a prospective observational cohort study of consecutive patients participating in Phase II CR at University Hospitals Harrington Heart & Vascular Institute’s nationally certified Cardiovascular Rehabilitation Programs. There were 222 patients assessed for eligibility and subsequently 150 were enrolled in our study. Inclusion criteria included all patients enrolling in one of the Phase II Cardiac Rehabilitation programs. Individuals requiring the use of assistive devices for ambulation or those who lacked capacity to give informed consent were excluded. The study was approved by the Institutional Review Board of University Hospitals Case Medical Center (Cleveland, OH) and written informed consent was obtained from all participants.
The rehabilitation staff screened patients for the study at the time of the patient’s initial intake visit. If enrollment criteria were met, a study investigator obtained informed consent when the patient presented for a subsequent CR visit. Consent to participate and enrollment into the study took place within the first six rehabilitation visits.
Our study was designed to have minimal interruption or alteration in the course of our typical Phase II Cardiac Rehabilitation program. For the purposes of screening for PAD, a validated screening tool (Edinburgh Claudication Questionnaire) 22 was administered and ABI measurements were obtained on the day of enrollment by the rehabilitation staff or a study investigator. Evaluation of functional impairment at low levels of activity was initially assessed on enrollment with a validated PAD functional assessment tool (Walking Impairment Questionnaire), 23 and subsequently by a standardized treadmill protocol (modified Gardner protocol: 2 mph or 3.2 kph, 0% grade, max = 10 minutes) 24 at the beginning of the next scheduled rehabilitation session. All the ensuing rehabilitation sessions proceeded as usual for the patient, with staff incrementing exercise prescription per routine. Demographic variables and medical history were also collected based on patient self-report and electronic medical record review. Estimated functional capacity in metabolic equivalents (METs) was obtained from monitored treadmill exercise at the first rehabilitation visit and the last rehabilitation visit (see below). Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at University Hospitals. REDCap is a secure, web-based application designed to support data capture for research studies, providing: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources. 25
Initial exercise prescription and exercise progression in our CR programs was unaltered for this observational study. In accord with our common practice and national recommendations, 22 patients were initially evaluated by a nurse and exercise physiologist and underwent a pre-program exercise treadmill stress test. The exercise stress test protocol was selected based upon the patient’s age, cardiac history, musculoskeletal status, and comorbitities (Cornell protocol was utilized in >80% of patients). The initial exercise prescription was set at 60–80% of heart rate reserve and an initial minimum duration (continuous or non-continuous) of 20 minutes. Patients exercised using a variety of aerobic exercise equipment (treadmill, bicycle, rower, NuStep). Based upon the overall clinical tolerability, symptoms as assessed by the Borg scale, heart rate response, and absence of ischemia or other adverse clinical findings, exercise intensity and/or duration was increased up to 10% every week. The target aerobic exercise duration was 45 minutes per session. Consistent with our historical practice, exercise prescription was not altered for those with diagnosed (by ABI) PAD but without claudication. All exercise prescriptions were reviewed and approved by the Medical Director or other responsible cardiologist. There were no conflicts of interest in the design of this study and no external sources of funding.
Data analysis
The prevalence of an abnormal ABI (<0.9 or >1.4) for the overall study population was described. Those with high ABI measurements were excluded from further analysis. Baseline characteristics of patients with a normal ABI were compared to those patients with a low ABI. Continuous variables were described with standard descriptive statistics including mean and standard deviation; between-group differences were tested for statistical significance with unpaired t-tests. Categorical variables were described as frequency and percentage; between-group differences were tested with Pearson’s chi-squared test. The test characteristics of the Edinburgh Claudication Questionnaire to detect a low ABI in this population were described in terms of sensitivity, specificity, positive predictive value and negative predictive value. Unpaired t-tests were used to compare the walking ability scores on the Walking Impairment Questionnaire, as well as the completion rate of walk tests between groups. Functional capacity was determined by the individual changes in estimated METs during treadmill exercise, and analyzed with unpaired t-tests. All statistical tests were two-sided with a 0.05 significance level. Analyses were performed with SPSS version 20 (IBM SPSS Statistics for Windows, Armonk, NY, USA).
Results
Patient population
Figure 1 details the study enrollment process. A total of 222 consecutive patients enrolled in Phase II Cardiac Rehabilitation were assessed for eligibility. A total of 72 patients were excluded from the study for the reasons described, leaving 150 to enroll in the study. Twelve patients dropped out before the initial ABI was performed. Eight patients with high ABI measurements were excluded from further analysis, and primary and secondary analyses were performed in the remaining 130 patients enrolled in the study.
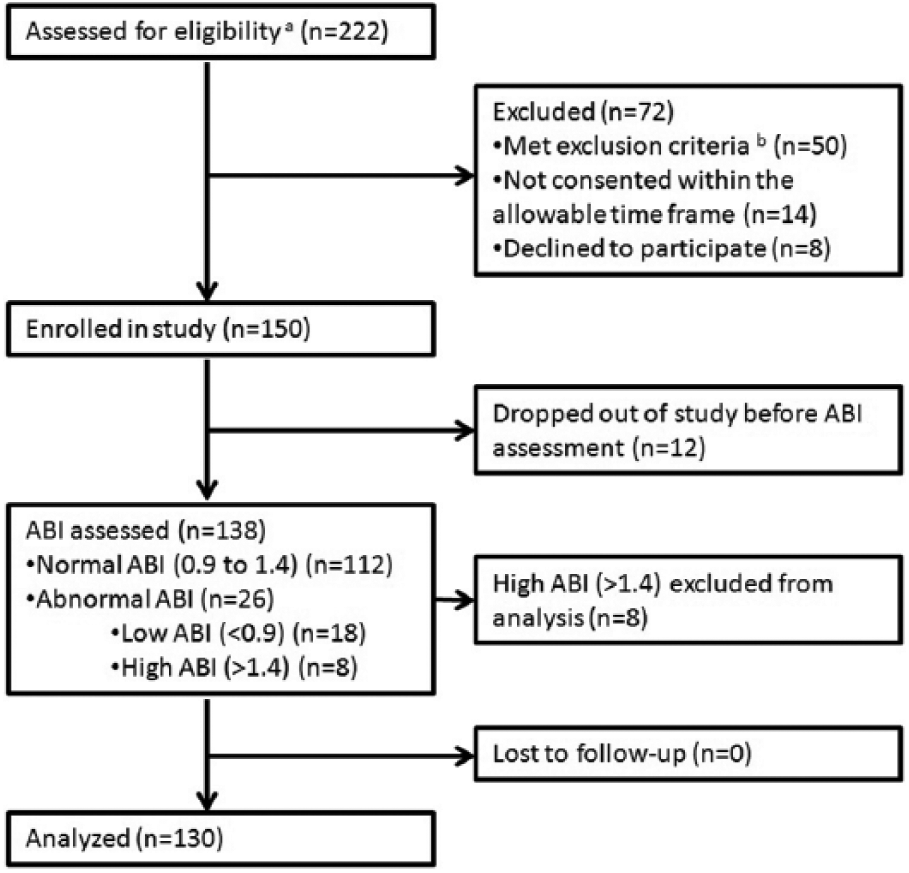
Flowchart of study population. aPatients met the inclusion criteria of enrolling in a Phase II Cardiac Rehabilitation program. bExclusion criteria included the use of assistive devices for ambulation or those who lacked the capacity to consent for the study. (ABI, ankle–brachial index.)
The overall prevalence of an abnormal ABI in the CR population was high at 19% (Figure 2). Eighteen patients (13%) had an abnormally low ABI (range: 0.50–0.89) and eight (6%) had an abnormally high ABI (range: 1.41–1.65, or non-compressible).
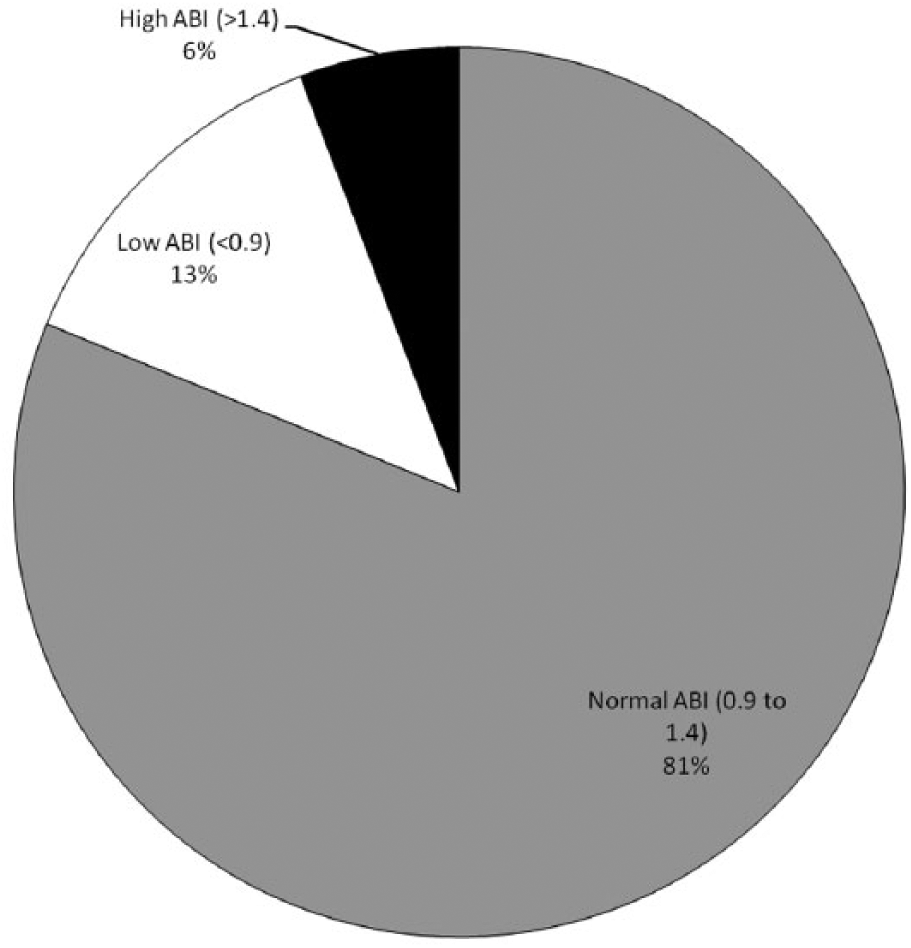
Prevalence of peripheral artery disease in the study population. (ABI, ankle–brachial index.)
The baseline characteristics of patients with a normal ABI compared to those with a low ABI are described in Table 1. No significant differences were found between the groups except for the presence of heart failure (p=0.02).
Baseline characteristics of the study population according to peripheral artery disease screening status.
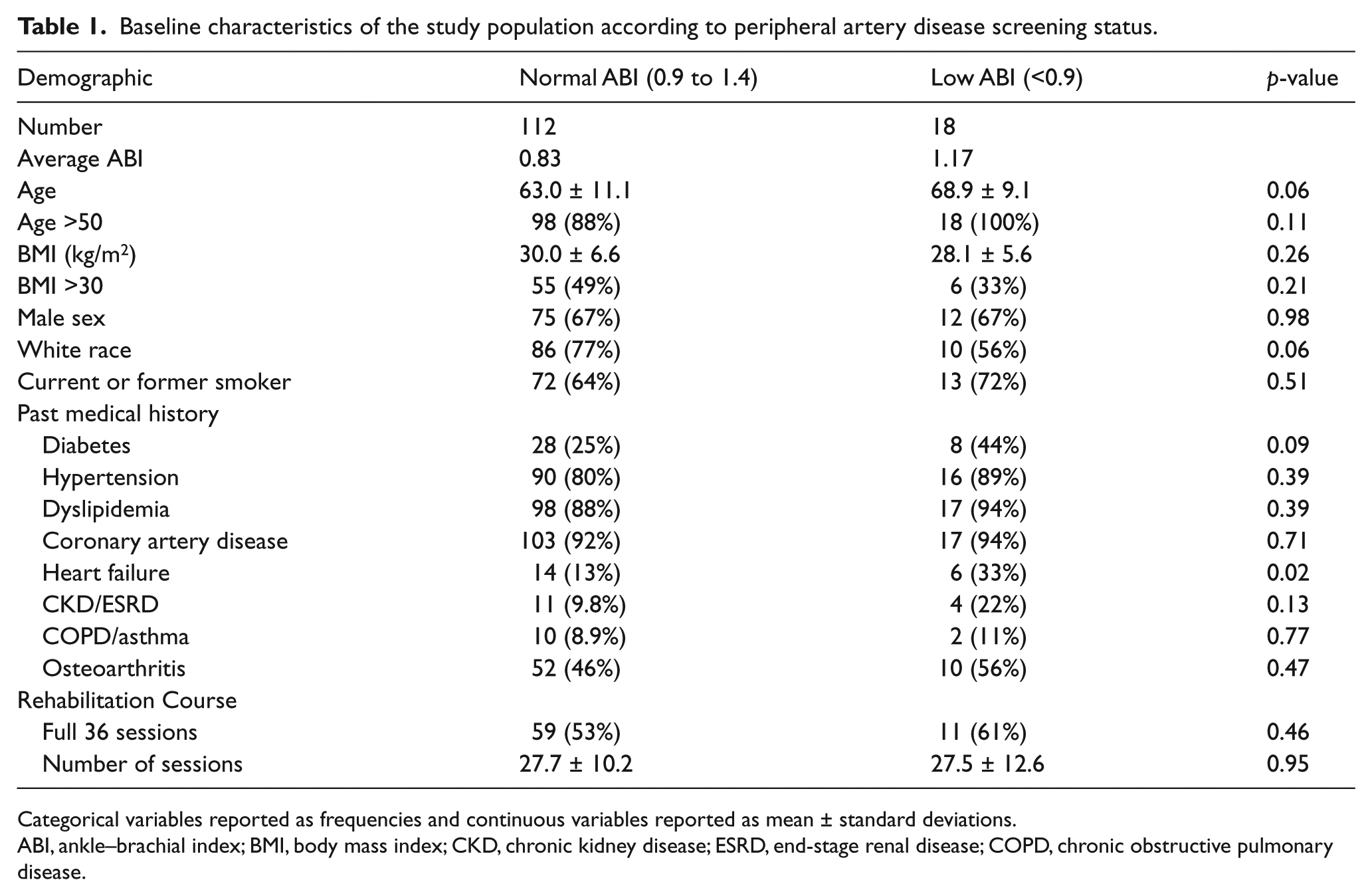
Categorical variables reported as frequencies and continuous variables reported as mean ± standard deviations.
ABI, ankle–brachial index; BMI, body mass index; CKD, chronic kidney disease; ESRD, end-stage renal disease; COPD, chronic obstructive pulmonary disease.
Risk factors
The total number of traditional risk factors for PAD was assessed for each group (Figure 3). These risk factors include the presence of a smoking history, diabetes, obesity (BMI >30), hypertension, dyslipidemia, and advanced age (>50 years). Each of the CR groups displayed a high number of risk factors. There was no statistically significant difference between the average number of risk factors when comparing patients with normal and low ABIs (3.94 vs 4.33, p=0.19).
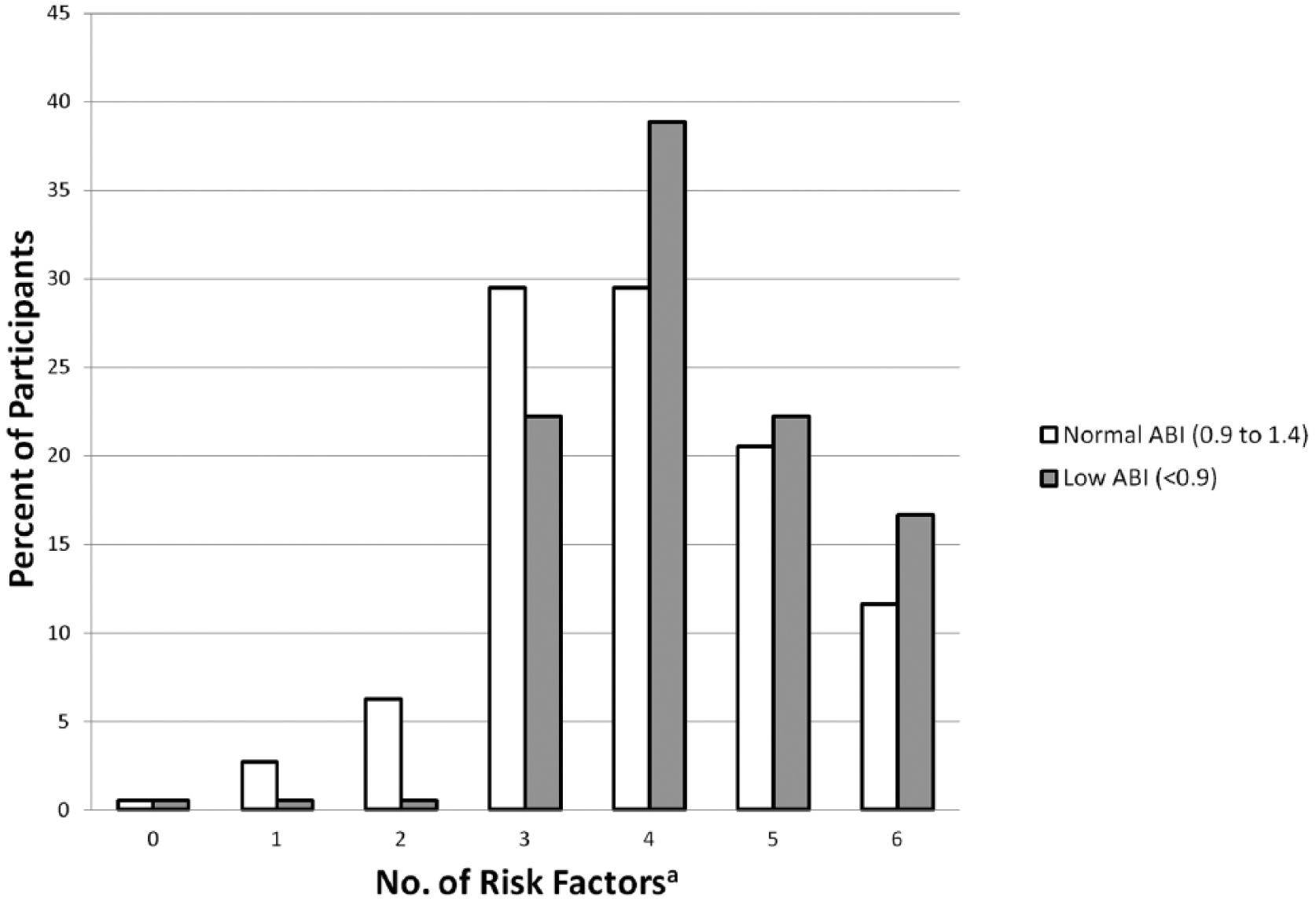
Peripheral artery disease risk factors. aRisk factors include smoking history, diabetes, obesity (body mass index >30), hypertension, dyslipidemia, age >50. (ABI, ankle–brachial index.)
Edinburgh Claudication Questionnaire (ECQ)
Of the 112 patients with normal ABI measurements, 107 had negative questionnaires. Of the 18 patients with a low ABI, only one had a positive ECQ. Based on these findings, the ECQ was specific but not sensitive for the detection of patients with PAD by low ABI (sensitivity 5.6%, specificity 95.5%, PPV 16.7%, NPV 86.3%).
Walking Impairment Questionnaire (WIQ)
Limitations to walking ability as determined by the WIQ were similar between those with normal and low ABIs. Specifically, there with no differences with regard to walking distance (67.0 vs 62.0, p=0.60), speed (45.2 vs 52.0, p=0.28) or symptoms (83.7 vs 87.5, p=0.21).
Modified Gardner Protocol Walk Test
In the treadmill walk test (2 mph or 3.2 kph, 0% grade), seven patients with a normal ABI and three with a low ABI were unable to complete the protocol without needing to stop. Reasons for ending the protocol included dyspnea, general fatigue, or joint pain. There were no reports of typical claudication symptoms ending the test, but four patients in total endorsed some form of leg pain during the walk test. Three had normal ABIs and one had a low ABI. Overall, there was not a difference in the completion rate between the normal and low ABI groups (94% vs 83%, p=0.28).
Outcomes at completion of cardiac rehabilitation
Maximum exercise capacity measured in METs achieved on treadmill exercise was determined for the groups before and after the completion of CR (Figure 4). Upon initiation of CR, the maximum MET level achieved was similar in the normal and low ABI groups (3.38 vs 3.07, p=0.35). At completion of rehabilitation, both groups demonstrated an increase in maximum exercise capacity, but a statistically significant difference in the final MET level was found (5.79 vs 4.47, p=0.009). This accounted for a statistically significant difference in absolute MET improvement (post-rehab MET minus pre-rehab MET) between the groups (+2.41 vs +1.39, p=0.002).
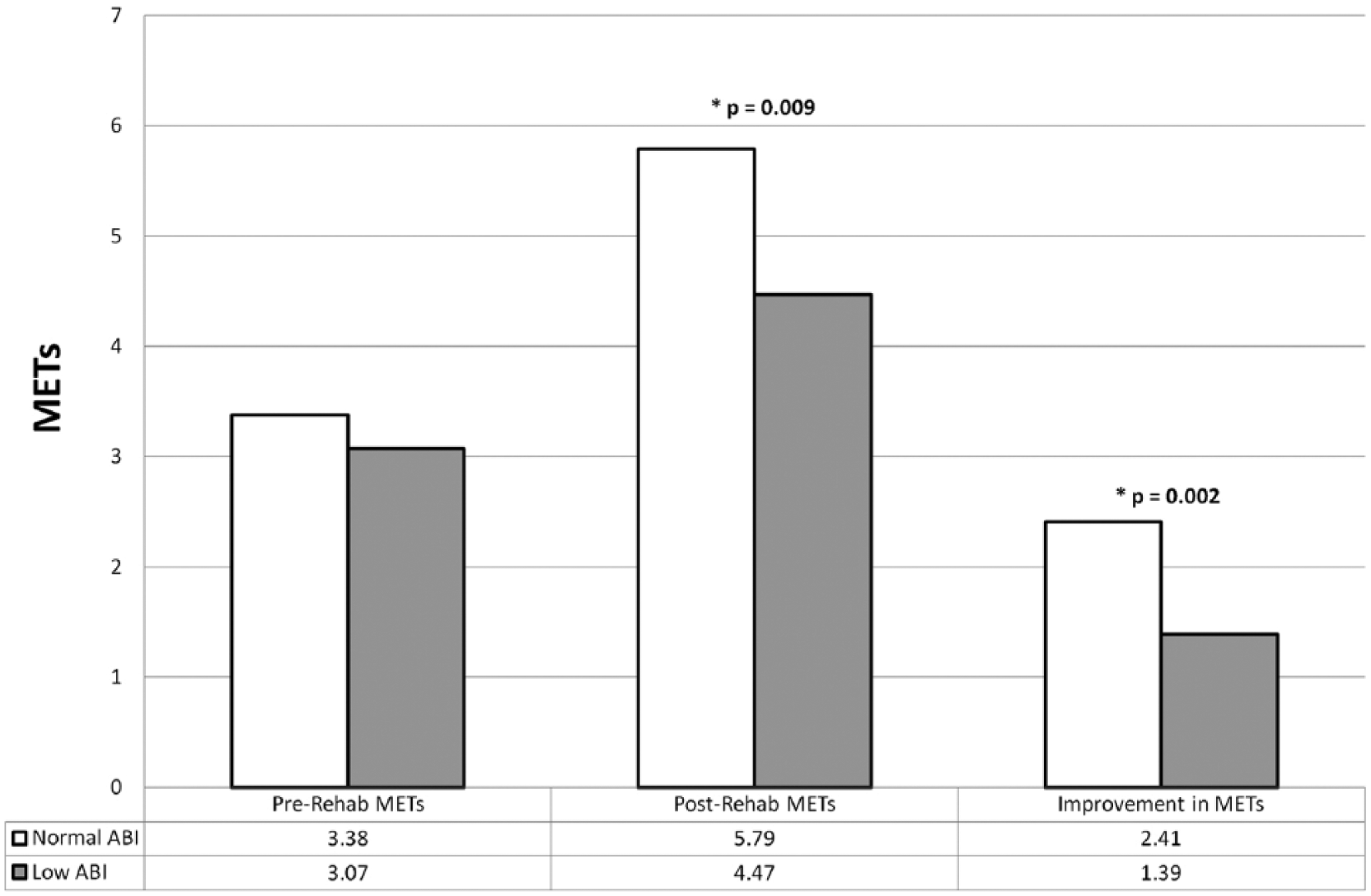
Functional outcomes of cardiac rehabilitation achieved by those with normal ankle–brachial indices compared to those with low indices. Statistical significance was detected between the normal and low ABI groups when comparing post-rehabilitation METs and individual improvement in METs achieved. (ABI, ankle–brachial index; MET, metabolic equivalent.)
Discussion
Screening for occult peripheral artery disease
In accordance with limited prior data, our study confirms the high prevalence of ABI-defined PAD in patients enrolled in CR. This is in contrast to Nelson Worel et al. who found in a smaller sample population (92 patients) a lower prevalence of PAD (4% with ABI <0.9, 12% with ABI >1.3) and recommended against routine ABI screening in the CR population, although they stated it can be considered in patients with diabetes and smoking history. 26 Another study of 231 consecutive CR patients by Spronk et al. recommended screening CR patients for PAD only if they had failed CR, rather than routine screening before CR or no screening. 27 The primary aim of this study, though, was to assess the cost effectiveness of various screening strategies. These data were not collected prospectively and there was a poor overall rate of screening (39/231=17%).
While screening modalities such as the Edinburgh Claudication Questionnaire are useful and have been validated in the general population for use by primary care physicians to detect PAD, 22 they are less sensitive in the CR population. This speaks to the occult nature of PAD in this population as the ECQ is a symptom-based questionnaire for classical claudication. CR patients are also likely to have other functionally limiting comorbid conditions that may mask the presence of typical claudication symptoms. In this study, we have demonstrated, that while identification of PAD by assessing conventional risk factors or validated questionnaires is insensitive at detecting PAD, direct measurement of ABI in patients enrolled in CR predicts rehabilitation potential.
Functional limitations with low level activity
It is interesting to note that patients with and without PAD did not report a significant difference in their walking ability based on the Walking Impairment Questionnaire. This suggests that CR patients with PAD may not perceive a decline in their functional capacity in their daily lives. Again, this may be a reflection of other co-morbid cardiopulmonary conditions masking limitations from PAD in this population. Additionally, when these patients were asked to perform a moderate amount of activity during the Modified Gardner Protocol Walk Test, there was not a significant difference in the completion rate between the normal and low ABI groups. The under-diagnosis of PAD could therefore be attributed to the lack of typical claudication symptoms and lack of significant functional limitation at lower levels of activity. This finding may also explain why clinicians infrequently identify PAD in patients enrolled in CR, underscoring the need to directly measure ABI.
PAD limiting improvement from cardiac rehabilitation
While patients with normal and low ABI measurements had similar treadmill exercise capacities at the beginning of CR, those with a low ABI improved their exercise capacity to a lesser degree than the comparison group. An explanation for this could be that at lower levels of activity there is sufficient blood flow as to not induce symptoms or limit walking ability, but when a more intensive exercise regimen is implemented, oxygen demand in the lower extremities surpasses the threshold of oxygen that the diseased arteries can provide. These differences can also be from patients subconsciously limiting their own activity before symptoms can develop. 7 Regardless, this suggests that patients with lower-extremity PAD with a low ABI are not able to achieve the maximum benefit from their traditional cardiac exercise prescriptions.
The link between functional status achieved in CR and reduction in clinical events and outcomes has been well established.16–21 Our study demonstrates that unrecognized PAD is an important determinant of attenuated exercise capacity, and may therefore contribute to increase cardiovascular events. Exercise and rehabilitation programs do exist specifically for PAD, but these are not identical to a traditional CR regimen. Knowledge of coexistent PAD and cardiac disease may allow for the design of alternative aerobic activities that could better serve this population and enhance performance. Such combined PAD and traditional CR programs may hold the key in treatment of this patient population. Also, future investigation will be needed to explore the potential outcomes benefits of treatment for PAD, whether it is conservative or invasive, in helping patients achieve greater functional improvement from rehabilitation.
Limitations
One of the study limitations is that the ABI is not the only accepted means of diagnosing lower-extremity PAD, but it is certainly a cost-effective and widely utilized screening strategy. For the purposes of this study, other screening and imaging modalities, including exercise ABIs, pulse volume recording, computed tomography angiography, magnetic resonance angiography, and catheter-based angiography, were deemed logistically and financially limiting.
An additional limitation relates to the course of CR itself. Exercise prescriptions were targeted to the patient’s heart disease, rather than PAD per se. The purpose of this strategy was to assess the impact of PAD on a standard course of CR rather than treat the PAD itself. Also, the length of program enrollment was not uniform in this study, with many patients not completing the full 36 exercise sessions. This, however, is not uncommon in the CR population based on a number of personal, logistical and financial reasons. An analysis of Medicare beneficiaries enrolled in Phase II CR by Suaya et al. demonstrated both low enrollment in CR and a highly variable number of sessions attended. 28 Nevertheless, this study is representative of CR practice and our trained staff functions in an American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR) nationally certified program. Overall, this enhances the generalizability of our findings.
A final limitation is that treadmill-derived estimated MET values are only surrogates for exercise capacity and are affected by a variety of factors. However, exercise capacity in our study was estimated from treadmill exercise in accordance with validated, standardized methods. Formal cardiopulmonary exercise testing would have provided more accurate individual measurements of exercise capacity; however, such testing is expensive, particularly if done more than once per patient, and not typical of CR practice. Our large sample size should mitigate the inaccuracies of individual patient measurements and enhance generalizability.
Conclusions
PAD is common in patients in Phase II CR and is often clinically occult. Commonly described PAD risk factors are not a useful screening tool in this population because of their high prevalence, and PAD is seldom detected by standard screening questionnaires in this population. This suggests a need for a broad-based screening strategy with ABI measurements. Importantly, while patients with a low ABI and PAD do not appear to have impairment at lower levels of activity, this study indicates they have significantly reduced improvements in exercise capacity at completion of CR. Given prior evidence correlating positive changes in exercise capacity achieved in CR to reductions in cardiovascular events, the attenuated response seen in patients with undiagnosed PAD has significant potential health implications.
Footnotes
Acknowledgements
We would like to give special thanks to the staff and patients of University Hospitals Harrington Heart & Vascular Institute Cardiopulmonary Rehabilitation Program.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.