
Abstract
Inadequate nutrient intake may contribute to the development and progression of peripheral arterial disease (PAD). This study’s aim was to assess intake of essential fatty acids and nutrients among veterans with PAD. All 88 subjects had ankle–brachial indices of <0.9 and claudication. A validated food frequency questionnaire evaluated dietary intake, and values were compared to guidelines established by the American Heart Association (AHA) and American College of Cardiology (ACC), as well as the AHA/ACC endorsed Dietary Approaches to Stop Hypertension (DASH) eating plan. The mean age was 69 ± 8 years. Compared to the AHA/ACC guidelines, subjects with PAD had an inadequate intake of long-chain polyunsaturated fatty acids (n-3 PUFA; 59% consumed >1 gram daily). Our subjects with PAD had an increased intake of cholesterol (31% met the cut-off established in the DASH plan), total fat (5%) and sodium (53%). They had an inadequate intake of magnesium (3%), calcium (5%), and soluble fiber (3%). Dietary potassium intake met the recommended guidelines. In our subjects with PAD, intake of critical nutrients deviated substantially from the recommended amounts. Further prospective studies should evaluate whether PAD patients experience clinical benefit if diets are modified to meet the AHA/ACC recommendations.
Introduction
Peripheral arterial disease (PAD) is a chronic inflammatory condition of the vasculature that continues to be associated with a higher risk of cardiovascular events compared to coronary artery disease, despite the availability of the US Food and Drug Administration (FDA)-approved medical therapies. 1 In addition to traditional risk factors, such as diabetes mellitus, smoking, hyperlipidemia and hypertension, a growing body of evidence suggests that inadequate nutrient intake and excessive caloric intake may spur the development of PAD.2–5 In particular, lower blood levels of omega-3 polyunsaturated fatty acids (n-3 PUFA), which are essential to our diet, may be related to the onset or progression of PAD. 6
Prior studies have surveyed nutritional intake and average dietary patterns among patients with PAD.3,6–8 Previous investigators showed that diagnosis of PAD and the presence of claudication correlate with a diet high in saturated fat, sodium, and cholesterol, and low in fiber, vitamin E, folate intake and lower levels of n-3 PUFA. The purpose of the current analysis was to assess the intake of n-3 PUFA and other essential nutrients, including fats, fiber, minerals and electrolytes in a contemporary group of patients with PAD. We hypothesized that relative to daily recommendations from the American Heart Association (AHA) and American College of Cardiology (ACC), our subjects would report a reduced intake of n-3 PUFA, dietary fiber, and vitamins and an excessive intake of sodium, saturated fat, and cholesterol.
Methods
Study population and protocol
This study utilized baseline data from a prospective trial investigating the effects of n-3 PUFA supplementation on inflammatory markers and vascular function in PAD patients (the OMEGA-PAD I trial).9,10 The investigator-initiated protocol was approved by the Committee on Human Research at the University of California, San Francisco (UCSF), and all patients provided informed consent. Patients referred to the outpatient vascular surgery clinic of the San Francisco Veterans Affairs Medical Center (SF VAMC) for evaluation of symptomatic PAD were screened for the study.
PAD diagnosis was based on current guidelines of having an ankle–brachial index (ABI) <0.9 on the affected limb(s) at presentation, with the presence of claudication. 11 We excluded patients with incompressible arteries or an ABI >1.4. Claudication was diagnosed based on fatigue, discomfort, or pain that occurs in specific limb muscle groups during effort due to exercise-induced ischemia. 12 The study exclusion criteria included: significant renal, hepatic, or inflammatory disease; concurrent severe infections; acute illness or other major surgery within 30 days of evaluation or ingestion of immunosuppressive medications. Those meeting the inclusion criteria were invited to enter the research study, at which time informed consent was obtained by study staff in accordance with the requirements of the Committee for Human Research. Data on demographics (age, race, and gender), anthropometrics (hip and waist circumference, body mass index), lifestyle (prior supplement use, walking duration, and cigarette smoking), cardiovascular disease history (e.g. coronary artery disease), cardiovascular risk factors (hypertension, diabetes, hypercholesterolemia, cigarette smoking and renal insufficiency), medications, and pertinent vascular examination findings were recorded. Circulating biomarkers were also measured, including the inflammatory marker C-reactive protein (CRP), lipid panel (low-density lipoprotein (LDL)-cholesterol (C), triglycerides, high-density lipoprotein (HDL)-C), blood pressure, and bilateral ABI. A validated food frequency questionnaire (2005 Block Food Frequency Questionnaire) was also administered to estimate dietary intake. 13
Blood analysis
Inflammatory marker: High-sensitivity C-reactive protein
To measure CRP, whole venous blood was collected in a fasting state in an SSTP tube, allowed to clot for a minimum of 30 minutes at room temperature, and centrifuged at 2800 rpm for 10 minutes at 4°C. Plasma obtained from the EDTA tubes described above was assayed for CRP the same day as collection by the SF VAMC lab per standard methodology (Beckman Coulter Analyzer; Miami, FL, USA). The coefficient of variation for CRP using this procedure is 5.1%.
Renal, lipid and metabolic measurements
EDTA blood samples were collected in a fasting state for measurement of creatinine (Cr), estimated glomerular filtration rate (eGFR), albumin, total cholesterol, triglycerides, LDL, and HDL. Plasma was assayed for these analytes on the same day as collection by the SF VAMC lab per standard methodology (Beckman Coulter Analyzer). Serum was isolated at the same time points as described above and assayed for homocysteine on the same day as collection by the SF VAMC lab per standard methodology (Abbott Diagnostics Architect i1000 Analyzer; Lake Forest, IL, USA).
Ankle–brachial index
The ABI was measured using current guidelines and standards. 11 ABI measurements were collected by trained vascular clinical staff of the Vascular Integrated Physiology and Experimental Therapeutics Laboratory (VIPERx Lab at www.viperxlab.org). Systolic blood pressures of the brachial, posterior tibial and dorsalis pedis arteries were measured bilaterally. For each lower extremity, the highest systolic pressure of the two pedal pulses was divided by the highest systolic pressure of the two brachial arteries.
Food frequency questionnaire
A validated questionnaire (2005 Block Food Frequency Questionnaire13,14) was used to estimate each subject’s average intake of a variety of foods. Every participant was asked to complete a food frequency questionnaire once at the initial visit. The questionnaire provides a list of foods and beverages, along with an explanation and images of measured portion sizes and a frequency response section, where respondents answer how often they consumed each item during a given time period. The validated FFQ prompted responders to supply basic demographic information (age, gender, height and weight) and to estimate their average frequency of intake of approximately 110 food items, with frequency options including ‘daily’, ‘5–6 times per week’, ‘3–4 times per week’, ‘1–2 times per week’, ‘weekly’, ‘monthly’, and ‘never’. They completed Scantron forms ordered from Nutritionquest®, the questionnaire distributor. The questionnaires were mailed to Nutritionquest for quantitative analysis. Calculations for nutrient intake were subsequently made using computerized software programs which multiply the reported frequency of each food item by the nutrient amount in each serving of that food. The software draws upon reference databases (primarily the National Health and Nutrition Examination Survey (NHANES)) to factor in differences in energy intake for various subgroups of adults in the United States (e.g. white individuals, black individuals, and Mexican Americans, and for men and women). The nutrient data were summarized in a computerized spreadsheet that was returned to our group for further statistical analysis.
Statistical analysis
Demographic and basic laboratory data for the patients were averaged, and the continuous variables are presented with a standard deviation while categorical variables are presented with proportionality estimates (%) (Table 1). Patient-reported data on the 2005 Block Food Frequency Questionnaire were compiled and the aggregate average for each nutrient group was tabulated. Table 2 summarizes our subjects’ nutritional intake, represented as proportions (%) relative to national guideline recommendations on intake for each nutrient. The comparison values listed in Table 2 were derived from the DASH (Dietary Approaches to Stop Hypertension) diet plan recommendations. The DASH plan is among the dietary patterns endorsed by the AHA/ACC Task Force and is the only one providing the highest quality evidence that it leads to improvements in blood pressure and lipid profiles. Adherence to the DASH plan, or similar dietary patterns, has been strongly correlated with a reduced risk of cardiovascular diseases, including PAD.15,16 The only nutrient included in our analysis that was not explicitly addressed in the DASH diet plan was n-3 PUFA. The cut-off value of 1 gram daily intake was obtained directly from the AHA/ACC recommendations. 17 Statistical analyses were performed using Stata/SE 13 (StataCorp, College Station, TX, USA).
Baseline characteristics of participants with PAD (n=88).
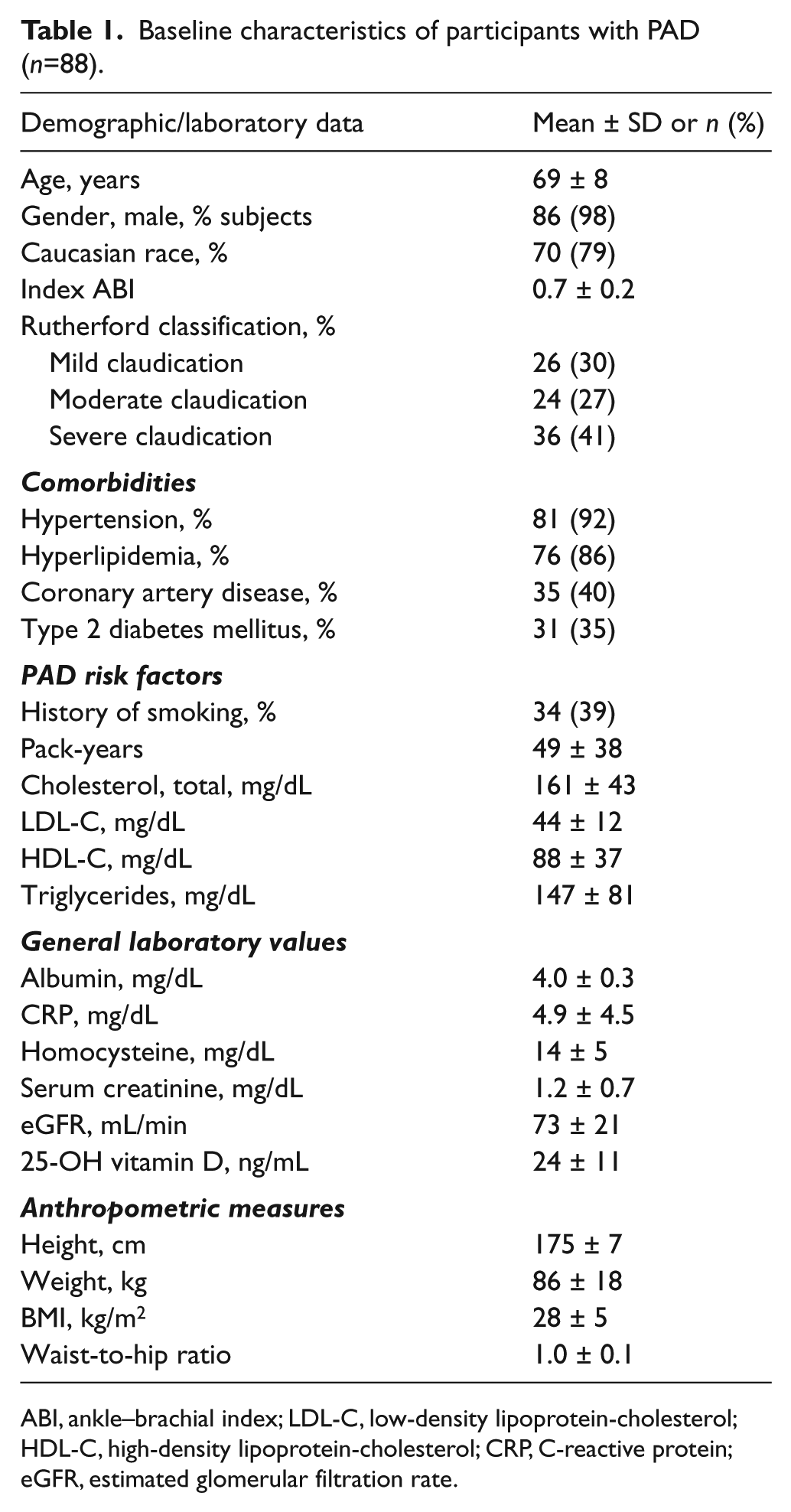
ABI, ankle–brachial index; LDL-C, low-density lipoprotein-cholesterol; HDL-C, high-density lipoprotein-cholesterol; CRP, C-reactive protein; eGFR, estimated glomerular filtration rate.
Proportion of nutrient intake among participants with PAD as compared to daily dietary recommendations from AHA/ACC.
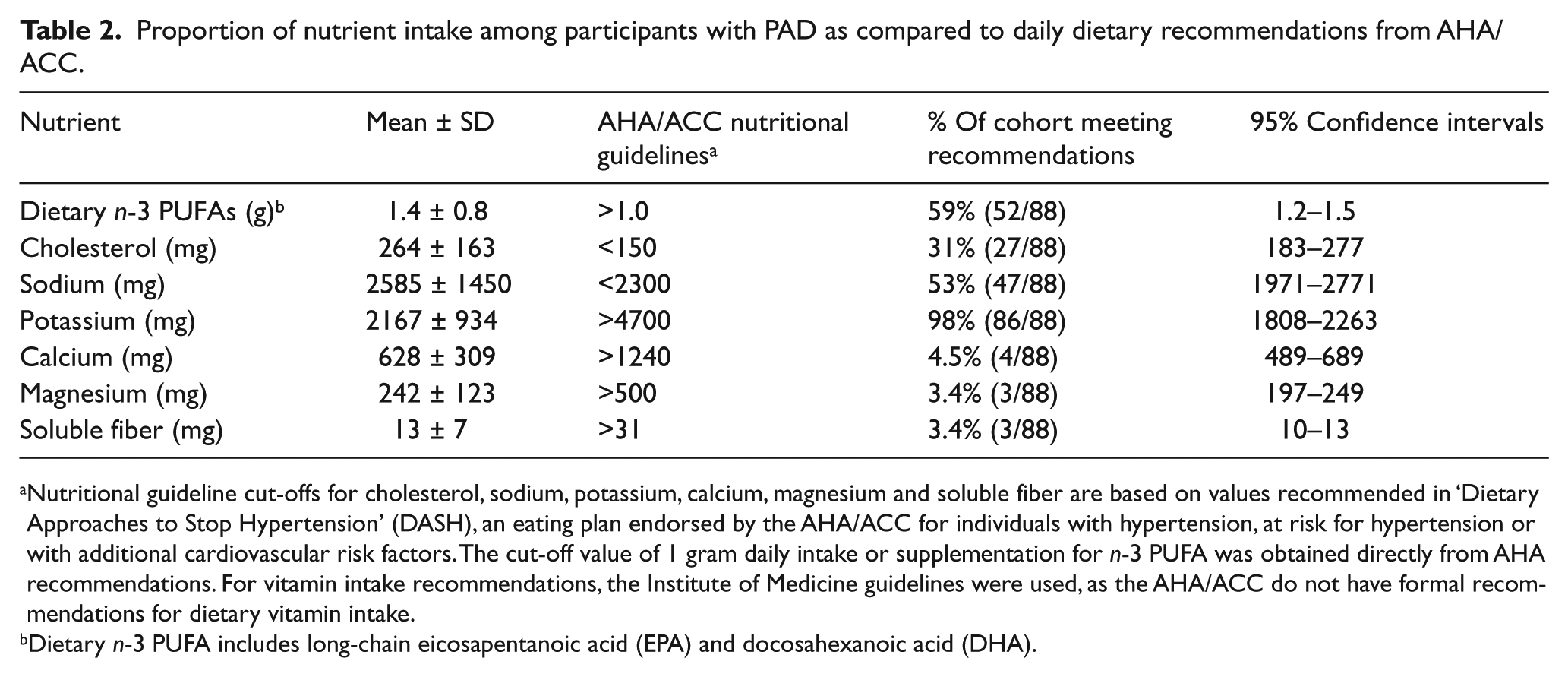
Nutritional guideline cut-offs for cholesterol, sodium, potassium, calcium, magnesium and soluble fiber are based on values recommended in ‘Dietary Approaches to Stop Hypertension’ (DASH), an eating plan endorsed by the AHA/ACC for individuals with hypertension, at risk for hypertension or with additional cardiovascular risk factors. The cut-off value of 1 gram daily intake or supplementation for n-3 PUFA was obtained directly from AHA recommendations. For vitamin intake recommendations, the Institute of Medicine guidelines were used, as the AHA/ACC do not have formal recommendations for dietary vitamin intake.
Dietary n-3 PUFA includes long-chain eicosapentanoic acid (EPA) and docosahexanoic acid (DHA).
Results
A total of 88 patients with PAD were recruited for the study, and all reported lifestyle-limiting lower-extremity claudication. The characteristics of the population and laboratory studies are summarized in Table 1. The mean age of the patients was 69 ± 8 years, 40% had coronary artery disease, 35% had type 2 diabetes mellitus and 86% had hyperlipidemia.
Table 2 details the average individual’s nutritional intake in relation to daily dietary recommendations from the AHA/ACC. Only 59% of our veteran subjects with established PAD consumed the daily-recommended amount for n-3 PUFA for people with diagnosed cardiovascular disease (⩽1 gram). Twenty-five individuals (28%) reported taking daily n-3 PUFA as supplements, though no one reported a daily supplementation greater than 0.5 grams, which is half of the AHA/ACC recommendation. 18 Our subjects had elevated intake levels of cholesterol (only 31% of the patients met the AHA/ACC cut-off, as suggested by the DASH diet plan recommendations) and sodium (53% met the DASH cut-off), and 95% had a total fat intake that exceeded the suggested amount (27% maximum of total daily calories is recommended according to the DASH diet plan). There was inadequate intake of magnesium, calcium and soluble fiber (only 3%, 5%, and 3%, respectively, met the DASH cut-offs). 18 Dietary potassium intake appeared to meet the recommended cut-off level proposed in the DASH eating plan and endorsed in the AHA/ACC guidelines.
We further stratified nutritional intake if patients carried a diagnosis of type 2 diabetes mellitus (Table 3) and by their degree of walking impairment (Table 4). Our aim was to evaluate whether a comorbid and strong cardiovascular risk factor (DM) or severity of PAD (according to Rutherford grade) affected dietary intake. No differences in nutritional intake patterns were observed among these groups.
Comparison of nutrient intake among participants with type 2 diabetes mellitus (T2DM) and those without DM.
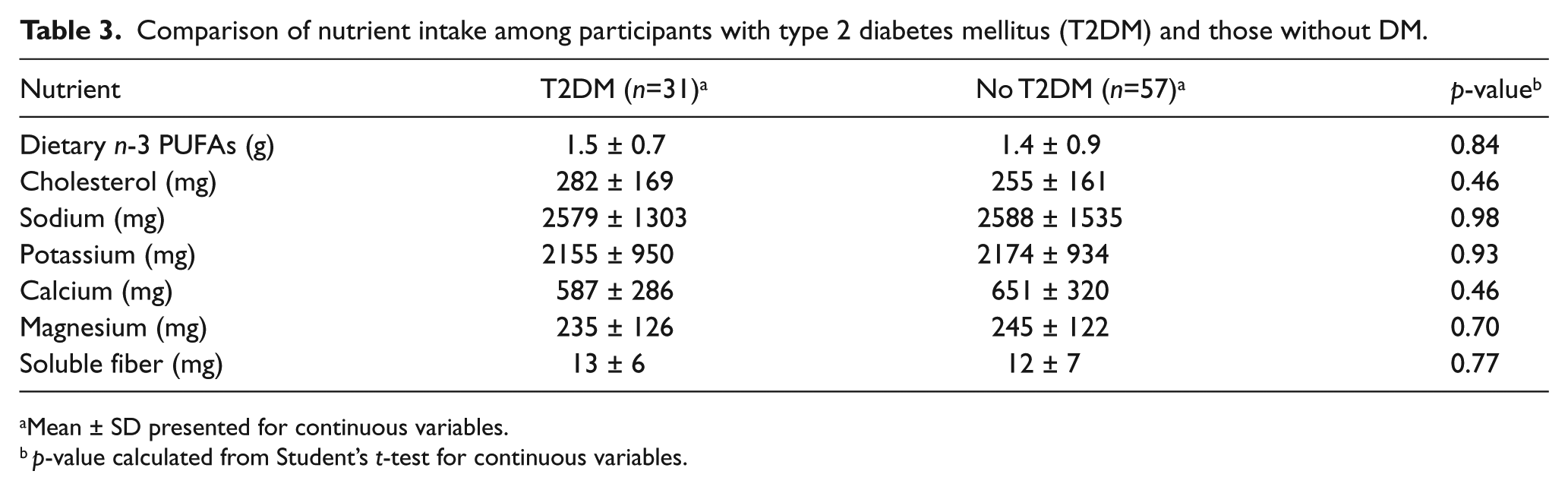
Mean ± SD presented for continuous variables.
p-value calculated from Student’s t-test for continuous variables.
Comparison of nutrient intake among participants by Rutherford grade.
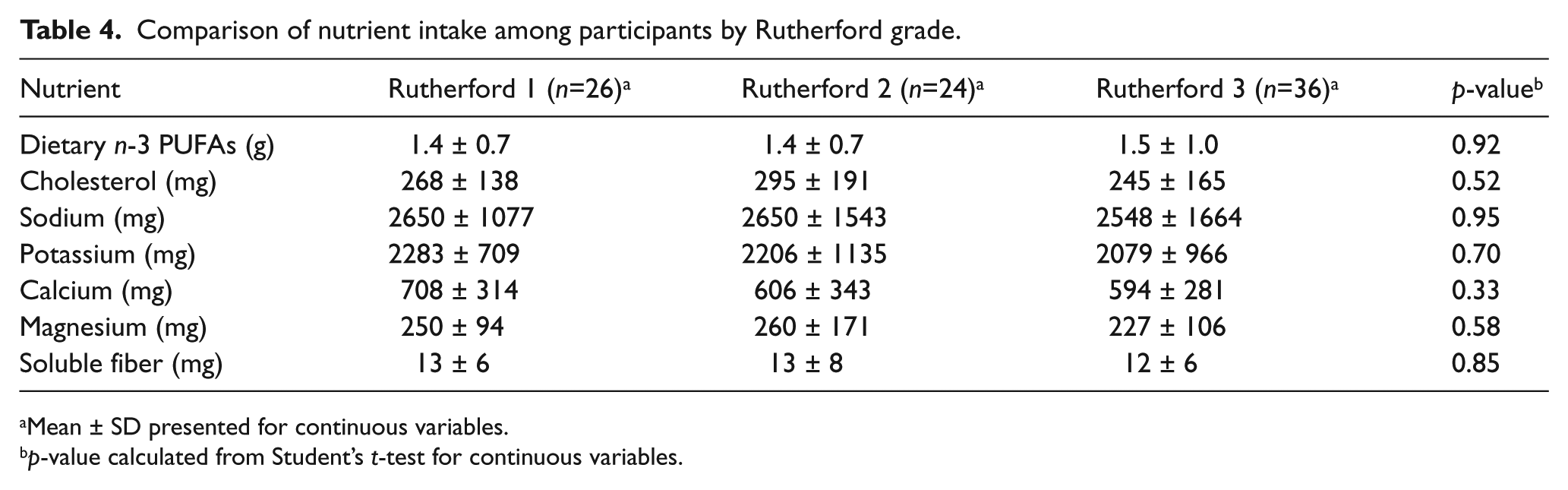
Mean ± SD presented for continuous variables.
p-value calculated from Student’s t-test for continuous variables.
Discussion
In a prospective study of patients presenting for evaluation of PAD in an outpatient vascular surgery clinic, we found that relative to the recently revised guidelines proposed by the AHA/ACC in 2013, 17 patients reported a lower than recommended intake of n-3 PUFA, dietary fiber, calcium, and magnesium and an excess intake of total fat, cholesterol and sodium. This manuscript summarizes our PAD patients’ nutrient intake based on reported data.
Current AHA/ACC dietary recommendations
The AHA/ACC Task Force recently published their updated guidelines on Lifestyle Management to Reduce Cardiovascular Risk, 17 in which they detail evidence-based recommendations for ‘heart-healthy nutrition’, blood pressure and lipid control, and physical activity. In regards to nutrition, the committee provided broad guidance, stating that individuals should ‘consume a dietary pattern that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, non-tropical vegetable oils and nuts; and limits intake of sodium, sweets, sugar, sweetened beverages and red meats’. Developed in the 1990s and endorsed by the AHA, ACC, National Heart, Lung, and Blood Institute and the US Department of Agriculture, the DASH plan emphasizes a diet high in fruits, vegetables, whole grains, fish, poultry, nuts and seeds, and low-fat dairy products. It also minimizes consumption of red meats, artificially sweetened desserts, and sugar-sweetened beverages. As a result, the diet plan is high in protein, fiber, potassium, calcium, and magnesium and low in cholesterol, overall fat, and saturated fat. According to the task force, the DASH plan provides the highest quality evidence for a diet pattern leading to improvements in blood pressure and lipid profiles. 17
PAD and n-3 long-chain polyunsaturated fatty acids
Long chain n-3 PUFAs, especially from marine sources, are among the nutrients that have been shown to reduce systemic inflammation 19 and protect against endothelial damage and atherosclerosis. 20 For secondary prevention among individuals with diagnosed cardiovascular disease, the AHA/ACC guidelines suggest that those who do not regularly eat fish may consider taking fish oil supplements that contain 1 gram of eicosapentanoic (EPA) and docosahexanoic (DHA) acids, based on supplementation studies in these patients.17,18 This recommendation should be applied to 100% of our patients since they suffer from PAD.
In a recent meta-analysis 21 that aggregated data to evaluate the long-term effects of n-3 PUFA for primary prevention, investigators found that prolonged supplementation (at least 1 year) with a minimum 1 gram/day EPA + DHA was protective against death from cardiac causes, sudden death and myocardial infarction. Specific to PAD, results from one prospective trial suggest that intake of n-3 PUFA may be associated with a reduced risk of developing the disease. In their analysis of the PREDIMED trial, 22 Ruiz-Canela and colleagues found that two variations of the Mediterranean diet (one supplemented with extra virgin olive oil and the other with nuts) were both associated with a significantly lower incidence of PAD compared to a control diet. Among individuals with diagnosed PAD, a prospective study by Schiano et al. 23 found that supplementing claudicants with 2 grams daily of n-3 PUFA for 12 weeks led to an improvement in endothelial function relative to the non-supplemented control group, hinting at a possible slower progression. Most other supplementation studies have also evaluated effects at daily dosages greater than 1 gram,19,24,25 suggesting that greater amounts of n-3 PUFA are optimal for achieving clinical benefits. Only 59% of our PAD subjects met the 1-gram cut-off, the minimum suggested daily intake. This low proportion raises such questions as whether increased intake earlier in life may affect disease onset or whether increased n-3 PUFA intake may have favorable effects on disease progression or outcomes.
It has been shown that n-3 PUFA, and primarily EPA + DHA, contributes to primary and secondary cardiovascular disease protection by increasing nitric oxide production, promoting endothelial relaxation and vascular compliance, decreasing production of inflammatory cytokines and mediators, reducing blood triglyceride concentration, lowering blood pressure, and decreasing thrombosis and cardiac arrhythmias.26,27 Increased consumption of n-3 PUFA has been shown to lead to a relative reduction in inflammatory signals and monocyte adhesion in the endothelial cells compared to n-6 PUFA, such as arachidonic acid. 28 In addition to their direct influences on inflammation and endothelial function, n-3 PUFA yield derivatives, namely protectins, lipoxins, resolvins, and maresins, 29 which have potent homeostatic effects. These lipid mediators help to activate endogenous pathways to terminate and promote the resolution of the inflammation process.27,30 The impact of n-3 PUFA on the resolution of inflammation may eventually prove to be beneficial for patients with PAD, who have a high inflammatory burden.
PAD and nutrient intake beyond n-3 PUFA
Findings from our current analysis confirm associations about poor dietary habits and PAD observed in other settings.31–34 Antonelli-Incalzi et al. 6 demonstrated that PAD was associated with a lower consumption of vegetables, fiber, vitamins C and E, folate and long-chain PUFA as compared to individuals without PAD. In another study by Gardner and colleagues, 7 similar patterns were evident: the presence of claudication was associated with a diet high in saturated fat, sodium, and cholesterol and low in fiber, vitamin E, and folate intake. In their study, a higher intake of monounsaturated fats correlated with lower peak walking times. Larger analyses utilizing population-based data have also been conducted. In their study using NHANES data, Lane et al. 3 evaluated 442 subjects with PAD. They found that consumption of vitamins A, C, E, B6, and B12 correlated with lower odds of having PAD. Intake of fiber, vitamins A, C, E, B6, folate, and n-3 PUFA was also related to a reduced prevalence of PAD. Most recently, in their study of nutrient intake among 6500 adult participants from the NHANES, Naqvi et al. 8 found inverse associations between the incidence of PAD and intake of folate and vitamins A, B6, C, and E, affirming the results observed by Lane et al. and the smaller cross-sectional studies described above.
Sodium
High sodium intake has long been implicated as a direct contributor to hypertension, itself a strong cardiovascular disease risk factor. 35 In fact, salt has a stronger association than any other dietary component with increased blood pressure and atherosclerosis, as well as stroke and heart failure. 35 Previous studies have shown that the average salt intake among patients with PAD is more than two-times that of national guideline recommendations and that rates of hypertension are significantly greater in PAD when compared to those without PAD.6,7 In terms of primary prevention, there are now several studies that demonstrate that reducing salt consumption is the most efficient and cost-effective method to curb cardiovascular disease on a population scale.36–38 Notably, Smith-Spangler and colleagues 37 created a model to evaluate to what extent cardiovascular disease rates in the United States adult population could be affected by a nearly 10% reduction in salt intake. They found that approximately 480,000 myocardial infarctions over the lifetime of adults ranging from 40 to 85 years could be avoided, parallel to a $32.1 billion saving in medical costs. Bibbins-Domingo et al. 36 had similar findings: their model construct showed that decreasing dietary salt intake by up to 3 grams each day could reduce the annual incidence of coronary artery disease by 60,000 and myocardial infarction by 45,000, and the annual number of deaths could be decreased by 46,000. These findings suggest that recommending substantial reductions in salt intake could be a useful measure for cardiovascular disease prevention in the general population and may be especially effective in decreasing event rates among patients with PAD.
Fiber
Increased dietary fiber has been linked to a decreased risk in cardiovascular disease and fewer cardiovascular events.39,40 In a meta-analysis of 67 controlled supplementation trials, daily consumption of 2–10 grams of soluble fiber (found mainly in oat bran and legumes) lowered LDL-C and had no significant effects on HDL-C or triglycerides. 18 Specific to PAD cohorts, a deficiency in dietary fiber has been reported in patients with claudication.3,8 However, prospective studies have failed to show that supplementation with dietary fiber improves inflammation levels or cardiovascular outcomes in PAD. 17 In light of these findings, the AHA and National Cholesterol Education Program (ATP III) guidelines recommend increasing dietary soluble fiber intake to protect against cardiovascular disease.
Future implications
PAD is a chronic inflammatory condition that is associated with longstanding poor nutrition habits. Our study demonstrates that the majority of veterans with PAD do not meet AHA/ACC nutritional guidelines for a healthy diet. Future studies are needed to understand whether PAD patients may experience clinical benefits from improved dietary habits including regular intake of fish or daily fish oil supplements, increased dietary soluble fiber intake, consumption of adequate amounts of electrolytes, vitamins, and minerals, as well as reduced saturated fat and sodium intake.
Limitations
This cross-sectional study was observational and included a small sample size. The patient population studied was not representative of the broader PAD population as it included predominantly male Caucasian veterans from SF VAMC. Gender could not be controlled for due to the two females included in the analysis. In addition, our study did not include patients with asymptomatic or premature PAD, or any individuals with more advanced stages of the disease (e.g. those with renal and/or hepatic failure). Lastly, this study lacked validation of patient-reported dietary intake on the food frequency questionnaire (e.g. through measurement of blood levels of specific nutrients).
Conclusion
In a sampling of patients with PAD, we observed that dietary intake of several critical nutrients, particularly n-3 PUFA, deviated substantially from the amounts recommended by national nutrition guidelines. Achieving a better understanding of overall diet patterns in PAD, as we have attempted in this analysis, may facilitate the design and execution of prospective and randomized trials with clinical outcomes such as major adverse cardiovascular events and limb-related endpoints (e.g. claudication distance, limb revascularization, amputation).
Footnotes
Acknowledgements
We thank the Clinical Research Center of the San Francisco Veterans Affairs Medical Center for their invaluable help with this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The present work was supported by grants from the National Institutes of Health and the Society for Vascular Surgery Foundation, as well as by start-up funds from the University of California, San Francisco and the Northern California Institute for Research and Education, by a Clinical Seed Grant from the Society for Vascular Surgery and by Award Number KL2RR024130 from the National Center for Research Resources. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health. The funding organizations were not involved in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.