
Abstract
The Peripheral Artery Questionnaire (PAQ), as developed in US English, is a validated scale to evaluate the health status of patients with peripheral artery disease (PAD). The aim of this study was to translate the PAQ into Korean and to evaluate its reliability and validity. A multi-step process of forward-translation, reconciliation, consultation with the developer, back-translation and proofreading was conducted. The test–retest reliability was evaluated at a 2-week interval using the intra-class correlation coefficient (ICC). The validity was assessed by identifying associations between Korean PAQ (KPAQ) scores and Korean Health Assessment Questionnaire (KHAQ) scores. A total of 100 PAD patients were enrolled: 63 without and 37 with severe claudication. The reliability of the KPAQ was adequate, with an ICC of 0.71. There were strong correlations between KPAQ’s subscales. Cronbach’s alpha for the summary score was 0.94, indicating good internal consistency and congruence with the original US version. The validity was supported by a significant correlation between the total KHAQ score and KPAQ physical function, stability, symptom, social limitation and quality of life scores (r = -0.24 to -0.90; p < 0.001) as well as between the KHAQ walking subscale and the KPAQ physical function score (r = −0.55, p < 0.001). Our results indicate that the KPAQ is a reliable, valid instrument to evaluate the health status of Korean patients with PAD.
Introduction
Peripheral artery disease (PAD) results from luminal narrowing and stiffening of the arteries supplying the lower limbs, most often due to systemic atherosclerotic disease. Its prevalence is high, and is associated with a high risk for fatal and non-fatal cardiovascular events (death, myocardial infarction and cerebral vascular accident). 1 Accordingly, guidelines and performance measures have been developed for PAD to support aggressive treatment of its risk factors, including hypertension and hyperlipidemia. Diagnosing PAD is very important, as the incidence of acute cardiovascular events is two to three times higher in patients with PAD as compared with people having no atherosclerosis of their peripheral arteries.2,3 Despite its prevalence and cardiovascular risk implications, only 25% of PAD patients are recognized and treated. 4
Although the majority of PAD patients are asymptomatic, the disease often progresses to cause symptoms that can impact patients’ functioning and quality of life. Intermittent claudication is the cardinal symptom of PAD and is a primary treatment target for afflicted patients. It occurs as a result of reduced blood flow to lower extremity skeletal muscle during exercise. The incidence of symptomatic PAD increases with age, affecting 22% of patients with PAD, and the cardiovascular risk factors mentioned contribute to the progression of PAD. 5 Because whether symptoms develop or not depends largely on an individual’s level of activity, patients suspected of having PAD should be questioned about any limitations they experience during exercise of the lower extremities that limits their walking ability. 5 In order to monitor patients’ symptoms in a reliable way, sensitive disease-specific instruments have been developed. A diagnostic questionnaire for PAD, such as the Edinburgh Claudication Questionnaire (ECQ), has been validated to diagnose intermittent claudication in epidemiological surveys of PAD, 6 but is not sensitive to changes over time and does not independently capture the range of clinical manifestations from patients’ perspectives. To better monitor the impact of PAD, from patients’ perspectives, as an endpoint in clinical trials and in daily clinical practice, a more comprehensive disease-specific instrument is needed.
When it comes to the evaluation of medical therapy and existing revascularization procedures, quantifying PAD patients’ health status becomes a particularly important issue, as the primary goal of revascularization procedures in PAD is to improve patients’ symptoms, function and quality of life. 7 Recently, marked methodological improvements in the measurement of PAD patients’ health status (their symptoms, function and quality of life) have been made. The psychometrically sound Peripheral Artery Questionnaire (PAQ), a disease-specific measure, was developed for this purpose in the US population. 8 This instrument has proved to be useful to quantify improvement in health status after peripheral endovascular revascularization. 9 Although the PAQ is available in an original English and validated Dutch language version, 10 and its dimensions were created to represent a clinical framework for quantifying patients’ health status, no empiric data supporting a patient-centered framework of the data have been published. In order to support the wider use of the PAQ, and to facilitate comparisons of PAD care and outcomes across different healthcare systems, we translated and validated a Korean version of the PAQ in Korean PAD patients. Its validity and reliability were examined and its convergent validity was tested against the Korean Health Assessment Questionnaire (KHAQ), a standardized and widely used health outcome instrument.11,12
Methods
Participants and selection criteria
One hundred Korean patients who agreed to take part in the study were enrolled from the Cardiologic and Rheumatologic Clinic of Maryknoll Hospital. Participants eligible for the study were those who were suspected of having PAD on the basis of an ABI < 0.9, poor pulses bilaterally or substantially weaker pulses on either side in the case of the popliteal artery or dorsalis pedis artery, and/or clinical symptoms of PAD. The study protocol was approved by the ethics review board and informed consent was obtained from each participant.
Questionnaires administered
The Peripheral Artery Questionnaire (PAQ)
The PAQ is a self-administered, 20-item health status measure for patients with PAD. Each question asks about symptoms attributable to PAD over the previous 4 weeks. Scores are available for six domains: symptoms, symptom stability (change in symptoms), physical limitation, treatment satisfaction, social functioning, and quality of life. A summary score is calculated as the average of the physical limitation, symptoms, quality of life, and social functioning scores. Scores range from 0 to 100; higher scores indicate less functional limitation, fewer symptoms, better treatment satisfaction, higher social functioning, and better quality of life. A symptom stability score of 50 represents no change over the preceding 4 weeks, whereas scores > 50 or < 50 represent recent improvement or worsening of symptoms, respectively.
The Edinburgh Claudication Questionnaire (ECQ)
The ECQ was developed to diagnose intermittent claudication in epidemiological research. It assesses whether patients develop pain in their calf, either with walking or at rest, while walking at an ordinary or hurried pace, or when walking uphill. 6 Using the ECQ, we classified patients as having claudication (‘yes’ versus ‘no’) and, for those with the symptom, the severity was classified as ‘severe’ when the symptom occurred as patients walked at an ordinary pace on the level and ‘not severe’ when the pain occurred only as patients walked uphill or in a hurry.
Health Assessment Questionnaire (HAQ)
Patient-reported assessments of current functional limitations were collected with the HAQ. 11 The HAQ is a self-administered disability instrument developed for patients with different rheumatic diseases. The patient indicates the level of difficulty for performing each activity and at least six values are summed and divided by the number of values. We used six domains (dressing, getting in and out of bed, bending down to pick up clothing from the floor, walking outdoors, washing and drying the entire body, getting in and out of a car) and did not use two domains (lifting a full cup or glass, turning regular faucets on and off). The HAQ has been translated into numerous languages, including a valid and reliable Korean language version. 12
Translation methodology
Permission for translation and acquisition of the original version of PAQ was obtained directly from the developer (John Spertus), who offered to assist in resolving any potential concerns related to the conceptual framework of the instrument.
The PAQ was then translated independently into Korean by three translators who were fluent in both Korean and English (versions 1.0a, 1.0b, and 1.0c). The three translators then reviewed each version (1.0a, 1.0b, and 1.0c) and produced a reconciled Korean version (Korean version 1.1) after two meetings. Korean version 1.1 was then back-translated by three translators who were born in the United States and were fluent in both languages. After the original and back-translated versions were compared, the developer was sent the discordant item concepts for clarification of the original conceptual framework. Those items then underwent additional forward-translation. The process was completed when the panel reviewed and accepted the new translation (Korean version 1.2).
Pilot testing
We performed a pilot test on 20 PAD patients to establish the appropriateness and comprehensibility of the question items for the patients’ situations, with a focus on their linguistical and cultural understanding of each item. Patients provided feedback when they had difficulty in understanding a question, when a question was vague or not relevant to them. After incorporating this feedback, we finalized the Korean version of PAQ (Korean version 1.3).
Reliability testing of the Korean PAQ
Reliability was tested using the test–retest method performed with a 2-week interval between the two administrations. The first test was done when the patient visited the clinic. Two weeks later, patients who reported no change in symptoms were asked to complete the questionnaire again. Twenty patients completed the retest. The other patients whose conditions were changed because of administration of new medication or revascularization, who refused the repeat test or were lost to follow-up were not included.
Statistical analyses
Statistical analyses of reliability and validity were performed using the SPSS version 12.0 (SPSS Inc., Chicago, IL, USA). To confirm reliability, test–retest correlation was assessed by intra-class correlation coefficient and verified by Spearman’s correlation coefficient. The internal consistency of each subscale was assessed by Cronbach’s alpha coefficient. Construct validity was evaluated by correlating the KPAQ items with the KHAQ score by Pearson’s correlation coefficient. Divergent validity was established by comparing the KPAQ scores of PAD patients by the severity of their claudication, as defined by the ECQ.
Results
Demographic and clinical characteristics
A total of 100 PAD patients were enrolled: 63 without severe claudication and 37 with severe claudication. The baseline characteristics of the subjects who entered into the final analysis are summarized in Table 1. Statistically significant differences in age, sex, body mass index, systolic blood pressure, total cholesterol, smoking status and prior diabetes mellitus were found between groups, with more adverse cardiovascular risk profiles in those with severe claudication. There were no significant differences in age, sex, education level and clinical findings between 20 PAD patients who participated in the test–retest reliability evaluation and the other 80 PAD patients.
Demographic and clinical characteristics of the Korean PAD sample
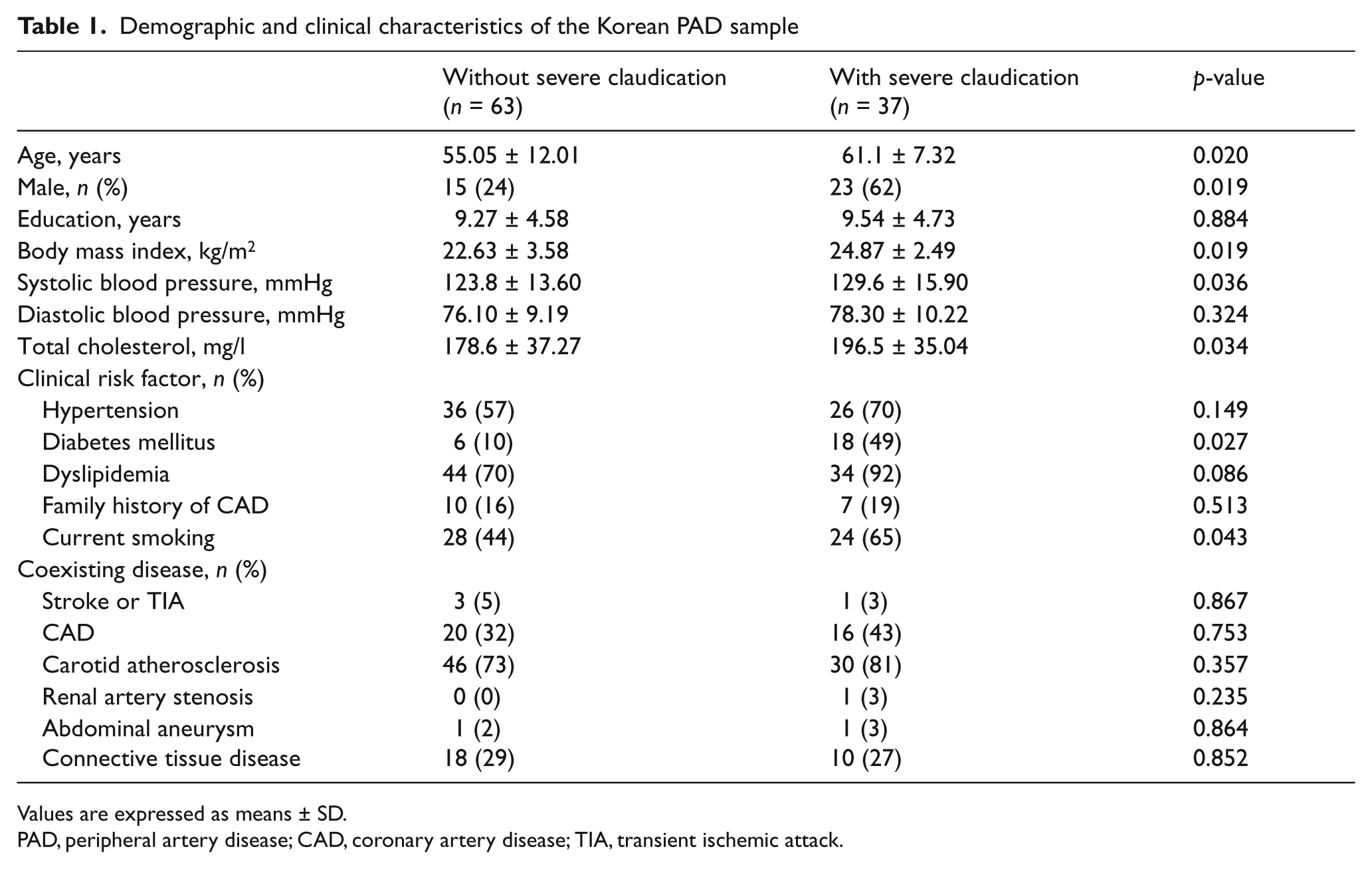
Values are expressed as means ± SD.
PAD, peripheral artery disease; CAD, coronary artery disease; TIA, transient ischemic attack.
Cross-cultural adaptation
The complete Korean version of PAQ is reproduced in the Appendix. During the translation/back-translation procedure, some questions were modified for the Korean culture. The term ‘blockages in the arteries’ was finally reconciled as ‘vascular problems or circulatory disturbance’, which was thought to be more easily understood in Korean culture and was confirmed in the pilot testing of 20 patients. The distance of ‘1–2 blocks’ was changed to ‘100–200 meters’ because the US reference to blocks is not common in Korea. Finally, minor grammatical changes, such as to the phrase ‘how much has discomfort, fatigue, pain, aching, or cramps in your calves (or buttocks) bothered you?’ were made to avoid contextual problems in Korean.
Pilot test
For 42 lines of the translated PAQ, all the lines of translation were understood by more than 80% of the 20 patients tested (median of 100%; range: 90–100%). No change to the text of the KPAQ was recommended by participants and no additional, important concepts not assessed in the PAQ were identified.
Clinical discriminant validity
The summary scores were 41.5 ± 19.8 (range 0–81.9) for the total PAD patients and the results of six domains were the following: the physical function score was 44.2 ± 25.6, stability score was 52.5 ± 27.3, symptom score was 45.2 ± 24.1, treatment satisfaction score was 69.4 ± 15.6, quality of life score was 30.6 ± 19.4, and social limitation score was 45.3 ± 27. Table 2 reports the results (mean ± SD) for the six PAQ domains in the patients with and without severe claudication as categorized by the ECQ. All domains, except stability score and treatment satisfaction, were clinically and statistically different between the groups.
The six domains (range 0–100) of PAQ between PAD patients without severe claudication and those with severe claudication tested by the Edinburgh Claudication Questionnaire
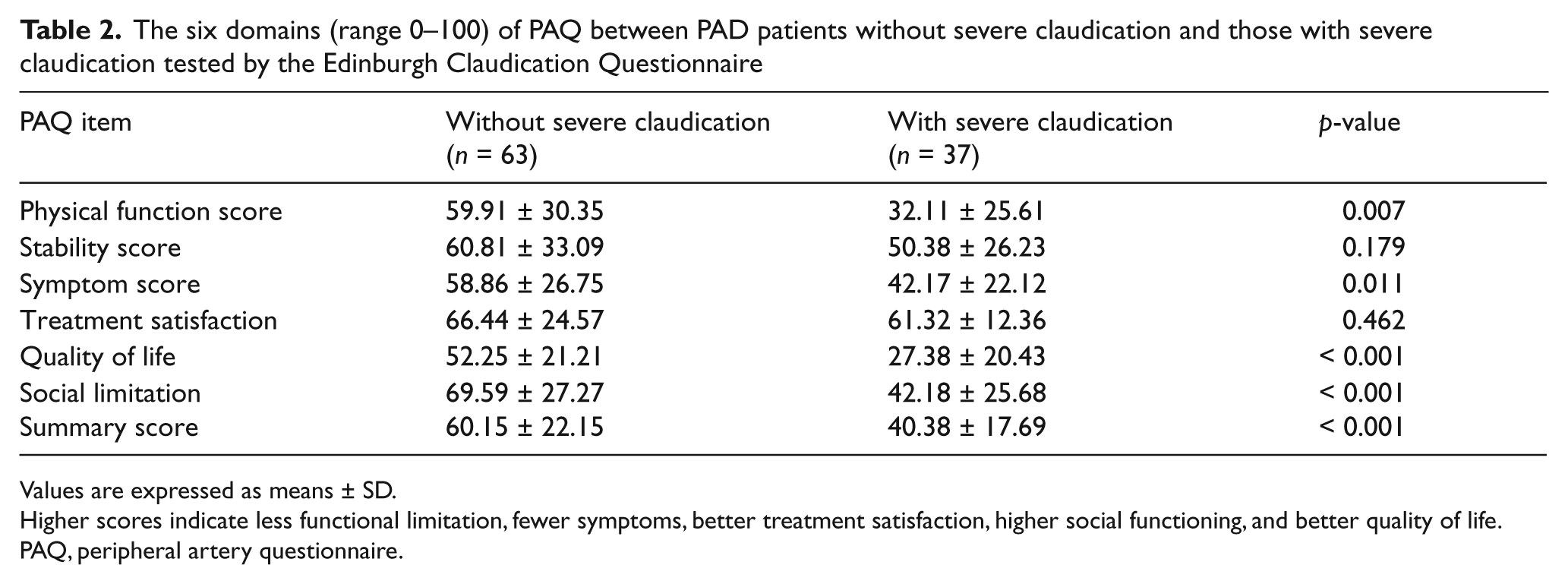
Values are expressed as means ± SD.
Higher scores indicate less functional limitation, fewer symptoms, better treatment satisfaction, higher social functioning, and better quality of life.
PAQ, peripheral artery questionnaire.
Internal consistency and test–retest reliability
Test–retest reliability was examined in 20 responders who reported no change in symptoms in the 2-week interval, and internal consistency was documented using Cronbach’s α. Cronbach’s α for each domain in all 100 PAD patients was > 0.80 for all domains. The paired t-test for change among the 20 participants in the test–retest reliability study revealed that the patient responded to the questionnaire consistently, without statistically significant differences. Mean inter-item correlations between the baseline and 2-week scores for the physical function domain was 0.97, for the symptom stability was 0.82, for the symptom scale was 0.96, for treatment satisfaction was 0.82, for quality of life was 0.91, for social limitation was 0.98, and for the summary score was 0.94 (all p < 0.001).
External validity between KPAQ and KHAQ
The correlations between KPAQ items and the KHAQ are summarized in Table 3. There were statistically significant correlations between the total KHAQ score, a generic measure of quality of life, and KPAQ physical function, stability, symptom, social limitation and quality of life scores (r = −0.24 ~ −0.90, all p < 0.05). Substantial correlations were obtained between the KHAQ walking subscale and the KPAQ physical function score (r = −0.55, p < 0.001).
External validity of the Korean PAQ (KPAQ); Spearman’s correlation coefficients between scores for the KPAQ items and for the Korean HAQ (KHAQ)
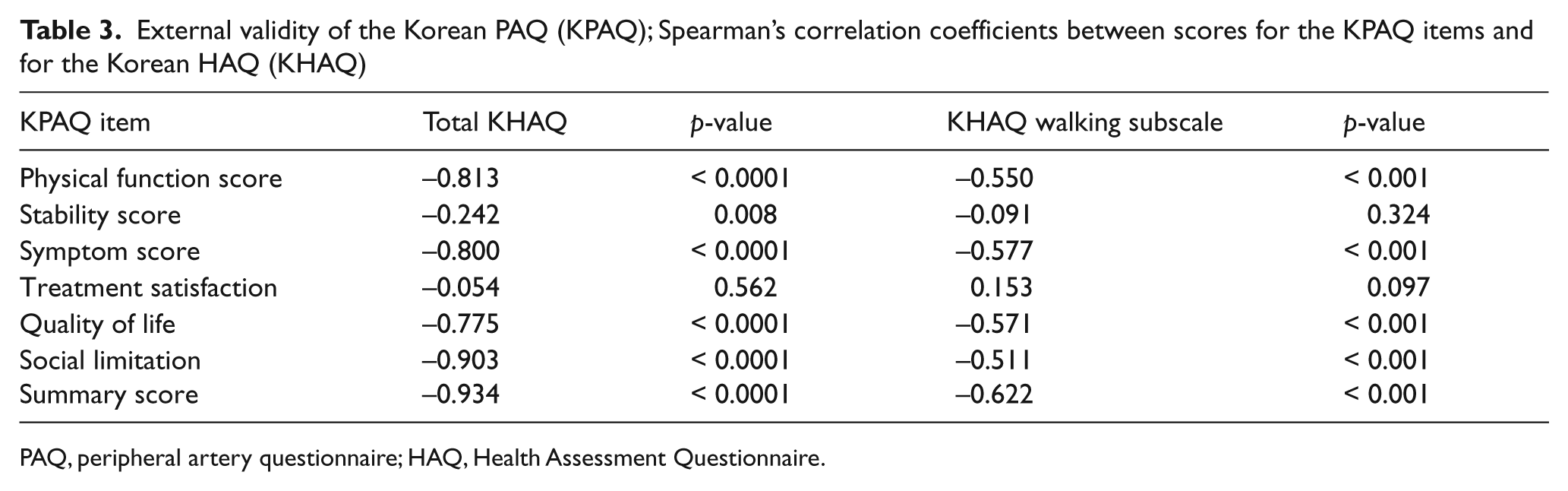
PAQ, peripheral artery questionnaire; HAQ, Health Assessment Questionnaire.
Discussion
PAD is a chronic arterial occlusive disease of the lower extremities caused by atherosclerosis. PAD can cause intermittent claudication, which is pain or weakness with walking that is relieved with rest. The prevalence of PAD increases with age and improving patients’ health status (their symptoms, function and quality of life) is a primary goal of treatment. To best measure patients’ perspectives of their PAD, a valid, reliable instrument is needed. In Korea, there are few methods to systematically monitor the health status of afflicted patients, particularly from their perspective. Accordingly, we sought to translate a previously established, disease-specific health status measure into Korean.
The results of our efforts suggest that the Korean version of the PAQ is a reliable and valid tool for the assessment of patients with PAD in Korea. The translation of an instrument from one language to another can present both cultural and linguistical problems, especially if the culture and socioeconomic characteristics of the populations differ. In this study, the Korean PAQ was fully cross-culturally adapted from the original English version with three forward and three back-translations. We attempted to deliver what was literally translated, as close as possible, to the original version, adjusting words and phrases as necessary. For example, ‘blockages in the arteries’ was finally reconciled as ‘vascular problems or circulatory disturbance’, which was better understood in the Korean culture. These changes resulted in near universal comprehension among Korean PAD patients undergoing careful debriefing of the instrument and provided good discriminant and construct validity, as well as good internal and test–retest reliability. For example, the internal consistency and test–retest correlation of the PAQ summary scale was similar to that reported by Smolderen et al. 10 Construct validity was evaluated by correlating the PAQ items with the scores of the Korean HAQ, with which we found substantial correlations. Importantly, PAQ items in which no similar domain was assessed with the HAQ, such as the treatment satisfaction scale, did not correlate with Korean HAQ scores. Additional work by Smolderen and colleagues found similar inter-correlations of the PAQ domains as our study. 13
Given that the goals of therapy are to improve symptoms and, thus, quality of life, several questionnaires have been used as endpoints to evaluate quality of life in PAD patients. The PAQ, 8 the ECQ, 6 the Walking Impairment Questionnaire (WIQ), 14 the Medical Outcomes Study 12-Item Short-Form (SF-12), 15 the EuroQol 5 Dimensions (EQ-5D) questionnaire, 13 and the San Diego Claudication Questionnaire 16 have all been used as the tools to evaluate improvements in functional status for patients with claudication. Other endpoints include peak walking time (PWT), changes in claudication onset time, change in community-based walking assessed by pedometer measurements over 7 days, and self-reported walking. Recently, 6-month outcomes of the Exercise Versus Endoluminal Revascularization (CLEVER) study assessed the disease-specific quality of life by the PAQ, WIQ, SF-12, PWT and cardiovascular risk factors. 17 Creating a Korean version of the PAQ creates the opportunity to monitor the disease-specific health status outcomes of PAD patients in Korea, both for clinical trials and routine clinical care.
Our findings should be interpreted in the context of the following potential limitations. While we examined a large population of patients to examine the internal consistency and validity, only a small population participated in the evaluation of test–retest reliability. Moreover, we did not explicitly test the responsiveness of the KPAQ to clinical changes. Further testing in additional Korean populations, including those undergoing revascularization, would be valuable to confirm similar sensitivities to clinical change as seen in the original version of the instrument. While we performed the cultural adaptation according to the recommended guidelines of the MAPI Institute 18 and mirrored established methods for performing culturally and linguistically valid translations, 18 residual difficulties in comprehensibility and performance may exist in other regions of Korea. Nevertheless, in light of our data that the Korean version of the PAQ has good reliability and validity, we believe that it is now ready to be used as a means for measuring health status and physical functioning in Korean patients with PAD.
Footnotes
Appendix
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
No potential conflict of interest relevant to this article was reported. Dr Spertus co-owns the copyright to the KPAQ.